The Prognostic Significance of Neutrophil-to-Lymphocyte Ratio in Head and Neck Cancer Patients Treated with Radiotherapy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Treatment Protocols
2.2. Hematologic Markers
2.3. Outcome Assessment
2.4. Statistical Analysis
3. Results
3.1. Patient and Treatment Characteristics
3.2. Hematologic Markers
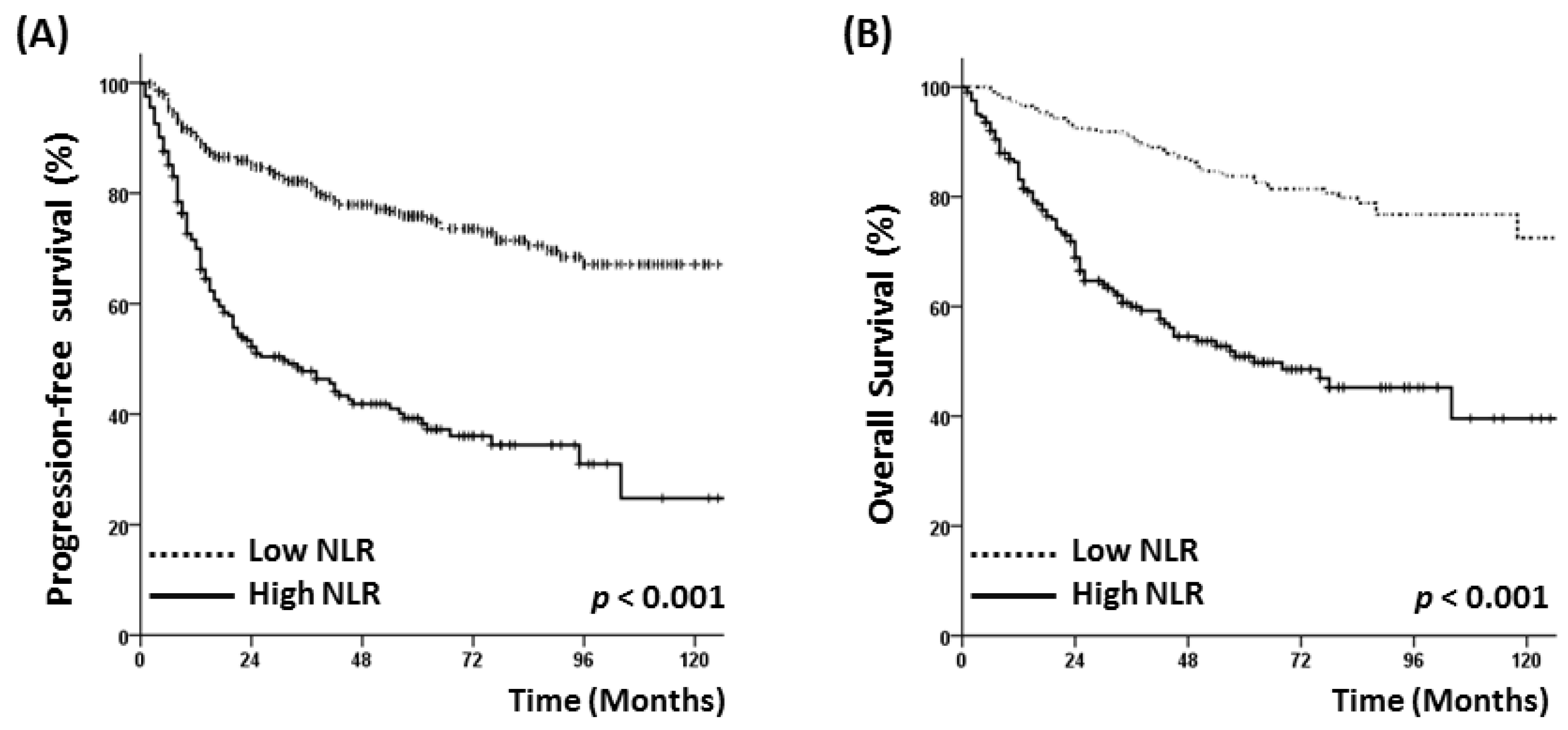
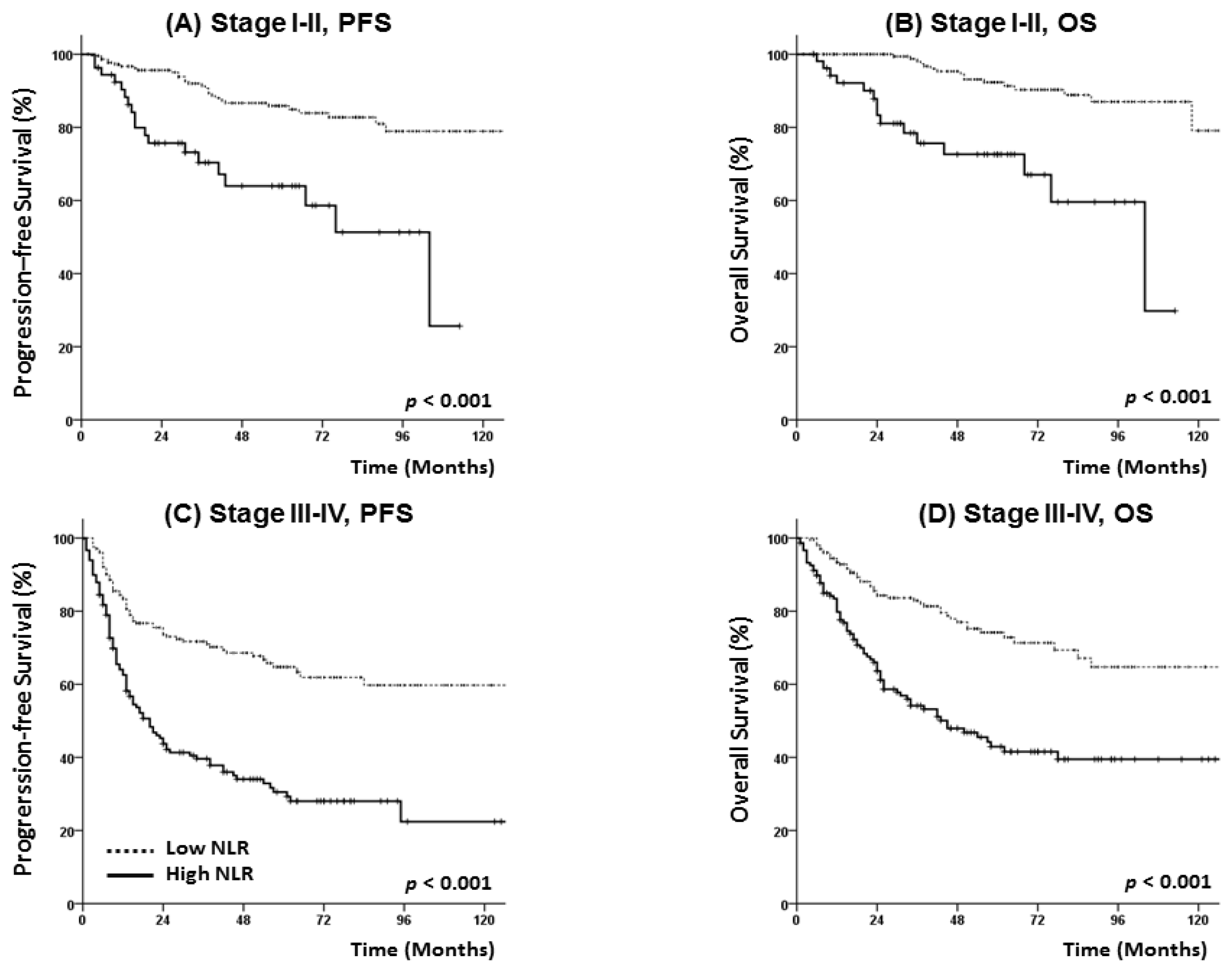
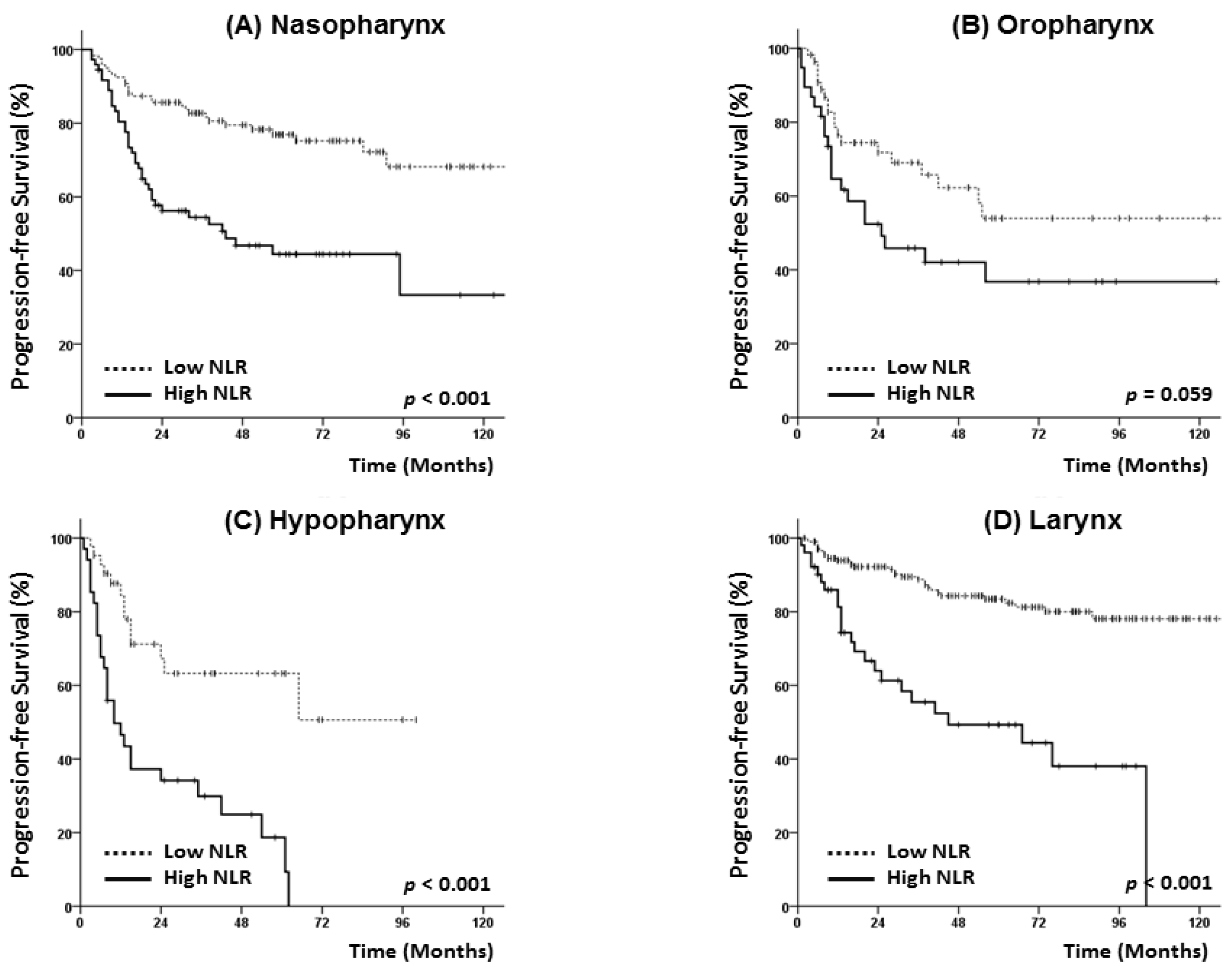
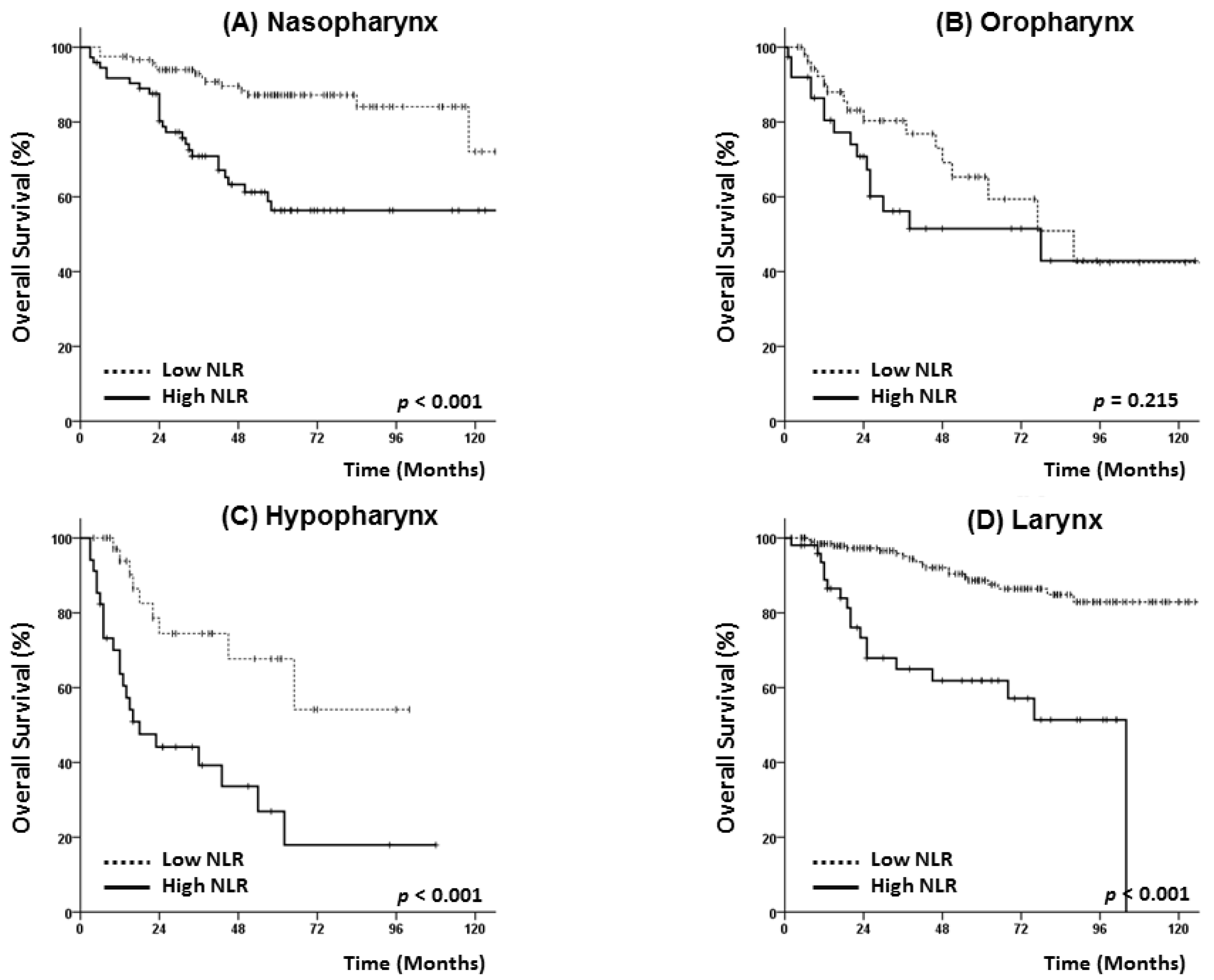
3.3. Survival Analysis
3.4. Analysis of Prognostic Factors
3.5. p16 Status and Hematologic Markers
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cho, Y.; Kim, K.H.; Yoon, H.I.; Kim, G.E.; Kim, Y.B. Tumor-related leukocytosis is associated with poor radiation response and clinical outcome in uterine cervical cancer patients. Ann. Oncol. 2016, 27, 2067–2074. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.C.; Kim, S.H.; Oh, S.Y.; Lee, S.; Lee, J.H.; Choi, H.J.; Park, K.J.; Roh, M.S.; Kim, S.G.; Kim, H.J.; et al. Clinical significance of preoperative neutrophil-lymphocyte versus platelet-lymphocyte ratio in patients with operable colorectal cancer. Biomarkers 2012, 17, 216–222. [Google Scholar] [CrossRef]
- Bhatti, I.; Peacock, O.; Lloyd, G.; Larvin, M.; Hall, R.I. Preoperative hematologic markers as independent predictors of prognosis in resected pancreatic ductal adenocarcinoma: Neutrophil-lymphocyte versus platelet-lymphocyte ratio. Am. J. Surg. 2010, 200, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Oh, S.Y.; Kim, S.H.; Lee, J.H.; Kim, M.C.; Kim, K.H.; Kim, H.J. Prognostic significance of neutrophil lymphocyte ratio and platelet lymphocyte ratio in advanced gastric cancer patients treated with folfox chemotherapy. BMC Cancer 2013, 13, 350. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Bitoux, M.A.; Stamenkovic, I. Tumor-host interactions: The role of inflammation. Histochem. Cell Biol. 2008, 130, 1079–1090. [Google Scholar] [CrossRef] [PubMed]
- Forget, P.; Khalifa, C.; Defour, J.P.; Latinne, D.; Van Pel, M.C.; De Kock, M. What is the normal value of the neutrophil-to-lymphocyte ratio? BMC Res. Note 2017, 10, 12. [Google Scholar] [CrossRef]
- Wang, J.; Jia, Y.; Wang, N.; Zhang, X.; Tan, B.; Zhang, G.; Cheng, Y. The clinical significance of tumor-infiltrating neutrophils and neutrophil-to-cd8+ lymphocyte ratio in patients with resectable esophageal squamous cell carcinoma. J. Transl. Med 2014, 12, 7. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, G.; Jiang, X.; Zhu, H.; Lu, Z.; Xu, L. Neutrophil to lymphocyte ratio in relation to risk of all-cause mortality and cardiovascular events among patients undergoing angiography or cardiac revascularization: A meta-analysis of observational studies. Atherosclerosis 2014, 234, 206–213. [Google Scholar] [CrossRef]
- Xue, P.; Kanai, M.; Mori, Y.; Nishimura, T.; Uza, N.; Kodama, Y.; Kawaguchi, Y.; Takaori, K.; Matsumoto, S.; Uemoto, S.; et al. Neutrophil-to-lymphocyte ratio for predicting palliative chemotherapy outcomes in advanced pancreatic cancer patients. Cancer Med. 2014, 3, 406–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rachidi, S.; Wallace, K.; Wrangle, J.M.; Day, T.A.; Alberg, A.J.; Li, Z. Neutrophil-to-lymphocyte ratio and overall survival in all sites of head and neck squamous cell carcinoma. Head Neck 2016, 38, E1068–E1074. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Kim, I.S.; Park, S.G.; Kim, H.; Choi, Y.J.; Seol, Y.M. Prognostic value of posttreatment neutrophil-lymphocyte ratio in head and neck squamous cell carcinoma treated by chemoradiotherapy. Auris Nasus Larynx 2017, 44, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Wang, H.; Yan, A.; Wang, H.; Li, X.; Liu, J.; Li, W. Pretreatment neutrophil to lymphocyte ratio in determining the prognosis of head and neck cancer: A meta-analysis. BMC Cancer 2018, 18, 383. [Google Scholar] [CrossRef]
- Park, B.; Yee, C.; Lee, K.M. The effect of radiation on the immune response to cancers. Int. J. Mol. Sci. 2014, 15, 927–943. [Google Scholar] [CrossRef]
- Golden, E.B.; Apetoh, L. Radiotherapy and immunogenic cell death. Semin. Radiat. Oncol. 2015, 25, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Chang, J.S.; Kwon, H.J.; Kim, S.H.; Shin, S.J.; Keum, K.C. Impact of p16 expression in oropharyngeal cancer in the postoperative setting: The necessity of re-evaluating traditional risk stratification. Jpn. J. Clin. Oncol. 2016, 46, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Charles, K.A.; Harris, B.D.; Haddad, C.R.; Clarke, S.J.; Guminski, A.; Stevens, M.; Dodds, T.; Gill, A.J.; Back, M.; Veivers, D.; et al. Systemic inflammation is an independent predictive marker of clinical outcomes in mucosal squamous cell carcinoma of the head and neck in oropharyngeal and non-oropharyngeal patients. BMC Cancer 2016, 16, 124. [Google Scholar] [CrossRef] [PubMed]
- Young, C.A.; Murray, L.J.; Karakaya, E.; Thygesen, H.H.; Sen, M.; Prestwich, R.J. The prognostic role of the neutrophil-to-lymphocyte ratio in oropharyngeal carcinoma treated with chemoradiotherapy. Clin. Med. Insight Oncol. 2014, 8, 81–86. [Google Scholar] [CrossRef]
- Fu, Y.; Liu, W.; OuYang, D.; Yang, A.; Zhang, Q. Preoperative neutrophil-to-lymphocyte ratio predicts long-term survival in patients undergoing total laryngectomy with advanced laryngeal squamous cell carcinoma: A single-center retrospective study. Medicine 2016, 95, e2689. [Google Scholar] [CrossRef]
- Sun, W.; Zhang, L.; Luo, M.; Hu, G.; Mei, Q.; Liu, D.; Long, G.; Hu, G. Pretreatment hematologic markers as prognostic factors in patients with nasopharyngeal carcinoma: Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio. Head Neck 2016, 38, E1332–E1340. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.H.; Waldron, J.N.; Milosevic, M.; Shen, X.; Ringash, J.; Su, J.; Tong, L.; Perez-Ordonez, B.; Weinreb, I.; Bayley, A.J.; et al. Prognostic value of pretreatment circulating neutrophils, monocytes, and lymphocytes in oropharyngeal cancer stratified by human papillomavirus status. Cancer 2015, 121, 545–555. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.S. P16 immunohistochemistry as a standalone test for risk stratification in oropharyngeal squamous cell carcinoma. Head Neck Pathol. 2012, 6, S75–S82. [Google Scholar] [CrossRef] [PubMed]
- Gupta, G.P.; Kumar, S.; Marron, D.; Amdur, R.J.; Hayes, D.N.; Weiss, J.; Grilley-Olson, J.; Zanation, A.; Hackman, T.; Zevallos, J.P.; et al. Circulating tumor hpv16 DNA as a biomarker of tumor genomics and disease control in hpv-associated oropharyngeal squamous cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 1310–1311. [Google Scholar] [CrossRef]
- Atzpodien, J.; Royston, P.; Wandert, T.; Reitz, M.; Group, D.G.C.R.C.C.-I.T. Metastatic renal carcinoma comprehensive prognostic system. Br. J. Cancer 2003, 88, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Walsh, S.R.; Cook, E.J.; Goulder, F.; Justin, T.A.; Keeling, N.J. Neutrophil-lymphocyte ratio as a prognostic factor in colorectal cancer. J. Surg. Oncol. 2005, 91, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Haram, A.; Boland, M.R.; Kelly, M.E.; Bolger, J.C.; Waldron, R.M.; Kerin, M.J. The prognostic value of neutrophil-to-lymphocyte ratio in colorectal cancer: A systematic review. J. Surg. Oncol. 2017, 115, 470–479. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Long, F.; Jaiswar, M.; Yang, L.; Wang, C.; Zhou, Z. Prognostic role of the neutrophil-to-lymphocyte ratio in pancreatic cancer: A meta-analysis. Sci. Rep. 2015, 5, 11026. [Google Scholar] [CrossRef] [PubMed]
- Rosculet, N.; Zhou, X.C.; Ha, P.; Tang, M.; Levine, M.A.; Neuner, G.; Califano, J. Neutrophil-to-lymphocyte ratio: Prognostic indicator for head and neck squamous cell carcinoma. Head Neck 2017, 39, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Motomura, T.; Shirabe, K.; Mano, Y.; Muto, J.; Toshima, T.; Umemoto, Y.; Fukuhara, T.; Uchiyama, H.; Ikegami, T.; Yoshizumi, T.; et al. Neutrophil-lymphocyte ratio reflects hepatocellular carcinoma recurrence after liver transplantation via inflammatory microenvironment. J. Hepatol. 2013, 58, 58–64. [Google Scholar] [CrossRef]
- Schetter, A.J.; Heegaard, N.H.; Harris, C.C. Inflammation and cancer: Interweaving microrna, free radical, cytokine and p53 pathways. Carcinogenesis 2010, 31, 37–49. [Google Scholar] [CrossRef]
- Mantovani, A.; Schioppa, T.; Porta, C.; Allavena, P.; Sica, A. Role of tumor-associated macrophages in tumor progression and invasion. Cancer Metastasis Rev. 2006, 25, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Templeton, A.J.; McNamara, M.G.; Seruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocana, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl Cancer Inst. 2014. [Google Scholar] [CrossRef] [PubMed]
- Nakahira, M.; Sugasawa, M.; Matsumura, S.; Kuba, K.; Ohba, S.; Hayashi, T.; Minami, K.; Ebihara, Y.; Kogashiwa, Y. Prognostic role of the combination of platelet count and neutrophil-lymphocyte ratio in patients with hypopharyngeal squamous cell carcinoma. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3863–3867. [Google Scholar] [CrossRef] [PubMed]
- Wojtukiewicz, M.Z.; Sierko, E.; Hempel, D.; Tucker, S.C.; Honn, K.V. Platelets and cancer angiogenesis nexus. Cancer Metastasis Rev. 2017, 36, 249–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sierko, E.; Wojtukiewicz, M.Z. Inhibition of platelet function: Does it offer a chance of better cancer progression control? Semin. Thrombosis Hemost. 2007, 33, 712–721. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Low NLR Group | High NLR Group | ||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | N = 621 | (%) | N = 425 | (%) | N = 196 | (%) | p Value | |
| Age | Median | 60 | 60 | 60 | 0.166 | |||
| (Range) | (18–94) | (18–89) | (18–94) | |||||
| Sex | Male | 514 | (82.8) | 365 | (85.9) | 149 | (76.0) | 0.002 |
| Female | 107 | (17.2 | 60 | (14.1) | 47 | (24.0) | ||
| Primary site | Nasopharynx | 192 | (30.9) | 119 | (28.0) | 73 | (37.2) | <0.001 |
| Oropharynx | 94 | (15.1) | 56 | (13.2) | 38 | (19.4) | ||
| Hypopharynx | 76 | (12.2) | 42 | (9.9) | 34 | (17.3) | ||
| Larynx | 259 | (41.7) | 208 | (48.9) | 51 | (26.0) | ||
| T classification | T1 | 259 | (41.7) | 206 | (48.5) | 53 | (27.0) | <0.001 |
| T2 | 145 | (23.3) | 97 | (22.8) | 48 | (24.5) | ||
| T3 | 94 | (15.1) | 52 | (12.2) | 42 | (21.4) | ||
| T4 | 123 | (19.8) | 70 | (16.5) | 53 | (27.0) | ||
| N classification | N0 | 294 | (47.3) | 236 | (55.5) | 58 | (29.6) | <0.001 |
| N1 | 87 | (14.0) | 56 | (13.2) | 31 | (15.8) | ||
| N2 | 219 | (35.3) | 124 | (29.2) | 95 | (48.5) | ||
| N3 | 21 | (3.4) | 9 | (2.1) | 12 | (6.1) | ||
| Overall stage | I | 188 | (30.3) | 165 | (38.8) | 23 | (11.7) | <0.001 |
| II | 89 | (14.3) | 58 | (13.6) | 31 | (15.8) | ||
| III | 118 | (19.0) | 76 | (17.9) | 42 | (21.4) | ||
| IVA | 204 | (32.9) | 116 | (27.3) | 88 | (44.9) | ||
| IVB | 22 | (3.5) | 10 | (2.4) | 12 | (6.1) | ||
| p16 | UE b | 56 | (59.6) | 31 | (55.4) | 25 | (65.8) | 0.529 |
| (in oropharynx) | negative | 12 | (1.9) | 6 | (10.7) | 6 | (15.8) | |
| positive | 26 | (4.2) | 19 | (33.9) | 7 | (18.4) | ||
| Treatment | RT alone | 270 | (43.5) | 221 | (52.0) | 49 | (25.0) | <0.001 |
| CCRT c | 234 | (37.7) | 130 | (30.6) | 104 | (53.1) | ||
| Induction + CCRT | 117 | (18.8) | 74 | (17.4) | 43 | (21.9) | ||
| RT modality | 3D-CRT d | 220 | (35.4) | 156 | (36.7) | 64 | (32.7) | 0.326 |
| IMRT e | 401 | (64.6) | 269 | (63.3) | 132 | (67.3) | ||
| RT duration | Median | 46 | 45 | 47 | <0.001 | |||
| (days) | (Range) | (23–99) | (23–99) | (31–97) | ||||
| Total dose | <70 | 385 | (61.0) | 277 | (64.6) | 108 | (53.5) | 0.016 |
| (EQD2Gy a, α/β = 10) | ≥70 | 236 | (37.4) | 148 | (34.5) | 88 | (43.6) | |
| Total | low NLR Group | High NLR Group | ||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | N = 621 | (%) | N = 425 | (%) | N = 196 | (%) | p Value | |
| WBC | Median | 6800 | 6300 | 7700 | <0.001 | |||
| (cells/μL) | (range) | (2000–21,100) | (2000–10,700) | (3700–21,100) | ||||
| ANC a | Median | 3900 | 3460 | 5520 | <0.001 | |||
| (cells/μL) | (range) | (560–18,310) | (940–6720) | (560–18,300) | ||||
| ALC b | Median | 1810 | 2040 | 1320 | <0.001 | |||
| (cells/ μL) | (range) | (160–3700) | (700–3700) | (160–2970) | ||||
| Platelet | Median | 237 | 232 | 250 | <0.001 | |||
| (×103 cells/μL) | (range) | (14–600) | (14–517) | (40–600) | ||||
| PLR c | Median | 131 | 116 | 194 | <0.001 | |||
| (range) | (20–1733) | 20–269 | (26–1733) | |||||
| Hemoglobin | Median | 14 | 14.1 | 13.5 | 0.01 | |||
| (mg/dL) | (range) | (51–15.1) | (5.1–17.4) | (8.3–51.1) | ||||
| Anemia | No | 497 | (80.0) | 359 | (84.5) | 138 | (70.4) | <0.001 |
| Yes | 124 | (20.0) | 66 | (15.5) | 58 | (29.6) | ||
| Albumin | Median | 4.4 | 4.4 | 4.3 | <0.001 | |||
| (g/dL) | (range) | (2.5–5.2) | (2.7–5.2) | (2.5–5.1) | ||||
| Hypoalbuminemia | UE e | 69 | (11.1) | 49 | (11.5) | 20 | (10.2) | 0.02 |
| (<3.3 g/dL) | No | 539 | (86.8) | 371 | (87.3) | 168 | (85.7) | |
| Yes | 13 | (2.1) | 5 | (1.2) | 8 | (4.1) | ||
| Onodera’s PNI d | Median | 53.1 | 55 | 49.7 | <0.001 | |||
| (range) | (27.8–67.6) | (32.8–67.6) | (27.8–61.7) | |||||
| Progression-Free Survival | Overall Survival | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||||||
| HR | 95%CI | p | HR | 95%CI | p | HR | 95%CI | p | HR | 95%CI | p | ||
| Age | <60 | 1 | 1 | 1 | 1 | ||||||||
| ≥60 | 1.61 | 1.22–2.12 | 0.001 | 1.54 | 1.08–2.19 | 0.017 | 2.40 | 1.71–3.37 | <0.001 | 2.43 | 1.57–3.75 | <0.001 | |
| Sex | Male | 1 | 1 | ||||||||||
| Female | 0.97 | 0.68–1.38 | 0.865 | 0.99 | 0.66–1.51 | 0.981 | |||||||
| Primary site | Nasopharynx | 1 | 1 | 1 | 1 | ||||||||
| Oropharynx | 1.78 | 1.21–2.62 | 0.003 | 1.04 | 0.67–1.61 | 0.859 | 2.29 | 1.44–3.62 | <0.001 | 1.19 | 0.68–2.09 | 0.54 | |
| Hypophrynx | 2.46 | 1.66–3.66 | <0.001 | 1.88 | 1.17–3.01 | 0.009 | 3.41 | 2.13–5.44 | <0.001 | 2.01 | 1.13–3.55 | 0.017 | |
| Larynx | 0.63 | 0.44–0.91 | 0.012 | 1.07 | 0.65–1.76 | 0.786 | 0.74 | 0.48–1.15 | 0.181 | 0.97 | 0.49–1.90 | 0.924 | |
| T classification | T1, 2 | 1 | 1 | 1 | 1 | ||||||||
| T3, 4 | 3.05 | 2.32–4.00 | <0.001 | 2.03 | 1.37–3.00 | <0.001 | 3.53 | 2.54–4.90 | <0.001 | 2.39 | 1.48–3.86 | <0.001 | |
| N classification | N0 | 1 | 1 | 1 | 1 | ||||||||
| N1-3 | 2.78 | 2.06–3.77 | <0.001 | 1.37 | 0.81–2.32 | 0.237 | 2.52 | 1.76–3.60 | <0.001 | 1.11 | 0.60–2.04 | 0.749 | |
| Overall stage | I-II | 1 | 1 | 1 | 1 | ||||||||
| III-IVB | 3.48 | 2.52–4.81 | <0.001 | 1.44 | 0.78-2.67 | 0.244 | 3.76 | 2.53–5.60 | <0.001 | 1.58 | 0.71–3.48 | 0.26 | |
| Treatment | RT alone | 1 | 1 | 1 | 1 | ||||||||
| CCRT e | 2.83 | 2.06–3.90 | <0.001 | 1.11 | 0.63–1.96 | 0.723 | 2.65 | 1.81–3.88 | <0.001 | 1.02 | 0.53–1.98 | 0.951 | |
| Induction + CCRT | 2.09 | 1.42–3.07 | <0.001 | 0.77 | 0.41–1.46 | 0.425 | 1.98 | 1.25–3.13 | 0.003 | 0.85 | 0.38–1.64 | 0.519 | |
| RT modality | 3D CRT f | 1 | 1 | ||||||||||
| IMRT g | 1.26 | 0.95–1.68 | 0.107 | 1.19 | 0.86–1.66 | 0.298 | |||||||
| Anemia | No | 1 | 1 | 1 | 1 | ||||||||
| Yes | 2.25 | 1.69–3.00 | <0.001 | 1.19 | 0.81–1.74 | 0.374 | 0.52 | 0.37–0.72 | <0.001 | 0.96 | 0.63–1.45 | 0.829 | |
| WBC (cells/μL) | <9000 | 1 | 1 | 1 | 1 | ||||||||
| (cells/μL) | ≥9000 | 1.81 | 1.30–2.52 | <0.001 | 0.93 | 0.61–1.43 | 0.748 | 1.62 | 1.08–2.42 | 0.021 | 0.73 | 0.43–1.23 | 0.233 |
| ANC a | <4000 | 1 | 1 | 1 | 1 | ||||||||
| (cells/μL) | ≥4000 | 1.81 | 1.38–2.39 | <0.001 | 0.75 | 0.51–1.10 | 0.142 | 2.02 | 1.45–2.81 | <0.001 | 0.79 | 0.50–1.27 | 0.333 |
| ALC b | <2000 | 1 | 1 | 1 | 1 | ||||||||
| (cells/μL) | ≥2000 | 0.61 | 0.45–0.82 | 0.001 | 1.10 | 0.72–1.68 | 0.672 | 0.55 | 0.38–0.79 | 0.001 | 1.10 | 0.64–1.89 | 0.72 |
| Platelet | <230 | 1 | 1 | ||||||||||
| (103 cells/μL) | ≥230 | 0.98 | 0.74–1.28 | 0.857 | 1.04 | 0.75–1.44 | 0.825 | ||||||
| NLR | <2.7 | 1 | 1 | 1 | 1 | ||||||||
| ≥2.7 | 3.39 | 2.58–4.46 | <0.001 | 4.10 | 2.66–6.34 | <0.001 | 3.86 | 2.78–5.35 | <0.001 | 4.63 | 2.69–7.94 | <0.001 | |
| PLR c | <150 | 1 | 1 | 1 | 1 | ||||||||
| ≥150 | 1.79 | 1.36–2.36 | 0.001 | 1.57 | 1.20–2.06 | 0.03 | 1.96 | 1.42–2.74 | 0.001 | 1.24 | 0.96–2.40 | 0.096 | |
| Hypoalbuminemia | No | 1 | 1 | 1 | 1 | ||||||||
| Yes | 4.18 | 2.20–7.93 | <0.001 | 1.92 | 0.95–3.85 | 0.068 | 0.44 | 0.3–0.66 | <0.001 | 1.54 | 0.69–3.42 | 0.288 | |
| Onodera’s PNI d | <50 | 1 | 1 | 1 | 1 | ||||||||
| ≥50 | 0.48 | 0.36–0.65 | <0.001 | 0.80 | 0.53–1.23 | 0.316 | 0.44 | 0.31–0.63 | <0.001 | 0.74 | 0.45–1.24 | 0.259 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, Y.; Kim, J.W.; Yoon, H.I.; Lee, C.G.; Keum, K.C.; Lee, I.J. The Prognostic Significance of Neutrophil-to-Lymphocyte Ratio in Head and Neck Cancer Patients Treated with Radiotherapy. J. Clin. Med. 2018, 7, 512. https://doi.org/10.3390/jcm7120512
Cho Y, Kim JW, Yoon HI, Lee CG, Keum KC, Lee IJ. The Prognostic Significance of Neutrophil-to-Lymphocyte Ratio in Head and Neck Cancer Patients Treated with Radiotherapy. Journal of Clinical Medicine. 2018; 7(12):512. https://doi.org/10.3390/jcm7120512
Chicago/Turabian StyleCho, Yeona, Jun Won Kim, Hong In Yoon, Chang Geol Lee, Ki Chang Keum, and Ik Jae Lee. 2018. "The Prognostic Significance of Neutrophil-to-Lymphocyte Ratio in Head and Neck Cancer Patients Treated with Radiotherapy" Journal of Clinical Medicine 7, no. 12: 512. https://doi.org/10.3390/jcm7120512