Clinical Impact of Sequence Type 131 in Adults with Community-Onset Monomicrobial Escherichia Coli Bacteremia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Microbiological and Molecular Methods
2.4. Definitions
2.5. Statistical Analysis
3. Results
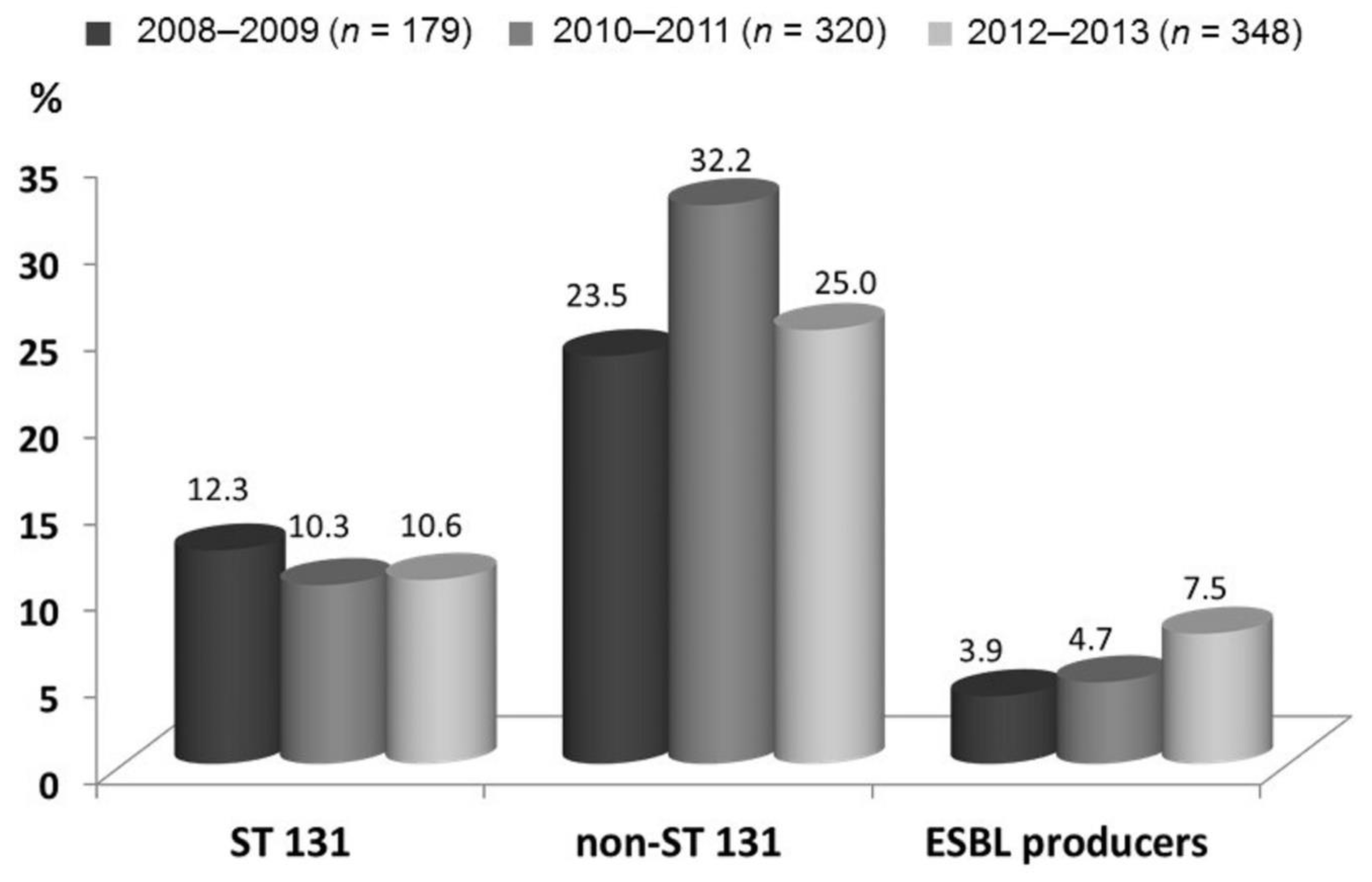
3.1. Demographics and Clinical Characteristics of the Study Population
3.2. Comparisons of Clinical Characteristics, Severity, Susceptibility, and Outcome Between ST131 and Non-ST131 Clonal Groups
3.3. Risk Factors of 28-Day Crude Mortality
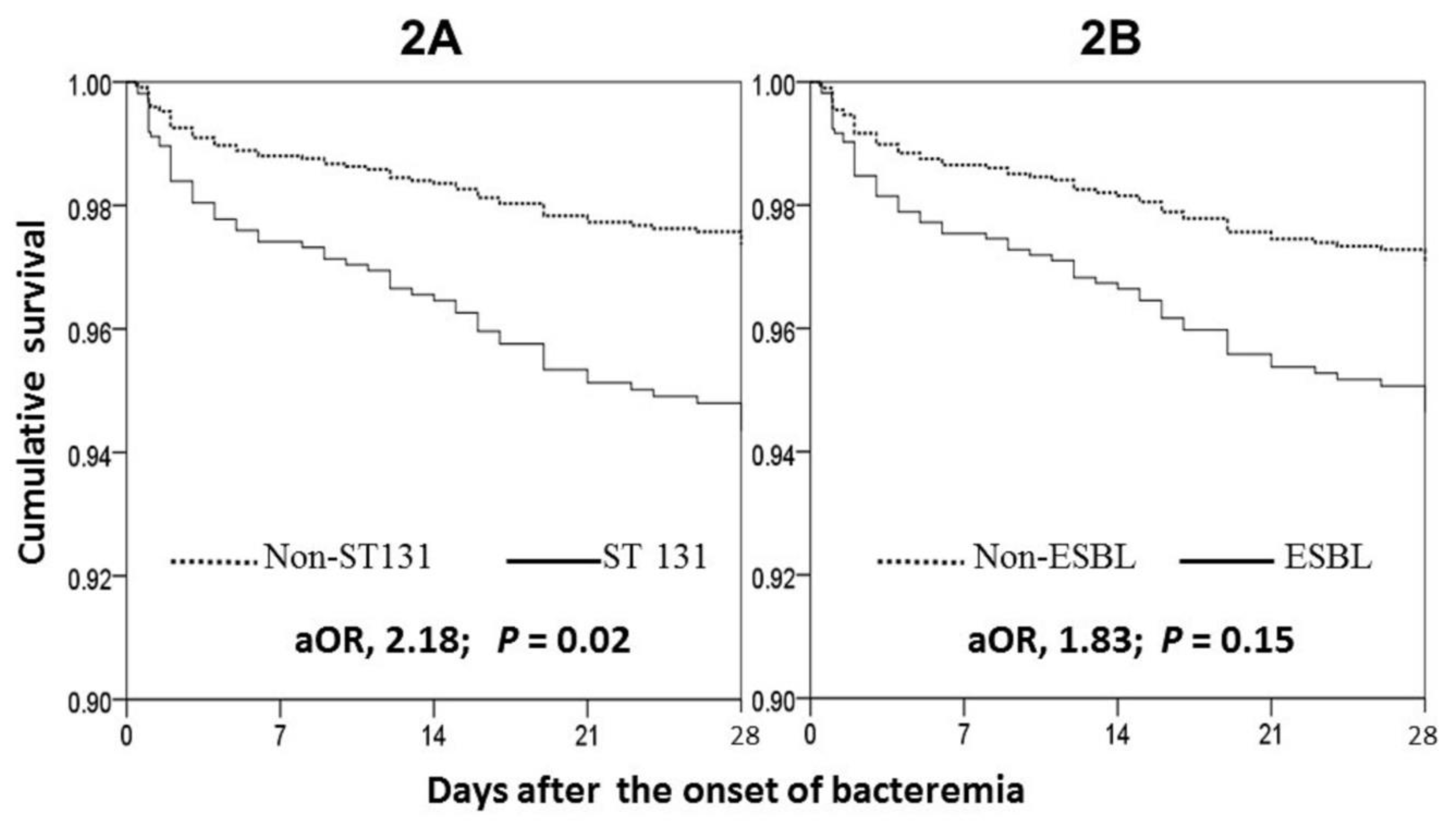
3.4. Clinical Impact of the ST131 Clone and ESBL Production
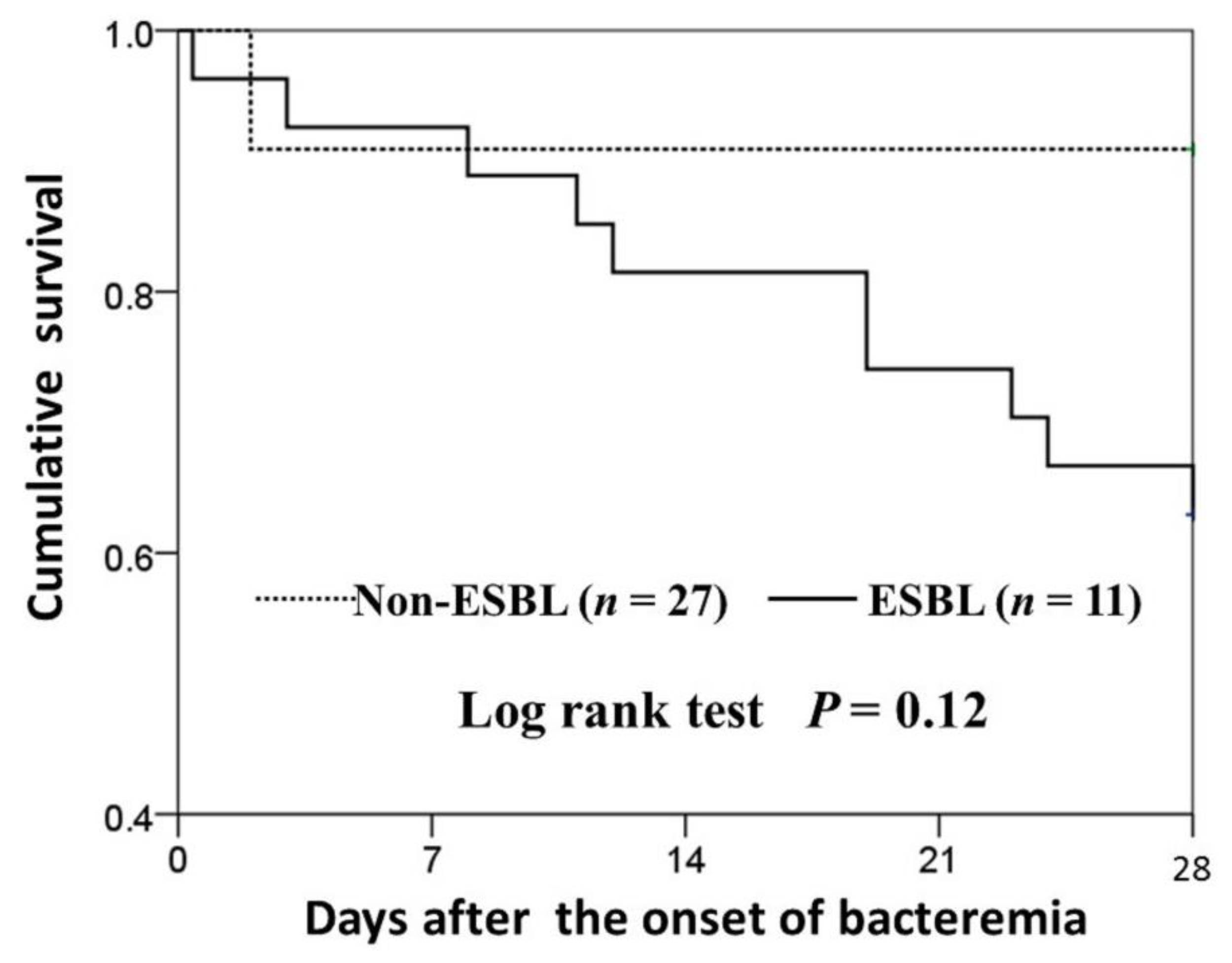
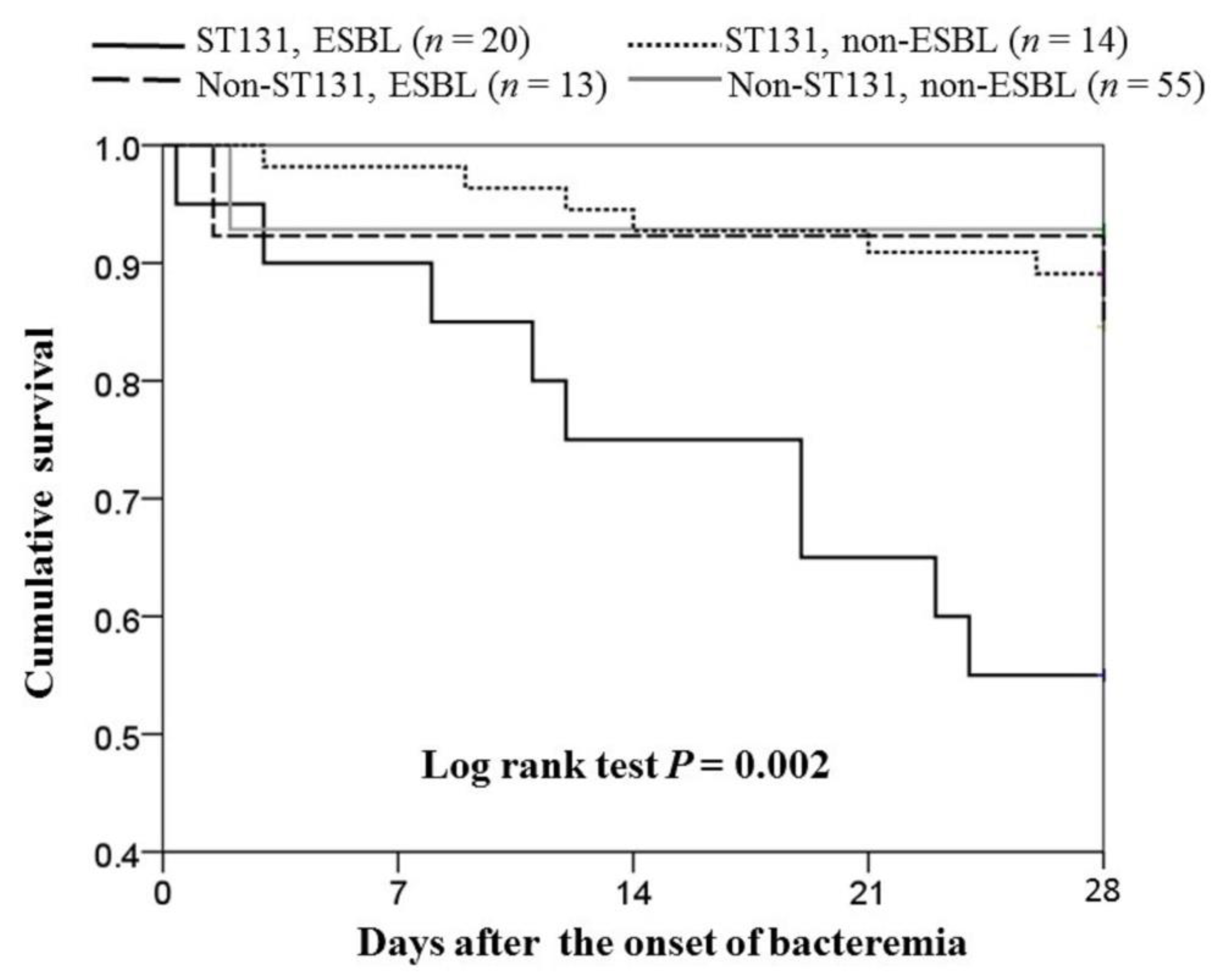
3.5. Clinical Impact of the ST131 Clone in the ESBL and Non-ESBL Subgroups
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Laupland, K.B.; Gregson, D.B.; Flemons, W.W.; Hawkins, D.; Ross, T.; Church, D.L. Burden of community-onset bloodstream infection: A population-based assessment. Epidemiol. Infect. 2007, 135, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.W.; Pruess, K.E.; Lee, T.H. How bad are bacteremia and sepsis? Outcomes in a cohort with suspected bacteremia. Arch Intern. Med. 1995, 155, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.C.; Lin, W.L.; Lin, C.C.; Hsieh, W.H.; Hsieh, C.H.; Wu, M.H.; Wu, J.Y.; Lee, C.C. Outcome of inadequate empirical antibiotic therapy in emergency department patients with community-onset bloodstream infections. J. Antimicrob. Chemother. 2013, 68, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.C.; Lee, C.H.; Hong, M.Y.; Tang, H.J.; Ko, W.C. Timing of appropriate empirical antimicrobial administration and outcome of adults with community-onset bacteremia. Crit. Care 2017, 21, 119. [Google Scholar] [CrossRef] [PubMed]
- Peralta, G.; Sanchez, M.B.; Garrido, J.C.; De Benito, I.; Cano, M.E.; Martinez-Martinez, L.; Roiz, M.P. Impact of antibiotic resistance and of adequate empirical antibiotic treatment in the prognosis of patients with Escherichia coli bacteraemia. J. Antimicrob. Chemother. 2007, 60, 855–863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lautenbach, E.; Metlay, J.P.; Bilker, W.B.; Edelstein, P.H.; Fishman, N.O. Association between fluoroquinolone resistance and mortality in Escherichia coli and Klebsiella pneumoniae infections: The role of inadequate empirical antimicrobial therapy. Clin. Infect. Dis. 2005, 41, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Horner, C.; Fawley, W.; Morris, K.; Parnell, P.; Denton, M.; Wilcox, M. Escherichia coli bacteraemia: 2 years of prospective regional surveillance (2010–2012). J. Antimicrob. Chemother. 2014, 69, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Riley, L.W. Pandemic lineages of extraintestinal pathogenic Escherichia coli. Clin. Microbiol. Infect. 2014, 20, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, R.; Johnson, J.R. A new clone sweeps clean: The enigmatic emergence of Escherichia coli sequence type 131. Antimicrob. Agents Chemother. 2014, 58, 4997–5004. [Google Scholar] [CrossRef]
- Cha, M.K.; Kang, C.I.; Kim, S.H.; Cho, S.Y.; Ha, Y.E.; Wi, Y.M.; Chung, D.R.; Peck, K.R.; Song, J.H.; Korean Network for Study on Infectious, D. Comparison of the microbiological characteristics and virulence factors of ST131 and non-ST131 clones among extended-spectrum beta-lactamase-producing Escherichia coli causing bacteremia. Diagn. Microbiol. Infect. Dis. 2016, 84, 102–104. [Google Scholar] [CrossRef]
- Chung, H.C.; Lai, C.H.; Lin, J.N.; Huang, C.K.; Liang, S.H.; Chen, W.F.; Shih, Y.C.; Lin, H.H.; Wang, J.L. Bacteremia caused by extended-spectrum-beta-lactamase-producing Escherichia coli sequence type ST131 and non-ST131 clones: Comparison of demographic data, clinical features, and mortality. Antimicrob. Agents Chemother. 2012, 56, 618–622. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Cerero, L.; Navarro, M.D.; Bellido, M.; Martin-Pena, A.; Vinas, L.; Cisneros, J.M.; Gomez-Langley, S.L.; Sanchez-Monteseirin, H.; Morales, I.; Pascual, A.; et al. Escherichia coli belonging to the worldwide emerging epidemic clonal group O25b/ST131: Risk factors and clinical implications. J. Antimicrob. Chemother. 2014, 69, 809–814. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, 26th ed.; CLSI supplement M100-S26; CLSI: Wayne, PA, USA, 2016. [Google Scholar]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, 19th ed.; CLSI supplement M100-S19; CLSI: Wayne, PA, USA, 2009. [Google Scholar]
- Gibreel, T.M.; Dodgson, A.R.; Cheesbrough, J.; Fox, A.J.; Bolton, F.J.; Upton, M. Population structure, virulence potential and antibiotic susceptibility of uropathogenic Escherichia coli from Northwest England. J. Antimicrob. Chemother. 2012, 67, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Doumith, M.; Day, M.; Ciesielczuk, H.; Hope, R.; Underwood, A.; Reynolds, R.; Wain, J.; Livermore, D.M.; Woodford, N. Rapid identification of major Escherichia coli sequence types causing urinary tract and bloodstream infections. J. Clin. Microbiol. 2015, 53, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Clermont, O.; Gordon, D.; Denamur, E. Guide to the various phylogenetic classification schemes for Escherichia coli and the correspondence among schemes. Microbiology 2015, 161, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Kallonen, T.; Brodrick, H.J.; Harris, S.R.; Corander, J.; Brown, N.M.; Martin, V.; Peacock, S.J.; Parkhill, J. Systematic longitudinal survey of invasive Escherichia coli in England demonstrates a stable population structure only transiently disturbed by the emergence of ST131. Genome Res. 2017, 27, 116. [Google Scholar] [CrossRef]
- Lee, C.C.; Wang, J.L.; Lee, C.H.; Hung, Y.P.; Hong, M.Y.; Chang, C.M.; Ko, W.C. Age-Related Trends in Adults with Community-Onset Bacteremia. Antimicrob. Agents Chemother. 2017, 61, e01050-17. [Google Scholar] [CrossRef]
- Gilbert, D.N.; Moellering, R.C., Jr.; Eliopoulos, G.M.; Chambers, H.F.; Saag, M.S. Selected pharmacologic faetures of antimicrobial agents. Sanford Guide Antimicrob. Ther. 2009, 1, 78–82. [Google Scholar]
- Schellevis, F.G.; van der Velden, J.; van de Lisdonk, E.; van Eijk, J.T.; van Weel, C. Comorbidity of chronic diseases in general practice. J. Clin. Epidemiol. 1993, 46, 469–473. [Google Scholar] [CrossRef]
- McCabe, W.R. Gram-negative bacteremia. Adv. Intern. Med. 1974, 19, 135–158. [Google Scholar] [PubMed]
- Dhanji, H.; Doumith, M.; Rooney, P.J.; O’Leary, M.C.; Loughrey, A.C.; Hope, R.; Woodford, N.; Livermore, D.M. Molecular epidemiology of fluoroquinolone-resistant ST131 Escherichia coli producing CTX-M extended-spectrum beta-lactamases in nursing homes in Belfast, UK. J. Antimicrob. Chemother. 2011, 66, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Arvand, M.; Moser, V.; Pfeifer, Y. Prevalence of extended-spectrum-beta-lactamase-producing Escherichia coli and spread of the epidemic clonal lineage ST131 in nursing homes in Hesse, Germany. J. Antimicrob. Chemother. 2013, 68, 2686–2688. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, R.; Johnston, B.; Lohse, C.; Porter, S.B.; Clabots, C.; Johnson, J.R. Escherichia coli sequence type 131 is a dominant, antimicrobial-resistant clonal group associated with healthcare and elderly hosts. Infect. Control Hosp. Epidemiol. 2013, 34, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.R.; Thuras, P.; Johnston, B.D.; Weissman, S.J.; Limaye, A.P.; Riddell, K.; Scholes, D.; Tchesnokova, V.; Sokurenko, E. The Pandemic H30 Subclone of Escherichia coli Sequence Type 131 Is Associated With Persistent Infections and Adverse Outcomes Independent From Its Multidrug Resistance and Associations With Compromised Hosts. Clin. Infect. Dis. 2016, 62, 1529–1536. [Google Scholar] [CrossRef] [PubMed]
- Liss, M.A.; Johnson, J.R.; Porter, S.B.; Johnston, B.; Clabots, C.; Gillis, K.; Nseyo, U.; Holden, M.; Sakamoto, K.; Fierer, J. Clinical and microbiological determinants of infection after transrectal prostate biopsy. Clin. Infect. Dis. 2015, 60, 979–987. [Google Scholar] [CrossRef] [PubMed]
- Van der Donk, C.F.; van de Bovenkamp, J.H.; De Brauwer, E.I.; De Mol, P.; Feldhoff, K.H.; Kalka-Moll, W.M.; Nys, S.; Thoelen, I.; Trienekens, T.A.; Stobberingh, E.E. Antimicrobial resistance and spread of multi drug resistant Escherichia coli isolates collected from nine urology services in the Euregion Meuse-Rhine. PLoS ONE 2012, 7, e47707. [Google Scholar] [CrossRef] [PubMed]
- Morales-Barroso, I.; Lopez-Cerero, L.; Molina, J.; Bellido, M.; Navarro, M.D.; Serrano, L.; Gonzalez-Galan, V.; Praena, J.; Pascual, A.; Rodriguez-Bano, J. Bacteraemia due to non-ESBL-producing Escherichia coli O25b:H4 sequence type 131: Insights into risk factors, clinical features and outcomes. Int. J. Antimicrob. Agents 2017, 49, 498–502. [Google Scholar] [CrossRef]
- Can, F.; Azap, O.K.; Seref, C.; Ispir, P.; Arslan, H.; Ergonul, O. Emerging Escherichia coli O25b/ST131 clone predicts treatment failure in urinary tract infections. Clin. Infect. Dis. 2015, 60, 523–527. [Google Scholar] [CrossRef]
- Johnson, J.R.; Porter, S.B.; Zhanel, G.; Kuskowski, M.A.; Denamur, E. Virulence of Escherichia coli clinical isolates in a murine sepsis model in relation to sequence type ST131 status, fluoroquinolone resistance, and virulence genotype. Infect. Immun. 2012, 80, 1554–1562. [Google Scholar] [CrossRef]
- Mora, A.; Dahbi, G.; Lopez, C.; Mamani, R.; Marzoa, J.; Dion, S.; Picard, B.; Blanco, M.; Alonso, M.P.; Denamur, E.; et al. Virulence patterns in a murine sepsis model of ST131 Escherichia coli clinical isolates belonging to serotypes O25b:H4 and O16:H5 are associated to specific virotypes. PLoS ONE 2014, 9, e87025. [Google Scholar] [CrossRef] [PubMed]
- Ciesielczuk, H.; Betts, J.; Phee, L.; Doumith, M.; Hope, R.; Woodford, N.; Wareham, D.W. Comparative virulence of urinary and bloodstream isolates of extra-intestinal pathogenic Escherichia coli in a Galleria mellonella model. Virulence 2015, 6, 145–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, A.; Ranjan, A.; Nandanwar, N.; Babbar, A.; Jadhav, S.; Ahmed, N. Genotypic and phenotypic profiles of Escherichia coli isolates belonging to clinical sequence type 131 (ST131), clinical non-ST131, and fecal non-ST131 lineages from India. Antimicrob. Agents Chemother. 2014, 58, 7240–7249. [Google Scholar] [CrossRef]
- Rodriguez-Bano, J.; Picon, E.; Gijon, P.; Hernandez, J.R.; Ruiz, M.; Pena, C.; Almela, M.; Almirante, B.; Grill, F.; Colomina, J.; et al. Community-onset bacteremia due to extended-spectrum beta-lactamase-producing Escherichia coli: Risk factors and prognosis. Clin. Infect. Dis. 2010, 50, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.J.; Shen, Y.H.; Hwang, K.P. Clinical implications, risk factors and mortality following community-onset bacteremia caused by extended-spectrum beta-lactamase (ESBL) and non-ESBL producing Escherichia coli. J. Microbiol. Immunol. Infect. 2010, 43, 240–248. [Google Scholar] [CrossRef]
- Mathers, A.J.; Peirano, G.; Pitout, J.D. The role of epidemic resistance plasmids and international high-risk clones in the spread of multidrug-resistant Enterobacteriaceae. Clin. Microbiol. Rev. 2015, 28, 565–591. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients Number (%) | p-Values | |
|---|---|---|---|
| ST131, n = 102 | Non-ST131, n = 741 | ||
| Gender, female | 55 (53.9) | 496 (66.9) | 0.01 |
| The elderly, ≥65 years | 78 (76.5) | 474 (64.0) | 0.01 |
| Nursing home residents | 13 (12.7) | 28 (3.8) | <0.001 |
| In vitro susceptibility | |||
| Cefazolin-S | 8 (7.8) | 380 (51.3) | <0.001 |
| Cefotaxime-S | 66 (64.7) | 678 (91.5) | <0.001 |
| Cefepime-S | 92 (90.2) | 727 (98.1) | <0.001 |
| Ertapenem-S | 98 (96.1) | 736 (99.3) | 0.02 |
| Levofloxacin-S | 64 (62.7) | 668 (90.1) | <0.001 |
| ESBL producers | 28 (27.5) | 20 (2.7) | <0.001 |
| Major comorbidity | |||
| Hypertension | 54 (52.9) | 389 (52.5) | 0.93 |
| Diabetes mellitus | 38 (37.3) | 277 (37.4) | 0.98 |
| Neurological disease | 29 (28.4) | 138 (18.6) | 0.02 |
| Malignancy | 28 (27.5) | 183 (24.7) | 0.55 |
| Coronary artery disease | 15 (14.7) | 70 (9.4) | 0.10 |
| Chronic kidney disease | 14 (13.7) | 109 (14.7) | 0.79 |
| Urological disorder | 14 (13.7) | 32 (4.3) | <0.001 |
| Liver cirrhosis | 13 (12.7) | 90 (12.1) | 0.86 |
| Major source of bacteremia | |||
| Urinary tract infection | 67 (65.7) | 460 (62.1) | 0.48 |
| Biliary tract infection | 12 (11.8) | 92 (12.4) | 0.85 |
| Intra-abdominal infection | 8 (7.8) | 95 (12.8) | 0.15 |
| Primary bacteremia | 7 (6.9) | 34 (4.6) | 0.32 |
| Pneumonia | 4 (3.9) | 34 (4.6) | 0.76 |
| Soft-tissue infection | 1 (1.0) | 11 (1.5) | 1.00 |
| Characteristics | Patients Number (%) | p-Values | |
|---|---|---|---|
| ST131, n = 102 | Non-ST131, n = 741 | ||
| Pitt bacteremia score ≥4 at onset | 15 (14.7) | 99 (13.4) | 0.71 |
| Initial sepsis-related syndrome | |||
| Severe sepsis | 36 (35.3) | 294 (39.7) | 0.40 |
| Septic shock | 14 (13.7) | 106 (14.3) | 0.88 |
| Comorbidity severity (McCabe classification) | 0.81 | ||
| Ultimately and rapidly fatal | 20 (19.6) | 138 (18.6) | |
| Nonfatal | 82 (80.4) | 603 (81.4) | |
| Length, day (mean ± standard deviation) | |||
| Time to appropriate antibiotic | 2.6 ± 6.1 | 0.8 ± 3.8 | 0.004 |
| Total hospital stays | 14.6 ± 17.1 | 11.1 ± 11.7 | 0.05 |
| Crude mortality rate | |||
| 14 days | 11 (10.8) | 32 (4.3) | 0.005 |
| 28 days | 15 (14.7) | 48 (6.5) | 0.003 |
| Susceptible to Indicated Drugs | Non-ESBL Producers | ESBL Producers | ||||
|---|---|---|---|---|---|---|
| ST131 n = 74 | Non-ST131 n = 721 | p-Values | ST131 n = 28 | Non-ST131 n = 20 | p-Values | |
| Cefazolin | 8 (10.8) | 380 (52.7) | <0.001 | 0 (0) | 0 (0) | - |
| Cefotaxime | 66 (89.2) | 678 (94.0) | 0.13 | 6 (21.4) | 4 (20.0) | 1.00 |
| Cefepime | 74 (100) | 719 (99.7) | 1.00 | 18 (63.4) | 8 (40.0) | 0.10 |
| Ertapenem | 71 (95.9) | 719 (99.7) | 0.007 | 27 (96.4) | 17 (85.0) | 0.29 |
| Levofloxacin | 63 (85.1) | 668 (96.2) | 0.02 | 1 (3.6) | 0 (0) | 1.00 |
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Values | Odds Ratio (95% CI) | p-Values | |
| Gender, female | 0.48 (0.29–0.81) | <0.001 | NS | NS |
| Nursing home residence | 6.98 (3.41–14.31) | 0.001 | 3.86 (1.32–11.31) | 0.01 |
| Fatal comorbidity (McCabe classification) | 5.76 (3.39–9.79) | <0.001 | 3.51 (1.63–7.58) | 0.001 |
| Inappropriate EAT | 3.31 (1.83–5.99) | <0.001 | 3.02 (1.20–7.59) | 0.02 |
| Pitt bacteremia score ≥4 at onset | 11.09 (6.41–19.20) | <0.001 | 17.95 (8.46–38.09) | <0.001 |
| Source of bacteremia | ||||
| Urinary tract infection | 0.25 (0.14–0.43) | <0.001 | NS | NS |
| Intra-abdominal infection | 2.46 (1.32–4.57) | 0.003 | 2.31 (0.98–5.48) | 0.06 |
| Primary bacteremia | 2.74 (1.16–6.47) | 0.03 | NS | NS |
| Pneumonia | 5.07 (2.34–10.99) | <0.001 | 4.55 (1.56–13.26) | 0.005 |
| Soft-tissue infection | 6.54 (1.91–22.36) | 0.009 | 12.38 (2.41–63.54) | 0.003 |
| Comorbidities | ||||
| Hypertension | 0.31 (0.17–0.55) | <0.001 | NS | NS |
| Diabetes mellitus | 0.55 (0.31–0.98) | 0.04 | NS | NS |
| Malignancy | 3.72 (2.21–6.27) | <0.001 | 2.00 (0.96–4.20) | 0.07 |
| Liver cirrhosis | 6.42 (3.69–11.16) | <0.001 | 4.51 (2.06–9.86) | <0.001 |
| Characteristics | Odds Ratio (95% CI) | ||||
|---|---|---|---|---|---|
| Non-ESBL Producers, n = 795 | ESBL Producers, n = 48 | ||||
| Univariate | Multivariate | Univariate | Multivariate | ||
| Gender, female | 0.59 (0.33–1.05) | – | 0.51 (0.13–1.94) | – | |
| The elderly, ≥65 years | 0.71 (0.40–1.27) | – | 1.13 (0.25–5.07) | – | |
| ST131 isolates | 1.12 (0.43–2.91) | 1.27 (0.37–4.41) | 2.22 (0.58–8.49) | 10.19 (1.02–101.39) | |
| Nursing home residence | 3.40 (1.11–10.42) | NS | 5.00 (1.32–18.95) | 7.09 (1.35–37.13) | |
| Comorbidities | |||||
| Liver cirrhosis | 7.75 (4.19–14.31) | 5.57 (2.49–12.46) | 1.87 (0.44–8.01) | – | |
| Malignancy | 3.95 (2.20–7.10) | 2.47 (1.11–5.49) | 1.83 (0.52–0.68) | – | |
| Chronic kidney disease | 1.18 (0.54–2.58) | – | 0.64 (0.12–3.56) | – | |
| Neurological disease | 0.58 (0.24–1.40) | – | 2.40 (0.67–6.48) | – | |
| Diabetes mellitus | 0.42 (0.20–0.84) | NS | 1.07 (0.30–3.78) | – | |
| Hypertension | 0.33 (0.17–0.62) | NS | 0.35 (0.08–1.47) | – | |
| Fatal comorbidity (McCabe classification) | 6.53 (3.60–11.86) | 4.20 (1.86–9.49) | 2.89 (0.75–11.11) | – | |
| Source of bacteremia | |||||
| Soft-tissue infection | 8.20 (2.38–28.26) | 8.52 (1.64–44.30) | – | – | |
| Pneumonia | 4.27 (1.76–10.35) | 4.14 (1.45–11.83) | 4.10 (2.44–6.84) | NS | |
| Primary bacteremia | 3.60 (1.50–8.62) | NS | 2.36 (0.14–40.40) | – | |
| Intra-abdominal infection | 3.03 (1.57–5.86) | NS | 2.54 (0.15–43.67) | – | |
| Biliary tract infection | 0.64 (0.23–1.82) | – | 0.64 (0.12–3.56) | – | |
| Urinary tract infection | 0.18 (0.09–0.35) | NS | 0.48 (0.13–1.77) | – | |
| Pitt bacteremia score ≥4 at onset | 11.75 (6.36–21.71) | 19.93 (8.89–44.64) | 10.33 (2.13–50.26) | 33.48 (2.92–383.93) | |
| Inappropriate empirical antibiotic therapy | 1.84 (0.79–4.27) | – | 2.00 (0.47–8.59) | – | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.-L.; Lee, C.-C.; Lee, C.-H.; Lee, N.-Y.; Hsieh, C.-C.; Hung, Y.-P.; Tang, H.-J.; Ko, W.-C. Clinical Impact of Sequence Type 131 in Adults with Community-Onset Monomicrobial Escherichia Coli Bacteremia. J. Clin. Med. 2018, 7, 508. https://doi.org/10.3390/jcm7120508
Wang J-L, Lee C-C, Lee C-H, Lee N-Y, Hsieh C-C, Hung Y-P, Tang H-J, Ko W-C. Clinical Impact of Sequence Type 131 in Adults with Community-Onset Monomicrobial Escherichia Coli Bacteremia. Journal of Clinical Medicine. 2018; 7(12):508. https://doi.org/10.3390/jcm7120508
Chicago/Turabian StyleWang, Jiun-Ling, Ching-Chi Lee, Chung-Hsun Lee, Nan-Yao Lee, Chih-Chia Hsieh, Yuan-Pin Hung, Hung-Jen Tang, and Wen-Chien Ko. 2018. "Clinical Impact of Sequence Type 131 in Adults with Community-Onset Monomicrobial Escherichia Coli Bacteremia" Journal of Clinical Medicine 7, no. 12: 508. https://doi.org/10.3390/jcm7120508