A Novel Machine Learning Algorithm to Automatically Predict Visual Outcomes in Intravitreal Ranibizumab-Treated Patients with Diabetic Macular Edema

Abstract
:1. Introduction
2. Patients and Methods
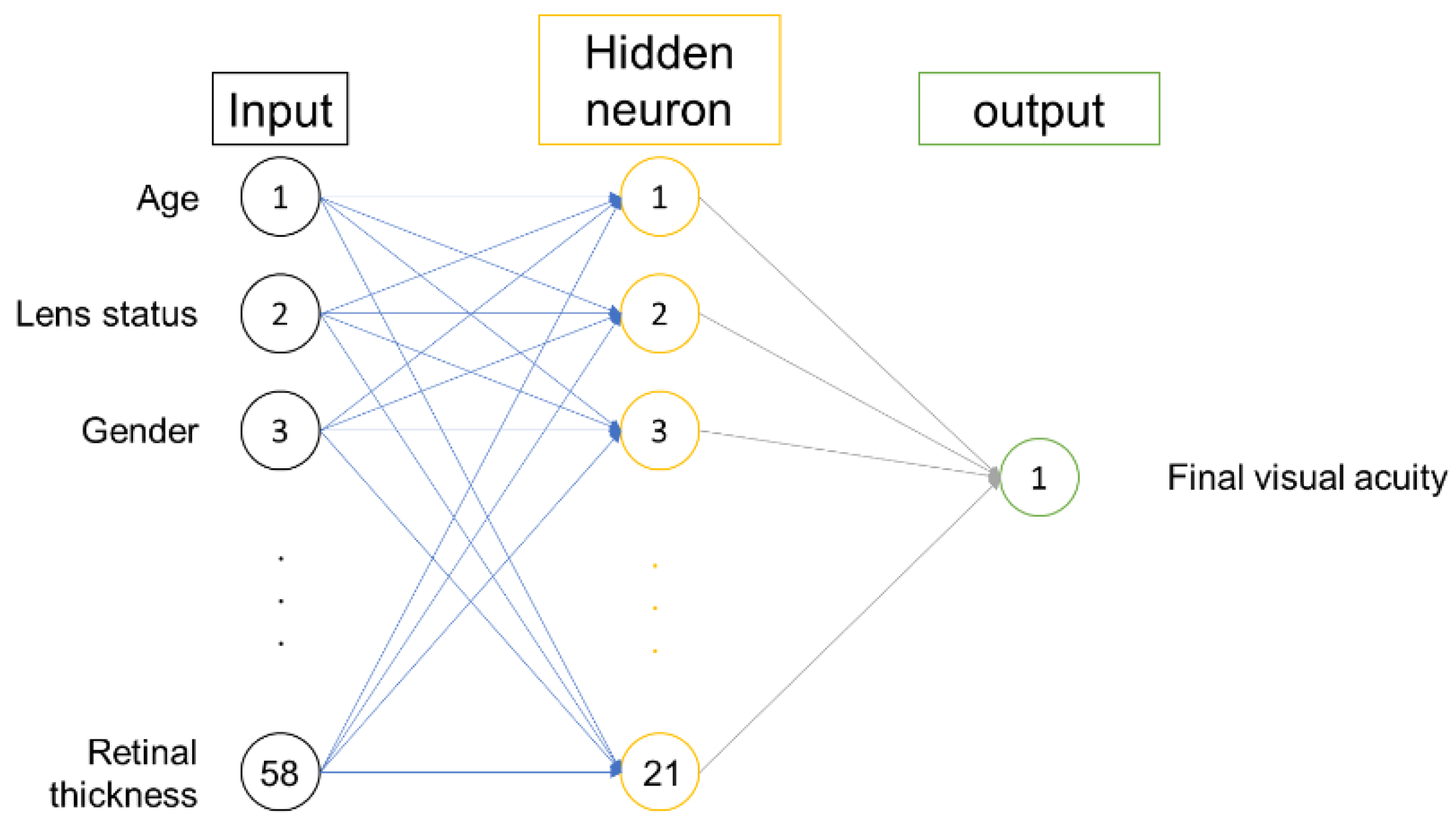
2.1. Prediction Model Input and Target Output
2.2. Machine Learning Development
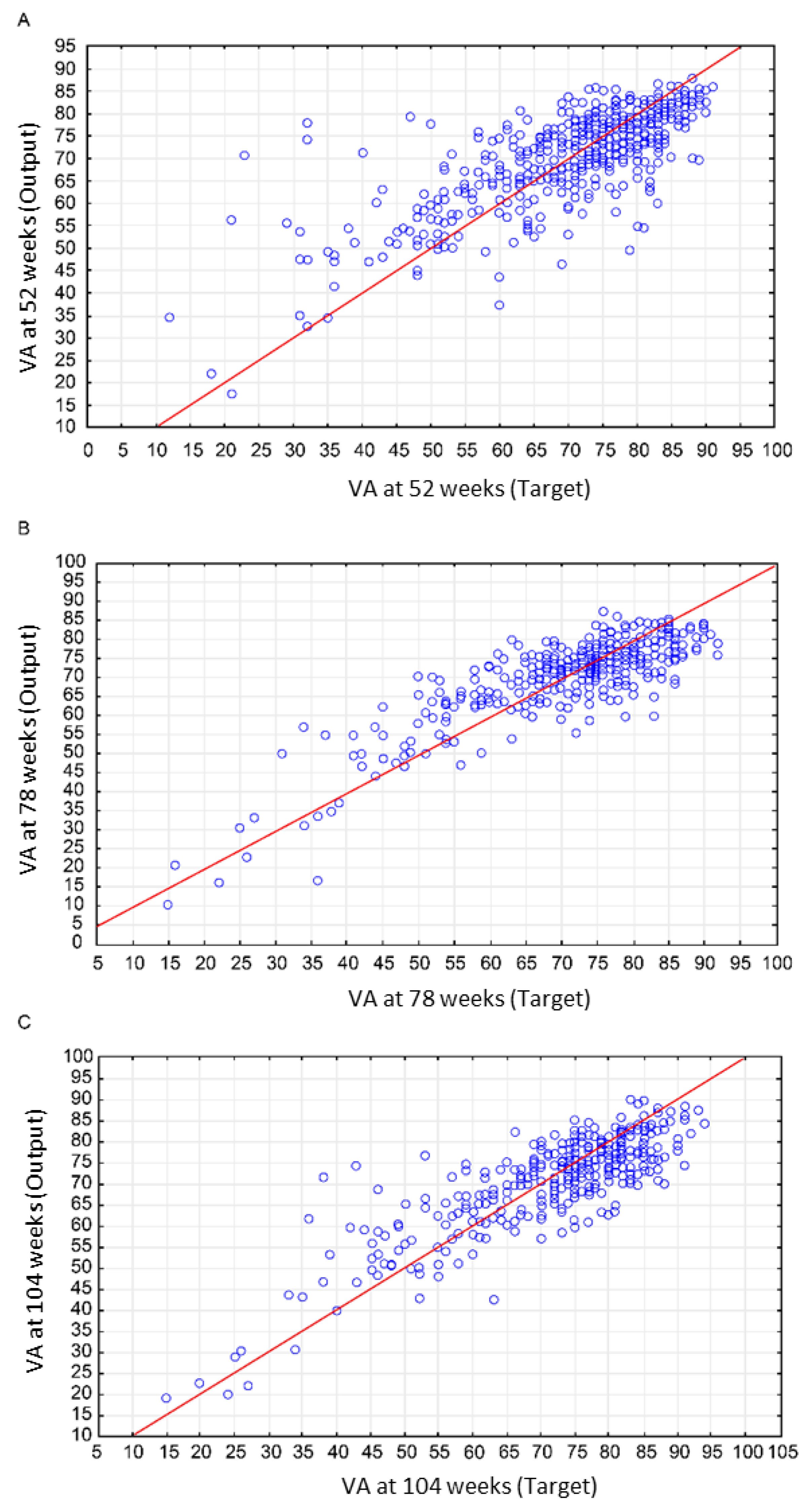
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pelletier, C.; Dai, S.; Roberts, K.C.; Bienek, A.; Onysko, J.; Pelletier, L. Report summary. Diabetes in Canada: Facts and figures from a public health perspective. Chronic Dis. Inj. Can. 2012, 33, 53–54. [Google Scholar] [PubMed]
- Varma, R.; Bressler, N.M.; Doan, Q.V.; Gleeson, M.; Danese, M.; Bower, J.K.; Selvin, E.; Dolan, C.; Fine, J.; Colman, S.; et al. Prevalence of and risk factors for diabetic macular edema in the United States. JAMA Ophthalmol. 2014, 132, 1334–1340. [Google Scholar] [CrossRef] [PubMed]
- Kiss, S.; Chandwani, H.S.; Cole, A.L.; Patel, V.D.; Lunacsek, O.E.; Dugel, P.U. Comorbidity and health care visit burden in working-age commercially insured patients with diabetic macular edema. Clin. Ophthalmol. 2016, 10, 2443–2453. [Google Scholar] [CrossRef] [PubMed]
- Aiello, L.P.; Avery, R.L.; Arrigg, P.G.; Keyt, B.A.; Jampel, H.D.; Shah, S.T.; Pasquale, L.R.; Thieme, H.; Iwamoto, M.A.; Park, J.E.; et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N. Engl. J. Med. 1994, 331, 1480–1487. [Google Scholar] [CrossRef] [PubMed]
- Antonetti, D.A.; Barber, A.J.; Hollinger, L.A.; Wolpert, E.B.; Gardner, T.W. Vascular endothelial growth factor induces rapid phosphorylation of tight junction proteins occludin and zonula occluden 1. A potential mechanism for vascular permeability in diabetic retinopathy and tumors. J. Biol. Chem. 1999, 274, 23463–23467. [Google Scholar] [CrossRef] [PubMed]
- Bressler, S.B.; Ayala, A.R.; Bressler, N.M.; Melia, M.; Qin, H.; Ferris, F.L.; Flaxel, C.J.; Friedman, S.M.; Glassman, A.R.; Jampol, L.M.; et al. Persistent macular thickening after ranibizumab treatment for diabetic macular edema with vision impairment. JAMA Ophthalmol. 2016, 134, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Bressler, S.B.; Glassman, A.R.; Almukhtar, T.; Melia, M.; Qin, H.; Ferris, F.L.; Flaxel, C.J.; Friedman, S.M.; Glassman, A.R.; Jampol, L.M.; et al. Five-year outcomes of ranibizumab with prompt or deferred laser versus laser or triamcinolone plus deferred ranibizumab for diabetic macular edema. Am. J. Ophthalmol. 2016, 164, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Bressler, S.B.; Melia, M.; Glassman, A.R.; Almukhtar, T.; Jampol, L.M.; Shami, M.; Berger, B.B.; Bressler, N.M. Diabetic Retinopathy Clinical Research Network. Ranibizumab plus prompt or deferred laser for diabetic macular edema in eyes with vitrectomy before anti-vascular endothelial growth factor therapy. Retina 2015, 35, 2516–2528. [Google Scholar] [CrossRef] [PubMed]
- Diabetic Retinopathy Clinical Research Network. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N. Engl. J. Med. 2015, 372, 1193–1203. [Google Scholar] [CrossRef] [PubMed]
- Mukkamala, L.; Bhagat, N.; Zarbin, M. Practical lessons from protocol T for the management of diabetic macular edema. Dev. Ophthalmol. 2017, 60, 109–124. [Google Scholar] [PubMed]
- Mukkamala, L.; Bhagat, N.; Zarbin, M.A. Practical lessons from protocol I for the management of diabetic macular edema. Dev. Ophthalmol. 2017, 60, 91–108. [Google Scholar] [PubMed]
- Kononenko, I. Machine learning for medical diagnosis: History, state of the art and perspective. Artif. Intell. Med. 2001, 23, 89–109. [Google Scholar] [CrossRef]
- Aikat, J.; Carsey, T.M.; Fecho, K.; Jeffay, K.; Krishnamurthy, A.; Mucha, P.J.; Rajasekar, A.; Ahalt, S.C. Scientific training in the era of big data: A New pedagogy for graduate education. Big Data 2017, 5, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Lek, S.; Aulagnier, S. Application of neural networks to modelling nonlinear relationships in ecology. Ecol. Model. 1996, 90, 39–52. [Google Scholar] [CrossRef]
- Mehdy, M.M.; Ng, P.Y.; Shair, E.F.; Saleh, N.I.M.; Gomes, C. Artificial neural networks in image processing for early detection of breast cancer. Comput. Math. Methods Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Valerio, M.S.; Graziella, R. An extreme learning machine approach to effective energy disaggregation. Electronics 2018, 7, 235. [Google Scholar]
- Siniscalchi, S.M.; Salerno, V.M. Adaptation to new microphones using artificial neural networks with trainable activation functions. IEEE Trans. Neural. Netw. Learn. Syst. 2016, 28, 1959–1965. [Google Scholar] [CrossRef] [PubMed]
- Siriyasatien, P.; Phumee, A.; Ongruk, P.; Jampachaisri, K.; Kesorn, K. Analysis of significant factors for dengue fever incidence prediction. BMC Bioinforma. 2016, 17, 166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehra, L.K.; Cowger, C.; Gross, K.; Ojiambo, P.S. Predicting pre-planting risk of stagonospora nodorum blotch in winter wheat using machine learning models. Front. Plant. Sci. 2016, 7, 390. [Google Scholar] [CrossRef] [PubMed]
- Giancardo, L.; Meriaudeau, F.; Karnowski, T.P.; Li, Y.; Garg, S.; Tobin, K.W., Jr.; Chaum, E. Exudate-based diabetic macular edema detection in fundus images using publicly available datasets. Med. Image Anal. 2012, 16, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Zhao, X.; Yang, Y.; Li, N. Learning-based visual saliency model for detecting diabetic macular edema in retinal image. Comput. Intell. Neurosci. 2016. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Feng, D.; Mi, H. Deep convolutional neural network-based early automated detection of diabetic retinopathy using fundus image. Molecules 2017, 22, 2054. [Google Scholar] [CrossRef] [PubMed]
- Bressler, S.B.; Qin, H.; Melia, M.; Bressler, N.M.; Beck, R.W.; Chan, C.K.; Grover, S.; Miller, D.G.; Diabetic Retinopathy Clinical Research Network. Exploratory analysis of the effect of intravitreal ranibizumab or triamcinolone on worsening of diabetic retinopathy in a randomized clinical trial. JAMA Ophthalmol. 2013, 131, 1033–1040. [Google Scholar] [CrossRef] [PubMed]
- Elman, M.J.; Qin, H.; Aiello, L.P.; Beck, R.W.; Bressler, N.M.; Ferris, F.L.; Glassman, A.R.; Maturi, R.K.; Melia, M. Intravitreal ranibizumab for diabetic macular edema with prompt versus deferred laser treatment: Three-year randomized trial results. Ophthalmology 2012, 119, 2312–2318. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhang, L.; Lian, G.; Zhan, R.; Xu, R.; Huang, Y.; Mitra, B.; Wu, J.; Luo, G. A novel mathematical model to predict prognosis of burnt patients based on logistic regression and support vector machine. Burns 2016, 42, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Qiu, X.; Shi, J.; Li, N.; Lu, Z.H.; Chen, P.; Yang, M.M.; Liu, F.Y.; Jia, W.J.; Zhang, Y. A pathological brain detection system based on extreme learning machine optimized by bat algorithm. CNS Neurol. Disord. Drug Targets 2017, 16, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.G.; Mukherjee, A.; Elmunzer, B.J.; Higgins, P.D.; Lok, A.S.; Zhu, J.; Marrero, J.A.; Waljee, A.K. Machine learning algorithms outperform conventional regression models in predicting development of hepatocellular carcinoma. Am. J. Gastroenterol. 2013, 108, 1723–1730. [Google Scholar] [CrossRef] [PubMed]
- Galatzer-Levy, I.R.; Karstoft, K.I.; Statnikov, A.; Shalev, A.Y. Quantitative forecasting of ptsd from early trauma responses: A machine learning application. J. Psychiatr. Res. 2014, 59, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Mori, Y.; Murakami, T.; Suzuma, K.; Ishihara, K.; Yoshitake, S.; Fujimoto, M.; Dodo, Y.; Yoshitake, T.; Miwa, Y.; Tsujikawa, A. Relation between macular morphology and treatment frequency during twelve months with ranibizumab for diabetic macular edema. PLoS ONE 2017, 12, e0175809. [Google Scholar] [CrossRef] [PubMed]
- Fursova, A.Z.; Chubar’, N.V.; Tarasov, M.S.; Saifullina, I.F.; Pustovaya, G.G. Clinical associations between photoreceptor status and visual outcomes in diabetic macular edema. Vestn. Oftalmol. 2017, 133, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Fursova, A.Z.; Chubar, N.V.; Tarasov, M.S.; Sayfullina, I.F.; Pustovaya, G.G. Effectiveness of diffuse diabetic macular edema treatment in relation to structural changes in macular region. Vestn. Oftalmol. 2016, 132, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Erfurth, U.; Lang, G.E.; Holz, F.G.; Schlingemann, R.O.; Lanzetta, P.; Massin, P.; Gerstner, O.; Bouazza, A.S.; Shen, H.; Osborne, A.; et al. Three-year outcomes of individualized ranibizumab treatment in patients with diabetic macular edema: The RESTORE extension study. Ophthalmology 2014, 121, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Anayol, M.A.; Sekeroglu, M.A.; Tirhis, H.; Gulpamuk, B.; Doguizi, S.; Yilmazbas, P. Objective evaluation of lens clarity after the intravitreal injection of sustained-release dexamethasone implant. J. Cataract. Refract. Surg. 2016, 42, 1477–1482. [Google Scholar] [CrossRef] [PubMed]
- Schmid, M.K.; Reich, O.; Faes, L.; Boehni, S.C.; Bittner, M.; Howell, J.P.; Thiel, M.A.; Signorell, A.; Bachmann, L.M. Comparison of outcomes and costs of ranibizumab and aflibercept treatment in real-life. PLoS ONE 2015, 10, e0135050. [Google Scholar] [CrossRef] [PubMed]
- Patrao, N.V.; Antao, S.; Egan, C.; Omar, A.; Hamilton, R.; Hykin, P.G.; Sivaprasad, S.; Rajendram, R.; Moorfields Diabetic Macular Edema Study Group. Real-world outcomes of ranibizumab treatment for diabetic macular edema in a United Kingdom National Health Service setting. Am. J. Ophthalmol. 2016, 172, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.Z.; Feng, K.; Lu, Y.; Qian, F.; Lu, X.R.; Zang, S.W.; Zhao, L. Predictors of short-term outcomes related to central subfield foveal thickness after intravitreal bevacizumab for macular edema due to central retinal vein occlusion. Int. J. Ophthalmol. 2016, 9, 86–92. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Characteristics | 52 Weeks | 78 Weeks | 104 Weeks |
|---|---|---|---|
| No. of study eyes | 512 | 483 | 464 |
| Sex, male No. (%) | 290 (56.6) | 272 (53.3) | 262 (56.5) |
| Age, mean (SD) (years) | 62.6 (9.5) | 62.5 (9.5) | 62.6 (9.5) |
| Diabetes | |||
| Type 2 No. (%) | 468 (91.4) | 442 (91.5) | 425 (91.6) |
| HbA1c level, (SD) | 7.67 (1.55) | 7.66 (1.52) | 7.66 (1.55) |
| Insulin using No. (%) | 308 (60.2) | 291 (60.2) | 278 (59.9) |
| Comorbidities under treatment, No. (%) | |||
| Hypertension | 404 (78.9) | 383 (79.3) | 367 (79.1) |
| Hyper cholesterol | 350 (68.4) | 333 (68.9) | 320 (69.0) |
| Lens status, pseudophakic No. (%) | 154 (30.1) | 149 (30.8) | 139 (30.0) |
| Diabetic retinopathy severity, No. (%) | |||
| Microaneurysms only | 16 (3.1) | 15 (3.1) | 15 (3.2) |
| Mild/moderate NPDR | 266 (52.0) | 250 (51.8) | 241 (51.9) |
| Severe NPDR | 105 (20.5) | 96 (19.9) | 93 (20.0) |
| PDR and/or prior scatter | 123 (24.0) | 120 (24.8) | 113 (24.4) |
| Visual acuity with ETDRS letter, mean (SD) | |||
| Baseline | 63.6 (12.5) | 63.2 (12.4) | 63.2 (12.4) |
| Final | 70.4 (13.5) | 70.2 (13.5) | 70.6 (13.9) |
| Intra-vitreous injection No. (SD) | 8.1 (2.7) | 10.2 (4.2) | 11.7 (5.5) |
| Retina thickness of grid (um) (SD) | |||
| Center Point | 391.6 (135.9) | 394.8 (136.5) | 396.7 (138.1) |
| Center subfield | 392.7 (122.6) | 395.4 (123.6) | 397.3 (125.0) |
| Inner/outer subfield | |||
| Superior | 358.2 (92.0)/291.6 (72.0) | 359.9 (93.4)/292.3 (72.3) | 360.8 (94.2)/292.6 (73.1) |
| Nasal | 359.8 (92.2)/299.5 (66.9) | 361.2 (93.5)/300.0 (67.0) | 362.3 (94.4)/300.4 (67.7) |
| Inferior | 364.4 (102.7)/286.6 (77.1) | 365.6 (104.3)/287.3 (78.3) | 366.5 (105.2)/287.3 (78.6) |
| Temporal | 368.0 (104.1)/289.1 (82.7) | 370.0 (105.9)/290.3 (84.4) | 370.7 (106.7)/290.1 (84.6) |
| Weeks | Net Name | Correlation Coefficients | Mean Standard Error (ETDRS Letters) | ||||
|---|---|---|---|---|---|---|---|
| Train Group | Test Group | Validation Group | Train Group | Test Group | Validation Group | ||
| 52 | MLP 58-21-1 | 0.75 | 0.77 | 0.70 | 6.50 | 6.11 | 6.40 |
| 78 | MLP 72-48-1 | 0.79 | 0.80 | 0.55 | 5.91 | 5.83 | 7.59 |
| 104 | MLP 84-21-1 | 0.83 | 0.47 | 0.81 | 5.39 | 8.70 | 6.81 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.-C.; Chiu, H.-W.; Chen, C.-C.; Woung, L.-C.; Lo, C.-M. A Novel Machine Learning Algorithm to Automatically Predict Visual Outcomes in Intravitreal Ranibizumab-Treated Patients with Diabetic Macular Edema. J. Clin. Med. 2018, 7, 475. https://doi.org/10.3390/jcm7120475
Chen S-C, Chiu H-W, Chen C-C, Woung L-C, Lo C-M. A Novel Machine Learning Algorithm to Automatically Predict Visual Outcomes in Intravitreal Ranibizumab-Treated Patients with Diabetic Macular Edema. Journal of Clinical Medicine. 2018; 7(12):475. https://doi.org/10.3390/jcm7120475
Chicago/Turabian StyleChen, Shao-Chun, Hung-Wen Chiu, Chun-Chen Chen, Lin-Chung Woung, and Chung-Ming Lo. 2018. "A Novel Machine Learning Algorithm to Automatically Predict Visual Outcomes in Intravitreal Ranibizumab-Treated Patients with Diabetic Macular Edema" Journal of Clinical Medicine 7, no. 12: 475. https://doi.org/10.3390/jcm7120475