Predictions of Preterm Birth from Early Pregnancy Characteristics: Born in Guangzhou Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Predictors
2.3. Outcomes
2.4. Model Development
2.5. Selection of Prediction Models for External Validation
3. Results
3.1. Characteristics of Participants
3.2. Discrimination of Models for Overall PTB
3.3. Discrimination of Models for Spontaneous and Iatrogenic PTB
3.4. Discrimination of Models for Late and Early PTB
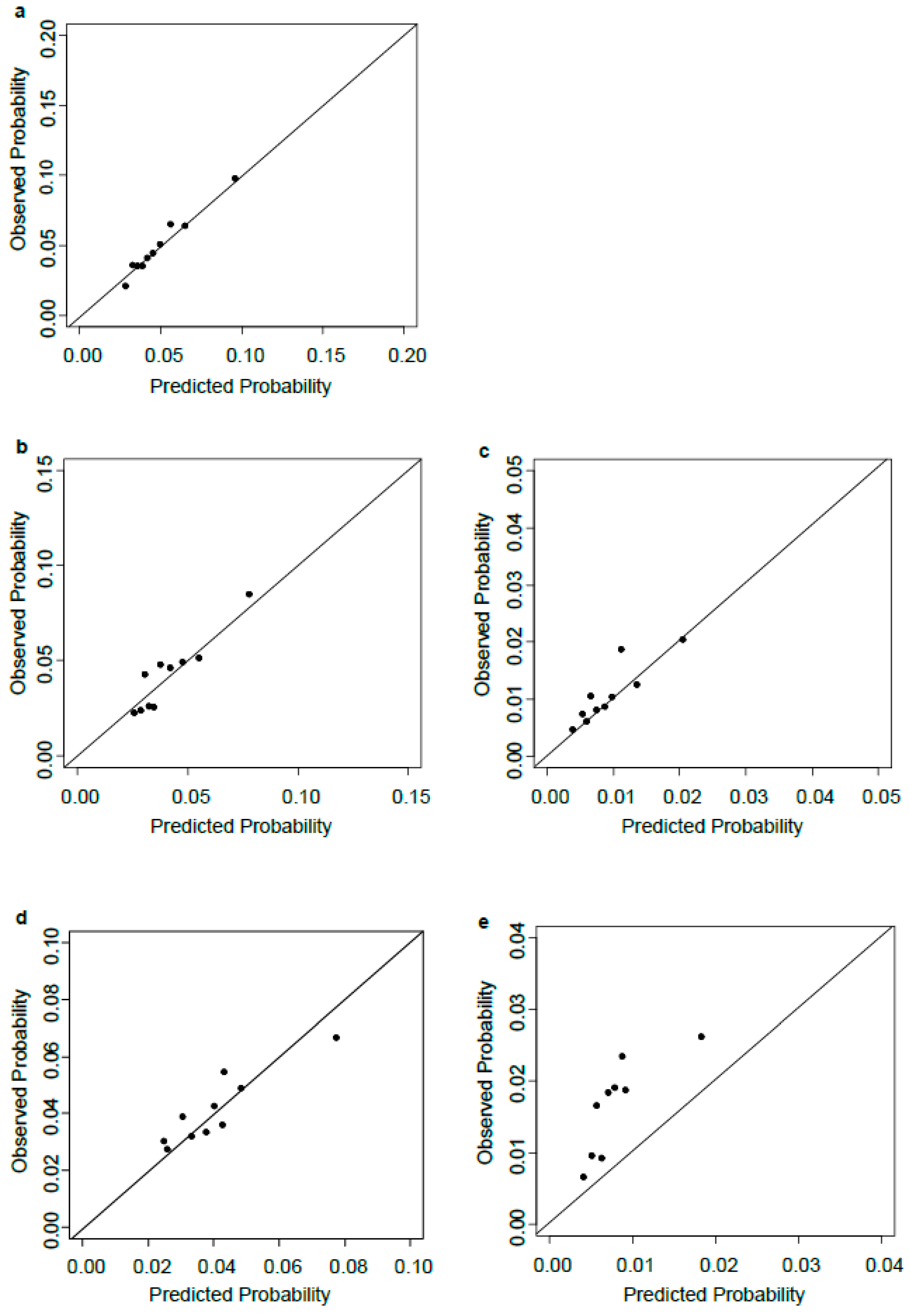
3.5. Calibration Plots
3.6. Models Stratified by Parity
3.7. External Validation for Published Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lawn, J.E.; Kinney, M. Preterm birth: Now the leading cause of child death worldwide. Sci. Transl. Med. 2014, 6, 263ed21. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Oza, S.; Hogan, D.; Perin, J.; Rudan, I.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: An updated systematic analysis. Lancet 2015, 385, 430–440. [Google Scholar] [CrossRef]
- Saigal, S.; Doyle, L.W. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 2008, 371, 261–269. [Google Scholar] [CrossRef]
- Kleinrouweler, C.E.; Cheong-See, F.M.; Collins, G.S.; Kwee, A.; Thangaratinam, S.; Khan, K.S.; Mol, B.W.J.; Pajkrt, E.; Moons, K.G.M.; Schuit, E. Prognostic models in obstetrics: Available, but far from applicable. Am. J. Obstet. Gynecol. 2016, 214, 79–90.e36. [Google Scholar] [CrossRef] [PubMed]
- Sananes, N.; Langer, B.; Gaudineau, A.; Kutnahorsky, R.; Aissi, G.; Fritz, G.; Viville, B.; Nisand, I.; Favre, R. Prediction of spontaneous preterm delivery in singleton pregnancies: Where are we and where are we going? A review of literature. J. Obstet. Gynaecol. 2014, 34, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Catley, C.; Frize, M.; Walker, C.R.; Petriu, D.C. Predicting high-risk preterm birth using artificial neural networks. IEEE Trans. Inf. Technol. Biomed. 2006, 10, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Raglan, G.B.; Lannon, S.M.; Jones, K.M.; Schulkin, J. Racial and Ethnic Disparities in Preterm Birth Among American Indian and Alaska Native Women. Matern. Child Health J. 2016, 20, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Culhane, J.F.; Goldenberg, R.L. Racial disparities in preterm birth. Semin. Perinatol. 2011, 35, 234–239. [Google Scholar] [CrossRef] [PubMed]
- York, T.P.; Strauss, J.F., III; Neale, M.C.; Eaves, L.J. Racial differences in genetic and environmental risk to preterm birth. PLoS ONE 2010, 5, e12391. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, X.; Ruan, Y.; Li, G.; Chen, Y.; Zhang, W. Preterm birth and neonatal mortality in China in 2011. Int. J. Gynaecol. Obstet. 2014, 127, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Tan, H.; Zhou, S.; He, Y.; Shen, L.; Liu, Y.; Hu, L.; Wang, X.; Li, X. Study on the application of Back-Propagation Artificial Neural Network used the model in predicting preterm birth. Zhonghua Liu Xing Bing Xue Za Zhi 2014, 35, 1028–1031. [Google Scholar] [PubMed]
- Leung, T.N.; Pang, M.W.; Leung, T.Y.; Poon, C.F.; Wong, S.M.; Lau, T.K. Cervical length at 18–22 weeks of gestation for prediction of spontaneous preterm delivery in Hong Kong Chinese women. Ultrasound Obstet. Gynecol. 2005, 26, 713–717. [Google Scholar] [CrossRef] [PubMed]
- He, J.R.; Yuan, M.Y.; Chen, N.N.; Lu, J.H.; Hu, C.Y.; Mai, W.B.; Zhang, R.; Pan, Y.; Qiu, L.; Wu, Y.; et al. Maternal dietary patterns and gestational diabetes mellitus: A large prospective cohort study in China. Br. J. Nutr. 2015, 113, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Qiu, X.; Lu, J.H.; He, J.R.; Lam, K.H.; Shen, S.Y.; Guo, Y.; Kuang, Y.S.; Yuan, M.Y.; Qiu, L.; Chen, N.N.; et al. The Born in Guangzhou Cohort Study (BIGCS). Eur. J. Epidemiol. 2017, 32, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Zung, W.W. A Self-Rating Depression Scale. Arch. Gen. Psychiatry 1965, 12, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Zung, W.W. A rating instrument for anxiety disorders. Psychosomatics 1971, 12, 371–379. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Newson, R.B. Comparing the predictive powers of survival models using Harrell’s C or Somers’ D. Stata J. 2010, 10, 339. [Google Scholar]
- Schuit, E.; Amer-Wahlin, I.; Groenwold, R.H.; Mol, B.W.; Moons, K.G.; Kwee, A. Prediction of neonatal metabolic acidosis in women with a singleton term pregnancy in cephalic presentation: An external validation study. Am. J. Perinatol. 2012, 29, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Demler, O.V.; Paynter, N.P.; Cook, N.R. Tests of calibration and goodness-of-fit in the survival setting. Stat. Med. 2015, 34, 1659–1680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, W.; Huning, E.Y.; Tran, T.; Phung, D.; Venkatesh, S. Screening for post 32-week preterm birth risk: How helpful is routine perinatal data collection? Heliyon 2016, 2, e00119. [Google Scholar] [CrossRef] [PubMed]
- Sananes, N.; Meyer, N.; Gaudineau, A.; Aissi, G.; Boudier, E.; Fritz, G.; Viville, B.; Nisand, I.; Langer, B.; Favre, R. Prediction of spontaneous preterm delivery in the first trimester of pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 171, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Beta, J.; Akolekar, R.; Ventura, W.; Syngelaki, A.; Nicolaides, K.H. Prediction of spontaneous preterm delivery from maternal factors, obstetric history and placental perfusion and function at 11–13 weeks. Prenat. Diagn. 2011, 31, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Parra-Cordero, M.; Sepulveda-Martinez, A.; Rencoret, G.; Valdes, E.; Pedraza, D.; Munoz, H. Is there a role for cervical assessment and uterine artery Doppler in the first trimester of pregnancy as a screening test for spontaneous preterm delivery? Ultrasound Obstet. Gynecol. 2014, 43, 291–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaaf, J.M.; Ravelli, A.C.; Mol, B.W.; Abu-Hanna, A. Development of a prognostic model for predicting spontaneous singleton preterm birth. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 164, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Meertens, L.J.; van Montfort, P.; Scheepers, H.C.; van Kuijk, S.M.; Aardenburg, R.; Langenveld, J.; van Dooren, I.M.A.; Zwaan, I.M.; Spaanderman, M.E.A.; Smits, L.J.M. Prediction models for the risk of spontaneous preterm birth based on maternal characteristics: A systematic review and independent external validation. Acta Obstet. Gynecol. Scand. 2018. [Google Scholar] [CrossRef] [PubMed]
- Jayaram, A.; Kanninen, T.; Sisti, G.; Inglis, S.R.; Morgan, N.; Witkin, S.S. Pregnancy History Influences the Level of Autophagy in Peripheral Blood Mononuclear Cells From Pregnant Women. Reprod. Sci. 2017. [Google Scholar] [CrossRef] [PubMed]
- Morken, N.H.; Kallen, K.; Jacobsson, B. Predicting risk of spontaneous preterm delivery in women with a singleton pregnancy. Paediatr. Perinat. Epidemiol. 2014, 28, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Kazemier, B.M.; Buijs, P.E.; Mignini, L.; Limpens, J.; de Groot, C.J.; Mol, B.W. Impact of obstetric history on the risk of spontaneous preterm birth in singleton and multiple pregnancies: a systematic review. BJOG 2014, 121, 1197–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iams, J.D.; Goldenberg, R.L.; Mercer, B.M.; Moawad, A.H.; Meis, P.J.; Das, A.F.; Caritis, S.N.; Miodovnik, M.; Menard, M.K.; Thurnau, G.R.; et al. The preterm prediction study: can low-risk women destined for spontaneous preterm birth be identified? Am. J. Obstet. Gynecol. 2001, 184, 652–655. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Predictors | HR (95% CI) | ||
|---|---|---|---|
| Model 1 1 | Model 2 2 | Model 3 3 | |
| Models for all PTB | |||
| Age (per year increase) | 1.06 (1.03–1.08) | 1.05 (1.02–1.08) | 1.05 (1.02–1.08) |
| Height (per cm increase) | 0.98 (0.96–1.00) | 0.98 (0.96–1.00) | 0.98 (0.96–1.00) |
| History of preterm delivery | |||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Yes | 3.97 (2.31–6.83) | 4.01 (2.36–6.81) | 3.95 (2.33–6.68) |
| Amount of vaginal-bleeding | |||
| Never | 1.00 (reference) | 1.00 (reference) | |
| Mild | 1.66 (1.35–2.05) | 1.66 (1.34–2.04) | |
| Moderate or severe | 1.46 (1.00–2.13) | 1.47 (1.00–2.14) | |
| Folic acid intake before pregnancy | |||
| Never | 1.00 (reference) | ||
| Ever | 0.78 (0.64–0.95) | ||
| Models for spontaneous PTB | |||
| Age (per year increase) | 1.05 (1.02–1.08) | 1.05 (1.02–1.08) | 1.05 (1.02–1.08) |
| History of preterm delivery | |||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Yes | 4.09 (2.42–6.91) | 4.06 (2.42–6.81) | 4.00 (2.39–6.72) |
| Amount of vaginal-bleeding | |||
| Never | 1.00 (reference) | 1.00 (reference) | |
| Mild | 1.64 (1.31–2.07) | 1.64 (1.30–2.06) | |
| Moderate or severe | 1.71 (1.15–2.52) | 1.71 (1.16–2.53) | |
| Folic acid intake before pregnancy | |||
| Never | 1.00 (reference) | ||
| Ever | 0.79 (0.63–0.98) | ||
| Models for iatrogenic PTB | |||
| Age (per year increase) | 1.09 (1.02–1.16) | 1.09 (1.02–1.16) | 1.09 (1.02–1.17) |
| Amount of vaginal-bleeding | |||
| Never | 1.00 (reference) | 1.00 (reference) | |
| Mild | 1.69 (1.05–2.72) | 1.69 (1.05–2.70) | |
| Moderate or severe | 0.41 (0.06–2.78) | 0.41 (0.06–2.74) | |
| Passive smoking during pregnancy | |||
| Never | 1.00 (reference) | ||
| Ever | 1.75 (1.09–2.83) | ||
| Predictors | HR (95% CI) | ||
|---|---|---|---|
| Model 1 1 | Model 2 2 | Model 3 3 | |
| Models for PTB at 34–36 weeks | |||
| Age (per year increase) | 1.05 (1.02–1.08) | 1.05 (1.02–1.08) | 1.05 (1.02–1.08) |
| History of preterm delivery | |||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Yes | 2.81 (1.36–5.82) | 2.82 (1.34–5.94) | 2.82 (1.34–5.94) |
| Amount of vaginal-bleeding | |||
| Never | 1.00 (reference) | 1.00 (reference) | |
| Mild | 1.65 (1.32–2.06) | 1.65 (1.32–2.06) | |
| Moderate or severe | 1.44 (0.95–2.18) | 1.44 (0.95–2.18) | |
| Model for PTB at <34 weeks | |||
| Nulliparous women | |||
| Age (per year increase) | 1.12 (1.04–1.20) | 1.12 (1.04–1.20) | 1.08 (1.01–1.16) |
| Multiparous women | |||
| History of preterm delivery | |||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Yes | 6.25 (2.06–19.0) | 6.25 (2.06–19.0) | 6.25 (2.06–19.0) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, J.-R.; Ramakrishnan, R.; Lai, Y.-M.; Li, W.-D.; Zhao, X.; Hu, Y.; Chen, N.-N.; Hu, F.; Lu, J.-H.; Wei, X.-L.; et al. Predictions of Preterm Birth from Early Pregnancy Characteristics: Born in Guangzhou Cohort Study. J. Clin. Med. 2018, 7, 185. https://doi.org/10.3390/jcm7080185
He J-R, Ramakrishnan R, Lai Y-M, Li W-D, Zhao X, Hu Y, Chen N-N, Hu F, Lu J-H, Wei X-L, et al. Predictions of Preterm Birth from Early Pregnancy Characteristics: Born in Guangzhou Cohort Study. Journal of Clinical Medicine. 2018; 7(8):185. https://doi.org/10.3390/jcm7080185
Chicago/Turabian StyleHe, Jian-Rong, Rema Ramakrishnan, Yu-Mian Lai, Wei-Dong Li, Xuan Zhao, Yan Hu, Nian-Nian Chen, Fang Hu, Jin-Hua Lu, Xue-Ling Wei, and et al. 2018. "Predictions of Preterm Birth from Early Pregnancy Characteristics: Born in Guangzhou Cohort Study" Journal of Clinical Medicine 7, no. 8: 185. https://doi.org/10.3390/jcm7080185