
The Surgical Histopathology of the Filum Terminale: Findings from a Large Series of Patients with Tethered Cord Syndrome

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Results
3.2. Case Illustrations
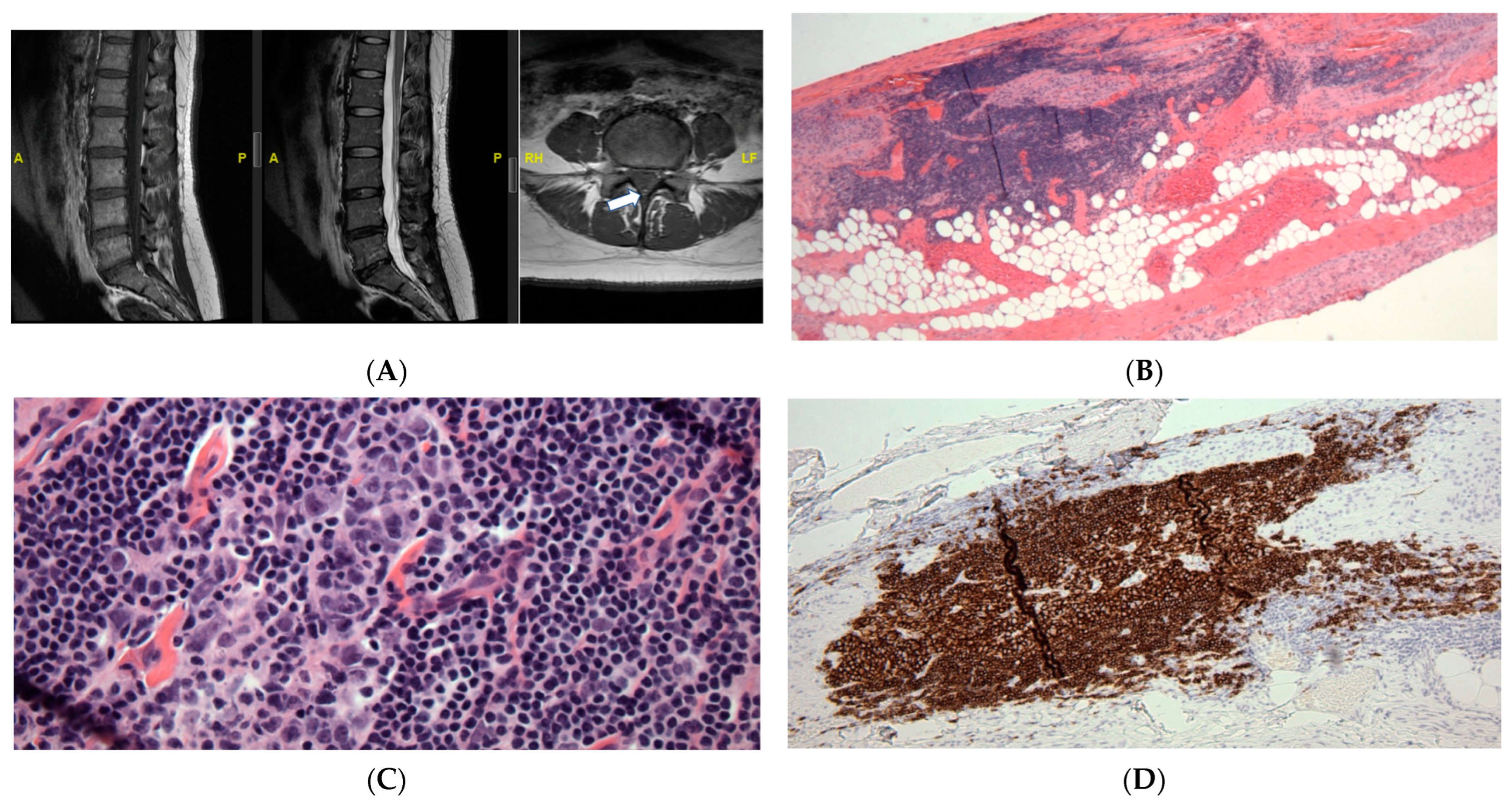
3.2.1. Case #1: Lymphoid Proliferation Suggestive of a Secondary Lymph Follicle
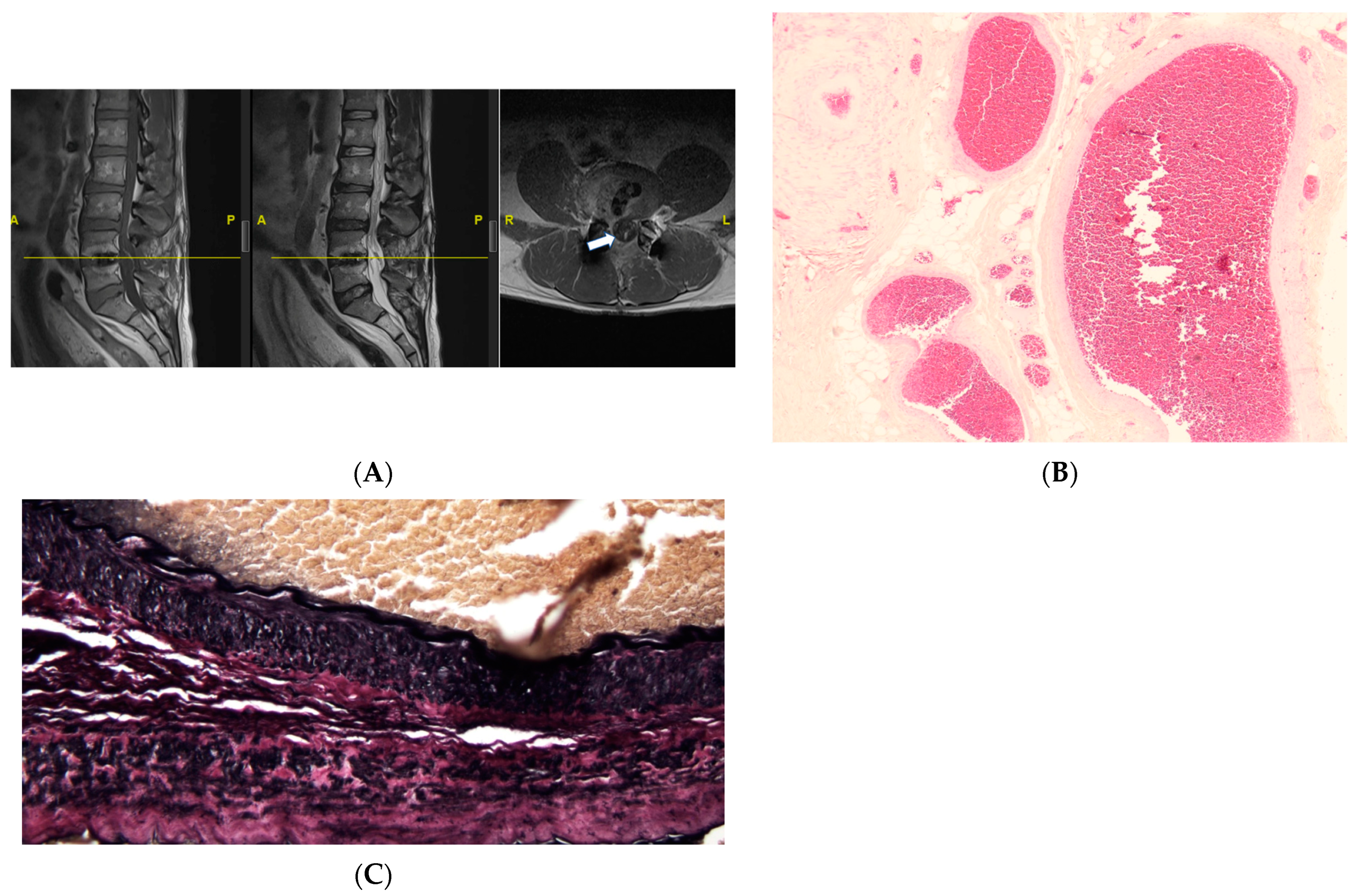
3.2.2. Case #2: Vascularity
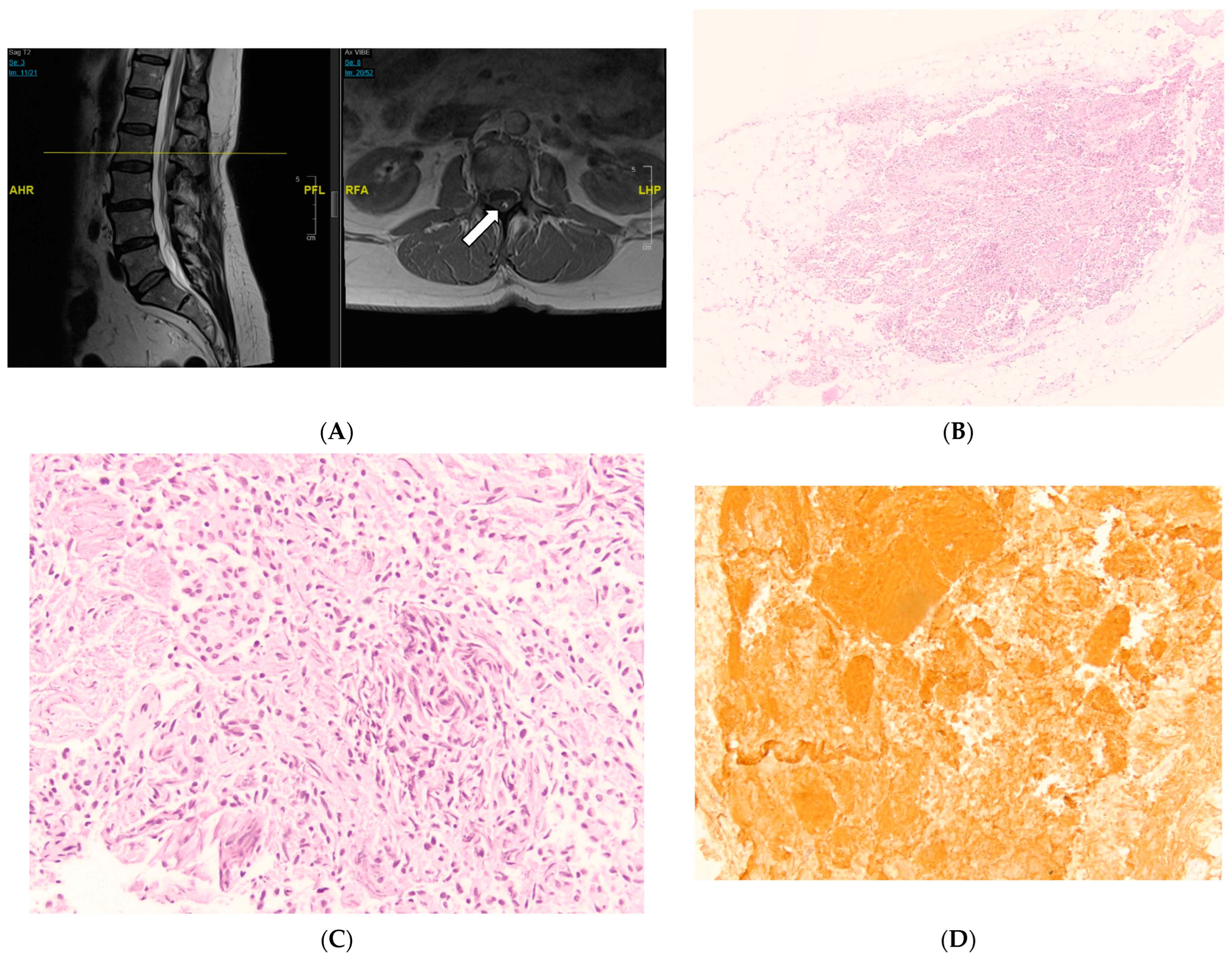
3.2.3. Case #3: Ependymal Cell Proliferation
3.2.4. Case #4: Focal Calcifications
4. Discussion
4.1. The Implication of Peripheral Nerves and Fat within the FT
4.2. Ependymal Proliferation and Vascularity within the FT
4.3. Inflammatory Cells and Calcifications
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pinto, F.C.G.; Fontes, R.B.d.V.; Leonhardt, M.d.C.; Amodio, D.T.; Porro, F.F.; Machado, J. Anatomic Study of the Filum Terminale and Its Correlations with the Tethered Cord Syndrome. Neurosurgery 2002, 51, 725–729. [Google Scholar] [CrossRef] [PubMed]
- De Vloo, P.; Monea, A.G.; Sciot, R.; van Loon, J.; Van Calenbergh, F. The Filum Terminale: A Cadaver Study of Anatomy, Histology, and Elastic Properties. World Neurosurg. 2016, 90, 565–573.e1. [Google Scholar] [CrossRef] [PubMed]
- Nasr, A.Y.; Hussein, A.M.; Zaghloul, S.A. Morphometric Parameters and Histological Study of the Filum Terminale of Adult Human Cadavers and Magnetic Resonance Images. Folia Morphol. 2018, 77, 609–619. [Google Scholar] [CrossRef]
- Klinge, P.M.; Srivastava, V.; McElroy, A.; Leary, O.P.; Ahmed, Z.; Donahue, J.E.; Brinker, T.; De Vloo, P.; Gokaslan, Z.L. Diseased Filum Terminale as a Cause of Tethered Cord Syndrome in Ehlers-Danlos Syndrome: Histopathology, Biomechanics, Clinical Presentation, and Outcome of Filum Excision. World Neurosurg. 2022, 162, e492–e502. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, K.P.; Smitherman, A.D.; Milton, C.K.; Palejwala, A.H.; Lu, V.M.; Johnston, S.E.; Homburg, H.; Zhao, D.; Martin, M.D. Surgical Treatment of Tethered Cord Syndrome in Adults: A Systematic Review and Meta-Analysis. World Neurosurg. 2020, 137, e221–e241. [Google Scholar] [CrossRef] [PubMed]
- Leary, O.P.; Hagan, M.; Sullivan, P.L.Z.; McElroy, A.; Syed, S.; Liu, D.D.; Donahue, J.E.; Scarfo, K.-A.; Carayannopoulos, A.G.; Li, J.; et al. Adult-Onset Tethered Cord Syndrome: Case Series from a Comprehensive Interdisciplinary Spine Center. Interdiscip. Neurosurg. 2023, 33, 101773. [Google Scholar] [CrossRef]
- Liu, F.-Y.; Li, J.-F.; Guan, X.; Luo, X.-F.; Wang, Z.-L.; Dang, Q.-H. SEM Study on Filum Terminale with Tethered Cord Syndrome. Childs Nerv. Syst. ChNS Off. J. Int. Soc. Pediatr. Neurosurg. 2011, 27, 2141–2144. [Google Scholar] [CrossRef]
- Klinge, P.M.; McElroy, A.; Leary, O.P.; Donahue, J.E.; Mumford, A.; Brinker, T.; Gokaslan, Z.L. Not Just an Anchor: The Human Filum Terminale Contains Stretch Sensitive and Nociceptive Nerve Endings and Responds to Electrical Stimulation with Paraspinal Muscle Activation. Neurosurgery 2022, 91, 618–624. [Google Scholar] [CrossRef]
- Gupta, P.; Kumar, A.; Kumar, A.; Goel, S. Congenital Spinal Cord Anomalies: A Pictorial Review. Curr. Probl. Diagn. Radiol. 2013, 42, 57–66. [Google Scholar] [CrossRef]
- Selçuki, M.; Vatansever, S.; Inan, S.; Erdemli, E.; Bağdatoğlu, C.; Polat, A. Is a Filum Terminale with a Normal Appearance Really Normal? Childs Nerv. Syst. ChNS Off. J. Int. Soc. Pediatr. Neurosurg. 2003, 19, 3–10. [Google Scholar] [CrossRef]
- Harmeier, J.W. The Normal Histology of the Intradural Filum Terminale. Arch. Neurol. Psychiatry 1933, 29, 308–316. [Google Scholar] [CrossRef]
- Pang, D.; Zovickian, J.; Moes, G.S. Retained Medullary Cord in Humans: Late Arrest of Secondary Neurulation. Neurosurgery 2011, 68, 1500–1519. [Google Scholar] [CrossRef] [PubMed]
- Agarwalla, P.K.; Dunn, I.F.; Scott, R.M.; Smith, E.R. Tethered Cord Syndrome. Neurosurg. Clin. N. Am. 2007, 18, 531–547. [Google Scholar] [CrossRef] [PubMed]
- Jones, V.; Wykes, V.; Cohen, N.; Thompson, D.; Jacques, T.S. The Pathology of Lumbosacral Lipomas: Macroscopic and Microscopic Disparity Have Implications for Embryogenesis and Mode of Clinical Deterioration. Histopathology 2018, 72, 1136–1144. [Google Scholar] [CrossRef] [PubMed]
- Cools, M.J.; Al-Holou, W.N.; Stetler, W.R.J.; Wilson, T.J.; Muraszko, K.M.; Ibrahim, M.; La Marca, F.; Garton, H.J.L.; Maher, C.O. Filum Terminale Lipomas: Imaging Prevalence, Natural History, and Conus Position. J. Neurosurg. Pediatr. 2014, 13, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Kural, C.; Guresci, S.; Simsek, G.G.; Arslan, E.; Tehli, O.; Solmaz, I.; Izci, Y. Histological Structure of Filum Terminale in Human Fetuses. J. Neurosurg. Pediatr. 2014, 13, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Fontes, R.B.V.; Saad, F.; Soares, M.S.; de Oliveira, F.; Pinto, F.C.G.; Liberti, E.A. Ultrastructural Study of the Filum Terminale and Its Elastic Fibers. Neurosurgery 2006, 58, 978–984. [Google Scholar] [CrossRef]
- Yamada, S.; Knerium, D.S.; Mandybur, G.M.; Schultz, R.L.; Yamada, B.S. Pathophysiology of Tethered Cord Syndrome and Other Complex Factors. Neurol. Res. 2004, 26, 722–726. [Google Scholar] [CrossRef]
- Thompson, E.M.; Strong, M.J.; Warren, G.; Woltjer, R.L.; Selden, N.R. Clinical Significance of Imaging and Histological Characteristics of Filum Terminale in Tethered Cord Syndrome. J. Neurosurg. Pediatr. 2014, 13, 255–259. [Google Scholar] [CrossRef]
- McElroy, A.; Rashmir, A.; Manfredi, J.; Sledge, D.; Carr, E.; Stopa, E.; Klinge, P. Evaluation of the Structure of Myodural Bridges in an Equine Model of Ehlers-Danlos Syndromes. Sci. Rep. 2019, 9, 9978. [Google Scholar] [CrossRef]
- Abdulrazeq, H.; Shao, B.; Sastry, R.A.; Klinge, P.M. Microsurgical Approach for Resection of the Filum Terminale Internum in Tethered Cord Syndrome-a Case Demonstration of Technical Nuances and Vignettes. Acta Neurochir. 2023, 165, 3505–3509. [Google Scholar] [CrossRef] [PubMed]
- Durdağ, E.; Börcek, P.B.; Öcal, Ö.; Börcek, A.Ö.; Emmez, H.; Baykaner, M.K. Pathological Evaluation of the Filum Terminale Tissue after Surgical Excision. Childs Nerv. Syst. ChNS Off. J. Int. Soc. Pediatr. Neurosurg. 2015, 31, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Rafiee, F.; Mehan, W.A.; Rincon, S.; Rohatgi, S.; Rapalino, O.; Buch, K. Diagnostic Utility of 3D Gradient-Echo MR Imaging Sequences through the Filum Compared with Spin-Echo T1 in Children with Concern for Tethered Cord. Am. J. Neuroradiol. 2023, 44, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Selden, N.R.; Nixon, R.R.; Skoog, S.R.; Lashley, D.B. Minimal Tethered Cord Syndrome Associated with Thickening of the Terminal Filum. J. Neurosurg. 2006, 105, 214–218. [Google Scholar] [CrossRef] [PubMed]
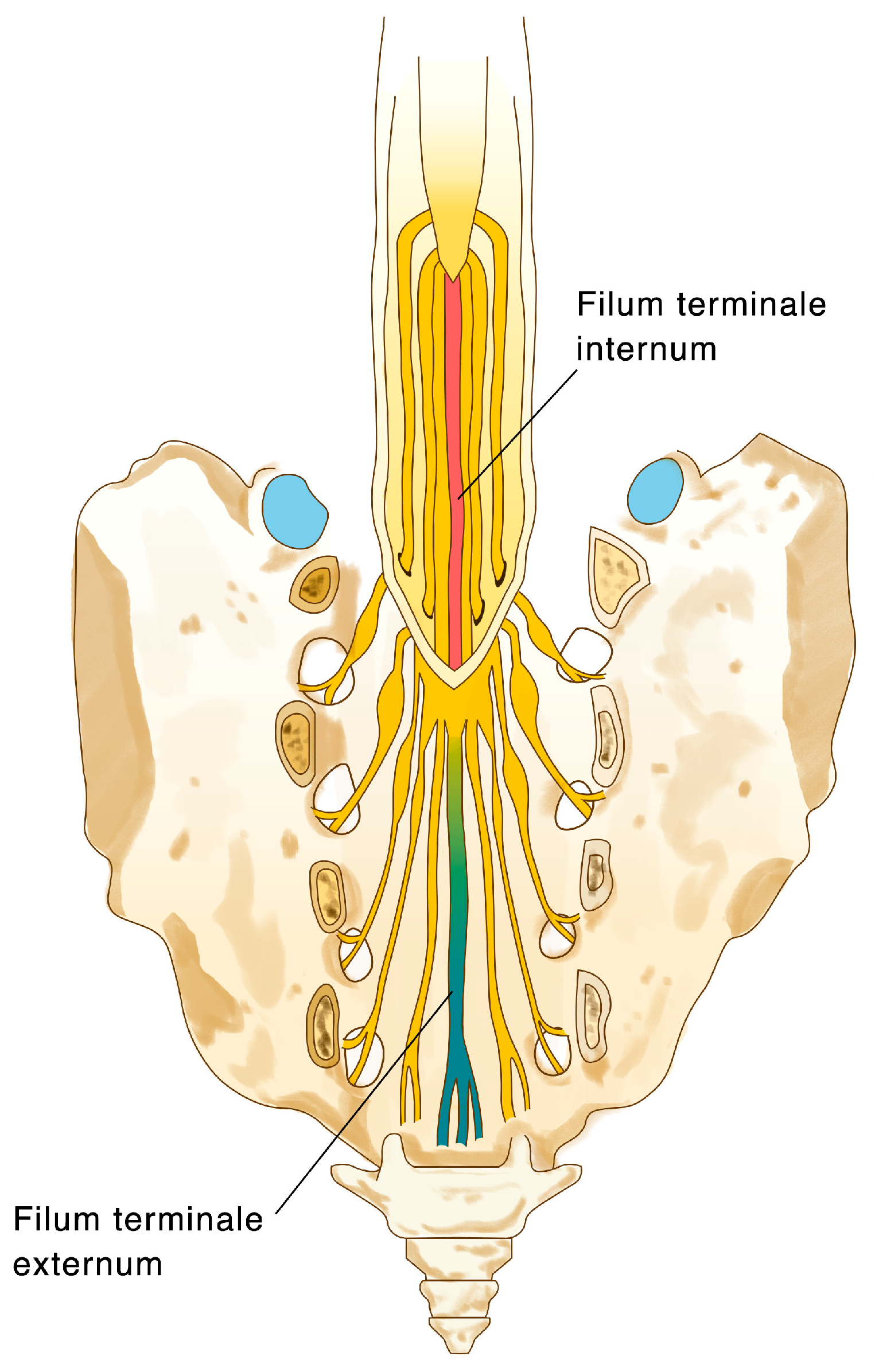
- Saker, E.; Henry, B.M.; Tomaszewski, K.A.; Loukas, M.; Iwanaga, J.; Oskouian, R.J.; Tubbs, R.S. The Filum Terminale Internum and Externum: A Comprehensive Review. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2017, 40, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Picart, T.; Barritault, M.; Simon, E.; Robinson, P.; Barrey, C.; Meyronet, D.; Mertens, P. Anatomical and Histological Analysis of a Complex Structure Too Long Considered a Simple Ligament: The Filum Terminale. World Neurosurg. 2019, 129, e464–e471. [Google Scholar] [CrossRef]
- Koeller, K.K.; Rosenblum, R.S.; Morrison, A.L. Neoplasms of the Spinal Cord and Filum Terminale: Radiologic-Pathologic Correlation. Radiographics 2000, 20, 1721–1749. [Google Scholar] [CrossRef]
- Djindjian, M.; Ribeiro, A.; Ortega, E.; Gaston, A.; Poirier, J. The Normal Vascularization of the Intradural Filum Terminale in Man. Surg. Radiol. Anat. 1988, 10, 201–209. [Google Scholar] [CrossRef]
- Selçuki, M.; Coşkun, K. Management of Tight Filum Terminale Syndrome with Special Emphasis on Normal Level Conus Medullaris (NLCM). Surg. Neurol. 1998, 50, 318–322; discussion 322. [Google Scholar] [CrossRef]
- Filippidis, A.S.; Kalani, M.Y.; Theodore, N.; Rekate, H.L. Spinal Cord Traction, Vascular Compromise, Hypoxia, and Metabolic Derangements in the Pathophysiology of Tethered Cord Syndrome. Neurosurg. Focus 2010, 29, E9. [Google Scholar] [CrossRef]
- Selden, N.R. Occult Tethered Cord Syndrome: The Case for Surgery. J. Neurosurg. 2006, 104, 302–304. [Google Scholar] [CrossRef] [PubMed]
- Takai, K.; Komori, T.; Taniguchi, M. Angioarchitecture of Filum Terminale Arteriovenous Fistulas: Relationship with a Tethered Spinal Cord. World Neurosurg. 2019, 122, e795–e804. [Google Scholar] [CrossRef] [PubMed]
- Giordan, E.; Brinjikji, W.; Ciceri, E.; Lanzino, G. Arteriovenous Fistulae of the Filum Terminale. J. Neurointerventional Surg. 2018, 10, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Law, A.J.; Scotter, J.; Brew, S. Lumbar Disc Herniation Exacerbating Venous Hypertension from a Spinal Perimedullary Arteriovenous Fistula of the Filum Terminale. J. Neurol. Sci. 2016, 369, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Witiw, C.D.; Fallah, A.; Radovanovic, I.; Wallace, M.C. Sacral Intradural Arteriovenous Fistula Treated Indirectly by Transection of the Filum Terminale: Technical Case Report. Neurosurgery 2011, 69, E780–E784. [Google Scholar] [CrossRef] [PubMed]
- Flores, B.C.; Klinger, D.R.; White, J.A.; Batjer, H.H. Spinal Vascular Malformations: Treatment Strategies and Outcome. Neurosurg. Rev. 2017, 40, 15–28. [Google Scholar] [CrossRef]
- Troude, L.J.; Melot, A.; Brunel, H.; Roche, P.-H. Arteriovenous Malformation of the Filum Terminale: An Exceptional Case. J. Neurosurg. 2016, 124, 1712–1715. [Google Scholar] [CrossRef]
- Baehring, J.M.; Damek, D.; Martin, E.C.; Betensky, R.A.; Hochberg, F.H. Neurolymphomatosis. Neuro-Oncol. 2003, 5, 104–115. [Google Scholar] [CrossRef]
- Alazawi, S.; Elomri, H.; Taha, R.; Bakr, M.; Abdelhamid, M.T.; Szabados, L.; Yassin, M.; Sabah, H.E.; Aboudi, K.; Ellahie, A.; et al. Neurolymphomatosis of the Median Nerve, Optic Nerve, L4 Spinal Nerve Root and Cauda Equina in Patients with B-Cell Malignancies: A Case Series. J. Med. Case Rep. 2021, 15, 133. [Google Scholar] [CrossRef]
- Seneviratne, S.L.; Maitland, A.; Afrin, L. Mast Cell Disorders in Ehlers-Danlos Syndrome. Am. J. Med. Genet. C Semin. Med. Genet. 2017, 175, 226–236. [Google Scholar] [CrossRef]
- Henderson, F.C.S.; Austin, C.; Benzel, E.; Bolognese, P.; Ellenbogen, R.; Francomano, C.A.; Ireton, C.; Klinge, P.; Koby, M.; Long, D.; et al. Neurological and Spinal Manifestations of the Ehlers-Danlos Syndromes. Am. J. Med. Genet. C Semin. Med. Genet. 2017, 175, 195–211. [Google Scholar] [CrossRef] [PubMed]
- Uhthoff, H.K.; Loehr, J.W. Calcific Tendinopathy of the Rotator Cuff: Pathogenesis, Diagnosis, and Management. J. Am. Acad. Orthop. Surg. 1997, 5, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Faure, A.; Khalfallah, M.; Perrouin-Verbe, B.; Caillon, F.; Deschamps, C.; Bord, E.; Mathe, J.-F.; Robert, R. Arachnoiditis Ossificans of the Cauda Equina. Case Report and Review of the Literature. J. Neurosurg. 2002, 97, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Benyaich, Z.; Laghmari, M.; Ait Benali, S. Arachnoiditis Ossificans of the Lumbar Spine: A Rare Cause of Progressive Cauda Equina Syndrome. World Neurosurg. 2021, 148, 116–117. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic (Total N = 288) | N (%) or Mean (SD) |
|---|---|
| Age at Surgery (years) | 29.0 (±21.3) |
| Adult Patients (>18 years) | 170 (59.0%) |
| Pediatric Patients (10–18 years) | 41 (14.2%) |
| Pediatric Patients (<10 years) | 77 (26.8%) |
| Gender (Female) | 202 (70.1%) |
| Diagnosis with Tethered Cord Syndrome | 288 (100%) |
| Mean # of TCS Triad Symptoms | 2.0 (±1.2) |
| Back and/or Leg Pain | 203 (70.5%) |
| Neurological Signs and Symptoms | 212 (73.6%) |
| Urological Symptoms | 182 (63.2%) |
| Patients at 3-month follow-up | 185 (64.2%) |
| Back and/or Leg Pain | 116 (62.7%) |
| Neurological Signs and Symptoms | 68 (26.8%) |
| Urological Symptoms | 64 (34.6%) |
| Patients at 12-month follow-up | 163 (56.6%) |
| Back and/or Leg Pain | 59 (63.2%) |
| Neurological Signs and Symptoms | 84 (51.5%) |
| Urological Symptoms | 80 (49.1%) |
| Histopathologic Finding (Total N = 288) | N (%) | Age Distribution (# of Patients, Percentage Out of Entire Sample) | ||
|---|---|---|---|---|
| Pediatric (<10 Years) | Pediatric (10–18 Years) | Adult Patients (>18 Years) | ||
| Peripheral Nerves | 281 (97.6%) | 81 (28.12%) | 40 (13.89%) | 160 (55.56%) |
| Ependymal Cells | 204 (70.8%) | 49 (17.01%) | 30 (10.42%) | 125 (43.4%) |
| Fatty infiltration | 118 (41%) | 47 (16.32%) | 16 (5.56%) | 55 (19.1%) |
| Ganglion Cells | 111 (38.5%) | 29 (10.07%) | 17 (5.9%) | 65 (22.57%) |
| Neuropil | 44 (15.3%) | 17 (5.9%) | 2 (0.69%) | 25 (8.68%) |
| Vascular findings | 36 (12.5%) | 11 (3.82%) | 4 (1.39%) | 21 (7.29%) |
| Meningothelial Cells | 14 (4.9%) | 5 (1.74%) | 1 (0.35%) | 8 (2.78%) |
| Inflammatory cells | 11 (3.8%) | 2 (0.69%) | 1 (0.35%) | 8 (2.78%) |
| Elastin Fibers | 9 (3.1%) | 4 (1.39%) | 1 (0.35%) | 4 (1.39%) |
| Corpora Amylacea | 6 (2.1%) | 0 (0.0%) | 0 (0.0%) | 6 (2.08%) |
| Psammoma bodies | 3 (1.0%) | 0 (0.0%) | 0 (0.0%) | 3 (1.04%) |
| Rosenthal fibers | 2 (0.07%) | 0 (0.0%) | 0 (0.0%) | 2 (0.69%) |
| Melanocytes | 1 (0.03%) | 1 (0.35%) | 0 (0.0%) | 0 (0.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdulrazeq, H.; Leary, O.P.; Tang, O.Y.; Karimi, H.; McElroy, A.; Gokaslan, Z.; Punsoni, M.; Donahue, J.E.; Klinge, P.M. The Surgical Histopathology of the Filum Terminale: Findings from a Large Series of Patients with Tethered Cord Syndrome. J. Clin. Med. 2024, 13, 6. https://doi.org/10.3390/jcm13010006
Abdulrazeq H, Leary OP, Tang OY, Karimi H, McElroy A, Gokaslan Z, Punsoni M, Donahue JE, Klinge PM. The Surgical Histopathology of the Filum Terminale: Findings from a Large Series of Patients with Tethered Cord Syndrome. Journal of Clinical Medicine. 2024; 13(1):6. https://doi.org/10.3390/jcm13010006
Chicago/Turabian StyleAbdulrazeq, Hael, Owen P. Leary, Oliver Y. Tang, Helen Karimi, Abigail McElroy, Ziya Gokaslan, Michael Punsoni, John E. Donahue, and Petra M. Klinge. 2024. "The Surgical Histopathology of the Filum Terminale: Findings from a Large Series of Patients with Tethered Cord Syndrome" Journal of Clinical Medicine 13, no. 1: 6. https://doi.org/10.3390/jcm13010006