
Systematic Evaluation of the Effects of Voluntary Activation on Lower Extremity Motor Thresholds

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
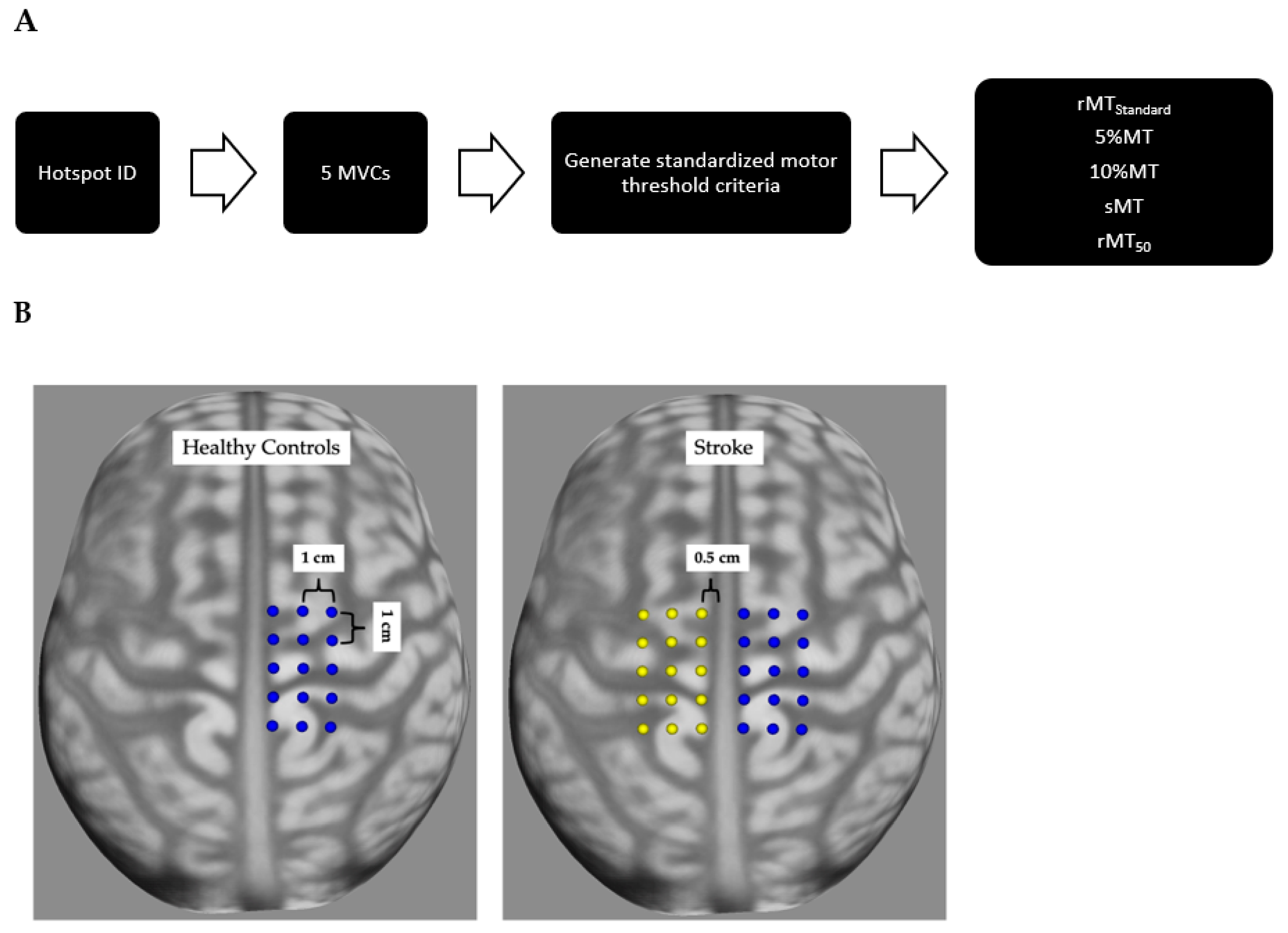
2.3. TMS Data Set-Up
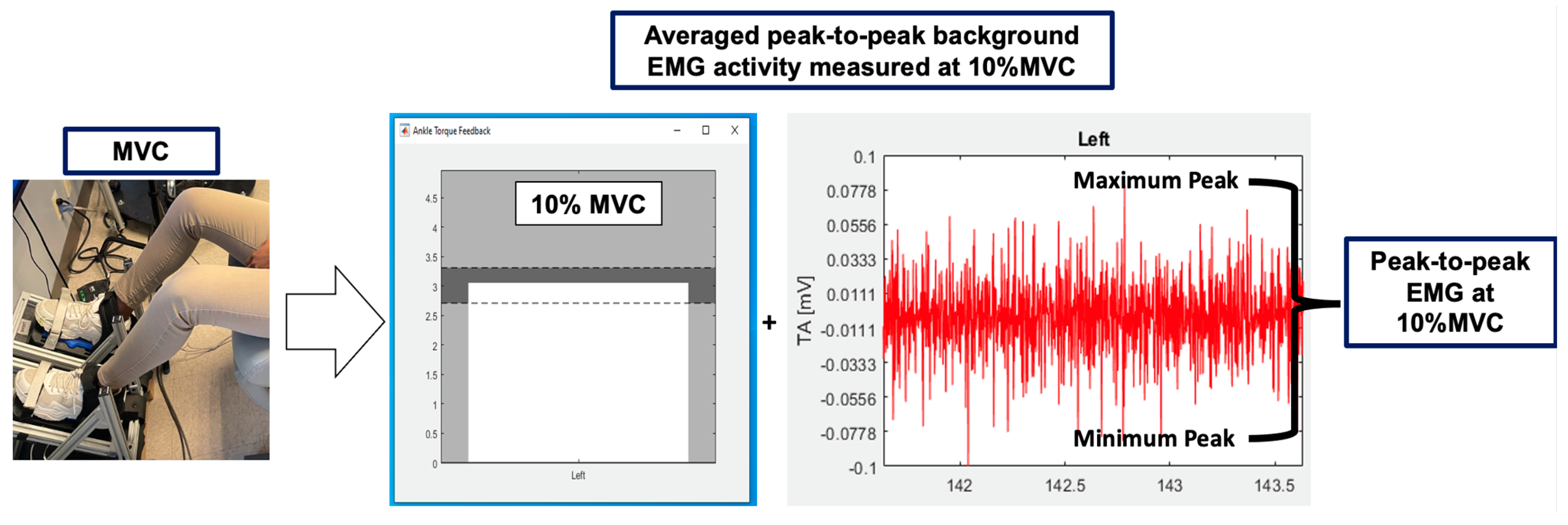
2.4. Motor Threshold Criterion
2.5. TMS Data Acquisition
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
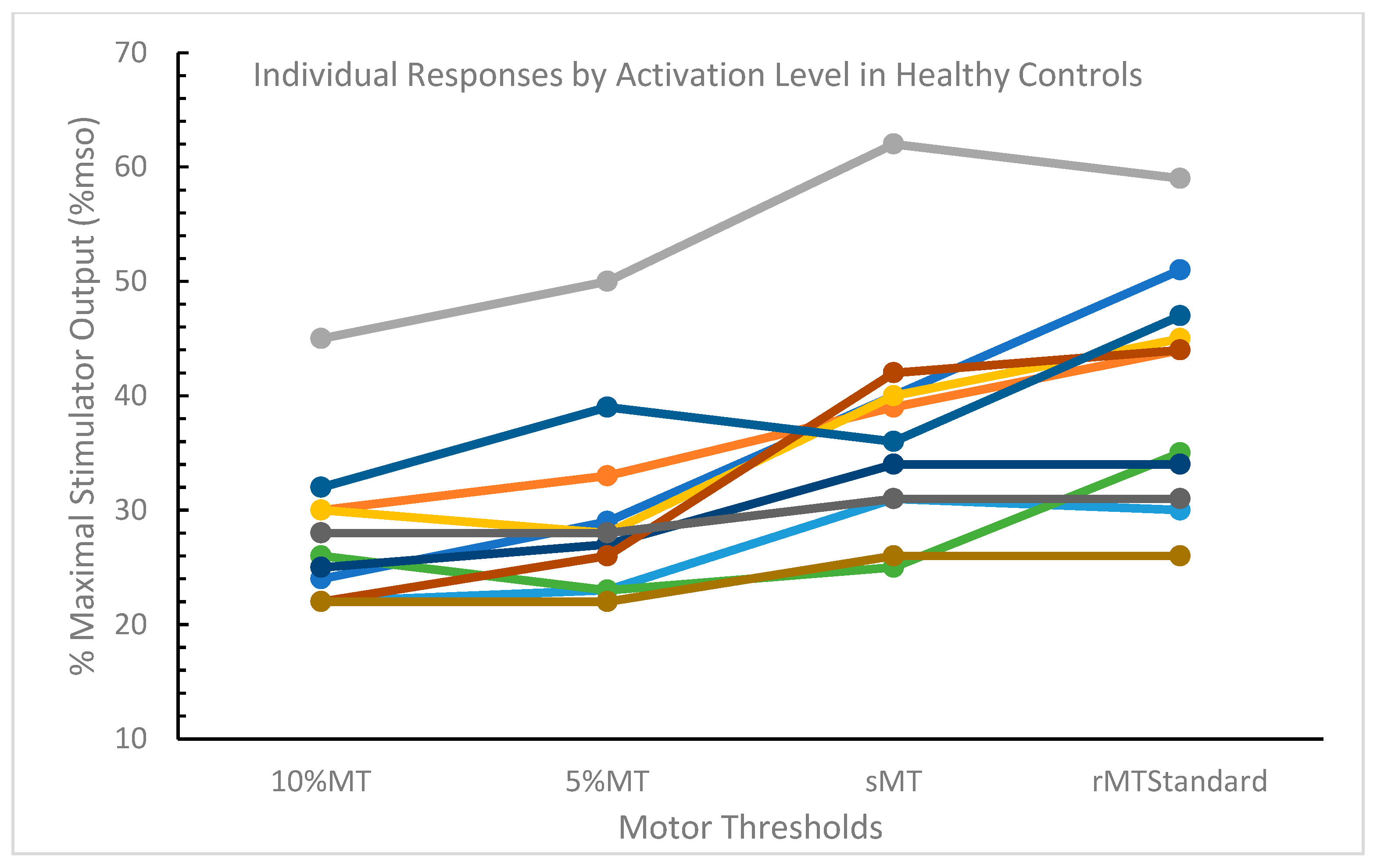
3.2. Healthy Control Participants
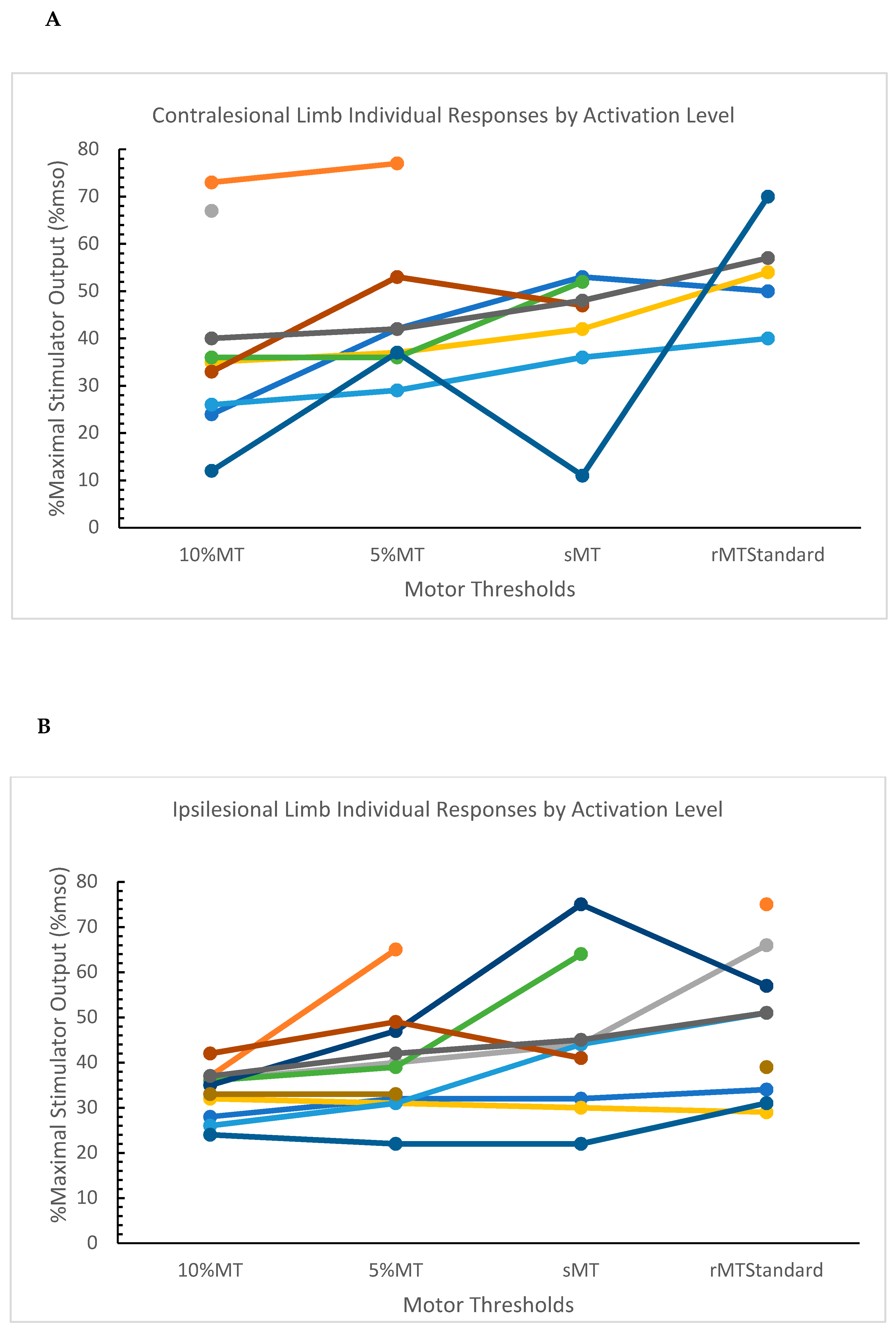
3.3. Post-Stroke Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fitzgerald, P.B.; Fountain, S.; Daskalakis, Z.J. A comprehensive review of the effects of rTMS on motor cortical excitability and inhibition. Clin. Neurophysiol. 2006, 117, 2584–2596. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Yan, L.; Huang, L.; Guan, X.; Dong, C.; Tao, H.; Wang, T.; Qin, X.; Wan, Q. Repetitive transcranial magnetic stimulation for the treatment of Alzheimer’s disease: A systematic review and meta-analysis of randomized controlled trials. PLoS ONE 2018, 13, e0205704. [Google Scholar] [CrossRef] [PubMed]
- Di Lazzaro, V.; Bella, R.; Benussi, A.; Bologna, M.; Borroni, B.; Capone, F.; Chen, K.-H.S.; Chen, R.; Chistyakov, A.V.; Classen, J.; et al. Diagnostic contribution and therapeutic perspectives of transcranial magnetic stimulation in dementia. Clin. Neurophysiol. 2021, 132, 2568–2607. [Google Scholar] [CrossRef] [PubMed]
- Starosta, M.; Cichoń, N.; Saluk-Bijak, J.; Miller, E. Benefits from Repetitive Transcranial Magnetic Stimulation in Post-Stroke Rehabilitation. J. Clin. Med. 2022, 11, 2149. [Google Scholar] [CrossRef]
- Sheng, R.; Chen, C.; Chen, H.; Yu, P. Repetitive transcranial magnetic stimulation for stroke rehabilitation: Insights into the molecular and cellular mechanisms of neuroinflammation. Front. Immunol. 2023, 14, 1197422. [Google Scholar] [CrossRef]
- Magnuson, J.; Ozdemir, M.A.; Mathieson, E.; Kirkman, S.; Passera, B.; Rampersad, S.; Dufour, A.B.; Brooks, D.; Pascual-Leone, A.; Fried, P.J.; et al. Neuromodulatory effects and reproducibility of the most widely used repetitive transcranial magnetic stimulation protocols. PLoS ONE 2023, 18, e0286465. [Google Scholar] [CrossRef]
- Vucic, S.; Stanley Chen, K.H.; Kiernan, M.C.; Hallett, M.; Benninger, D.; Di Lazzaro, V.; Rossini, P.M.; Benussi, A.; Berardelli, A.; Currà, A.; et al. Clinical diagnostic utility of transcranial magnetic stimulation in neurological disorders. Updated report of an IFCN committee. Clin. Neurophysiol. 2023, 150, 131–175. [Google Scholar] [CrossRef]
- Groppa, S.; Oliviero, A.; Eisen, A.; Quartarone, A.; Cohen, L.; Mall, V.; Kaelin-Lang, A.; Mima, T.; Rossi, S.; Thickbroom, G.; et al. A practical guide to diagnostic transcranial magnetic stimulation: Report of an IFCN committee. Clin. Neurophysiol. 2012, 123, 858–882. [Google Scholar] [CrossRef]
- Palmer, J.A.; Kesar, T.M.; Wolf, S.L.; Borich, M.R. Motor Cortical Network Flexibility is Associated With Biomechanical Walking Impairment in Chronic Stroke. Neurorehabil Neural Repair 2021, 35, 1065–1075. [Google Scholar] [CrossRef]
- Hof, A.L. The relationship between electromyogram and muscle force. Sport. Sportschaden 1997, 11, 79–86. [Google Scholar] [CrossRef]
- Cacchio, A.; Paoloni, M.; Cimini, N.; Mangone, M.; Liris, G.; Aloisi, P.; Santilli, V.; Marrelli, A. Reliability of TMS-related measures of tibialis anterior muscle in patients with chronic stroke and healthy subjects. J. Neurol. Sci. 2011, 303, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Kesar, T.M.; Stinear, J.W.; Wolf, S.L. The use of transcranial magnetic stimulation to evaluate cortical excitability of lower limb musculature: Challenges and opportunities. Restor. Neurol. Neurosci. 2018, 36, 333–348. [Google Scholar] [CrossRef] [PubMed]
- Charalambous, C.C.; Liang, J.N.; Kautz, S.A.; George, M.S.; Bowden, M.G. Bilateral Assessment of the Corticospinal Pathways of the Ankle Muscles Using Navigated Transcranial Magnetic Stimulation. JoVE J. Vis. Exp. 2019, 144, e58944. [Google Scholar] [CrossRef]
- van de Ruit, M.; Grey, M.J. The TMS Map Scales with Increased Stimulation Intensity and Muscle Activation. Brain Topogr. 2016, 29, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Ah Sen, C.B.; Fassett, H.J.; El-Sayes, J.; Turco, C.V.; Hameer, M.M.; Nelson, A.J. Active and resting motor threshold are efficiently obtained with adaptive threshold hunting. PLoS ONE 2017, 12, e0186007. [Google Scholar] [CrossRef]
- Rossi, S.; Antal, A.; Bestmann, S.; Bikson, M.; Brewer, C.; Brockmöller, J.; Carpenter, L.L.; Cincotta, M.; Chen, R.; Daskalakis, J.D.; et al. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines. Clin. Neurophysiol. 2021, 132, 269–306. [Google Scholar] [CrossRef]
- Kindred, J.H.; Finetto, C.; Cash, J.J.; Bowden, M.G. Standing Neurophysiological Assessment of Lower Extremity Muscles Post-Stroke. J. Vis. Exp. 2021, 173, e62601. [Google Scholar] [CrossRef]
- Mishory, A.; Molnar, C.; Koola, J.; Li, X.; Kozel, F.A.; Myrick, H.; Stroud, Z.; Nahas, Z.; George, M.S. The maximum-likelihood strategy for determining transcranial magnetic stimulation motor threshold, using parameter estimation by sequential testing is faster than conventional methods with similar precision. J. ECT 2004, 20, 160–165. [Google Scholar] [CrossRef]
- Borckardt, J.J.; Nahas, Z.; Koola, J.; George, M.S. Estimating resting motor thresholds in transcranial magnetic stimulation research and practice: A computer simulation evaluation of best methods. J. ECT 2006, 22, 169–175. [Google Scholar] [CrossRef]
- Ahn, Y.H.; Ahn, S.H.; Kim, H.; Hong, J.H.; Jang, S.H. Can stroke patients walk after complete lateral corticospinal tract injury of the affected hemisphere? Neuroreport 2006, 17, 987–990. [Google Scholar] [CrossRef]
- Peters, D.M.; Fridriksson, J.; Richardson, J.D.; Stewart, J.C.; Rorden, C.; Bonilha, L.; Middleton, A.; Fritz, S.L. Upper and Lower Limb Motor Function Correlates with Ipsilesional Corticospinal Tract and Red Nucleus Structural Integrity in Chronic Stroke: A Cross-Sectional, ROI-Based MRI Study. Behav. Neurol. 2021, 2021, e3010555. [Google Scholar] [CrossRef] [PubMed]
- Ngomo, S.; Leonard, G.; Moffet, H.; Mercier, C. Comparison of transcranial magnetic stimulation measures obtained at rest and under active conditions and their reliability. J. Neurosci. Methods 2012, 205, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Quartarone, A.; Rizzo, V.; Bagnato, S.; Morgante, F.; Sant’Angelo, A.; Girlanda, P.; Roman Siebner, H. Rapid-rate paired associative stimulation of the median nerve and motor cortex can produce long-lasting changes in motor cortical excitability in humans. J. Physiol. 2006, 575, 657–670. [Google Scholar] [CrossRef]
- Wassermann, E. Variation in the response to transcranial magnetic brain stimulation in the general population. Clin. Neurophysiol. 2002, 113, 1165–1171. [Google Scholar] [CrossRef]
- Deblieck, C.; Thompson, B.; Iacoboni, M.; Wu, A.D. Correlation between motor and phosphene thresholds: A transcranial magnetic stimulation study. Hum. Brain Mapp. 2008, 29, 662–670. [Google Scholar] [CrossRef]
- Deng, Z.D.; Lisanby, S.H.; Peterchev, A.V. Electric field depth-focality tradeoff in transcranial magnetic stimulation: Simulation comparison of 50 coil designs. Brain Stimul. 2013, 6, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Temesi, J.; Gruet, M.; Rupp, T.; Verges, S.; Millet, G.Y. Resting and active motor thresholds versus stimulus–response curves to determine transcranial magnetic stimulation intensity in quadriceps femoris. J. Neuroeng. Rehabil. 2014, 11, 40. [Google Scholar] [CrossRef]
- Yoder, R.D.; Seidenfeld, A.; Suwa, K. Normal hemoglobin-oxygen affinity. Anesthesiology 1975, 42, 741–744. [Google Scholar] [CrossRef]
- Kløvgaard, M.; Nielsen, N.O.; Sørensen, T.L.; Bjerregaard, P.; Olsen, B.; Júlíusson, P.B.; Roelants, M.; Christesen, H.T. Growth of children in Greenland exceeds the World Health Organization growth charts. Acta Paediatr. 2018, 107, 1953–1965. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Post-Stroke (n = 11) | Healthy Control (n = 11) | ||
|---|---|---|---|
| Age, µ (SD) | 60.9 (8.1) | 39.9 (9.4) | |
| Sex (F), n (%) | 7 (63.6) | 6 (54.5) | |
| Stroke Hemisphere (L), n (%) | 7 (63.6) | ||
| Stroke Type (Ischemic), n (%) | 9 (81.8) | ||
| Walking Aid Use, n (%) | 2 (18.2) | ||
| Time Since Stroke (months), n (%) | 65.5 (28.7) | ||
| 5-Times Sit to Stand (s), n (%) | 15.6 (6.6) | ||
| Limb, µ (SD) | Contralesional | Ipsilesional | Dominant |
| MVC (Nm) | 22.4 (9.6) | 28.1 (12.2) | 40.9 (50.1) |
| Criterion (mV) | 0.2 (0.1) | 0.3 (0.2) | 0.4 (0.2) |
| Healthy Control | Post-Stroke | |||||
|---|---|---|---|---|---|---|
| Limb | Dominant | Contralesional | Ipsilesional | |||
| Motor Threshold | n | LSM (SE) | n | LSM (SE) | n | LSM (SE) |
| 10%MT | 11 | 27.8 (2.7) | 9 | 38.4 (6.2) | 11 | 33.3 (3.9) |
| 5%MT | 11 | 29.8 (2.7) | 8 | 46.6 (6.4) | 11 | 39.2 (3.9) |
| sMT | 11 | 36.9 (2.7) a,b | 7 | 48.0 (6.6) | 9 | 45.3 (4.1) a |
| rMTStandard | 11 | 40.6 (2.7) a,b,c | 5 | 63.0 (7.1) a,b,c | 9 | 49.2 (4.1) a,b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cash, J.J.; Bowden, M.G.; Boan, A.D.; McTeague, L.M.; Kindred, J.H. Systematic Evaluation of the Effects of Voluntary Activation on Lower Extremity Motor Thresholds. J. Clin. Med. 2023, 12, 5993. https://doi.org/10.3390/jcm12185993
Cash JJ, Bowden MG, Boan AD, McTeague LM, Kindred JH. Systematic Evaluation of the Effects of Voluntary Activation on Lower Extremity Motor Thresholds. Journal of Clinical Medicine. 2023; 12(18):5993. https://doi.org/10.3390/jcm12185993
Chicago/Turabian StyleCash, Jasmine J., Mark G. Bowden, Andrea D. Boan, Lisa M. McTeague, and John H. Kindred. 2023. "Systematic Evaluation of the Effects of Voluntary Activation on Lower Extremity Motor Thresholds" Journal of Clinical Medicine 12, no. 18: 5993. https://doi.org/10.3390/jcm12185993