


Self-Efficacy and Self-Care as Risk Factors for Ischemic Stroke: Development and Validation of a Nomogram

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Eligibility Criteria
2.2. Sample Calculation and Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chugh, C. Acute Ischemic Stroke: Management Approach. Indian J. Crit. Care Med. 2019, 23 (Suppl. 2), S140–S146. [Google Scholar] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [PubMed]
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef]
- Donkor, E.S. Stroke in the 21(st) Century: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res. Treat. 2018, 2018, 3238165. [Google Scholar]
- Feigin, V.L.; Wang, W.; Fu, H.; Liu, L.; Krishnamurthi, R.; Bhattacharjee, R.; Parmar, P.; Hussein, T.; Barker-Collo, S. Primary stroke prevention in China—A new approach. Neurol. Res. 2015, 37, 378–380. [Google Scholar] [CrossRef] [PubMed]
- Szczepańska-Gieracha, J.; Mazurek, J. The Role of Self-Efficacy in the Recovery Process of Stroke Survivors. Psychol. Res. Behav. Manag. 2020, 13, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Frost, Y.; Weingarden, H.; Zeilig, G.; Nota, A.; Rand, D. Self-Care Self-Efficacy Correlates with Independence in Basic Activities of Daily Living in Individuals with Chronic Stroke. J. Stroke Cerebrovasc. Dis. 2015, 24, 1649–1655. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Orem, D. Nursing: Concepts of Practice, 4th ed.; Mosby Year Book: St. Louis, MO, USA, 1991. [Google Scholar]
- Boehme, A.K.; Esenwa, C.; Elkind, M.S. Stroke Risk Factors, Genetics, and Prevention. Circ. Res. 2017, 120, 472–495. [Google Scholar] [CrossRef]
- Lee, H.Y.; List, A. Examining students’ self-efficacy and perceptions of task difficulty in learning from multiple texts. Learn. Individ. Differ. 2021, 90, 102052. [Google Scholar] [CrossRef]
- Latkin, C.A.; Edwards, C.; Davey-Rothwell, M.A.; Tobin, K.E. The relationship between social desirability bias and self-reports of health, substance use, and social network factors among urban substance users in Baltimore, Maryland. Addict. Behav. 2017, 73, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Bi, G.; Li, R.; Liang, J.; Hu, Z.; Zhan, C. A nomogram with enhanced function facilitated by nomogramEx and nomogramFormula. Ann. Transl. Med. 2020, 8, 78. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [PubMed]
- Broderick, J.P.; Adeoye, O.; Elm, J. Evolution of the Modified Rankin Scale and Its Use in Future Stroke Trials. Stroke 2017, 48, 2007–2012. [Google Scholar] [CrossRef] [PubMed]
- Quinn, T.J.; Langhorne, P.; Stott, D.J. Barthel index for stroke trials: Development, properties, and application. Stroke 2011, 42, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Rasyid, A.; Harris, S.; Kurniawan, M.; Mesiano, T.; Hidayat, R. Fibrinogen and LDL Influence on Blood Viscosity and Outcome of Acute Ischemic Stroke Patients in Indonesia. Ann. Neurosci. 2019, 26, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Pemila, U. Pengaruh Model Edukasi Pencegahan Stroke Dalam Menurunkan Faktor Risiko Dan Meningkatkan Kemampuan Merawat Diri Pasien Risiko Tinggi Stroke. In Nursing Dissertation; University of Indonesia: Depok, Indonesia, 2020; p. 66. [Google Scholar]
- Han, H.R.; Lee, H.; Commodore-Mensah, Y.; Kim, M. Development and validation of the Hypertension Self-care Profile: A practical tool to measure hypertension self-care. J. Cardiovasc. Nurs. 2014, 29, E11–E20. [Google Scholar] [CrossRef]
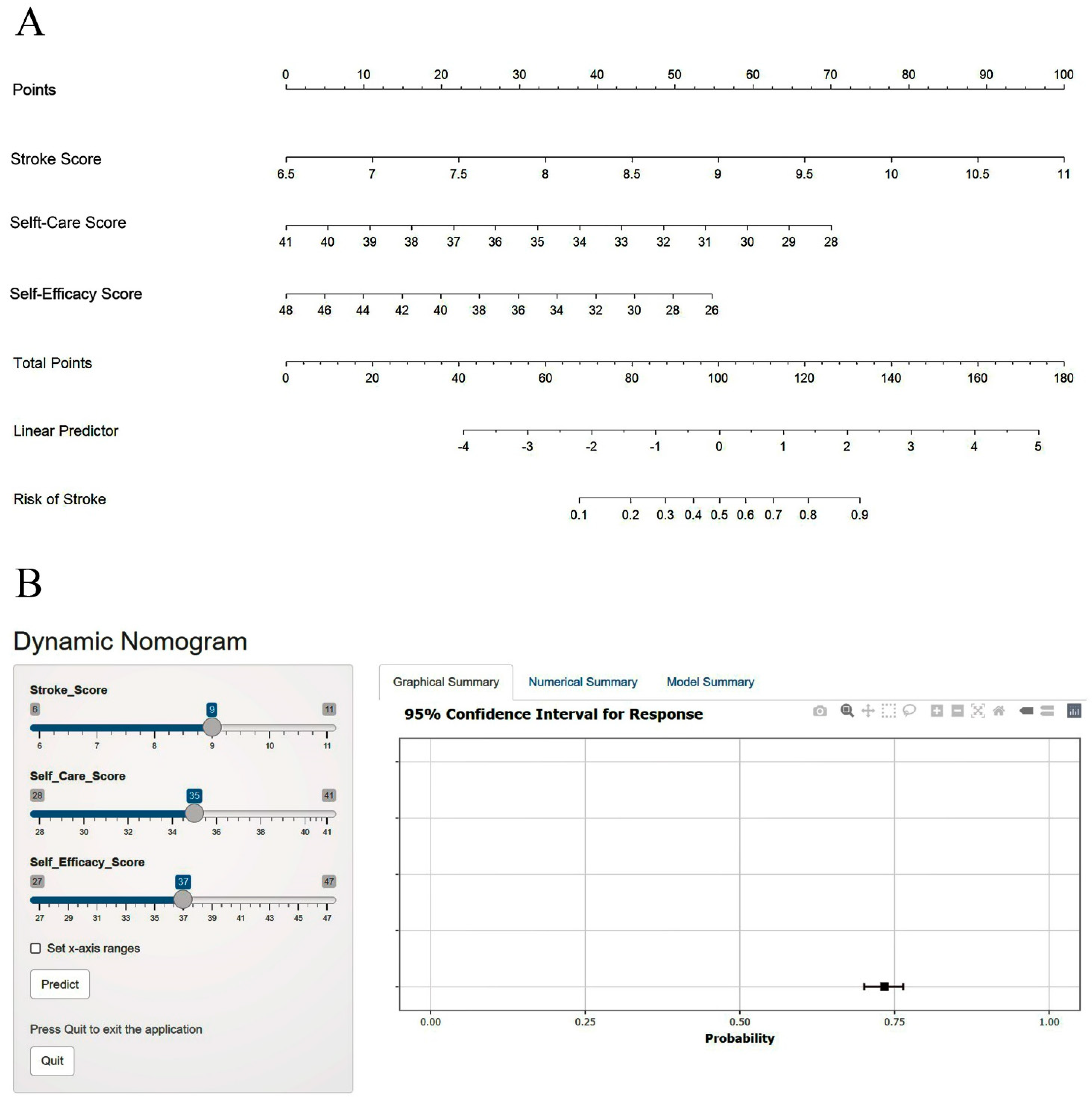
- Jalali, A.; Alvarez-Iglesias, A.; Roshan, D.; Newell, J. Visualising statistical models using dynamic nomograms. PLoS ONE 2019, 14, e0225253. [Google Scholar] [CrossRef]
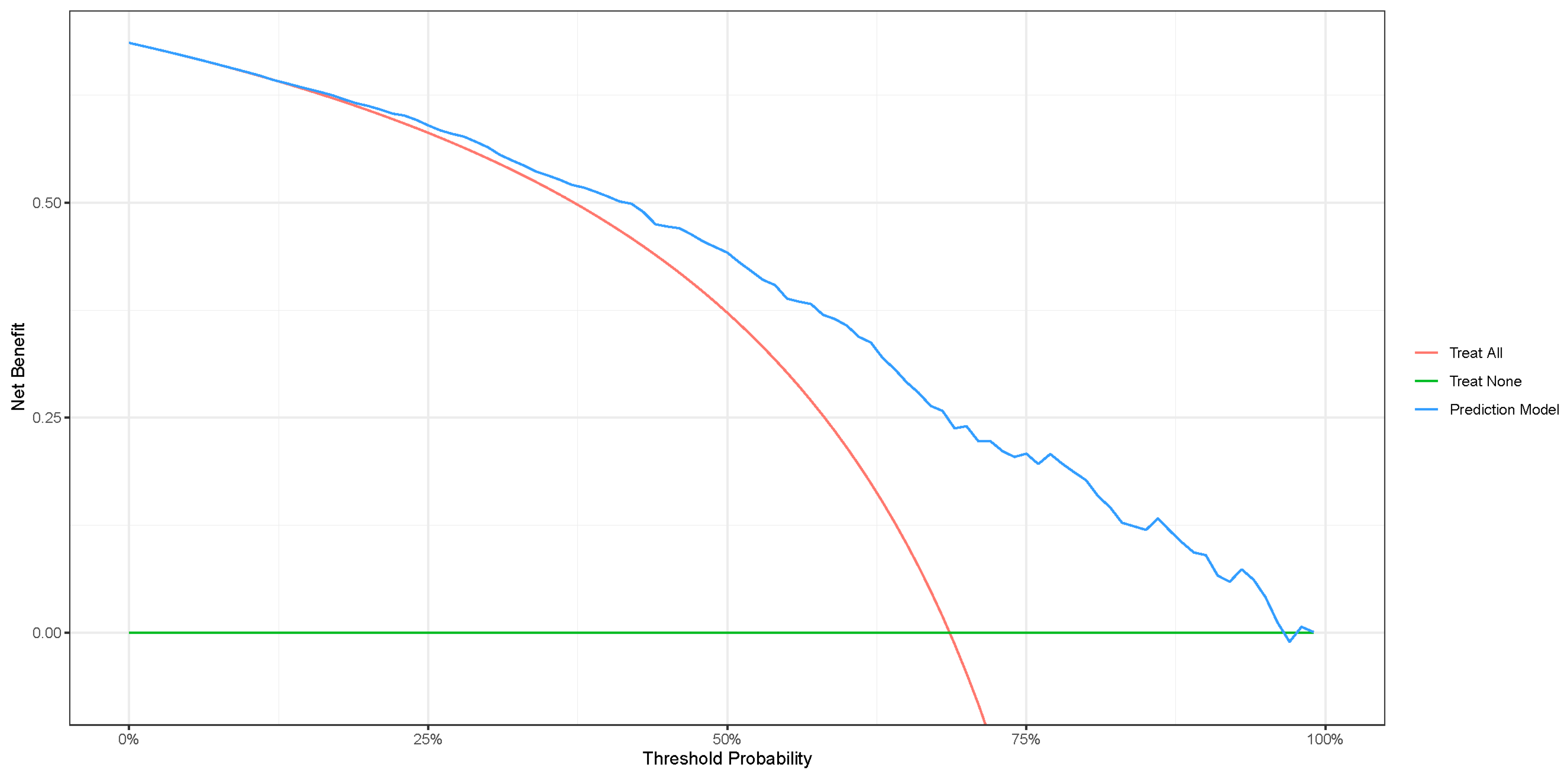
- Vickers, A.J.; Cronin, A.M. Everything you always wanted to know about evaluating prediction models (but were too afraid to ask). Urology 2010, 76, 1298–1301. [Google Scholar] [CrossRef]
- Warren-Findlow, J.; Seymour, R.B.; Brunner Huber, L.R. The association between self-efficacy and hypertension self-care activities among African American adults. J. Community Health 2012, 37, 15–24. [Google Scholar] [CrossRef]
- Bonger, Z.; Shiferaw, S.; Tariku, E.Z. Adherence to diabetic self-care practices and its associated factors among patients with type 2 diabetes in Addis Ababa, Ethiopia. Patient Prefer. Adherence 2018, 12, 963–970. [Google Scholar] [CrossRef]
- Tan, F.C.J.H.; Oka, P.; Dambha-Miller, H.; Tan, N.C. The association between self-efficacy and self-care in essential hypertension: A systematic review. BMC Fam. Pract. 2021, 22, 44. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Stroke | p-Value | OR | 95% CI | ||
|---|---|---|---|---|---|---|
| Yes (n = 120) | No (n = 120) | Min | Max | |||
| Gender | ||||||
| Male | 63 (53.4%) | 55 (46.6%) | 0.37 | 1.31 | 0.78 | 2.17 |
| Female | 57 (46.7%) | 65 (53.3%) | ||||
| Age | 57.43 (13.6) | 55.4 (11.9) | 0.22 | 1.01 | 0.99 | 1.03 |
| Ethnicity | ||||||
| Javanese | 52 (46.8%) | 59 (53.2%) | 0.83 | 1 (ref) | ||
| Sundanese | 39 (52.0%) | 36 (48.0%) | 1.23 | 0.68 | 2.21 | |
| Bataknese | 11 (55.0%) | 9 (45.0%) | 1.39 | 0.53 | 3.61 | |
| Others | 18 (52.9%) | 16 (47.1%) | 1.28 | 0.59 | 2.76 | |
| Locality | ||||||
| Urban | 65 (49.6%) | 66 (50.4%) | 1.00 | 0.97 | 0.58 | 1.61 |
| Rural | 55 (50.5%) | 54 (49.5%) | ||||
| Education | ||||||
| Senior high school or above | 89 (49.4%) | 91 (50.6%) | 0.88 | 0.92 | 0.51 | 1.64 |
| Junior high school or below | 31 (51.7%) | 29 (48.3%) | ||||
| Marital Status | ||||||
| Married | 111 (51.2%) | 106 (48.8%) | 0.49 | 1.51 | 0.62 | 3.69 |
| Unmarried | 9 (40.9%) | 13 (59.1%) | ||||
| Employment | ||||||
| Employed | 38 (45.8%) | 45 (54.2%) | 0.42 | 0.77 | 0.45 | 1.32 |
| Unemployed | 82 (52.2%) | 75 (47.8%0 | ||||
| Caregiver | ||||||
| Parent | 8 (61.5%) | 5 (38.5%) | 0.69 | 1 (ref) | ||
| Siblings | 15 (50.0%) | 15 (50.0%) | 0.66 | 0.17 | 2.36 | |
| Spouse | 23 (44.2%) | 29 (55.8%) | 0.49 | 0.14 | 1.72 | |
| Children | 74 (51.0%) | 71 (49.0%) | 0.65 | 0.20 | 2.09 | |
| Social Environment | ||||||
| Family | 79 (47.0%) | 89 (53.0%) | 0.31 | 1 (ref) | ||
| Friends | 25 (54.3%) | 21 (45.7%) | 1.34 | 0.69 | 2.58 | |
| Neighbors | 16 (61.5%) | 10 (38.5%) | 1.80 | 0.77 | 4.20 | |
| Blood Viscosity (cP) | 6.48 (1.51) | 5.30 (2.11) | <0.001 * | 1.42 | 1.22 | 1.65 |
| Barthel Index | 51.96 (27.21) | 66.44 (27.13) | <0.001 * | 0.98 | 0.97 | 0.99 |
| mRS | 2.62 (1.42) | 2.23 (1.26) | 0.026 * | 1.24 | 1.03 | 1.51 |
| Stroke Risk Score | 14.72 (2.95) | 6.81 (2.24) | <0.001 * | 3.52 | 2.39 | 5.18 |
| Self-Care Score | 22.39 (5.37) | 39.95 (6.08) | <0.001 * | 0.70 | 0.64 | 0.77 |
| Self-Efficacy Score | 21.73 (4.70) | 45.04 (7.39) | <0.001 * | 0.68 | 0.60 | 0.76 |
| Predictor | β | SE β | Wald | df | p-Value | eβ (Odds Ratio) |
|---|---|---|---|---|---|---|
| Stroke Risk Score | 1.257 | 0.445 | 7.959 | 1 | 0.005 * | 3.513 |
| Self-Care Score | −0.284 | 0.144 | 3.911 | 1 | 0.048 * | 0.753 |
| Self-Efficacy Score | −0.202 | 0.086 | 5.553 | 1 | 0.018 * | 0.817 |
| Constant | 7.131 | 4.938 | 2.085 | 1 | 0.149 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rasyid, A.; Pemila, U.; Aisah, S.; Harris, S.; Wiyarta, E.; Fisher, M. Self-Efficacy and Self-Care as Risk Factors for Ischemic Stroke: Development and Validation of a Nomogram. J. Clin. Med. 2023, 12, 5665. https://doi.org/10.3390/jcm12175665
Rasyid A, Pemila U, Aisah S, Harris S, Wiyarta E, Fisher M. Self-Efficacy and Self-Care as Risk Factors for Ischemic Stroke: Development and Validation of a Nomogram. Journal of Clinical Medicine. 2023; 12(17):5665. https://doi.org/10.3390/jcm12175665
Chicago/Turabian StyleRasyid, Al, Uke Pemila, Siti Aisah, Salim Harris, Elvan Wiyarta, and Marc Fisher. 2023. "Self-Efficacy and Self-Care as Risk Factors for Ischemic Stroke: Development and Validation of a Nomogram" Journal of Clinical Medicine 12, no. 17: 5665. https://doi.org/10.3390/jcm12175665