
Executive Functions and Psychopathology Dimensions in Deficit and Non-Deficit Schizophrenia
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Neuropsychological Assessment
2.2.1. General Intellectual Ability
2.2.2. Tasks from MCCB
2.2.3. Color Trail Test
2.2.4. Berg Card Sorting Test
2.3. Clinical Assessment
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
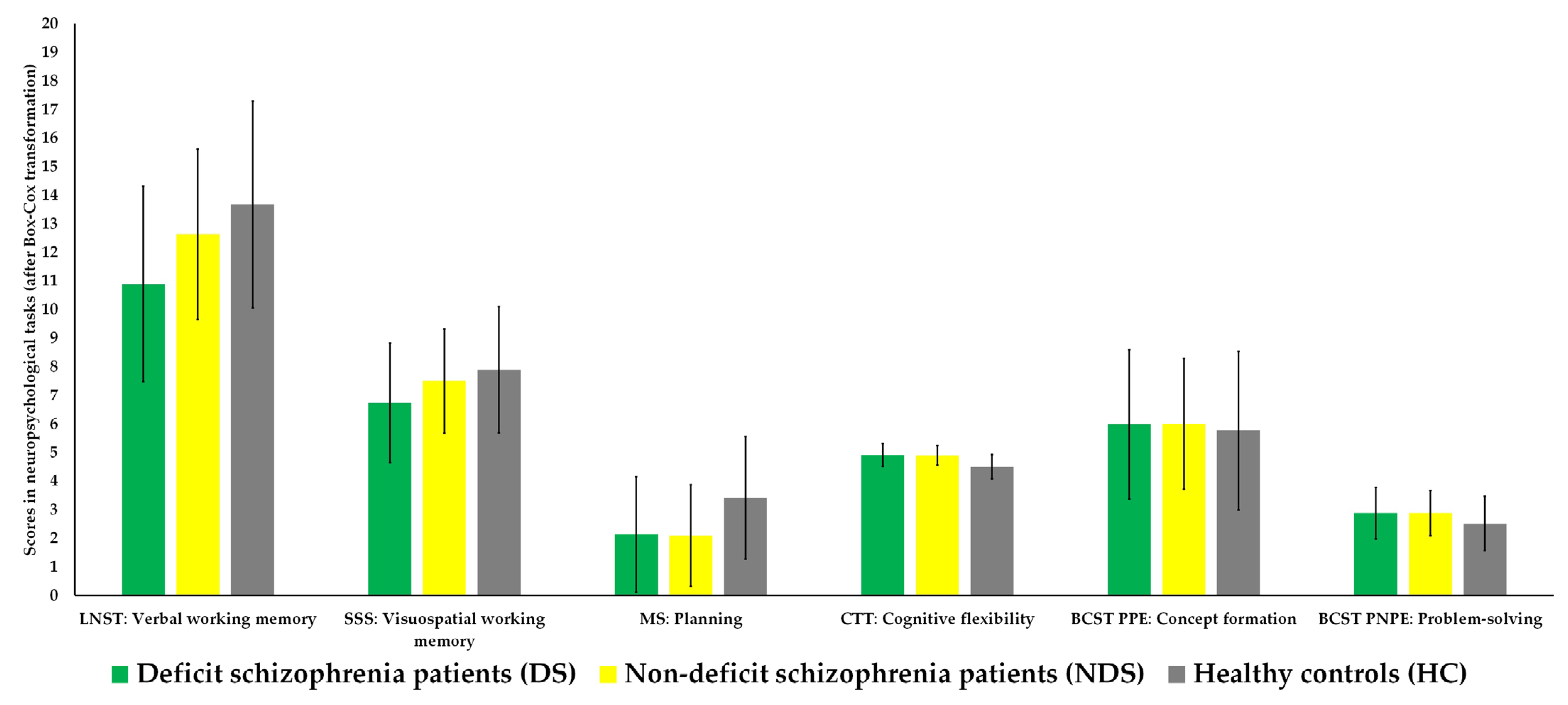
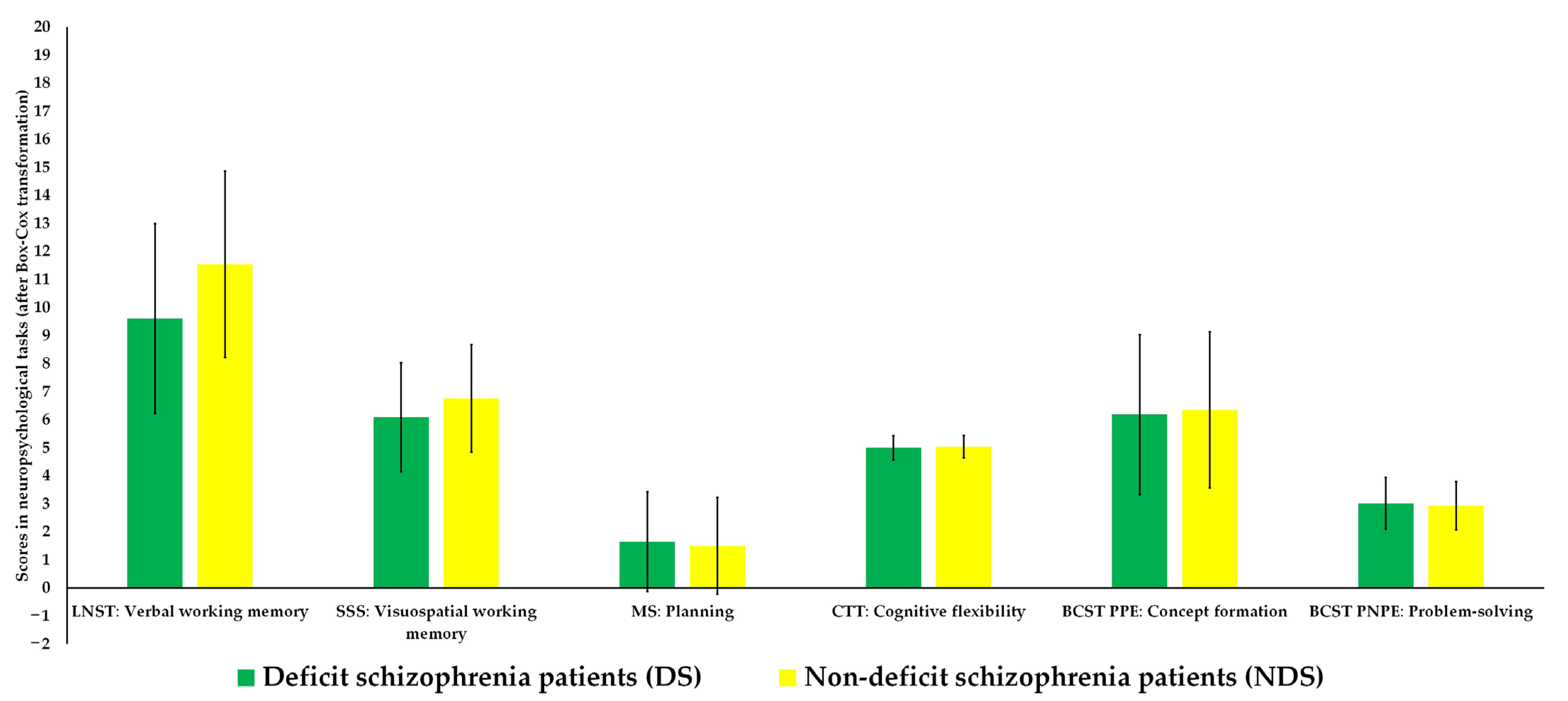
3.2. Differences in Executive Functions
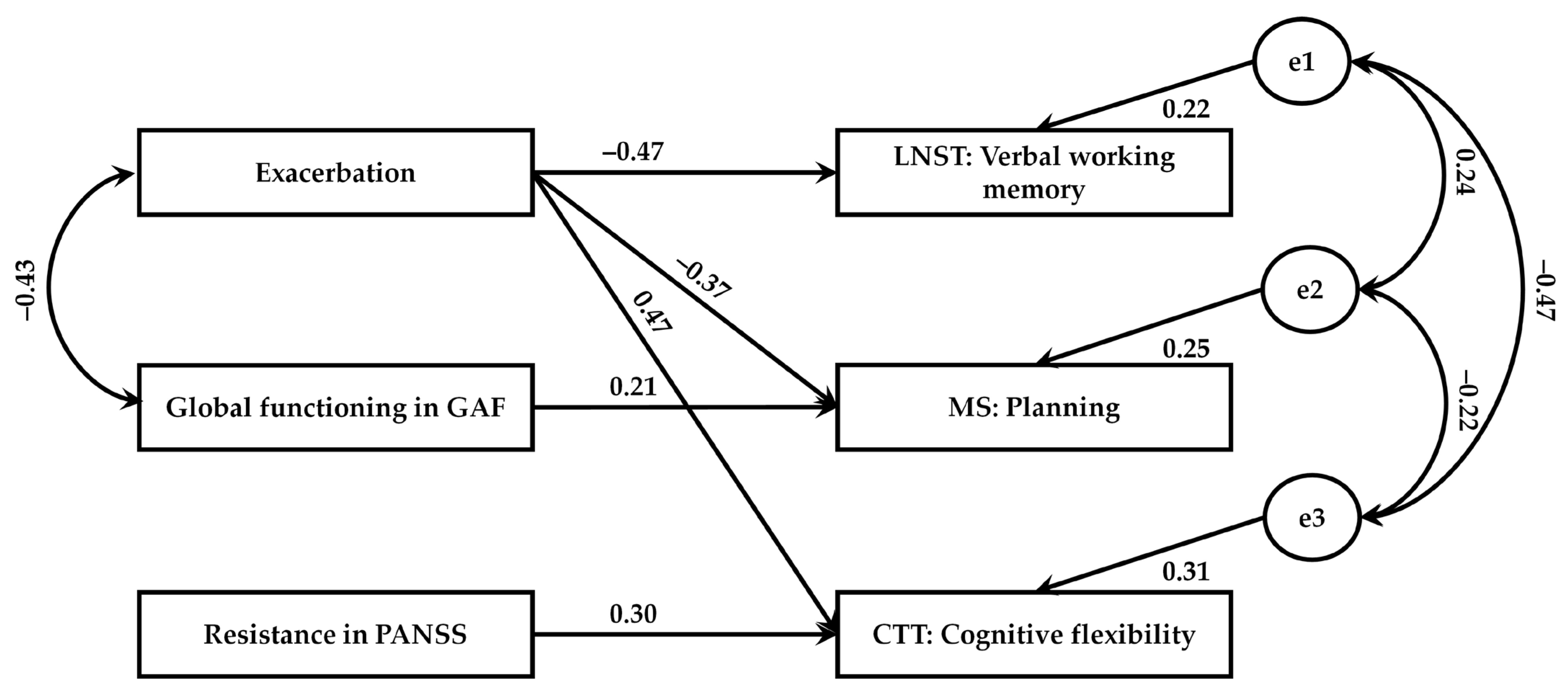
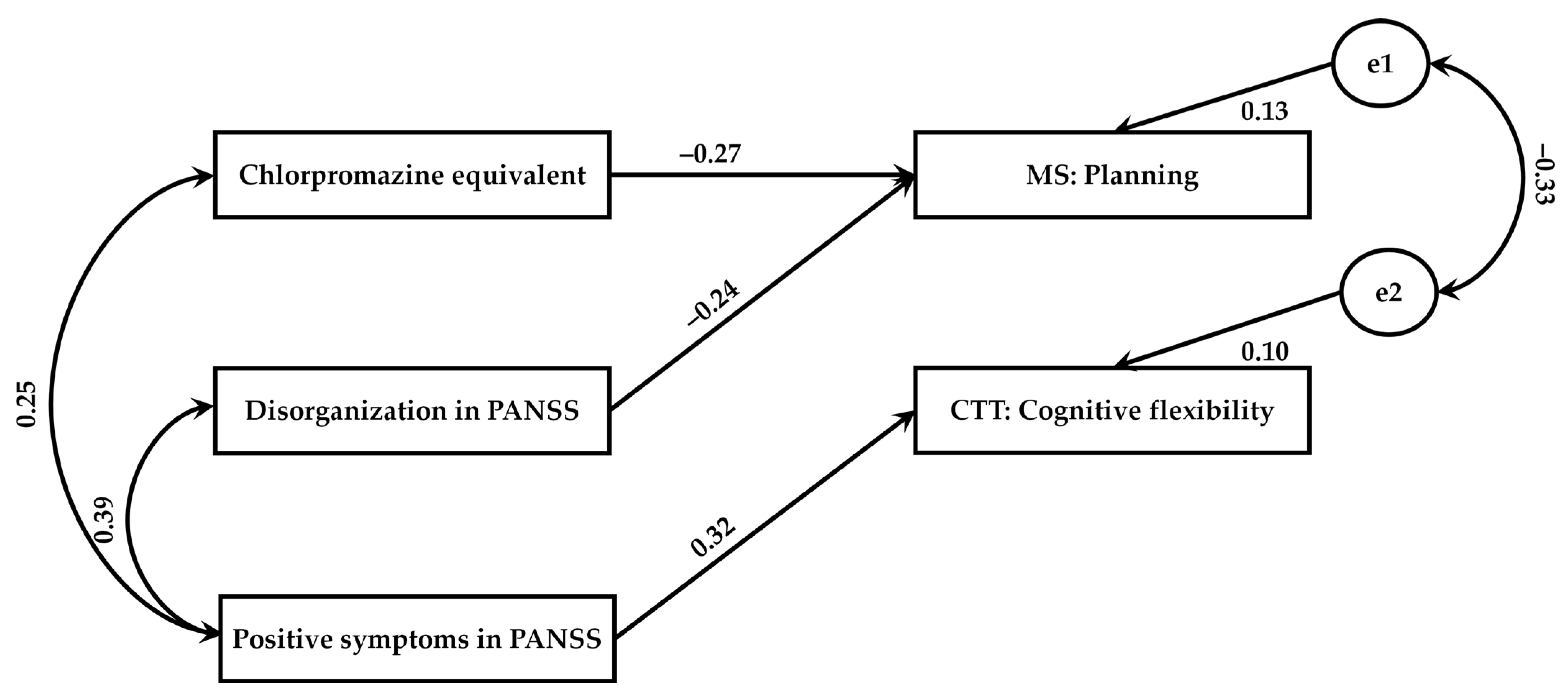
3.3. Relationships between Psychopathological Dimensions and Executive Functions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vyas, N.S.; Patel, N.H.; Puri, B.K. Neurobiology and phenotypic expression in early onset schizophrenia. Early. Interv. Psychiatry 2011, 5, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Bitanihirwe, B.K.; Mauney, S.A.; Woo, T.U. Weaving a net of neurobiological mechanisms in schizophrenia and unraveling the underlying pathophysiology. Biol. Psychiatry 2016, 80, 589–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lesh, T.A.; Niendam, T.A.; Minzenberg, M.J.; Carter, C.S. Cognitive control deficits in schizophrenia: Mechanisms and meaning. Neuropsychopharmacology 2011, 36, 316–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkpatrick, B.; Galderisi, S. Deficit schizophrenia: An update. World Psychiatry 2008, 7, 143–147. [Google Scholar] [CrossRef] [Green Version]
- Messias, E.; Kirkpatrick, B.; Bromet, E.; Ross, D.; Buchanan, R.W.; Carpenter, W.T., Jr.; Tek, C.; Kendler, K.S.; Walsh, D.; Dollfus, S. Summer birth and deficit schizophrenia: A pooled analysis from six countries. Arch. Gen. Psychiatry 2004, 61, 985–989. [Google Scholar] [CrossRef] [Green Version]
- Dickerson, F.; Kirkpatrick, B.; Boronow, J.; Stallings, C.; Origoni, A.; Yolken, R. Deficit schizophrenia: Association with serum antibodies to cytomegalovirus. Schizophr. Bull. 2006, 32, 396–400. [Google Scholar] [CrossRef] [Green Version]
- Hong, L.E.; Avila, M.T.; Adami, H.; Elliot, A.; KThaker, G. Components of the smooth pursuit function in deficit and non-deficit schizophrenia. Schizophr. Res. 2003, 63, 39–48. [Google Scholar] [CrossRef]
- Tek, C.; Kirkpatrick, B.; Buchanan, R.W. A five-year follow-up study of deficit and non-deficit schizophrenia. Schizophr. Res. 2001, 49, 253–260. [Google Scholar] [CrossRef]
- Chemerinski, E.; Reichenberg, A.; Kirkpatrick, B.; Bowie, C.R.; Harvey, P.D. Three dimensions of clinical symptoms in elderly patients with schizophrenia: Prediction of six-year cognitive and functional status. Schizophr. Res. 2006, 85, 12–19. [Google Scholar] [CrossRef]
- Samochowiec, J.; Pełka-Wysiecka, J. Deficit schizophrenia—How to diagnose and treat? Guide GPs 2012, 15, 110–114. [Google Scholar]
- Cohen, A.S.; Saperstein, A.M.; Gold, J.M.; Kirkpatrick, B.; Carpenter, W.T., Jr.; Buchanan, R.W. Neuropsychology of the deficit syndrome: New data and meta-analysis of findings to date. Schizophr. Bull. 2007, 33, 1201–1212. [Google Scholar] [CrossRef] [Green Version]
- Buchanan, R.W.; Strauss, M.E.; Kirkpatrick, B.; Holstein, C.; Breier, A.; Carpenter, W.T., Jr. Neuropsychological impairments in deficit vs nondeficit forms of schizophrenia. Arch. Gen. Psychiatry 1994, 51, 804–811. [Google Scholar] [CrossRef]
- Galderisi, S.; Quarantelli, M.; Volpe, U.; Mucci, A.; Cassano, G.B.; Invernizzi, G.; Rossi, A.; Vita, A.; Pini, S.; Cassano, P. Patterns of structural MRI abnormalities in deficit and nondeficit schizophrenia. Schizophr. Bull. 2008, 34, 393–401. [Google Scholar] [CrossRef] [Green Version]
- Bora, E.; Akdede, B.B.; Alptekin, K. Neurocognitive impairment in deficit and non-deficit schizophrenia: A meta-analysis. Psychol. Med. 2017, 47, 2401–2413. [Google Scholar] [CrossRef]
- Lewandowski, K.E.; Sperry, S.H.; Cohen, B.M.; Ongür, D. Cognitive variability in psychotic disorders: A cross diagnostic cluster analysis. Psychol. Med. 2014, 44, 3239–3248. [Google Scholar] [CrossRef] [Green Version]
- Bora, E. Differences in cognitive impairment between schizophrenia and bipolar disorder: Considering the role of heterogeneity. Psychiatry. Clin. Neurosci. 2016, 70, 424–433. [Google Scholar] [CrossRef] [Green Version]
- Tyburski, E.; Pełka-Wysiecka, J.; Mak, M.; Samochowiec, A.; Bieńkowski, P.; Samochowiec, J. Neuropsychological Profile of Specific Executive Dysfunctions in Patients with Deficit and Non-deficit Schizophrenia. Front. Psychol. 2017, 8, e1459. [Google Scholar] [CrossRef] [Green Version]
- Cohen, A.S.; Brown, L.A.; Minor, K.S. The psychiatric symptomatology of deficit schizophrenia: A meta-analysis. Schizophr. Res. 2010, 118, 122–127. [Google Scholar] [CrossRef]
- Enticott, P.G.; Ogloff, J.R.; Bradshaw, J.L. Associations between laboratory measures of executive inhibitory control and self-reported impulsivity. Pers. Individ. Differ. 2006, 41, 285–294. [Google Scholar] [CrossRef]
- Carpenter, W.T.; Heinrichs, D.W.; Wagman, A.M. Deficit and Nondeficit Forms of Schizophrenia: The Concept. Am. J. Psychiatry 1988, 145, 578–583. [Google Scholar] [CrossRef]
- Strauss, G.P.; Harrow, M.; Grossman, L.S.; Rosen, C. Periods of recovery in deficit syndrome schizophrenia: A 20-year multi–follow-up longitudinal study. Schizophr. Bull. 2010, 36, 788–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, S.J.; Bird, J.; Brindley, R.; Frith, C.D.; Burgess, P.W. Atypical recruitment of medial prefrontal cortex in autism spectrum disorders: An fMRI study of two executive function tasks. Neuropsychologia 2008, 46, 2281–2291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scherbaum, S.; Frisch, S.; Holfert, A.M.; O'Hora, D.; Dshemuchadse, M. No evidence for common processes of cognitive control and self-control. Acta Psychol. 2018, 182, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, J.A.; Emory, E. Executive function and the frontal lobes: A meta-analytic review. Neuropsychol. Rev. 2006, 16, 17–42. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.C.; Shum, D.; Toulopoulou, T.; Chen, E.Y. Assessment of executive functions: Review of instruments and identification of critical issues. Arch. Clin. Neuropsychol. 2008, 23, 201–216. [Google Scholar] [CrossRef] [Green Version]
- Jurado, M.B.; Rosselli, M. The elusive nature of executive functions: A review of our current understanding. Neuropsychol. Rev. 2007, 17, 213–233. [Google Scholar] [CrossRef]
- Lezak, M.D.; Howieson, D.B.; Loring, D.W. Neuropsychological Assessment, 4th ed.; Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Barkley, R.A. The executive functions and self-regulation: An evolutionary neuropsychological perspective. Neuropsychol. Rev. 2001, 11, 1–29. [Google Scholar] [CrossRef]
- Dibben, C.R.; Rice, C.; Laws, K.; McKenna, P.J. Is executive impairment associated with schizophrenic syndromes? A meta-analysis. Psychol. Med. 2009, 39, 381–392. [Google Scholar] [CrossRef] [Green Version]
- Bucci, P.; Mucci, A.; Piegari, G.; Nobile, M.; Pini, S.; Rossi, A.; Vita, A.; Galderisi, S.; Maj, M. Characterization of premorbid functioning during childhood in patients with deficit vs. non-deficit schizophrenia and in their healthy siblings. Schizophr. Res. 2016, 174, 172–176. [Google Scholar] [CrossRef]
- Seckinger, R.A.; Goudsmit, N.; Coleman, E.; Harkavy-Friedman, J.; Yale, S.; Rosenfield, P.J.; Malaspina, D. Olfactory identification and WAIS-R performance in deficit andvnondeficit schizophrenia. Schizophr. Res. 2004, 69, 55–65. [Google Scholar] [CrossRef]
- Brazo, P.; Marié, R.M.; Halbecq, I.; Benali, K.; Segard, L.; Delamillieure, P.; Langlois-Théry, S.; Van Der Elst, A.; Thibaut, F.; Petit, M.; et al. Cognitive patterns in subtypes of schizophrenia. Eur. Psychiatry 2002, 17, 155–162. [Google Scholar] [CrossRef]
- Galderisi, S.; Maj, M.; Mucci, A.; Cassano, G.B.; Invernizzi, G.; Rossi, A.; Vita, A.; Dell’Osso, L.; Daneluzzo, E.; Pini, S. Historical, psychopathological, neurological, and neuropsychological aspects of deficit schizophrenia: A multicenter study. Am. J. Psychiatry 2002, 159, 983–990. [Google Scholar] [CrossRef] [Green Version]
- Horan, W.P.; Blanchard, J.J. Neurocognitive, social, and emotional dysfunction in deficit syndrome schizophrenia. Schizophr. Res. 2003, 65, 125–137. [Google Scholar] [CrossRef]
- Wang, X.; Yao, S.; Kirkpatrick, B.; Shi, C.; Yi, J. Psychopathology and neuropsychological impairments in deficit and nondeficit schizophrenia of Chinese origin. Psychiatry. Res. 2008, 158, 195–205. [Google Scholar] [CrossRef]
- Shafer, A.; Dazzi, F. Meta-analysis of the positive and Negative Syndrome Scale (PANSS) factor structure. J. Psychiatr. Res. 2019, 115, 113–120. [Google Scholar] [CrossRef]
- World Health Organization (WHO). The ICD-10 Classification of Mental and Behavioural Disorders; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The Development and Validation of a Structured Diagnostic Psychiatric Interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar]
- Bora, E.; Murray, R.M. Meta-analysis of cognitive deficits in ultra-high risk to psychosis and first-episode psychosis: Do the cognitive deficits progress over, or after, the onset of psychosis? Schizophr. Bull. 2014, 40, 744–755. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Wang, G.; Jin, H.; Lyu, H.; Liu, Y.; Guo, W.; Shi, C.; Meyers, J.; Wang, J.; Zhao, J.; et al. Cognitive deficits in subjects at risk for psychosis, first-episode and chronic schizophrenia patients. Psychiatry Res. 2019, 274, 235–242. [Google Scholar] [CrossRef]
- Xiong, Y.B.; Bo, Q.J.; Wang, C.M.; Tian, Q.; Liu, Y.; Wang, C.Y. Differential of frequency and duration mismatch negativity and theta power deficits in first-episode and chronic schizophrenia. Front. Behav. Neurosci. 2019, 13, e37. [Google Scholar] [CrossRef] [Green Version]
- Hulshoff Pol, H.E.; Kahn, R.S. What happens after the first episode? A review of progressive brain changes in chronically ill patients with schizophrenia. Schizophr. Bull. 2008, 34, 354–366. [Google Scholar] [CrossRef]
- Chatterjee, I.; Kumar, V.; Rana, B.; Agarwal, M.; Kumar, N. Impact of ageing on the brain regions of the schizophrenia patients: An fMRI study using evolutionary approach. Multimed. Tools. Appl. 2020, 79, 24757–24779. [Google Scholar] [CrossRef]
- Diaz-Asper, C.M.; Schretlen, D.J.; Pearlson, G.D. How well does IQ predict neuropsychological test performance in normal adults? J. Int. Neuropsychol. Soc. 2004, 10, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Khandaker, G.M.; Barnett, J.H.; White, I.R.; Jones, P.B. A quantitative meta-analysis of population-based studies of premorbid intelligence and schizophrenia. Schizophr. Res. 2011, 132, 220–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Missar, C.D.; Gold, J.M.; Goldberg, T.E. WAIS-R short forms in chronic schizophrenia. Schizophr. Res. 1994, 12, 247–250. [Google Scholar] [CrossRef]
- Russell, A.J.; Munro, J.; Jones, P.B.; Hayward, P.; Hemsley, D.R.; Murray, R.M. The National Adult Reading Test as a measure of premorbid IQ in schizophrenia. Br. J. Clin. Psychol. 2000, 39, 297–305. [Google Scholar] [CrossRef]
- Blyler, C.R.; Gold, J.M.; Iannone, V.N.; Buchanan, R.W. Short form of the WAIS-III for use with patients with schizophrenia. Schizophr. Res. 2000, 46, 209–215. [Google Scholar] [CrossRef]
- Miller, H.R.; Streiner, D.L.; Goldberg, J.O. Short, shorter, shortest: The efficacy of WAIS-R short forms with mixed psychiatric patients. Assessment 1996, 3, 165–169. [Google Scholar] [CrossRef]
- Christensen, B.K.; Girard, T.A.; Bagby, R.M. Wechsler Adult Intelligence Scale-short form for index and IQ scores in a psychiatric population. Psychol. Assess. 2007, 19, 236–240. [Google Scholar] [CrossRef]
- Sumiyoshi, C.; Fujino, H.; Sumiyoshi, T.; Yasuda, Y.; Yamamori, H.; Ohi, K.; Fujimoto, M.; Takeda, M.; Hashimoto, R. Usefulness of the Wechsler Intelligence Scale short form for assessing functional outcomes in patients with schizophrenia. Psychiatry Res. 2016, 245, 371–378. [Google Scholar] [CrossRef]
- Bulzacka, E.; Meyers, J.E.; Boyer, L.; Le Gloahec, T.; Fond, G.; Szöke, A.; Leboyer, M.; Schürhoff, F. WAIS-IV seven-subtest short form: Validity and clinical use in schizophrenia. Arch. Clin. Neuropsychol. 2016, 31, 915–925. [Google Scholar] [CrossRef] [Green Version]
- Jędrasik-Styła, M.; Ciołkiewicz, A.; Styła, R.; Linke, M.; Parnowska, D.; Gruszka, A.; Denisiuk, M.; Jarema, M.; Green, M.F.; Wichniak, A. The Polish academic version of the MATRICS Consensus Cognitive Battery (MCCB): Evaluation of psychometric properties. Psychiatr. Q. 2015, 8, 435–447. [Google Scholar] [CrossRef] [Green Version]
- Nuechterlein, K.H.; Green, M.F.; Kern, R.S.; Baade, L.E.; Barch, D.M.; Cohen, J.D.; Essock, S.; Fenton, W.S.; Frese, F.J., 3rd; Gold, J.M.; et al. The MATRICS Consensus Cognitive Battery, part 1: Test selection, reliability, and validity. Am. J. Psychiatry 2008, 165, 203–213. [Google Scholar] [CrossRef] [Green Version]
- D’Elia, L.F.; Satz, P.; Uchiyama, C.L.; White, T. Color Trails Test; Psychological Assessment Resources Inc.: Lutz, FL, USA, 1996. [Google Scholar]
- Łojek, E.; Stańczak, J. Color Trails Test for Adults. A Polish Normalization; Psychological Test Laboratory of the Polish Psychological Association: Warsaw, Poland, 2012. [Google Scholar]
- Fox, C.J.; Mueller, S.T.; Gray, H.M.; Raber, J.; Piper, B.J. Evaluation of a shortform of the berg card sorting test. PLoS ONE 2013, 8, e63885. [Google Scholar] [CrossRef] [Green Version]
- Mueller, S.T.; Piper, B.J. The psychology experiment building language (PEBL) and PEBL test battery. J. Neurosci. Methods 2014, 222, 250–259. [Google Scholar] [CrossRef] [Green Version]
- Tümkaya, S.; Hancı Yenigün, E.; Topak, O.Z.; Şendur, İ.; Öztürk Atkaya, N.; Özdel, O. Is clinical insight associated with working memory components in schizophrenia and schizoaffective disorder? Turk. Psikiyatri. Derg. 2019, 30, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Tyburski, E.; Mak, M.; Samochowiec, A.; Plichta, P.; Bielecki, M.; Rek-Owodziń, K.; Podwalski, P.; Rudkowski, K.; Waszczuk, K.; Pełka-Wysiecka, J.; et al. The relationship between cingulum bundle integrity and different aspects of executive functions in chronic schizophrenia. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2020, 102, e109955. [Google Scholar] [CrossRef]
- Polgár, P.; Réthelyi, J.M.; Bálint, S.; Komlósi, S.; Czobor, P.; Bitter, I. Executive function in deficit schizophrenia: What do the dimensions of the Wisconsin card sorting test tell us? Schizophr. Res. 2010, 122, 85–93. [Google Scholar] [CrossRef]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Rzewuska, M. Validity and reliability of the Polish version of the Positive and Negative Syndrome Scale (PANSS). Int. J. Methods Psychiatr. Res. 2002, 11, 27–32. [Google Scholar] [CrossRef]
- Tatsumi, K.; Kirkpatrick, B.; Strauss, G.P.; Opler, M. The Brief Negative Symptom Scale in Translation: A Review of Psychometric Properties and Beyond. Eur. Neuropsychopharmacol. 2020, 33, 36–44. [Google Scholar] [CrossRef]
- Dollfus, S.; Mach, C.; Morello, R. Self-Evaluation of Negative Symptoms. Schizophr. Bull. 2016, 42, 571–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, R.C. Global Assessment of Functioning: A Modified Scale. Psychosomatics. 1995, 36, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Educational International: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Brzeziński, J.; Gaul, M.; Hornowska, E.; Jaworowska, A.; Machowski, A.; Zakrzewska, M. Wechsler Adult Intelligence Scale—Revised. Polish Normalization; Psychological Test Laboratory of the Polish Psychological Association: Warsaw, Poland, 2004. [Google Scholar]
- Sakia, R.M. The Box-Cox transformation technique: A review. J. R. Stat. Soc. 1992, 41, 169–178. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Streukens, S.; Leroi-Werelds, S. Bootstrapping and PLS-SEM: A step-by-step guide to get more out of your bootstrap results. Eur. Manag. Rev. 2016, 34, 618–632. [Google Scholar] [CrossRef]
- Cascella, N.G.; Testa, S.M.; Meyer, S.M.; Rao, V.A.; Diaz-Asper, C.M.; Pearlson, G.D.; Schretlen, D.J. Neuropsychological impairment in deficit vs. non-deficit schizophrenia. J. Psychiatr. Res. 2008, 42, 930–937. [Google Scholar] [CrossRef]
- Harvey, P.D.; Koren, D.; Reichenberg, A.; Bowie, C.R. Negative symptoms and cognitive deficits: What is the nature of their relationship? Schizophr. Bull. 2006, 32, 250–258. [Google Scholar] [CrossRef] [Green Version]
- Liddle, P.F.; Morris, D.L. Schizophrenic syndromes and frontal lobe performance. Br. J. Psychiatry 1991, 158, 340–345. [Google Scholar] [CrossRef]
- Brown, K.W.; White, T. Syndromes of chronic schizophrenia and some clinical correlates. Br. J. Psychiatry 1992, 161, 317–322. [Google Scholar] [CrossRef]
- Girard, R.; Météreau, E.; Thomas, J.; Pugeat, M.; Qu, C.; Dreher, J.C. Hormone therapy at early post-menopause increases cognitive control-related prefrontal activity. Sci. Rep. 2017, 7, e44917. [Google Scholar] [CrossRef] [Green Version]
- Mucci, A.; Merlotti, E.; Üçok, A.; Aleman, A.; Galderisi, S. Primary and Persistent Negative Symptoms: Concepts, Assessments and Neurobiological Bases. Schizophr. Res. 2017, 186, 19–28. [Google Scholar] [CrossRef]
- Suzuki, H.; Gen, K.; Inoue, Y.; Hibino, H.; Mikami, A.; Matsumoto, H.; Mikami, K. The influence of switching from risperidone to paliperidone on the extrapyramidal symptoms and cognitive function in elderly patients with schizophrenia: A preliminary open-label trial. Int. J. Psychiatry. Clin. Pract. 2014, 18, 58–62. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Deficit Schizophrenia Patients (DS) (n = 29) | Non-Deficit Schizophrenia Patients (NDS) (n = 44) | Healthy Controls (HC) (n = 39) | F/χ2/t | η2/V/d | |
|---|---|---|---|---|---|
| Age: M (SD) | 38.59 (6.17) | 39.27 (7.25) | 37.08 (7.94) | 0.97 c | 0.02 f |
| Years of education: M (SD) | 12.66 (3.24) i * | 13.45 (2.62) | 14.59 (2.62) | 4.15 c * | 0.07 f |
| Sex: female/male | 7/22 | 24/20 | 23/16 | 9.25 d * | 0.29 g |
| Premorbid IQ in WAIS-R-IV: | |||||
| Picture Completion: M (SD) | 17.86 (7.60)/20.52 (13.35) b,i ***, j * | 22.50 (6.19)/29.43 (13.37) b, k *** | 29.62 (3.63)/47.46 (10.34) b | 42.98 c *** | 0.44 f |
| Vocabulary: M (SD) | 33.97 (14.47) i ***, j ** | 43.07 (10.05) k *** | 56.18 (6.55) | 39.43 c *** | 0.42 f |
| Antipsychotic medications: | |||||
| Atypical: n (%) | 20 (68.97) | 28 (63.64) | - | 2.14 d | 0.17 g |
| Atypical and typical: n (%) | 8 (27.58) | 12 (27.27) | - | ||
| Typical: n (%) | 0 (0.00) | 3 (6.82) | - | ||
| No medications: n (%) | 1 (3.45) | 1 (2.27) | - | ||
| Chlorpromazine equivalent (mg): M (SD) | 695.86 (311.57) | 642.66 (313.15) | - | 0.71 e | 0.17 h |
| Duration of illness: M (SD) | 16.97 (5.73) | 14.09 (5.16) | - | 2.23 e | 0.53 h |
| Exacerbation: M (SD) | 5.69 (2.44)/1.64 (0.48) a | 6.50 (5.07)/1.65 (0.65) a | - | −0.09 e | −0.02 h |
| Global functioning in GAF: M (SD) | 50.93 (14.34) | 58.02 (14.15) | - | −2.09 e | −0.50 h |
| Psychopathological symptoms in PANSS: | |||||
| Positive symptoms: M (SD) | 7.38 (2.73)/0.53 (0.01) b | 8.14 (4.39)/0.53 (0.01) b | - | −0.10 e | −0.02 h |
| Negative symptoms: M (SD) | 22.24 (4.66)/0.59 (0.00) b | 13.80 (5.25)/0.58 (0.00) b | - | 7.39 e *** | 1.52 h |
| Disorganization: M (SD) | 12.62 (3.48)/0.54 (0.00) b | 11.45 (4.02)/0.53 (0.00) b | - | 1.90 e | 0.46 h |
| Affect: M (SD) | 8.24 (3.45)/0.53 (0.01) b | 9.25 (3.56)/0.53 (0.01) b | - | −1.59 e | −0.38 h |
| Resistance: M (SD) | 4.34 (0.61)/0.52 (0.00) b | 4.91 (2.46)/0.52 (0.01) b | - | −1.13 e | −0.25 h |
| Total score: M (SD) | 56.83 (11.17)/0.54 (0.00) b | 49.43 (14.83)/0.54 (0.00) b | - | 3.27 e * | 0.73 h |
| Negative symptoms in BNSS: | |||||
| Total score: M (SD) | 47.07 (9.28)/0.47 (0.09) b | 20.23 (12.78)/0.20 (0.13) b | - | 9.74 e *** | 2.33 h |
| Negative symptoms in SNS: | |||||
| Total score: M (SD) | 22.28 (7.38)/0.75 (0.16) b | 9.86 (6.90)/0.43 (0.19) b | - | −7.40 e *** | −1.78 h |
| Deficit Schizophrenia Patients (DS) (n = 29) | Non-Deficit Schizophrenia Patients (NDS) (n = 44) | Healthy Control (HC) (n = 39) | F | η2 | |
|---|---|---|---|---|---|
| LNST: Verbal working memory: M (SD) | 8.69 (3.95)/10.89 (3.42) a, b * | 12.14 (3.50)/12.63 (2.98) a | 15.87 (3.26)/13.68 (3.61) a | 4.29 * | 0.08 |
| SSS: Visuospatial working memory: M (SD) | 5.48 (2.29)/6.73 (2.09) a | 7.16 (2.21)/7.50 (1.83) a | 9.21 (1.74)/7.89 (2.21) a | 2.07 | 0.04 |
| MS: Planning: M (SD) | 11.62 (6.35)/2.13 (2.02) a | 13.18 (7.77)/2.09 (1.77) a, c * | 21.79 (5.05)/3.41 (2.14) a | 4.25 * | 0.07 |
| CTT: Cognitive flexibility: M (SD) | 121.93 (41.51)/4.91 (0.40) a,b *** | 109.70 (53.53)/4.90 (0.34) a, c *** | 57.10 (14.37)/4.50 (0.42) a | 10.45 *** | 0.17 |
| BCST PPE: Concept formation: M (SD) | 18.48 (10.03)/5.98 (2.62) a | 17.44 (11.82)/6.00 (2.29) a | 12.49 (5.28)/5.77 (2.77) a | 0.08 | 0.00 |
| BCST PNPE: Problem-solving: M (SD) | 15.63 (11.37)/2.88 (0.90) a | 15.27 (13.90)/2.88 (0.79) a | 8.13 (4.18)/2.51 (0.95) a | 1.68 | 0.03 |
| Deficit Schizophrenia Patients (DS) (n = 29) | Non-Deficit Schizophrenia Patients (NDS) (n = 44) | F | η2 | |
|---|---|---|---|---|
| LNST: Verbal working memory | 9.60 (3.39) a | 11.54 (3.32) a | 5.26 * | 0.07 |
| SSS: Visuospatial working memory | 6.09 (1.94) a | 6.76 (1.92) a | 1.85 | 0.03 |
| MS: Planning | 1.65 (1.78) a | 1.50 (1.72) a | 0.12 | 0.00 |
| CTT: Cognitive flexibility | 5.00 (0.43) a | 5.04 (0.40) a | 0.15 | 0.00 |
| BCST PPE: Concept formation | 6.18 (2.85) a | 6.35 (2.79) a | 0.06 | 0.00 |
| BCST PNPE: Problem-solving | 3.02 (0.92) a | 2.93 (0.86) a | 0.14 | 0.00 |
| Deficit Schizophrenia Patients (DS) (n = 29) | ||||||
|---|---|---|---|---|---|---|
| LNST: Verbal Working Memory | SSS: Visuospatial Working Memory | MS: Planning | CTT: Cognitive Flexibility | BCST PPE: Concept Formation | BCST PNPE: Problem-solving | |
| r | r | r | r | r | r | |
| Duration of illness | −0.24 | −0.11 | −0.02 | 0.18 | −0.24 | 0.00 |
| Exacerbation | −0.47 * | −0.09 | −0.46 * | 0.48 ** | 0.25 | 0.07 |
| Global functioning in GAF | 0.16 | 0.06 | 0.37 * | −0.32 | −0.19 | 0.02 |
| Chlorpromazine equivalent | −0.14 | −0.26 | −0.02 | 0.05 | 0.00 | 0.33 |
| Positive symptoms in PANSS | −0.04 | −0.02 | −0.26 | 0.28 | −0.15 | 0.16 |
| Negative symptoms in PANSS | 0.05 | −0.29 | 0.04 | 0.18 | 0.28 | −0.15 |
| Disorganization in PANSS | 0.02 | −0.05 | −0.20 | 0.21 | 0.12 | −0.20 |
| Affect in PANSS | 0.14 | −0.17 | 0.18 | −0.03 | −0.07 | −0.23 |
| Resistance in PANSS | −0.19 | −0.20 | −0.16 | 0.40 * | −0.10 | 0.24 |
| Negative symptoms in BNSS | 0.10 | 0.16 | −0.16 | 0.16 | −0.23 | −0.24 |
| Negative symptoms in SNS | −0.13 | −0.11 | −0.01 | 0.29 | −0.03 | 0.03 |
| Non-deficit schizophrenia patients (NDS) (n = 44) | ||||||
| LNST: Verbal working memory | SSS: Visuospatial working memory | MS: Planning | CTT: Cognitive flexibility | BCST PPE: Concept formation | BCST PNPE: Problem-solving | |
| r | r | r | r | r | r | |
| Duration of illness | −0.05 | −0.23 | −0.10 | −0.09 | 0.08 | 0.06 |
| Exacerbation | −0.08 | −0.25 | −0.11 | 0.08 | −0.06 | 0.00 |
| Global functioning in GAF | 0.16 | 0.02 | 0.23 | −0.25 | −0.07 | 0.10 |
| Chlorpromazine equivalent | −0.03 | −0.05 | −0.34 * | 0.18 | −0.10 | −0.10 |
| Positive symptoms in PANSS | −0.29 | −0.16 | −0.27 | 0.35 * | 0.10 | 0.07 |
| Negative symptoms in PANSS | 0.05 | 0.06 | −0.08 | 0.12 | 0.06 | −0.13 |
| Disorganization in PANSS | −0.18 | −0.18 | −0.35 * | 0.30 | 0.28 | −0.13 |
| Affect in PANSS | −0.04 | −0.20 | −0.10 | 0.09 | 0.06 | 0.03 |
| Resistance in PANSS | −0.03 | 0.03 | −0.21 | 0.12 | −0.18 | −0.19 |
| Negative symptoms in BNSS | −0.23 | −0.18 | −0.18 | 0.21 | 0.29 | −0.09 |
| Negative symptoms in SNS | −0.23 | −0.18 | −0.18 | 0.21 | 0.29 | −0.09 |
| Estimate | Lower | Upper | |
|---|---|---|---|
| Exacerbation—Verbal working memory in LNST | −0.472 ** | −0.694 | −0.172 |
| Exacerbation—Planning in MS | −0.369 | −0.704 | 0.021 |
| Exacerbation—Cognitive flexibility in CTT | 0.472 ** | 0.177 | 0.684 |
| Global functioning in GAF—Planning in MS | 0.207 | −0.209 | 0.521 |
| Resistance in PANSS—Cognitive flexibility in CTT | 0.301 | −0.038 | 0.581 |
| Estimate | Lower | Upper | |
|---|---|---|---|
| Chlorpromazine equivalent—Planning in MS | −0.265 | −0.508 | 0.107 |
| Disorganization in PANSS—Planning in MS | −0.235 | −0.524 | 0.120 |
| Positive symptoms in PANSS—Cognitive flexibility in CTT | 0.322 * | 0.036 | 0.553 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bielecki, M.; Tyburski, E.; Plichta, P.; Mak, M.; Kucharska-Mazur, J.; Podwalski, P.; Rek-Owodziń, K.; Waszczuk, K.; Sagan, L.; Mueller, S.T.; et al. Executive Functions and Psychopathology Dimensions in Deficit and Non-Deficit Schizophrenia. J. Clin. Med. 2023, 12, 1998. https://doi.org/10.3390/jcm12051998
Bielecki M, Tyburski E, Plichta P, Mak M, Kucharska-Mazur J, Podwalski P, Rek-Owodziń K, Waszczuk K, Sagan L, Mueller ST, et al. Executive Functions and Psychopathology Dimensions in Deficit and Non-Deficit Schizophrenia. Journal of Clinical Medicine. 2023; 12(5):1998. https://doi.org/10.3390/jcm12051998
Chicago/Turabian StyleBielecki, Maksymilian, Ernest Tyburski, Piotr Plichta, Monika Mak, Jolanta Kucharska-Mazur, Piotr Podwalski, Katarzyna Rek-Owodziń, Katarzyna Waszczuk, Leszek Sagan, Shane T. Mueller, and et al. 2023. "Executive Functions and Psychopathology Dimensions in Deficit and Non-Deficit Schizophrenia" Journal of Clinical Medicine 12, no. 5: 1998. https://doi.org/10.3390/jcm12051998