
Prediction of Surgical Approach in Mitral Valve Disease by XGBoost Algorithm Based on Echocardiographic Features
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Complexity and Technique Scores
2.3. Endpoint
2.4. Database Setup
2.5. Statistical Analysis
3. Results
3.1. Complexity Score and Patient Characteristics
3.2. Repair Feasibility and Surgical Outcomes
3.3. Case Example
- In the simple group, the etiology was primarily secondary annular enlargement or mitral valve prolapse in an isolated segment leading to mitral regurgitation. The most commonly used technique was annuloplasty. The coaptation area of the valve leaflets was increased to reduce or even eliminate mitral regurgitation. For example, the complexity score was 3 (2 + 1) for a patient with A1 segment prolapses, a mitral anterior leaflet cleft, no chordae tendineae rupture, and no leaflet calcification, which classified the patient in the simple group. The cleft was sutured during the operation and a mitral annuloplasty ring was placed. The surgical technique score was 2 (1 + 1). After resuscitation, the surgical effect was good and no obvious regurgitation signal was observed (Figure 7).
- The most common pathogenesis in the intermediate group was mitral valve prolapse involving multiple segments, with or without ruptured chordae tendineae. Mitral valve prolapses most often involved the posterior leaflet, specifically the P2 segment [17,19,22]. A patient with mitral valve prolapses involving the A1, A2, and A3 segments but no rupture of chordae tendineae had a complexity score of 7 (3 × 2 + 1) and a surgical technique score of 5 (2 × 1 + 1). The prolapsed leaflets were processed to reconstruct the artificial chordae tendineae and suture the sector junction to provide enough support when the leaflets were closed, thus increasing the coaptation area to reduce regurgitation (Figure 8).
- Patients in the complex group had a variety of etiologies, including multiple segmental mitral valve prolapse (12.5%), Barlow’s syndrome (7.1%), infective endocarditis (12.5%), and rheumatic valvular heart disease (67.9%). The proportion of patients with each of the three less common etiologies was essentially the same. These diseases not only involve a wide range of lesions but are also accompanied by changes in valve morphology and structure, which increases the difficulty of surgery. Preoperative evaluation of the lesion is also a challenge for echocardiologists. A patient with preoperative suspicion of Barlow’s syndrome exhibited prolapse involving the A2 and A3 segments and posteromedial commissure, accompanied by redundant valve leaflets. The complexity score was 9 (2 × 2 + 2 + 3). Two artificial chordae tendineae were implanted in each of the A2 and A3 segments and a mitral annuloplasty ring was placed. The surgical technique score was 5 (4 × 1 + 1) and the surgical effect was good (Figure 9).
- The fourth case was an unsuccessful mitral valve repair that was converted to mitral valve replacement (Figure 10). The patient had rheumatic valvular disease, with thickened leaflets, restricted leaflet mobility, thickened and shortened sub-valvular chordae tendineae, and commissural fusion observed on three-dimensional images. The complexity score was 8 (1 + 3 + 2 + 2). According to the surgeon’s experience, mitral valve repair was expected to be performed, but the surgical effect was not satisfactory and the patient required a second bypass run. After resuscitation, the intraoperative TEE examination showed that the function of the artificial valve was good.
3.4. Prediction of a Surgical Approach Based on Complexity Score
3.5. XGBoost Model Accuracy and Confusion Matrix
3.6. Feature Importance
4. Discussion
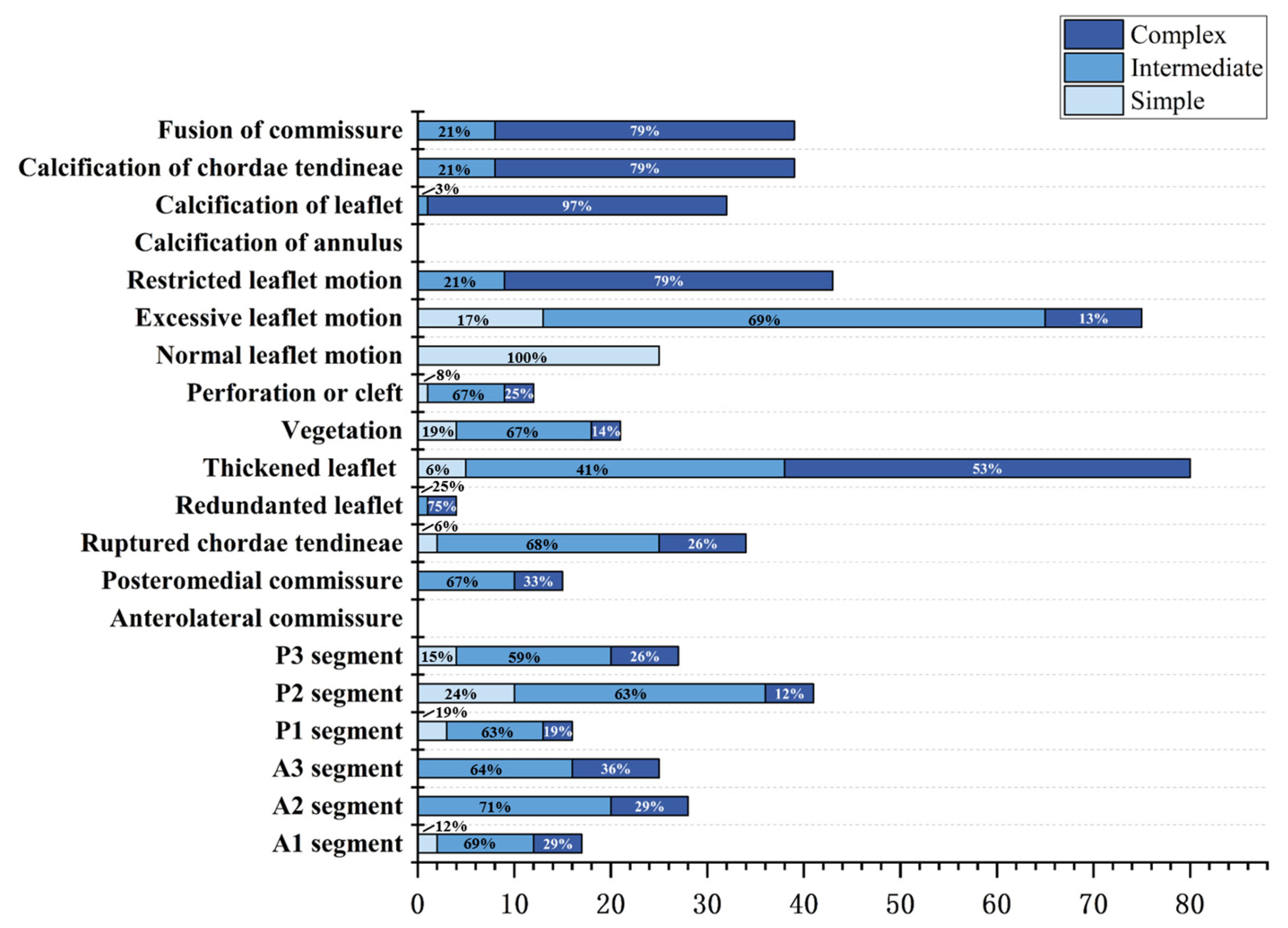
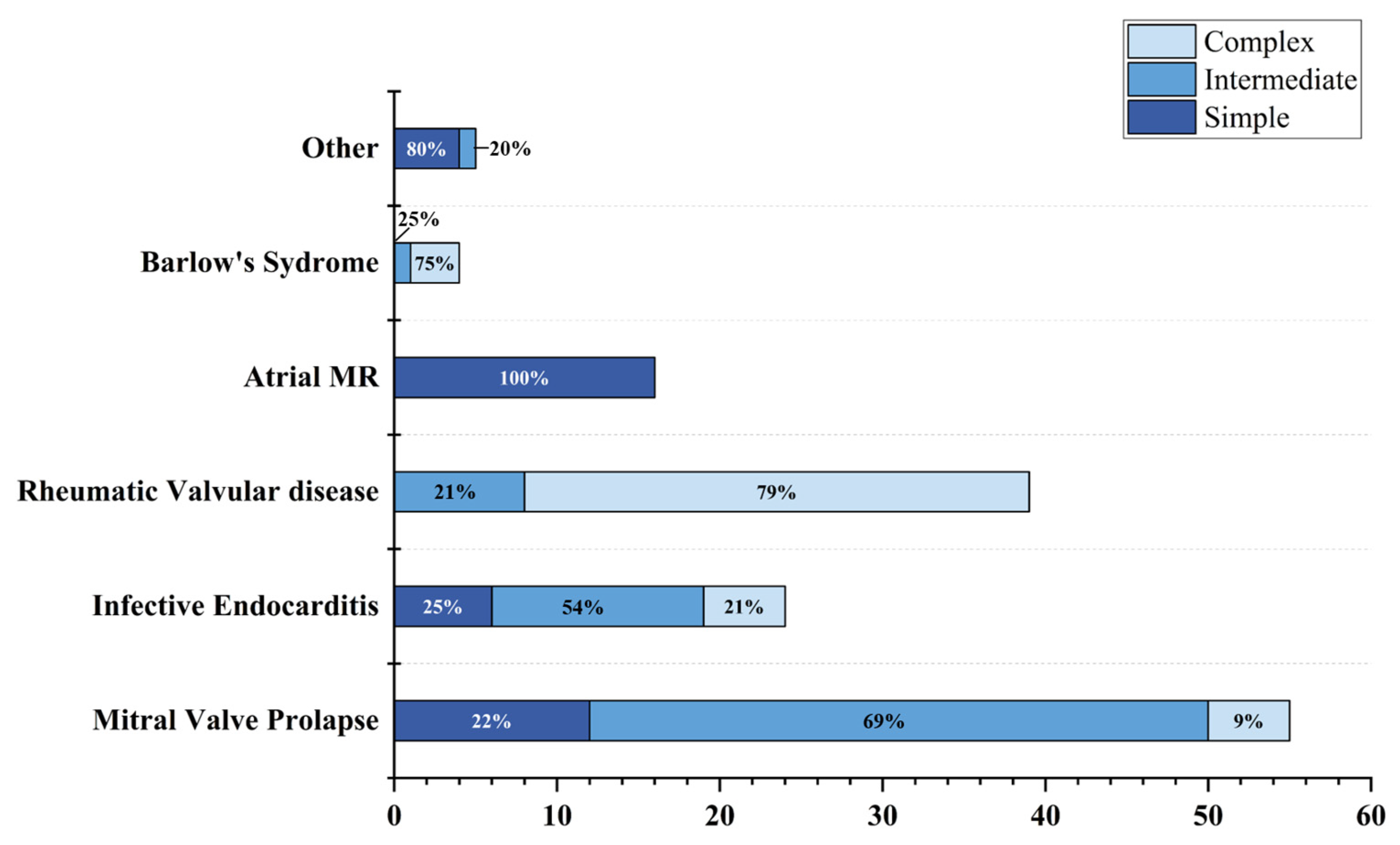
4.1. Proportion of Disease Components
4.2. Correlation between the Complexity Score and Surgical Technique Score
4.3. Advantages of Building a Prediction Model for Surgical Approach Based on the XGBoost Algorithm
5. Conclusions
6. Limitation and Strengths
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El Sabbagh, A.; Reddy, Y.N.V.; Nishimura, R.A. Mitral Valve Regurgitation in the Contemporary Era: Insights Into Diagnosis, Management, and Future Directions. JACC Cardiovasc. Imaging 2018, 11, 628–643. [Google Scholar] [CrossRef]
- Iung, B.; Delgado, V.; Rosenhek, R.; Price, S.; Prendergast, B.; Wendler, O.; De Bonis, M.; Tribouilloy, C.; Evangelista, A.; Bogachev-Prokophiev, A.; et al. Contemporary Presentation and Management of Valvular Heart Disease: The EURObservational Research Programme Valvular Heart Disease II Survey. Circulation 2019, 140, 1156–1169. [Google Scholar] [CrossRef]
- Coffey, S.; Roberts-Thomson, R.; Brown, A.; Carapetis, J.; Chen, M.; Enriquez-Sarano, M.; Zuhlke, L.; Prendergast, B.D. Global epidemiology of valvular heart disease. Nat. Rev. Cardiol. 2021, 18, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e1159–e1195. [Google Scholar] [CrossRef]
- Lawrie, G.M. Surgical treatment of mitral regurgitation. Curr. Opin. Cardiol. 2020, 35, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Lazam, S.; Vanoverschelde, J.L.; Tribouilloy, C.; Grigioni, F.; Suri, R.M.; Avierinos, J.F.; de Meester, C.; Barbieri, A.; Rusinaru, D.; Russo, A.; et al. Twenty-Year Outcome After Mitral Repair Versus Replacement for Severe Degenerative Mitral Regurgitation: Analysis of a Large, Prospective, Multicenter, International Registry. Circulation 2017, 135, 410–422. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.C.; Jang, M.J.; Hwang, H.Y. Meta-Analysis Comparing Mitral Valve Repair Versus Replacement for Degenerative Mitral Regurgitation Across All Ages. Am. J. Cardiol. 2019, 123, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Munoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef]
- Bolling, S.F.; Li, S.; O’Brien, S.M.; Brennan, J.M.; Prager, R.L.; Gammie, J.S. Predictors of mitral valve repair: Clinical and surgeon factors. Ann. Thorac. Surg. 2010, 90, 1904–1911; discussion 1912. [Google Scholar] [CrossRef]
- Trumello, C.; Giambuzzi, I.; Bonalumi, G.; Bargagna, M.; Naliato, M.; Ruggeri, S.; Fileccia, D.; Castiglioni, A.; Alfieri, O.; Alamanni, F.; et al. Rheumatic mitral regurgitation: Is repair justified by the long-term results? Interact. Cardiovasc. Thorac. Surg. 2021, 33, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, G.F.; Antunes, M.J. Mitral valve repair for degenerative mitral valve disease: Surgical approach, patient selection and long-term outcomes. Heart 2017, 103, 1663–1669. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Zou, Y.; Liu, J.; Wang, Y.; Chen, Y.; Sun, F.; Yang, Z.; Cui, G.; Zhu, X.; Cui, X.; et al. Ultrasound-based radiomics XGBoost model to assess the risk of central cervical lymph node metastasis in patients with papillary thyroid carcinoma: Individual application of SHAP. Front. Oncol. 2022, 12, 897596. [Google Scholar] [CrossRef] [PubMed]
- Kadiyala, A.; Kumar, A. Applications of python to evaluate the performance of decision tree-based boosting algorithms. Environ. Prog. Sustain. Energy 2018, 37, 618–623. [Google Scholar] [CrossRef]
- Hu, B.; Wang, C.; Jiang, K.; Shen, Z.; Yang, X.; Yin, M.; Liang, B.; Xie, Q.; Ye, Y.; Gao, Z. Development and validation of a novel diagnostic model for initially clinical diagnosed gastrointestinal stromal tumors using an extreme gradient-boosting machine. BMC Gastroenterol. 2021, 21, 481. [Google Scholar] [CrossRef] [PubMed]
- Anyanwu, A.C.; Itagaki, S.; Chikwe, J.; El-Eshmawi, A.; Adams, D.H. A complexity scoring system for degenerative mitral valve repair. J. Thorac. Cardiovasc. Surg. 2016, 151, 1661–1670. [Google Scholar] [CrossRef]
- Althunayyan, A.; Petersen, S.E.; Lloyd, G.; Bhattacharyya, S. Mitral valve prolapse. Expert Rev. Cardiovasc. Ther. 2019, 17, 43–51. [Google Scholar] [CrossRef]
- Gheorghe, L.L.; Mobasseri, S.; Agricola, E.; Wang, D.D.; Milla, F.; Swaans, M.; Pandis, D.; Adams, D.H.; Yadav, P.; Sievert, H.; et al. Imaging for Native Mitral Valve Surgical and Transcatheter Interventions. JACC Cardiovasc. Imaging 2021, 14, 112–127. [Google Scholar] [CrossRef]
- Wunderlich, N.C.; Dalvi, B.; Ho, S.Y.; Kux, H.; Siegel, R.J. Rheumatic Mitral Valve Stenosis: Diagnosis and Treatment Options. Curr. Cardiol. Rep. 2019, 21, 14. [Google Scholar] [CrossRef]
- Passos, L.S.A.; Nunes, M.C.P.; Aikawa, E. Rheumatic Heart Valve Disease Pathophysiology and Underlying Mechanisms. Front Cardiovasc. Med. 2020, 7, 612716. [Google Scholar] [CrossRef] [PubMed]
- Padang, R.; Enriquez-Sarano, M.; Pislaru, S.V.; Maalouf, J.F.; Nkomo, V.T.; Mankad, S.V.; Maltais, S.; Suri, R.M.; Schaff, H.V.; Michelena, H.I. Coexistent bicuspid aortic valve and mitral valve prolapse: Epidemiology, phenotypic spectrum, and clinical implications. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 677–686. [Google Scholar] [CrossRef]
- Suri, R.M.; Clavel, M.A.; Schaff, H.V.; Michelena, H.I.; Huebner, M.; Nishimura, R.A.; Enriquez-Sarano, M. Effect of Recurrent Mitral Regurgitation Following Degenerative Mitral Valve Repair: Long-Term Analysis of Competing Outcomes. J. Am. Coll. Cardiol. 2016, 67, 488–498. [Google Scholar] [CrossRef] [PubMed]
- Javadikasgari, H.; Mihaljevic, T.; Suri, R.M.; Svensson, L.G.; Navia, J.L.; Wang, R.Z.; Tappuni, B.; Lowry, A.M.; McCurry, K.R.; Blackstone, E.H.; et al. Simple versus complex degenerative mitral valve disease. J. Thorac. Cardiovasc. Surg. 2018, 156, 122–129.e16. [Google Scholar] [CrossRef] [PubMed]
- Karthikeyan, A.; Garg, A.; Vinod, P.K.; Priyakumar, U.D. Machine Learning Based Clinical Decision Support System for Early COVID-19 Mortality Prediction. Front. Public Health 2021, 9, 626697. [Google Scholar] [CrossRef] [PubMed]
- Okada, Y.; Nakai, T.; Kitai, T. Role of Mitral Valve Repair for Mitral Infective Endocarditis. Cardiol. Clin. 2021, 39, 189–196. [Google Scholar] [CrossRef]
- Mestres, C.A.; Fita, G.; Azqueta, M.; Miro, J.M. Role of echocardiogram in decision making for surgery in endocarditis. Curr. Infect. Dis. Rep. 2010, 12, 321–328. [Google Scholar] [CrossRef]
- David, T.E. Perspectives on surgical treatment of mitral valve disease. Asian Cardiovasc. Thorac. Ann. 2020, 28, 360–365. [Google Scholar] [CrossRef]
- Fishbein, G.A.; Fishbein, M.C. Mitral Valve Pathology. Curr. Cardiol. Rep. 2019, 21, 61. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Complexity Variable | Weight |
|---|---|
| Prolapse segments | |
| P1 segment | 1 |
| P2 segment | 1 |
| P3 segment | 1 |
| A1 segment | 2 |
| A2 segment | 2 |
| A3 segment | 2 |
| Anterolateral commissure | 2 |
| Posteromedial commissure | 2 |
| Ruptured chordae tendineae | 1 |
| Leaflet morphology | |
| Normal | 0 |
| Thickening | 1 |
| Redundant | 3 |
| Calcification | |
| Leaflet | 1 |
| Annulus | 3 |
| Chordae tendineae | 3 |
| Fusion of commissure | 2 |
| Perforation or Cleft | |
| 1 | 1 |
| ≥2 | 2 |
| Vegetation | |
| 1 | 1 |
| ≥2 | 2 |
| Leaflet Motion | |
| Normal | 0 |
| Excessive | 1 |
| Restriction | 2 |
| Reference Variable | Class | Detailed Parameters |
|---|---|---|
| Effective variables | ||
| Ruptured chordae tendineae | 2 | Yes; No |
| Leaflet morphology | 3 | Normal; Thickening; Redundant |
| Leaflet motion | 2 | Normal; Hypermobility; Restriction |
| Vegetation | 3 | 0; 1; ≥2 |
| Perforation or Cleft | 3 | 0; 1; ≥2 |
| Calcification | 4 | Annulus; Leaflet, Chordae tendineae; Fusion of commissure |
| Uncertain variables | ||
| Prolapsed segments | 8 | P1 segment; P2 segment; P3 segment; A1 segment; A2 segment; A3 segment; Anterolateral commissure; Posteromedial commissure |
| Ineffective variables | ||
| Sex | 2 | Man; Female |
| Age | - | - |
| Diagnosis | 6 | Mitral valve prolapses; Barlow’s syndrome; Rheumatic heart valve disease; Infective endocarditis; Atrial mitral regurgitation and other causes of mitral valve regurgitation or stenosis |
| Variable | Simple (Score: 1–4) (n = 38) | Intermediate (Score: 5–8) n = 61 | Complex (Score: ≥9) n = 44 |
|---|---|---|---|
| Sex | |||
| Male | 23 (60.5) | 41 (67.2) | 24 (54.5) |
| Female | 15 (39.5) | 20 (32.8) | 20 (45.5) |
| Surgical Approach | |||
| Mitral Valve Repair | 33 (86.8) | 45 (73.8) | 9 (20.5) |
| Mitral Valve Replacement | 5 (13.2) | 16 (26.2) | 36 (79.5) |
| Diagnosis | |||
| Mitral Valve Prolapse | 12 (31.6) | 38 (62.3) | 5 (11.4) |
| Infective Endocarditis | 6 (15.8) | 13 (21.3) | 5 (11.4) |
| Rheumatic Heart Disease | 0 | 8 (13.1) | 31 (70.5) |
| Atrial mitral regurgitation | 16 (42.1) | 0 | 0 |
| Barlow’s Syndrome | 0 | 1 (1.6) | 3 (6.8) |
| Others | 4 (10.5) | 1 (1.6) | 0 |
| Prolapsed segments | |||
| A1 segment | 2 (5.3) | 10 (16.4) | 5 (11.4) |
| A2 segment | 0 | 20 (32.8) | 8 (18.2) |
| A3 segment | 0 | 16 (26.2) | 9 (20.5) |
| P1 segment | 3 (7.9) | 10 (16.4) | 3 (6.8) |
| P2 segment | 10 (26.3) | 26 (42.6) | 5 (11.4) |
| P3 segment | 4 (10.5) | 16 (26.2) | 7 (15.9) |
| Anterolateral commissure | 0 | 0 | 0 |
| Posteromedial commissure | 0 | 10 (16.4) | 5 (11.4) |
| Ruptured chordae tendineae | |||
| No | 36 (94.7) | 38 (62.2) | 35 (79.6) |
| Yes | 2 (5.3) | 23 (37.8) | 9 (20.4) |
| Leaflet morpholopy | |||
| Normal | 33 (86.8) | 27 (44.3) | 0 |
| Redundant | 0 | 1 (1.6) | 3 (4.5) |
| Thickening | 5 (13.2) | 33 (54.1) | 42 (95.5) |
| Leaflet motion | |||
| Normal | 25 (65.8) | 0 | 0 |
| Excessive | 13 (34.2) | 52 (85.2) | 10 (22.7) |
| Restriction | 0 | 9 (14.8) | 34 (77.3) |
| Vegetation | |||
| 0 | 34 (89.5) | 47 (77.0) | 41 (93.2) |
| 1 | 4 (10.5) | 10 (16.4) | 2 (4.5) |
| ≥2 | 0 | 4 (6.6) | 1 (2.3) |
| Perforation or Cleft | |||
| 0 | 37 (97.4) | 53 (86.9) | 41 (93.2) |
| 1 | 1 (2.6) | 7 (11.5) | 1 (2.3) |
| ≥2 | 0 | 1 (1.6) | 2 (4.5) |
| Calcification | |||
| Annulus | 0 | 0 | 0 |
| Leaflet | 0 | 1 (1.6) | 31 (70.5) |
| Chordae tendineae | 0 | 8 (13.1) | 31 (70.5) |
| Fusion of Commissure | 0 | 8 (13.1) | 31 (70.5) |
| Endpoint | Simple (n = 38) | Intermediate (n = 61) | Complex (n = 44) |
|---|---|---|---|
| Mitral valve repair | 33 | 45 | 9 |
| Mitral valve replacement | 5 | 16 | 35 |
| Unsuccessful repair | 4 | 6 | 5 |
| Diverted to mitral valve replacement | 3 | 4 | 4 |
| More than mild regurgitation during follow-up | 1 | 2 | 1 |
| AUC | Cut-Off Value | 1-Specificity | Sensitivity | True Positive | True Negative | False Negative |
|---|---|---|---|---|---|---|
| 0.75 | 8.5 | 0.33 | 0.73 | 0.73 | 0.67 | 0.33 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, X.; Chen, L.; Zhang, D.; Luo, S.; Sheng, Y.; Liu, X.; Liu, Q.; Li, J.; Shi, B.; Peng, G.; et al. Prediction of Surgical Approach in Mitral Valve Disease by XGBoost Algorithm Based on Echocardiographic Features. J. Clin. Med. 2023, 12, 1193. https://doi.org/10.3390/jcm12031193
Lin X, Chen L, Zhang D, Luo S, Sheng Y, Liu X, Liu Q, Li J, Shi B, Peng G, et al. Prediction of Surgical Approach in Mitral Valve Disease by XGBoost Algorithm Based on Echocardiographic Features. Journal of Clinical Medicine. 2023; 12(3):1193. https://doi.org/10.3390/jcm12031193
Chicago/Turabian StyleLin, Xiaoxuan, Lixin Chen, Defu Zhang, Shuyu Luo, Yuanyuan Sheng, Xiaohua Liu, Qian Liu, Jian Li, Bobo Shi, Guijuan Peng, and et al. 2023. "Prediction of Surgical Approach in Mitral Valve Disease by XGBoost Algorithm Based on Echocardiographic Features" Journal of Clinical Medicine 12, no. 3: 1193. https://doi.org/10.3390/jcm12031193