
Maternal Mental Health Care Matters: The Impact of Prenatal Depressive and Anxious Symptoms on Child Emotional and Behavioural Trajectories in the French EDEN Cohort
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
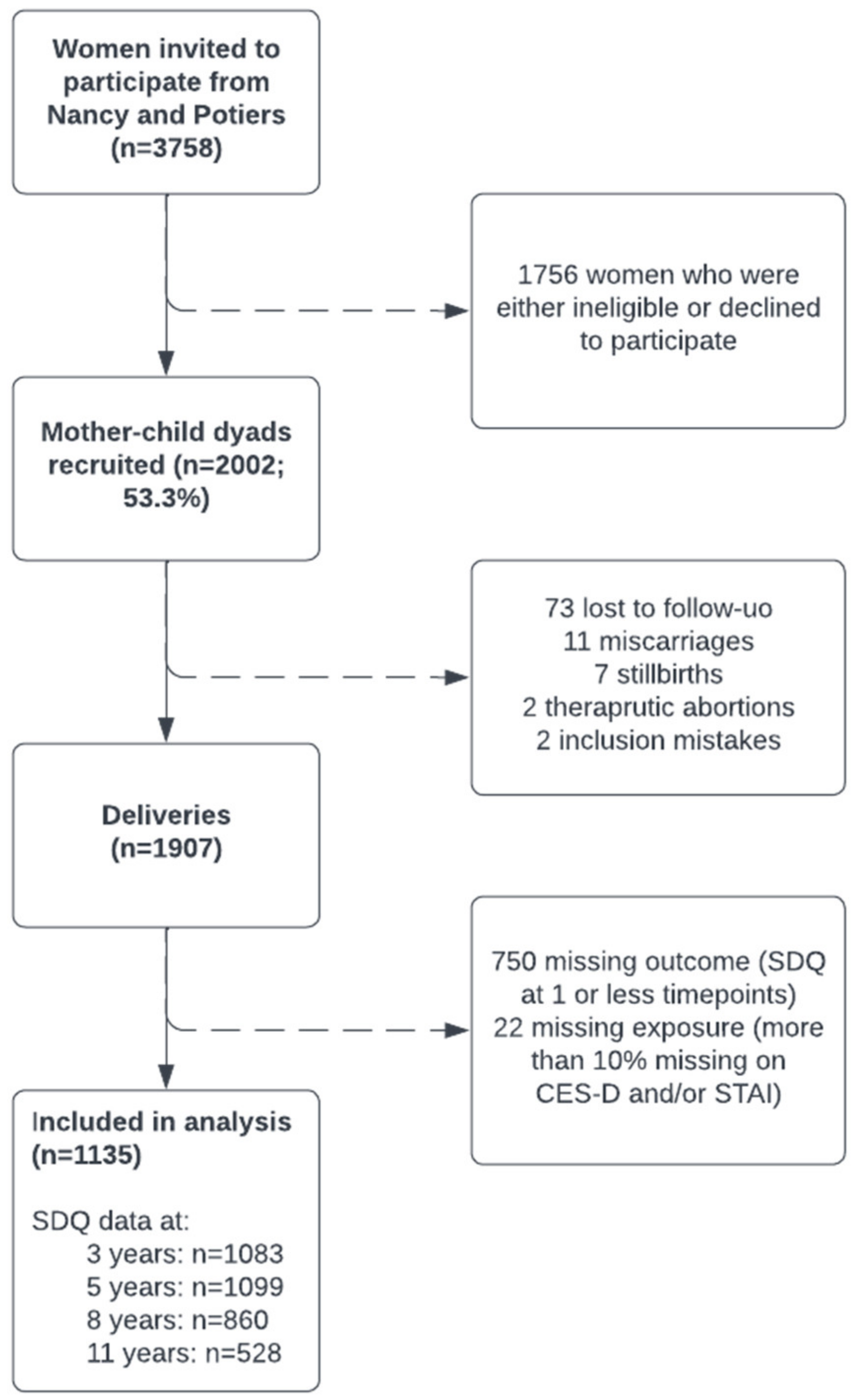
2.1. The EDEN Cohort
2.2. Variables
2.2.1. Maternal Prenatal Depression and Anxiety
2.2.2. Children’s Emotional and Behavioural Characteristics
2.2.3. Prenatal Mental Health Consultations
2.2.4. Covariates
2.3. Statistical Methods
3. Results
3.1. Description of the Study Population
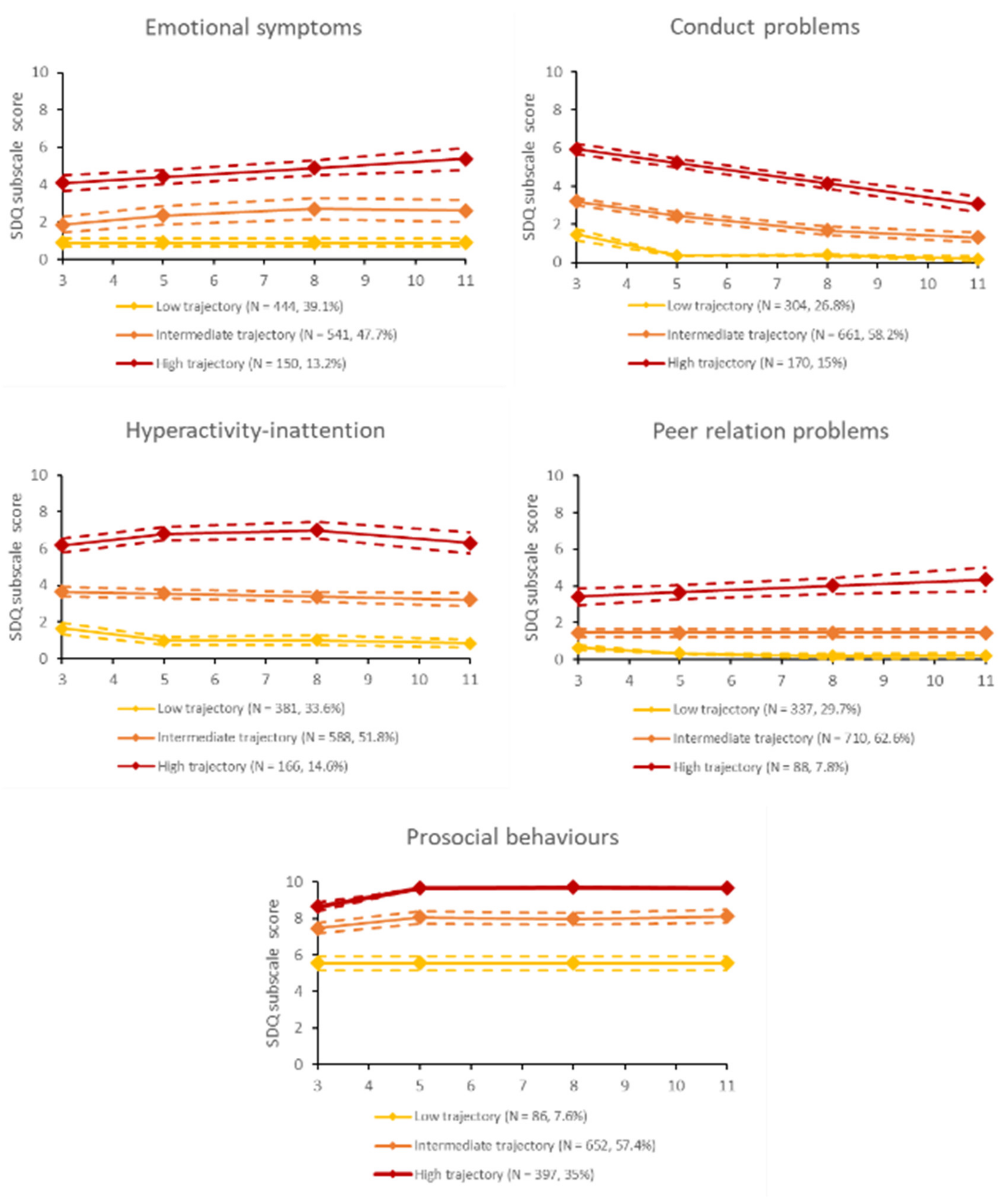
3.2. Child Emotional and Behavioural Trajectories
3.3. Prenatal Depression and Anxiety and Child Trajectories
3.4. Stratification by Prenatal Consultations with a Psychologist or Psychiatrist
3.4.1. Women Who Did Not Report Prenatal Consultations
3.4.2. Women Who Reported Prenatal Consultations
4. Discussion
4.1. Child Trajectories of Emotional and Behavioural Problems
4.2. Associations between Prenatal Mental Health and Child Outcomes
4.3. Prenatal Consultation of a Psychologist or Psychiatrist
4.4. Strengths and Limitations
4.5. Recommendations for Research and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dennis, C.-L.; Falah-Hassani, K.; Shiri, R. Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 210, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Bennett, H.A.; Einarson, A.; Taddio, A.; Koren, G.; Einarson, T.R. Prevalence of depression during pregnancy: Systematic review. Obstet. Gynecol. 2004, 103, 698–709. [Google Scholar] [CrossRef] [PubMed]
- Dadi, A.F.; Miller, E.R.; Bisetegn, T.A.; Mwanri, L. Global burden of antenatal depression and its association with adverse birth outcomes: An umbrella review. BMC Public Health 2020, 20, 173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalifeh, H.; Hunt, I.M.; Appleby, L.; Howard, L.M. Suicide in perinatal and non-perinatal women in contact with psychiatric services: 15 year findings from a UK national inquiry. Lancet Psychiatry 2016, 3, 233–242. [Google Scholar] [CrossRef]
- Field, T. Prenatal depression risk factors, developmental effects and interventions: A review. J. Pregnancy Child Health 2017, 4, 301. [Google Scholar] [CrossRef]
- Suri, R.; Lin, A.S.; Cohen, L.S.; Altshuler, L.L. Acute and long-term behavioral outcome of infants and children exposed in utero to either maternal depression or antidepressants: A review of the literature. J. Clin. Psychiatry 2014, 75, e1142–e1152. [Google Scholar] [CrossRef]
- Grigoriadis, S.; Graves, L.; Peer, M.; Mamisashvili, L.; Tomlinson, G.; Vigod, S.N.; Dennis, C.L.; Steiner, M.; Brown, C.; Cheung, A.; et al. Maternal Anxiety During Pregnancy and the Association With Adverse Perinatal Outcomes: Systematic Review and Meta-Analysis. J. Clin Psychiatry 2018, 79, 17r12011. [Google Scholar] [CrossRef] [Green Version]
- Barker, D.J. The origins of the developmental origins theory. J. Intern. Med. 2007, 261, 412–417. [Google Scholar] [CrossRef]
- Hentges, R.F.; Graham, S.A.; Plamondon, A.; Tough, S.; Madigan, S. A developmental cascade from prenatal stress to child internalizing and externalizing problems. J. Pediatr. Psychol. 2019, 44, 1057–1067. [Google Scholar] [CrossRef]
- Wolford, E.; Lahti, M.; Tuovinen, S.; Lahti, J.; Lipsanen, J.; Savolainen, K.; Heinonen, K.; Hämäläinen, E.; Kajantie, E.; Pesonen, A.K.; et al. Maternal depressive symptoms during and after pregnancy are associated with attention-deficit/hyperactivity disorder symptoms in their 3- to 6-year-old children. PLoS ONE 2017, 12, e0190248. [Google Scholar] [CrossRef]
- Irwin, J.L.; Davis, E.P.; Hobel, C.J.; Coussons-Read, M.; Schetter, C.D. Maternal prenatal anxiety trajectories and infant developmental outcomes in one-year-old offspring. Infant Behav. Dev. 2020, 60, 101468. [Google Scholar] [CrossRef] [PubMed]
- Van den Bergh, B.R.; van den Heuvel, M.I.; Lahti, M.; Braeken, M.; de Rooij, S.R.; Entringer, S.; Hoyer, D.; Roseboom, T.; Räikkönen, K.; King, S.; et al. Prenatal developmental origins of behavior and mental health: The influence of maternal stress in pregnancy. Neurosci. Biobehav. Rev. 2020, 117, 26–64. [Google Scholar] [CrossRef] [Green Version]
- Field, T.; Diego, M.; Hernandez-Reif, M. Prenatal depression effects and interventions: A review. Infant Behav. Dev. 2010, 33, 409–418. [Google Scholar] [CrossRef] [Green Version]
- Reef, J.; Diamantopoulou, S.; van Meurs, I.; Verhulst, F.C.; van der Ende, J. Developmental trajectories of child to adolescent externalizing behavior and adult DSM-IV disorder: Results of a 24-year longitudinal study. Soc. Psychiatry Psychiatr. Epidemiol. 2011, 46, 1233–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKinnon, N.; Kingsbury, M.; Mahedy, L.; Evans, J.; Colman, I. The association between prenatal stress and externalizing symptoms in childhood: Evidence from the avon longitudinal study of parents and children. Biol. Psychiatry 2018, 83, 100–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’donnell, K.J.; Glover, V.; Barker, E.D.; O’connor, T.G. The persisting effect of maternal mood in pregnancy on childhood psychopathology. Dev. Psychopathol. 2014, 26, 393–403. [Google Scholar] [CrossRef] [Green Version]
- Field, T. Prenatal depression effects on early development: A review. Infant Behav. Dev. 2011, 34, 1–14. [Google Scholar] [CrossRef]
- Rogers, A.; Obst, S.; Teague, S.J.; Rossen, L.; Spry, E.A.; Macdonald, J.A.; Sunderland, M.; Olsson, C.A.; Youssef, G.; Hutchinson, D. Association between maternal perinatal depression and anxiety and child and adolescent development: A meta-analysis. JAMA Pediatr. 2020, 174, 1082–1092. [Google Scholar] [CrossRef]
- Van Ravesteyn, L.M.; Lambregtse-van den Berg, M.P.; Hoogendijk, W.J.; Kamperman, A.M. Interventions to treat mental disorders during pregnancy: A systematic review and multiple treatment meta-analysis. PLoS ONE 2017, 12, e0173397. [Google Scholar] [CrossRef] [Green Version]
- Battle, C.L.; Salisbury, A.L.; Schofield, C.A.; Ortiz-Hernandez, S. Perinatal antidepressant use: Understanding women’s preferences and concerns. J. Psychiatr. Pract. 2013, 19, 443. [Google Scholar] [CrossRef]
- Glasheen, C.; Richardson, G.A.; Fabio, A. A systematic review of the effects of postnatal maternal anxiety on children. Arch. Women’s Ment. Health 2010, 13, 61–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsivos, Z.-L.; Calam, R.; Sanders, M.R.; Wittkowski, A. Interventions for postnatal depression assessing the mother–infant relationship and child developmental outcomes: A systematic review. Int. J. Women’s Health 2015, 7, 429. [Google Scholar]
- Poobalan, A.S.; Aucott, L.S.; Ross, L.; Smith, W.C.S.; Helms, P.J.; Williams, J.H. Effects of treating postnatal depression on mother-infant interaction and child development: Systematic review. Br. J. Psychiatry 2007, 191, 378–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayden, T.; Perantie, D.C.; Nix, B.D.; Barnes, L.D.; Mostello, D.J.; Holcomb, W.L.; Svrakic, D.M.; Scherrer, J.F.; Lustman, P.J.; Hershey, T. Treating prepartum depression to improve infant developmental outcomes: A study of diabetes in pregnancy. J. Clin. Psychol. Med. Settings 2012, 19, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Milgrom, J.; Holt, C.; Holt, C.J.; Ross, J.; Ericksen, J.; Gemmill, A.W. Feasibility study and pilot randomised trial of an antenatal depression treatment with infant follow-up. Arch. Women’s Ment. Health 2015, 18, 717–730. [Google Scholar] [CrossRef]
- Bleker, L.S.; Milgrom, J.; Sexton-Oates, A.; Parker, D.; Roseboom, T.J.; Gemmill, A.W.; Holt, C.J.; Saffery, R.; Connelly, A.; Burger, H.; et al. Cognitive behavioral therapy for antenatal depression in a pilot randomized controlled trial and effects on neurobiological, behavioral and cognitive outcomes in offspring 3–7 Years Postpartum: A perspective article on study findings, limitations and future aims. Front. Psychiatry 2020, 11, 34. [Google Scholar]
- Forman, D.R.; O’Hara, M.W.; Stuart, S.; Gorman, L.L.; Larsen, K.E.; Coy, K.C. Effective treatment for postpartum depression is not sufficient to improve the developing mother–child relationship. Dev. Psychopathol. 2007, 19, 585–602. [Google Scholar] [CrossRef]
- Tearne, J.E.; Allen, K.L.; Herbison, C.E.; Lawrence, D.; Whitehouse, A.J.; Sawyer, M.G.; Robinson, M. The association between prenatal environment and children’s mental health trajectories from 2 to 14 years. Eur. Child Adolesc. Psychiatry 2015, 24, 1015–1024. [Google Scholar] [CrossRef]
- Shore, L.; Toumbourou, J.W.; Lewis, A.J.; Kremer, P. Longitudinal trajectories of child and adolescent depressive symptoms and their predictors–a systematic review and meta-analysis. Child Adolesc. Ment. Health 2018, 23, 107–120. [Google Scholar] [CrossRef]
- Heude, B.; Forhan, A.; Slama, R.; Douhaud, L.; Bedel, S.; Saurel-Cubizolles, M.-J.; Hankard, R.; Thiebaugeorges, O.; De Agostini, M.; Annesi-Maesano, I.; et al. Cohort Profile: The EDEN mother-child cohort on the prenatal and early postnatal determinants of child health and development. Int. J. Epidemiol. 2015, 45, 353–363. [Google Scholar] [CrossRef] [Green Version]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Nast, I.; Bolten, M.; Meinlschmidt, G.; Hellhammer, D.H. How to measure prenatal stress? A systematic review of psychometric instruments to assess psychosocial stress during pregnancy. Paediatr. Perinat. Epidemiol. 2013, 27, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. Psychometric properties of the strengths and difficulties questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Muris, P.; Meesters, C.; van den Berg, F. The strengths and difficulties questionnaire (SDQ). Eur. Child Adolesc. Psychiatry 2003, 12, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Brookhart, M.A.; Schneeweiss, S.; Rothman, K.J.; Glynn, R.J.; Avorn, J.; Stürmer, T. Variable selection for propensity score models. Am. J. Epidemiol. 2006, 163, 1149–1156. [Google Scholar] [CrossRef] [Green Version]
- Chesnaye, N.C.; Stel, V.S.; Tripepi, G.; Dekker, F.W.; Fu, E.L.; Zoccali, C.; Jager, K.J. An introduction to inverse probability of treatment weighting in observational research. Clin. Kidney J. 2022, 15, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Jager, K.; Zoccali, C.; Macleod, A.; Dekker, F. Confounding: What it is and how to deal with it. Kidney Int. 2008, 73, 256–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodner, T.E. What improves with increased missing data imputations? Struct. Equ. Model. Multidiscip. J. 2008, 15, 651–675. [Google Scholar] [CrossRef]
- Cepeda, M.S.; Boston, R.; Farrar, J.T.; Strom, B.L. Comparison of logistic regression versus propensity score when the number of events is low and there are multiple confounders. Am. J. Epidemiol. 2003, 158, 280–287. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.-L.; Collins, G.S.; Spence, J.; Daurès, J.-P.; Devereaux, P.; Landais, P.; Le Manach, Y. Double-adjustment in propensity score matching analysis: Choosing a threshold for considering residual imbalance. BMC Med. Res. Methodol. 2017, 17, 78. [Google Scholar] [CrossRef] [Green Version]
- Xu, S.; Ross, C.; Raebel, M.A.; Shetterly, S.; Blanchette, C.; Smith, D. Use of stabilized inverse propensity scores as weights to directly estimate relative risk and its confidence intervals. Value Health 2010, 13, 273–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The World Health Report 2001: Mental Health: New Understanding, New Hope; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Beyer, T.; Postert, C.; Müller, J.M.; Furniss, T. Prognosis and continuity of child mental health problems from preschool to primary school: Results of a four-year longitudinal study. Child Psychiatry Hum. Dev. 2012, 43, 533–543. [Google Scholar] [CrossRef]
- Capron, C.; Thérond, C.; Duyme, M. Psychometric properties of the French version of the self-report and teacher Strengths and Difficulties Questionnaire (SDQ). Eur. J. Psychol. Assess. 2007, 23, 79–88. [Google Scholar] [CrossRef]
- Fekom, M.; Bonello, K.; Gomajee, R.; Ibanez, G.; Martin, S.; Keyes, K.; Nakamura, A.; Lepeule, J.; Strandberg-Larsen, K.; Melchior, M. Smoking during pregnancy and children’s emotional and behavioural trajectories. Eur. J. Public Health 2022, 32, ckac129.669. [Google Scholar] [CrossRef]
- Galéra, C.; Heude, B.; Forhan, A.; Bernard, J.Y.; Peyre, H.; Van der Waerden, J.; Pryor, L.; Bouvard, M.P.; Melchior, M.; Lioret, S. Prenatal diet and children’s trajectories of hyperactivity–inattention and conduct problems from 3 to 8 years: The EDEN mother–child cohort. J. Child Psychol. Psychiatry 2018, 59, 1003–1011. [Google Scholar] [CrossRef] [PubMed]
- Gomajee, R.; El-Khoury, F.; Côté, S.; van der Waerden, J.; Pryor, L.; Melchior, M. Early childcare type predicts children’s emotional and behavioural trajectories into middle childhood. Data from the EDEN mother–child cohort study. J. Epidemiol Community Health 2018, 72, 1033–1043. [Google Scholar] [CrossRef] [PubMed]
- López-Romero, L.; Romero, E.; Andershed, H. Conduct problems in childhood and adolescence: Developmental trajectories, predictors and outcomes in a six-year follow up. Child Psychiatry Hum. Dev. 2015, 46, 762–773. [Google Scholar] [CrossRef] [PubMed]
- Korhonen, M.; Luoma, I.; Salmelin, R.K.; Helminen, M.; Kaltiala-Heino, R.; Tamminen, T. The trajectories of child’s internalizing and externalizing problems, social competence and adolescent self-reported problems in a Finnish normal population sample. Sch. Psychol. Int. 2014, 35, 561–579. [Google Scholar] [CrossRef]
- Dekker, M.C.; Ferdinand, R.F.; Van Lang, N.D.; Bongers, I.L.; Van Der Ende, J.; Verhulst, F.C. Developmental trajectories of depressive symptoms from early childhood to late adolescence: Gender differences and adult outcome. J. Child Psychol. Psychiatry 2007, 48, 657–666. [Google Scholar] [CrossRef]
- Gaugue-Finot, J.; Devouche, E.; Wendland, J.; Varescon, I. Repérage de la dépression prénatale dans un échantillon de femmes françaises: Liens avec la détresse psychologique, l’anxiété et le soutien social perçu. Neuropsychiatr. L’enfance L’adolescence 2010, 58, 441–447. [Google Scholar] [CrossRef]
- Fatori, D.; Zuccolo, P.F.; Polanczyk, G.V. A Global Challenge: Maternal Depression and Offspring Mental Disorder; Springer: Berlin/Heidelberg, Germany, 2020; Volume 29, pp. 569–571. [Google Scholar]
- Fawcett, E.J.; Fairbrother, N.; Cox, M.L.; White, I.R.; Fawcett, J.M. The prevalence of anxiety disorders during pregnancy and the postpartum period: A multivariate Bayesian meta-analysis. J. Clin. Psychiatry 2019, 80, 1181. [Google Scholar] [CrossRef] [PubMed]
- Wallwiener, S.; Goetz, M.; Lanfer, A.; Gillessen, A.; Suling, M.; Feisst, M.; Sohn, C.; Wallwiener, M. Epidemiology of mental disorders during pregnancy and link to birth outcome: A large-scale retrospective observational database study including 38,000 pregnancies. Arch. Gynecol. Obstet. 2019, 299, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Falah-Hassani, K.; Shiri, R.; Dennis, C.-L. The prevalence of antenatal and postnatal co-morbid anxiety and depression: A meta-analysis. Psychol. Med. 2017, 47, 2041–2053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madigan, S.; Oatley, H.; Racine, N.; Fearon, R.P.; Schumacher, L.; Akbari, E.; Cooke, J.E.; Tarabulsy, G.M. A meta-analysis of maternal prenatal depression and anxiety on child socioemotional development. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 645–657.e8. [Google Scholar] [CrossRef]
- Ibanez, G.; Charles, M.-A.; Forhan, A.; Magnin, G.; Thiebaugeorges, O.; Kaminski, M.; Saurel-Cubizolles, M.-J.; EDEN Mother–Child Cohort Study Group. Depression and anxiety in women during pregnancy and neonatal outcome: Data from the EDEN mother–child cohort. Early Hum. Dev. 2012, 88, 643–649. [Google Scholar] [CrossRef]
- Glover, V.; O’Donnell, K.J.; O’Connor, T.G.; Fisher, J. Prenatal maternal stress, fetal programming, and mechanisms underlying later psychopathology—A global perspective. Dev. Psychopathol. 2018, 30, 843–854. [Google Scholar] [CrossRef]
- Sapolsky, R.M. Stress and the brain: Individual variability and the inverted-U. Nat. Neurosci. 2015, 18, 1344–1346. [Google Scholar] [CrossRef]
- Gustafsson, H.C.; Sullivan, E.L.; Nousen, E.K.; Sullivan, C.A.; Huang, E.; Rincon, M.; Nigg, J.T.; Loftis, J.M. Maternal prenatal depression predicts infant negative affect via maternal inflammatory cytokine levels. Brain Behav. Immun. 2018, 73, 470–481. [Google Scholar] [CrossRef]
- McGuinn, L.A.; Tamayo-Ortiz, M.; Rosa, M.J.; Harari, H.; Osorio-Valencia, E.; Schnaas, L.; Hernandez-Chavez, C.; Wright, R.J.; Klein, D.N.; Téllez-Rojo, M.M.; et al. The influence of maternal anxiety and cortisol during pregnancy on childhood anxiety symptoms. Psychoneuroendocrinology 2022, 139, 105704. [Google Scholar] [CrossRef]
- Swales, D.A.; Winiarski, D.A.; Smith, A.K.; Stowe, Z.N.; Newport, D.J.; Brennan, P.A. Maternal depression and cortisol in pregnancy predict offspring emotional reactivity in the preschool period. Dev. Psychobiol. 2018, 60, 557–566. [Google Scholar] [CrossRef]
- Jami, E.S.; Hammerschlag, A.R.; Bartels, M.; Middeldorp, C.M. Parental characteristics and offspring mental health and related outcomes: A systematic review of genetically informative literature. Transl. Psychiatry 2021, 11, 197. [Google Scholar] [CrossRef]
- Underwood, L.; Waldie, K.; D’Souza, S.; Peterson, E.R.; Morton, S. A review of longitudinal studies on antenatal and postnatal depression. Arch. Women’s Ment. Health 2016, 19, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Lahti, M.; Savolainen, K.; Tuovinen, S.; Pesonen, A.-K.; Lahti, J.; Heinonen, K.; Hämäläinen, E.; Laivuori, H.; Villa, P.M.; Reynolds, R.M.; et al. Maternal depressive symptoms during and after pregnancy and psychiatric problems in children. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 30–39.e37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amuli, K.; Decabooter, K.; Talrich, F.; Renders, A.; Beeckman, K. Born in Brussels screening tool: The development of a screening tool measuring antenatal psychosocial vulnerability. BMC Public Health 2021, 21, 1522. [Google Scholar] [CrossRef] [PubMed]
- Lee-Carbon, L.; Nath, S.; Trevillion, K.; Byford, S.; Howard, L.M.; Challacombe, F.L.; Heslin, M. Mental health service use among pregnant and early postpartum women. Soc. Psychiatry Psychiatr. Epidemiol. 2022, 57, 2229–2240. [Google Scholar] [CrossRef] [PubMed]
- Bales, M.; Pambrun, E.; Melchior, M.; Glangeaud-Freudenthal, N.-C.; Charles, M.-A.; Verdoux, H.; Sutter-Dallay, A.-L. Prenatal psychological distress and access to mental health care in the ELFE cohort. Eur. Psychiatry 2015, 30, 322–328. [Google Scholar] [CrossRef]
- Jones, T.L.; Prinz, R.J. Potential roles of parental self-efficacy in parent and child adjustment: A review. Clin. Psychol. Rev. 2005, 25, 341–363. [Google Scholar] [CrossRef]
- Baron, E.; Bass, J.; Murray, S.M.; Schneider, M.; Lund, C. A systematic review of growth curve mixture modelling literature investigating trajectories of perinatal depressive symptoms and associated risk factors. J. Affect. Disord. 2017, 223, 194–208. [Google Scholar] [CrossRef]
- Sin, N.L.; Lyubomirsky, S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: A practice-friendly meta-analysis. J. Clin. Psychol. 2009, 65, 467–487. [Google Scholar] [CrossRef] [Green Version]
- Grande, L.A.; Swales, D.A.; Sandman, C.A.; Glynn, L.M.; Davis, E.P. Maternal caregiving ameliorates the consequences of prenatal maternal psychological distress on child development. Dev. Psychopathol. 2022, 34, 1376–1385. [Google Scholar] [CrossRef]
- Zietlow, A.-L.; Nonnenmacher, N.; Reck, C.; Ditzen, B.; Müller, M. Emotional stress during pregnancy–Associations with maternal anxiety disorders, infant cortisol reactivity, and mother–child interaction at pre-school age. Front. Psychol. 2019, 10, 2179. [Google Scholar] [CrossRef]
- Teti, D.M.; Gelfand, D.M. Behavioral competence among mothers of infants in the first year: The mediational role of maternal self-efficacy. Child Dev. 1991, 62, 918–929. [Google Scholar] [CrossRef] [PubMed]
- Clayborne, Z.M.; Nilsen, W.; Torvik, F.A.; Gustavson, K.; Bekkhus, M.; Gilman, S.E.; Khandaker, G.M.; Fell, D.B.; Colman, I. Positive maternal mental health attenuates the associations between prenatal stress and children’s internalizing and externalizing symptoms. Eur. Child Adolesc. Psychiatry 2022. [Google Scholar] [CrossRef] [PubMed]
- Phua, D.Y.; Kee, M.Z.; Meaney, M.J. Positive maternal mental health, parenting, and child development. Biol. Psychiatry 2020, 87, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Javo, C.; Rønning, J.A.; Handegård, B.H.; Rudmin, F.W. Social competence and emotional/behavioral problems in a birth cohort of Sami and Norwegian preadolescents in Arctic Norway as reported by mothers and teachers. Nord. J. Psychiatry 2009, 63, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; La Porte, L.M.; Corcoran, M.; Magasi, S.; Batza, J.; Silver, R.K. Barriers to mental health treatment among obstetric patients at risk for depression. Am. J. Obstet. Gynecol. 2010, 202, 312.e1–312.e5. [Google Scholar] [CrossRef]
- Goodman, S.H.; Gotlib, I.H. Risk for psychopathology in the children of depressed mothers: A developmental model for understanding mechanisms of transmission. Psychol. Rev. 1999, 106, 458. [Google Scholar] [CrossRef]
- L’Assurance Maladie. Devenir Parents. Available online: https://www.ameli.fr/assure/sante/themes/grossesse/preparation-parentalite#:~:text=L’entretien%20pr%C3%A9natal%20pr%C3%A9coce%20est%20un%20entretien%2C%20individuel%20ou%20en,%25%20par%20l’Assurance%20Maladie (accessed on 14 December 2022).
- Guedeney, A.; Benarous, X. Un cahier de suivi psychologique périnatal: Favoriser le dépistage et la continuité entre soins pré-et postnataux en maternité. Bull. L’académie Natl. Médecine 2021, 205, 587–591. [Google Scholar] [CrossRef]
- Revenson, T.A.; Kayser, K.E.; Bodenmann, G.E. Couples Coping with Stress: Emerging Perspectives on Dyadic Coping; American Psychological Association: Washington, DC, USA, 2005. [Google Scholar]



{kind=link}
{kind=link}
| Maternal Prenatal Mental Health | |||||
|---|---|---|---|---|---|
| Variables | No Symptoms (n = 805) | Anxious Symptoms Only (n = 83) | Depressive Symptoms Only (n = 131) | Comorbid (n = 116) | |
| n (%) | n (%) | n (%) | n (%) | p-Value a | |
| Recruitment center (Nancy) | 387 (48.07) | 34 (40.96) | 69 (52.67) | 45 (38.79) | 0.094 |
| Primiparous (yes) | 396 (49.19) | 37 (44.50) | 55 (41.98) | 45 (38.79) | 0.031 * |
| Mother unemployed and not studying | 121 (15.03) | 18 (21.69) | 27 (20.61) | 25 (21.55) | 0.231 |
| Father unemployed and not studying | 34 (4.22) | 3 (3.61) | 4 (3.05) | 7 (6.03) | 0.074 |
| Migrant background | 0.199 | ||||
| None | 706 (87.70) | 74 (89.16) | 111 (84.73) | 94 (81.03) | |
| Second generation | 65 (8.07) | 5 (6.02) | 16 (12.21) | 15 (12.93) | |
| First generation | 16 (1.99) | 1 (1.20) | 3 (2.29) | 5 (4.31) | |
| Household income <1500 EUR/month | 70 (8.70) | 13 (15.66) | 14 (10.69) | 22 (18.97) | 0.018 * |
| At least one financial difficulty | 29 (3.60) | 7 (8.43) | 12 (2.76) | 17 (14.66) | <0.001 *** |
| Antidepressant use before pregnancy | 25 (3.11) | 4 (4.82) | 7 (5.34) | 20 (17.24) | <0.001 *** |
| Not receiving practical support (partner) | 57 (7.08) | 9 (10.84) | 14 (10.69) | 11 (9.48) | 0.010 ** |
| Not receiving practical support (other) | 122 (15.16) | 18 (21.69) | 30 (22.90) | 18 (15.52) | 0.085 |
| Not receiving emotional support (partner) | 13 (1.61) | 4 (4.82) | 5 (3.82) | 7 (6.03) | 0.002 ** |
| Not receiving emotional support (other) | 36 (4.47) | 7 (8.43) | 11 (8.40) | 12 (10.34) | 0.027 * |
| Living with father of the child (no) | 15 (1.86) | 4 (4.82) | 10 (7.63) | 8 (6.90) | 0.001 *** |
| Childhood adversity (yes) | 176 (21.86) | 19 (22.89) | 44 (33.59) | 46 (39.66) | <0.001 *** |
| Childhood behaviour problems (mother) | 35 (4.35) | 3 (3.61) | 12 (9.16) | 15 (12.93) | 0.009 ** |
| Childhood behaviour problems (father) | 72 (8.94) | 6 (7.23) | 21 (16.03) | 6 (5.17) | 0.028 * |
| Child sex (female) | 363 (45.09) | 37 (44.58) | 73 (55.73) | 59 (50.86) | 0.109 |
| Consulted psychologist/psychiatrist in pregnancy | 40 (4.97) | 14 (16.87) | 18 (13.74) | 26 (22.41) | <0.001 *** |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | p-value b | |
| Maternal age (years) | 30.52 (4.60) | 30.96 (4.58) | 30.29 (4.88) | 31.69 (5.17) | 0.067 |
| Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | p-value c | |
| Maternal education (years) | 14 (12–17) | 14 (11–17) | 14 (12–17) | 12 (11–14) | <0.001 *** |
| Paternal education (years) | 14 (11–17) | 12 (11–17) | 12 (11–17) | 12 (11–14) | 0.410 |
| Anxious, Non-Depressive (n = 83) | Depressive, Non-Anxious (n = 131) | Depressive and Anxious (n = 116) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SDQ Subscales | Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | |||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | ||
| Emotional symptoms | Low | Ref | Ref | Ref | Ref | Ref | Ref | ||||||
| Intermediate | 1.12 | (0.68–1.84) | 1.01 | (0.59–1.71) | 1.29 | (0.86–1.93) | 1.21 | (0.78–1.87) | 1.67 | (1.06–2.63) | 1.85 | (1.09–3.16) | |
| High | 1.53 | (0.77–3.05) | 1.50 | (0.73–3.08) | 1.70 | (0.97–3.00) | 1.63 | (0.90–2.96) | 2.74 | (1.54–4.88) | 2.46 | (1.26–4.80) | |
| Conduct problems | Low | ||||||||||||
| Intermediate | 1.24 | (0.72–2.16) | 1.04 | (0.58–1.84) | 1.14 | (0.72–1.80) | 0.98 | (0.60–1.61) | 1.23 | (0.76–2.01) | 1.10 | (0.63–1.93) | |
| High | 1.85 | (0.90–3.80) | 1.40 | (0.65–3.01) | 2.35 | (1.34–4.10) | 1.65 | (0.90–3.02) | 2.53 | (1.40–4.59) | 2.02 | (1.01–4.07) | |
| Inattention-hyperactivity | Low | ||||||||||||
| Intermediate | 1.33 | (0.79–2.23) | 1.22 | (0.71–2.10) | 1.48 | (0.96–2.29) | 1.49 | (0.93–2.38) | 1.35 | (0.86–2.12) | 1.30 | (0.76–2.22) | |
| High | 1.65 | (0.82–3.31) | 1.54 | (0.72–3.29) | 2.16 | (1.24–3.77) | 1.63 | (0.89–2.98) | 2.03 | (1.14–3.63) | 1.83 | (0.86–3.86) | |
| Peer relation problems | Low | ||||||||||||
| Intermediate | 1.09 | (0.65–1.81) | 1.07 | (0.62–1.86) | 1.50 | (0.97–2.33) | 1.44 | (0.90–2.29) | 1.33 | (0.84–2.12) | 1.02 | (0.59–1.74) | |
| High | 1.63 | (0.70–3.84) | 1.42 | (0.55–3.63) | 2.12 | (1.04–4.35) | 1.63 | (0.76–3.47) | 2.63 | (1.31–5.26) | 1.85 | (0.84–4.08) | |
| Prosocial behaviours | Low | 1.98 | (0.88–4.47) | 1.96 | (0.80–4.78) | 1.43 | (0.74–2.76) | 1.32 | (0.66–2.65) | 2.56 | (1.25–5.27) | 2.24 | (0.98–5.13) |
| Intermediate | 1.13 | (0.68–1.85) | 1.07 | (0.63–1.80) | 0.66 | (0.45–0.98) | 0.64 | (0.42–0.97) | 1.56 | (0.99–2.45) | 1.32 | (0.80–2.19) | |
| High | |||||||||||||
| SDQ Subscales | Did Not Report a Consultation (n = 1037; Any Negative Mental Health Symptoms in 272 (26.2%)) | Reported Mental Health Consultations during Pregnancy (n = 98; Any Negative Mental Health Symptoms in 58 (59.2%)) | |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | ||
| Emotional symptoms | Low | Ref | Ref |
| Intermediate | 1.27 (0.92–1.76) | 1.12 (0.41–3.03) | |
| High | 2.32 (1.50–3.58) | 0.38 (0.08–1.80) | |
| Conduct problems | Low | Ref | Ref |
| Intermediate | 1.16 (0.81–1.65) | 0.37 (0.11–1.22) | |
| High | 2.26 (1.44–3.56) | 0.09 (0.02–0.48) | |
| Inattention- hyperactivity | Low | Ref | Ref |
| Intermediate | 1.49 (1.06–2.10) | 0.32 (0.12–0.84) | |
| High | 2.06 (1.33–3.20) | 0.15 (0.03–0.77) | |
| Peer relation problems | Low | Ref | Ref |
| Intermediate | 1.36 (0.96–1.93) | 0.93 (0.35–2.48) | |
| High | 2.10 (1.21–3.63) | 1.79 (0.18–17.54) | |
| Prosocial behaviours | Low | 2.07 (1.22–3.54) | 0.47 (0.17–1.46) |
| Intermediate | 1.06 (0.77–1.45) | 0.47 (0.18–1.20) | |
| High | Ref | Ref |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kallas, K.-A.; Marr, K.; Moirangthem, S.; Heude, B.; Koehl, M.; van der Waerden, J.; Downes, N. Maternal Mental Health Care Matters: The Impact of Prenatal Depressive and Anxious Symptoms on Child Emotional and Behavioural Trajectories in the French EDEN Cohort. J. Clin. Med. 2023, 12, 1120. https://doi.org/10.3390/jcm12031120
Kallas K-A, Marr K, Moirangthem S, Heude B, Koehl M, van der Waerden J, Downes N. Maternal Mental Health Care Matters: The Impact of Prenatal Depressive and Anxious Symptoms on Child Emotional and Behavioural Trajectories in the French EDEN Cohort. Journal of Clinical Medicine. 2023; 12(3):1120. https://doi.org/10.3390/jcm12031120
Chicago/Turabian StyleKallas, Kadri-Ann, Ketevan Marr, Simi Moirangthem, Barbara Heude, Muriel Koehl, Judith van der Waerden, and Naomi Downes. 2023. "Maternal Mental Health Care Matters: The Impact of Prenatal Depressive and Anxious Symptoms on Child Emotional and Behavioural Trajectories in the French EDEN Cohort" Journal of Clinical Medicine 12, no. 3: 1120. https://doi.org/10.3390/jcm12031120