
Chagas Heart Disease: Beyond a Single Complication, from Asymptomatic Disease to Heart Failure

 , , ,
, , , 
Abstract
:1. Introduction
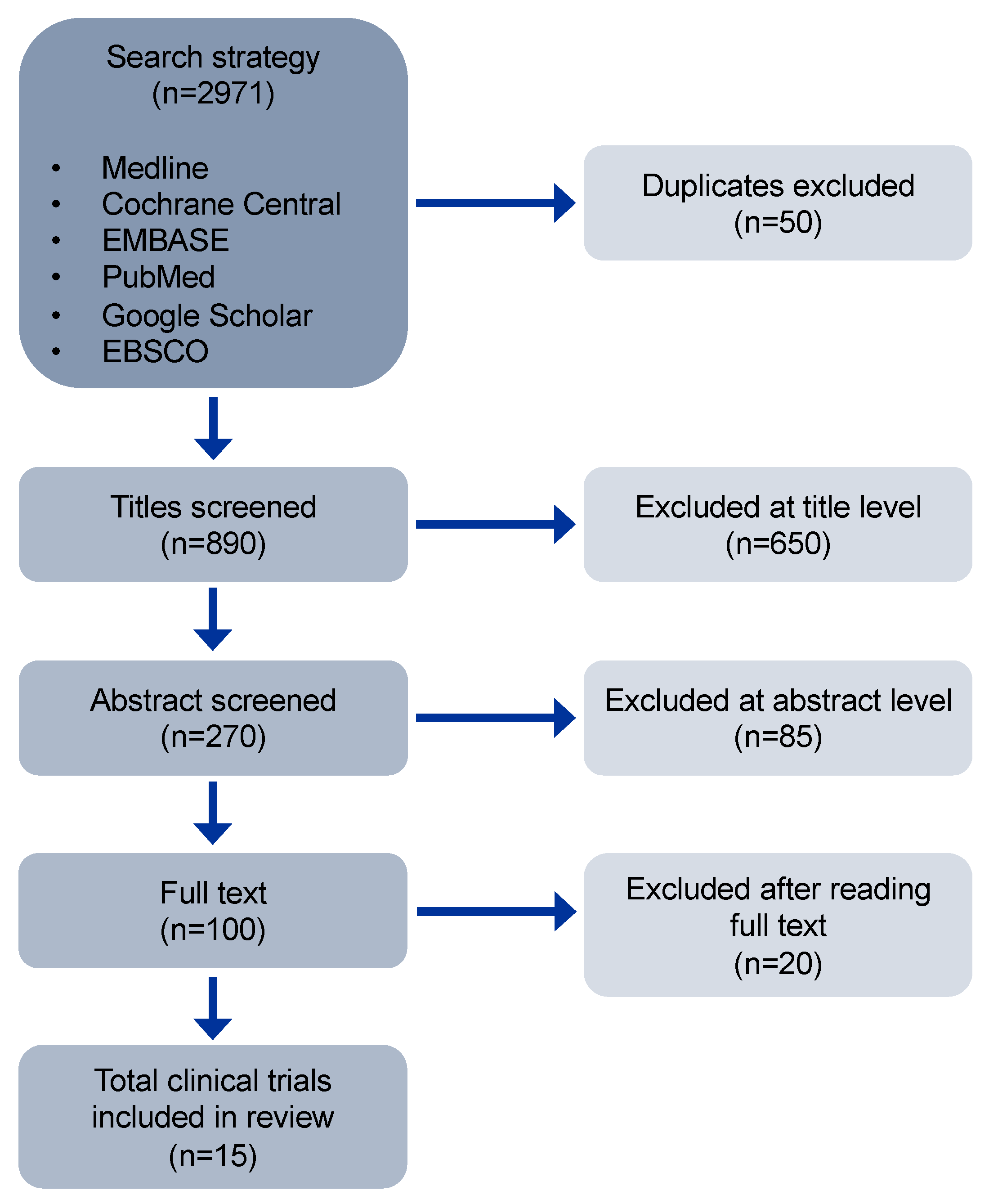
2. Methods
Literature Search
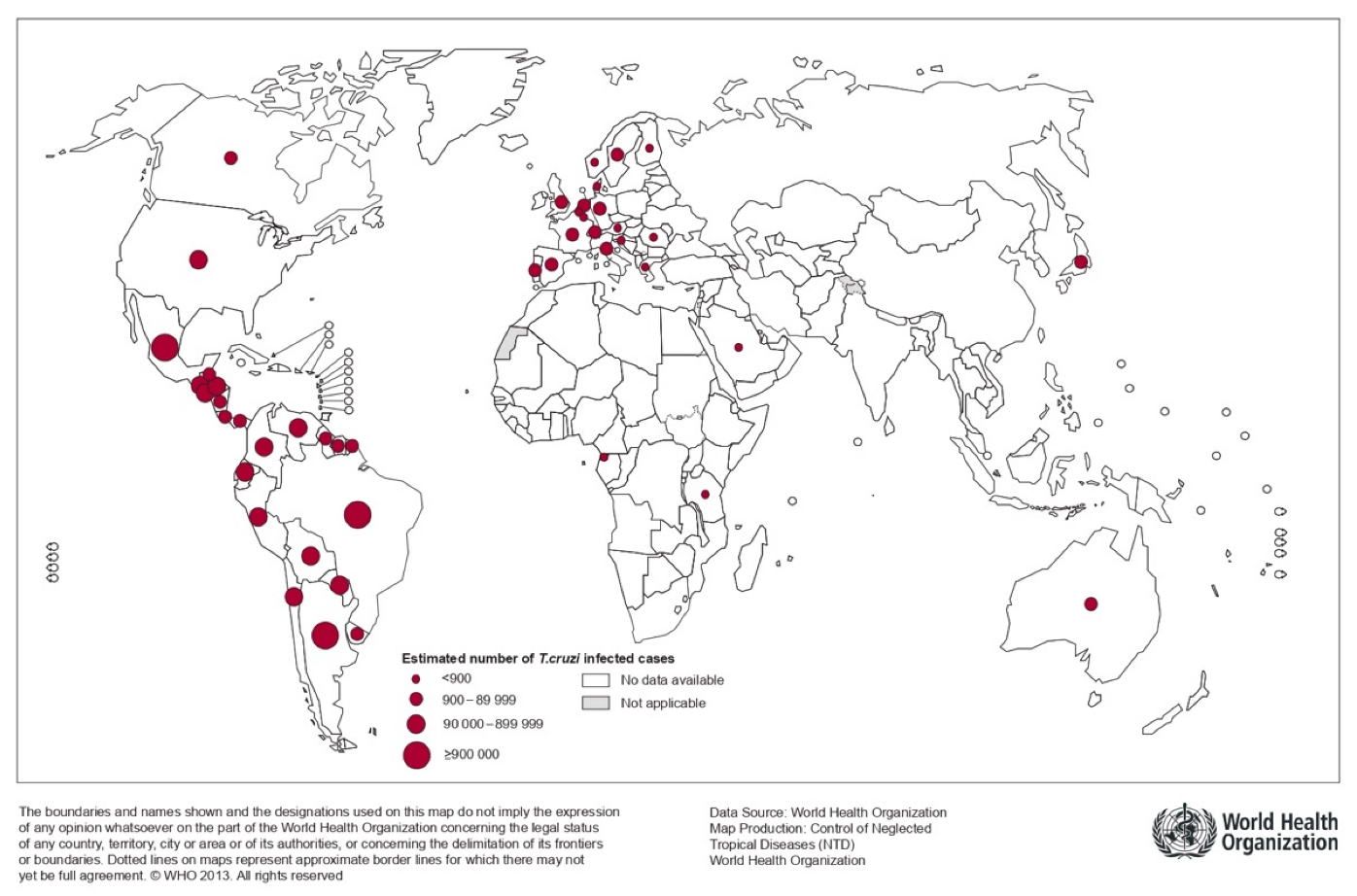
3. Epidemiology and Socioeconomic Impact
4. Pathophysiology of Chagas Cardiomyopathy
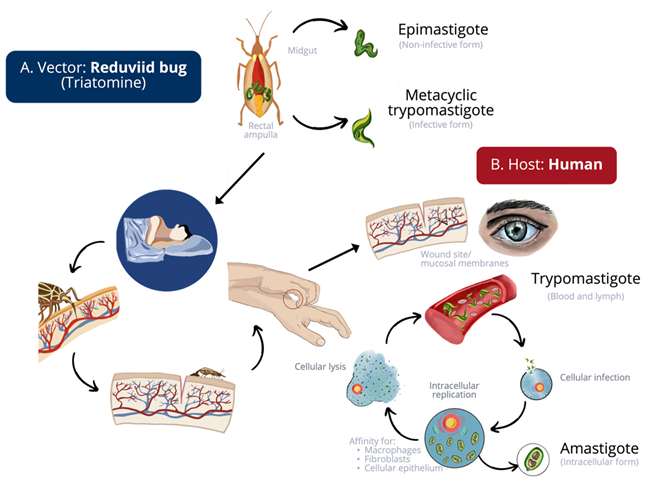
4.1. Biology and Transmission Routes of Trypanosoma cruzi
4.2. Genetics
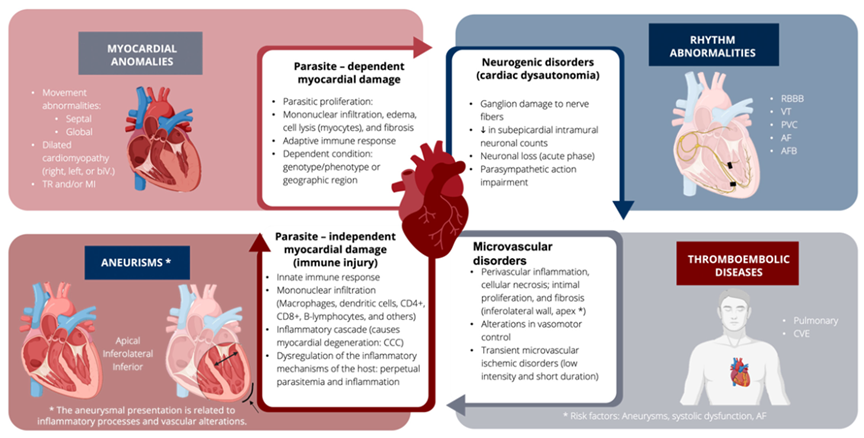
4.3. Pathogenesis
4.3.1. Parasite-Dependent Myocardial Damage
4.3.2. Parasite-Independent or Immune-Independent Myocardial Damage
4.3.3. Microvascular Disorders
4.3.4. Neurogenic Disorders
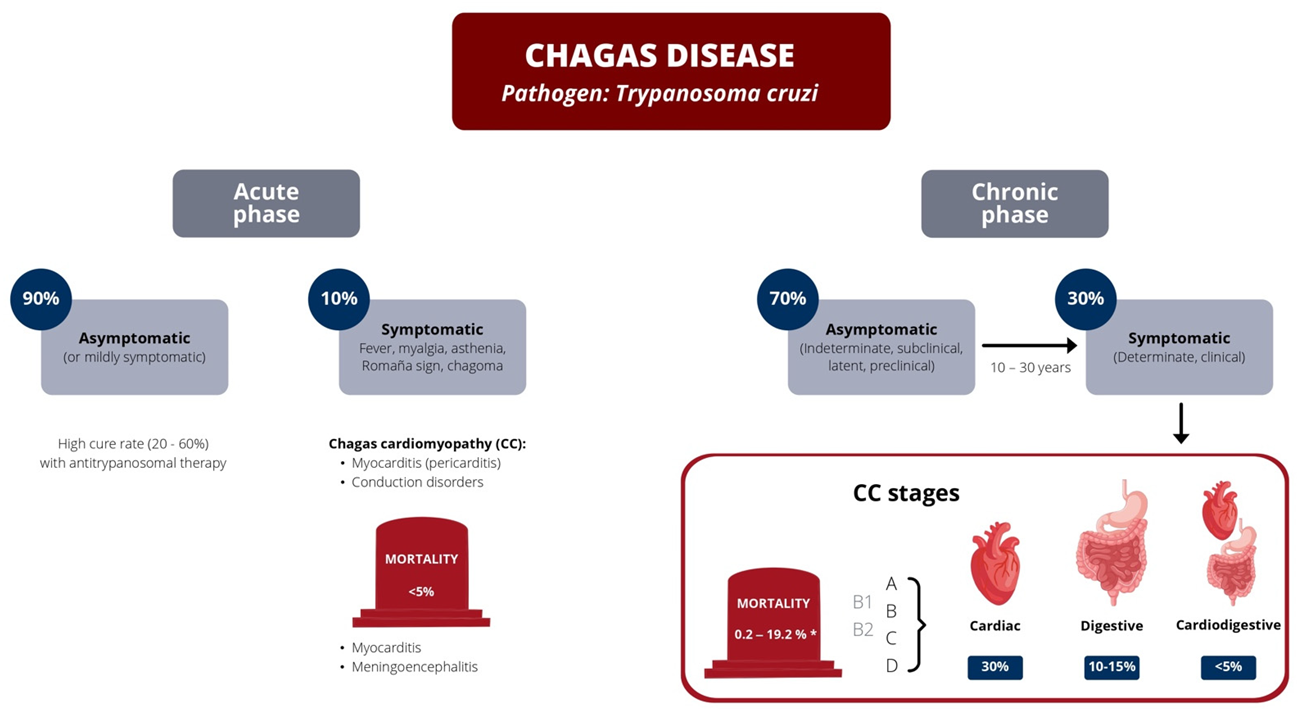
5. Clinical Presentation
5.1. Acute Stage
5.2. Chronic Stage
5.2.1. Chronic Asymptomatic Phase
5.2.2. Chronic Symptomatic Stage
Chagas Cardiomyopathy (CC)
6. Diagnosis
6.1. Biomarkers
6.2. Electrocardiogram (ECG)
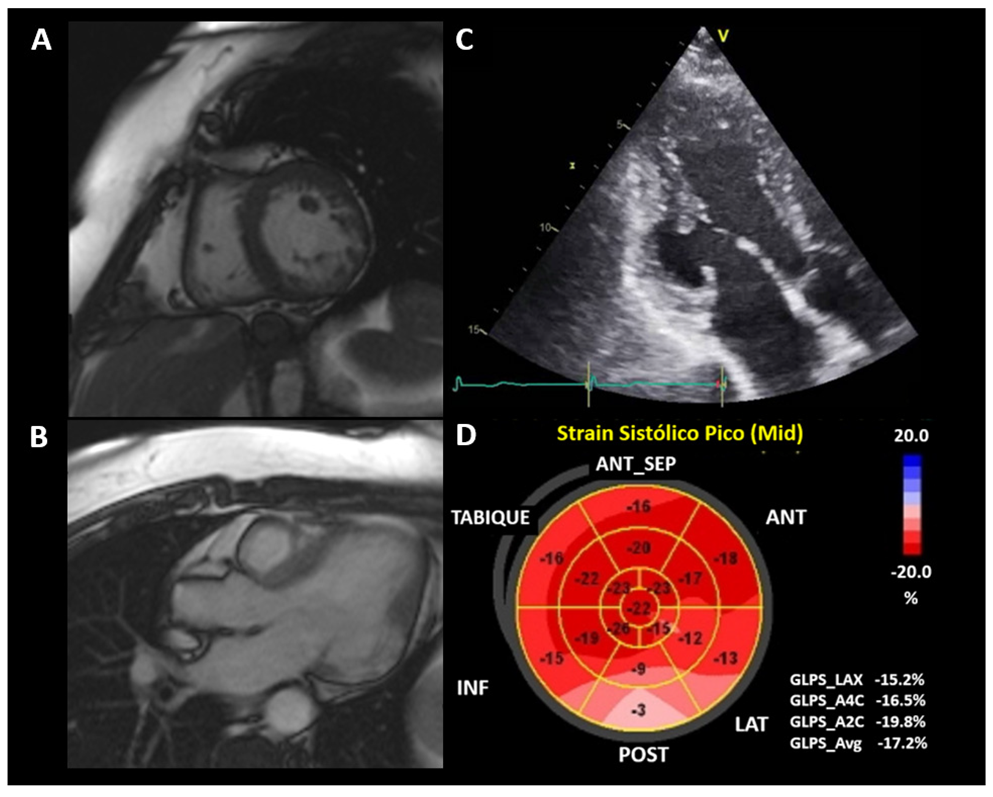
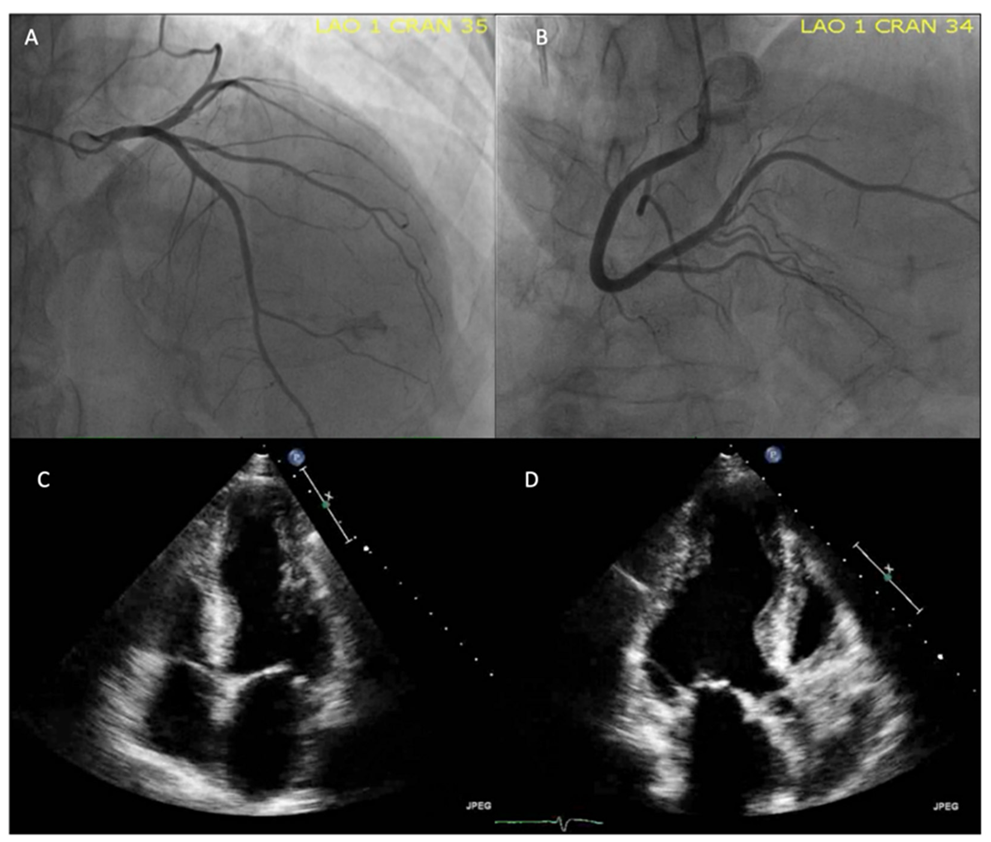
6.3. Echocardiogram
6.4. Cardiac Magnetic Resonance (CMR) Imaging
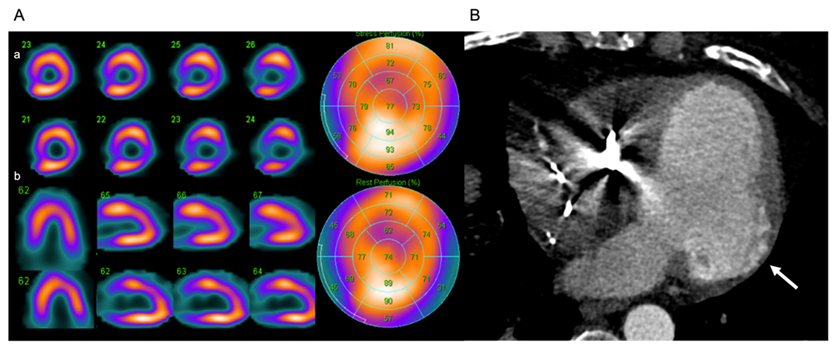
6.5. Nuclear Cardiology
7. Treatment
7.1. Medical Treatment
7.2. Surgical Treatment
7.2.1. Heart Transplant
7.2.2. Implantable Cardioverter Defibrillator (ICD)
8. Prevention
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chagas’ Heart Disease. Curr. Probl. Cardiol. 1995, 20, 831–924. [CrossRef]
- Pino-Marín, A.; Medina-Rincón, G.J.; Gallo-Bernal, S.; Duran-Crane, A.; Arango Duque, Á.I.; Rodríguez, M.J.; Medina-Mur, R.; Manrique, F.T.; Forero, J.F.; Medina, H.M. Chagas Cardiomyopathy: From Romaña Sign to Heart Failure and Sudden Cardiac Death. Pathogens 2021, 10, 505. [Google Scholar] [CrossRef] [PubMed]
- de Souza, A.L.A.D.A.G.; Mesquita, C.T. Chagas Disease–Past and Future. Int. J. Cardiovasc. Sci. 2020, 33, 601–603. [Google Scholar] [CrossRef]
- Chagas Disease (Also Known as American Trypanosomiasis). Available online: https://www.who.int/news-room/fact-sheets/detail/chagas-disease-(american-trypanosomiasis) (accessed on 9 August 2020).
- Romano, M.M.D.; Moreira, H.T.; Marin-Neto, J.A.; Baccelli, P.E.; Alenezi, F.; Klem, I.; Maciel, B.C.; Kisslo, J.; Schmidt, A.; Velazquez, E.J. Early Impairment of Myocardial Deformation Assessed by Regional Speckle-Tracking Echocardiography in the Indeterminate Form of Chagas Disease without Fibrosis Detected by Cardiac Magnetic Resonance. PLoS Negl. Trop. Dis. 2020, 14, e0008795. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, J.V.; Pereira, B.V.M.; Couceiro, K.D.N.; da Silva e Silva, M.R.H.; Doria, S.S.; da Silva, P.R.L.; de Lira, E.D.F.; Guerra, M.D.G.V.B.; Guerra, J.A.D.O.; Ferreira, J.M.B.B. Cardiac Evaluation in the Acute Phase of Chagas’ Disease with Post-Treatment Evolution in Patients Attended in the State of Amazonas, Brazil. Arq. Bras. Cardiol. 2019, 112, 240–246. [Google Scholar] [CrossRef]
- Echeverría, L.E.; Marcus, R.; Novick, G.; Sosa-Estani, S.; Ralston, K.; Zaidel, E.J.; Forsyth, C.; Ribeiro, A.L.P.; Mendoza, I.; Falconi, M.L.; et al. WHF IASC Roadmap on Chagas Disease. Glob. Heart 2020, 15, 26. [Google Scholar] [CrossRef] [Green Version]
- Lidani, K.C.F.; Andrade, F.A.; Bavia, L.; Damasceno, F.S.; Beltrame, M.H.; Messias-Reason, I.J.; Sandri, T.L. Chagas Disease: From Discovery to a Worldwide Health Problem. Front. Public Health 2019, 7, 166. [Google Scholar] [CrossRef]
- Bonney, K.M.; Luthringer, D.J.; Kim, S.A.; Garg, N.J.; Engman, D.M. Pathology and Pathogenesis of Chagas Heart Disease. Annu. Rev. Pathol. Mech. Dis. 2019, 14, 421–447. [Google Scholar] [CrossRef]
- Arce-Fonseca, M.; Carrillo-Sánchez, S.C.; Molina-Barrios, R.M.; Martínez-Cruz, M.; Cedillo-Cobián, J.R.; Henao-Díaz, Y.A.; Rodríguez-Morales, O. Seropositivity for Trypanosoma Cruzi in Domestic Dogs from Sonora, Mexico. Infect. Dis. Poverty 2017, 6, 120. [Google Scholar] [CrossRef] [Green Version]
- Chagas Disease (American Trypanosomiasis). Available online: https://cdn.who.int/media/docs/default-source/ntds/chagas-disease/chagas-2018-cases.pdf?sfvrsn=f4e94b3b_2 (accessed on 20 July 2021).
- Echavarría, N.G.; Echeverría, L.E.; Stewart, M.; Gallego, C.; Saldarriaga, C. Chagas Disease: Chronic Chagas Cardiomyopathy. Curr. Probl. Cardiol. 2019, 46, 100507. [Google Scholar] [CrossRef]
- Schofield, C.J.; Dias, J.C.P. A Cost-Benefit Analisys of Chagas Disease Control. Mem. Inst. Oswaldo Cruz 1991, 86, 285–295. [Google Scholar] [CrossRef] [Green Version]
- Nunes, M.C.P.; Beaton, A.; Acquatella, H.; Bern, C.; Bolger, A.F.; Echeverría, L.E.; Dutra, W.O.; Gascon, J.; Morillo, C.A.; Oliveira-Filho, J.; et al. Chagas Cardiomyopathy: An Update of Current Clinical Knowledge and Management: A Scientific Statement from the American Heart Association. Circulation 2018, 138, e169–e209. [Google Scholar] [CrossRef]
- Malik, L.H.; Singh, G.D.; Amsterdam, E.A. The Epidemiology, Clinical Manifestations, and Management of Chagas Heart Disease: Chagas Heart Disease. Clin. Cardiol. 2015, 38, 565–569. [Google Scholar] [CrossRef]
- Benziger, C.P.; do Carmo, G.A.L.; Ribeiro, A.L.P. Chagas Cardiomyopathy. Cardiol. Clin. 2017, 35, 31–47. [Google Scholar] [CrossRef]
- Moncayo, Á.; Silveira, A.C. Current Epidemiological Trends for Chagas Disease in Latin America and Future Challenges in Epidemiology, Surveillance and Health Policy. Mem. Inst. Oswaldo Cruz 2009, 104, 17–30. [Google Scholar] [CrossRef] [Green Version]
- Kraef, C.; Ramharter, M. Kardiale Beteiligung bei Tropenerkrankungen. Herz 2019, 44, 83–91. [Google Scholar] [CrossRef]
- World Health Organization = Organisation mondiale de la Santé. Chagas Disease in Latin America: An Epidemiological Update Based on 2010 Estimates = Maladie de Chagas En Amérique Latine: Le Point Épidémiologique Basé Sur Les Estimations de 2010. Wkly. Epidemiol. Rec. Relev. Épidémiologique Hebd. 2015, 90, 33–44. [Google Scholar]
- Santos, É.; Menezes Falcão, L. Chagas Cardiomyopathy and Heart Failure: From Epidemiology to Treatment. Rev. Port. Cardiol. 2020, 39, 279–289. [Google Scholar] [CrossRef]
- Lima, N.d.A.; Martin, D.T.; Vos, D.; Melgar, T.A.; de Castro, R.L., Jr.; Ladzinski, A.; Ring, A. Hospitalization for Chagas Heart Disease in the United States From 2002 to 2017. JAMA Netw. Open 2021, 4, e2129959. [Google Scholar] [CrossRef]
- Beatty, N.L.; Klotz, S.A. Autochthonous Chagas Disease in the United States: How Are People Getting Infected? Am. J. Trop. Med. Hyg. 2020, 103, 967–969. [Google Scholar] [CrossRef]
- Wirtz, V.J.; Manne-Goehler, J.; Reich, M.R. Access to Care for Chagas Disease in the United States: A Health Systems Analysis. Am. J. Trop. Med. Hyg. 2015, 93, 108–113. [Google Scholar] [CrossRef]
- Bern, C.; Montgomery, S.P. An Estimate of the Burden of Chagas Disease in the United States. Clin. Infect. Dis. 2009, 49, e52–e54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traina, M.I.; Hernandez, S.; Sanchez, D.R.; Dufani, J.; Salih, M.; Abuhamidah, A.M.; Olmedo, W.; Bradfield, J.S.; Forsyth, C.J.; Meymandi, S.K. Prevalence of Chagas Disease in a U.S. Population of Latin American Immigrants with Conduction Abnormalities on Electrocardiogram. PLoS Negl. Trop. Dis. 2017, 11, e0005244. [Google Scholar] [CrossRef] [PubMed]
- Requena-Méndez, A.; Aldasoro, E.; de Lazzari, E.; Sicuri, E.; Brown, M.; Moore, D.A.J.; Gascon, J.; Muñoz, J. Prevalence of Chagas Disease in Latin-American Migrants Living in Europe: A Systematic Review and Meta-Analysis. PLoS Negl. Trop. Dis. 2015, 9, e0003540. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.Y.; Bacon, K.M.; Bottazzi, M.E.; Hotez, P.J. Global Economic Burden of Chagas Disease: A Computational Simulation Model. Lancet Infect. Dis. 2013, 13, 342–348. [Google Scholar] [CrossRef] [Green Version]
- Bartholomeu, D.C.; Teixeira, S.M.R.; El-Sayed, N.M.A. Genetics of Trypanosoma Cruzi. In American Trypanosomiasis Chagas Disease; Elsevier: Amsterdam, The Netherlands, 2017; pp. 429–454. ISBN 978-0-12-801029-7. [Google Scholar]
- de Lana, M.; de Menezes Machado, E.M. Biology of Trypanosoma Cruzi and Biological Diversity. In American Trypanosomiasis Chagas Disease; Elsevier: Amsterdam, The Netherlands, 2017; pp. 345–369. ISBN 978-0-12-801029-7. [Google Scholar]
- de Souza, W.; de Carvalho, T.U.; Barrias, E.S. Ultrastructure of Trypanosoma Cruzi and Its Interaction with Host Cells. In American Trypanosomiasis Chagas Disease; Elsevier: Amsterdam, The Netherlands, 2017; pp. 401–427. ISBN 978-0-12-801029-7. [Google Scholar]
- Marin-Neto, J.A.; Rassi, A. Update on Chagas Heart Disease on the First Centennial of Its Discovery. Rev. Española Cardiol. (Engl. Ed.) 2009, 62, 1211–1216. [Google Scholar] [CrossRef]
- Machado, F.S.; Jelicks, L.A.; Kirchhoff, L.V.; Shirani, J.; Nagajyothi, F.; Mukherjee, S.; Nelson, R.; Coyle, C.M.; Spray, D.C.; de Carvalho, A.C.C.; et al. Chagas Heart Disease: Report on Recent Developments. Cardiol. Rev. 2012, 20, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Brenière, S.F.; Villacis, A.; Aznar, C. Vector Transmission. In American Trypanosomiasis Chagas Disease; Elsevier: Amsterdam, The Netherlands, 2017; pp. 497–515. ISBN 978-0-12-801029-7. [Google Scholar]
- Anis, R.J.; Anis, R.; José Antonio, M.-N. Chagas Disease. Lancet 2010, 375, 1388–1402. [Google Scholar] [CrossRef]
- Guhl, F. Geographical Distribution of Chagas Disease. In American Trypanosomiasis Chagas Disease; Elsevier: Amsterdam, The Netherlands, 2017; pp. 89–112. ISBN 978-0-12-801029-7. [Google Scholar]
- Bocchi, E.A.; Bestetti, R.B.; Scanavacca, M.I.; Cunha Neto, E.; Issa, V.S. Chronic Chagas Heart Disease Management. J. Am. Coll. Cardiol. 2017, 70, 1510–1524. [Google Scholar] [CrossRef]
- Muñoz-Saravia, S.G.; Haberland, A.; Wallukat, G.; Schimke, I. Chronic Chagas’ Heart Disease: A Disease on Its Way to Becoming a Worldwide Health Problem: Epidemiology, Etiopathology, Treatment, Pathogenesis and Laboratory Medicine. Heart Fail. Rev. 2012, 17, 45–64. [Google Scholar] [CrossRef]
- Álvarez-Hernández, D.-A.; Franyuti-Kelly, G.-A.; Díaz-López-Silva, R.; González-Chávez, A.-M.; González-Hermosillo-Cornejo, D.; Vázquez-López, R. Chagas Disease: Current Perspectives on a Forgotten Disease. Rev. Médica Del. Hosp. Gen. México 2018, 81, 154–164. [Google Scholar] [CrossRef]
- Rassi, A., Jr.; Rassi, A.; Little, W.C. Chagas’ Heart Disease. Clin. Cardiol. 2000, 23, 883–889. [Google Scholar] [CrossRef]
- Bonney, K.; Engman, D. Chagas Heart Disease Pathogenesis: One Mechanism or Many? Curr. Mol. Med. 2008, 8, 510–518. [Google Scholar] [CrossRef] [Green Version]
- Parada, H.; Carrasco, H.A.; Añez, N.; Fuenmayor, C.; Inglessis, I. Cardiac Involvement Is a Constant Finding in Acute Chagas’ Disease: A Clinical, Parasitological and Histopathological Study. Int. J. Cardiol. 1997, 60, 49–54. [Google Scholar] [CrossRef]
- Herreros-Cabello, A.; Callejas-Hernández, F.; Fresno, M.; Gironès, N. Comparative Proteomic Analysis of Trypomastigotes from Trypanosoma Cruzi Strains with Different Pathogenicity. Infect. Genet. Evol. 2019, 76, 104041. [Google Scholar] [CrossRef]
- Callejas-Hernández, F.; Rastrojo, A.; Poveda, C.; Gironès, N.; Fresno, M. Genomic Assemblies of Newly Sequenced Trypanosoma Cruzi Strains Reveal New Genomic Expansion and Greater Complexity. Sci. Rep. 2018, 8, 14631. [Google Scholar] [CrossRef] [Green Version]
- Reis-Cunha, J.L.; Valdivia, H.O.; Bartholomeu, D.C. Gene and Chromosomal Copy Number Variations as an Adaptive Mechanism Towards a Parasitic Lifestyle in Trypanosomatids. Curr. Genom. 2018, 19, 87–97. [Google Scholar] [CrossRef]
- Lewis, M.D.; Llewellyn, M.S.; Yeo, M.; Messenger, L.A.; Miles, M.A. Experimental and Natural Recombination in Trypanosoma Cruzi. In American Trypanosomiasis Chagas Disease; Elsevier: Amsterdam, The Netherlands, 2017; pp. 455–473. ISBN 978-0-12-801029-7. [Google Scholar]
- Acosta-Herrera, M.; Strauss, M.; Casares-Marfil, D.; Martín, J. Genomic Medicine in Chagas Disease. Acta Trop. 2019, 197, 105062. [Google Scholar] [CrossRef]
- Ferreira Filho, J.C.R.; Braz, L.M.A.; Andrino, M.L.A.; Yamamoto, L.; Kanunfre, K.A.; Okay, T.S. Mitochondrial and Satellite Real Time-PCR for Detecting, T. Cruzi DTU II Strain in Blood and Organs of Experimentally Infected Mice Presenting Different Levels of Parasite Load. Exp. Parasitol. 2019, 200, 13–15. [Google Scholar] [CrossRef]
- Nonaka, C.K.V.; Sampaio, G.L.; de Aragão França, L.; Cavalcante, B.R.; Silva, K.N.; Khouri, R.; Torres, F.G.; Meira, C.S.; de Souza Santos, E.; Macedo, C.T.; et al. Therapeutic MiR-21 Silencing Reduces Cardiac Fibrosis and Modulates Inflammatory Response in Chronic Chagas Disease. IJMS 2021, 22, 3307. [Google Scholar] [CrossRef]
- Rassi, A., Jr.; Marin Neto, J.A.; Rassi, A. Chronic Chagas Cardiomyopathy: A Review of the Main Pathogenic Mechanisms and the Efficacy of Aetiological Treatment Following the BENznidazole Evaluation for Interrupting Trypanosomiasis (BENEFIT) Trial. Mem. Inst. Oswaldo Cruz 2017, 112, 224–235. [Google Scholar] [CrossRef] [PubMed]
- Simões, M.V.; Romano, M.M.D.; Schmidt, A.; Martins, K.S.M.; Marin-Neto, J.A. Chagas Disease Cardiomyopathy. Int. J. Cardiovasc. Sci. 2018, 31, 173–189. [Google Scholar] [CrossRef]
- Burke, S.; Nagajyothi, F.; Thi, M.M.; Hanani, M.; Scherer, P.E.; Tanowitz, H.B.; Spray, D.C. Adipocytes in Both Brown and White Adipose Tissue of Adult Mice Are Functionally Connected via Gap Junctions: Implications for Chagas Disease. Microbes Infect. 2014, 16, 893–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velasco, A.; Morillo, C.A. Chagas Heart Disease: A Contemporary Review. J. Nucl. Cardiol. 2018, 27, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Medina-Rincón, G.J.; Gallo-Bernal, S.; Jiménez, P.A.; Cruz-Saavedra, L.; Ramírez, J.D.; Rodríguez, M.J.; Medina-Mur, R.; Díaz-Nassif, G.; Valderrama-Achury, M.D.; Medina, H.M. Molecular and Clinical Aspects of Chronic Manifestations in Chagas Disease: A State-of-the-Art Review. Pathogens 2021, 10, 1493. [Google Scholar] [CrossRef]
- Malik, L.H.; Singh, G.D.; Amsterdam, E.A. Chagas Heart Disease: An Update. Am. J. Med. 2015, 128, 1251.e7–1251.e9. [Google Scholar] [CrossRef]
- Marin-Neto, J.A.; Cunha-Neto, E.; Maciel, B.C.; Simões, M.V. Pathogenesis of Chronic Chagas Heart Disease. Circulation 2007, 115, 1109–1123. [Google Scholar] [CrossRef]
- Lidani, K.C.F.; Bavia, L.; Ambrosio, A.R.; de Messias-Reason, I.J. The Complement System: A Prey of Trypanosoma Cruzi. Front. Microbiol. 2017, 8, 607. [Google Scholar] [CrossRef] [Green Version]
- Prado, C.M.; Jelicks, L.A.; Weiss, L.M.; Factor, S.M.; Tanowitz, H.B.; Rossi, M.A. The Vasculature in Chagas Disease. In Advances in Parasitology; Elsevier: Amsterdam, The Netherlands, 2011; Volume 76, pp. 83–99. ISBN 978-0-12-385895-5. [Google Scholar]
- Rada, J.; Donato, M.; Penas, F.N.; Alba Soto, C.; Cevey, Á.C.; Pieralisi, A.V.; Gelpi, R.; Mirkin, G.A.; Goren, N.B. IL-10-Dependent and -Independent Mechanisms Are Involved in the Cardiac Pathology Modulation Mediated by Fenofibrate in an Experimental Model of Chagas Heart Disease. Front. Immunol. 2020, 11, 572178. [Google Scholar] [CrossRef]
- Grijalva, A.; Gallo Vaulet, L.; Agüero, R.N.; Toledano, A.; Risso, M.G.; Quarroz Braghini, J.; Sosa, D.; Ruybal, P.; Repetto, S.; Alba Soto, C.D. Interleukin 10 Polymorphisms as Risk Factors for Progression to Chagas Disease Cardiomyopathy: A Case-Control Study and Meta-Analysis. Front. Immunol. 2022, 13, 946350. [Google Scholar] [CrossRef]
- Nunes, J.P.S.; Andrieux, P.; Brochet, P.; Almeida, R.R.; Kitano, E.; Honda, A.K.; Iwai, L.K.; Andrade-Silva, D.; Goudenège, D.; Alcântara Silva, K.D.; et al. Co-Exposure of Cardiomyocytes to IFN-γ and TNF-α Induces Mitochondrial Dysfunction and Nitro-Oxidative Stress: Implications for the Pathogenesis of Chronic Chagas Disease Cardiomyopathy. Front. Immunol. 2021, 12, 755862. [Google Scholar] [CrossRef]
- Duaso, J.; Yanez, E.; Castillo, C.; Galanti, N.; Cabrera, G.; Corral, G.; Maya, J.D.; Zulantay, I.; Apt, W.; Kemmerling, U. Reorganization of Extracellular Matrix in Placentas from Women with Asymptomatic Chagas Disease: Mechanism of Parasite Invasion or Local Placental Defense? J. Trop. Med. 2012, 2012, 758357. [Google Scholar] [CrossRef] [Green Version]
- Calvet, C.M.; Melo, T.G.; Garzoni, L.R.; Oliveira, F.O.R., Jr.; Neto, D.T.S.; Meirelles, M.N.S.L.; Pereira, M.C.S. Current Understanding of the Trypanosoma Cruzi-Cardiomyocyte Interaction. Front. Immun. 2012, 3, 327. [Google Scholar] [CrossRef] [Green Version]
- De Bona, E.; Lidani, K.C.F.; Bavia, L.; Omidian, Z.; Gremski, L.H.; Sandri, T.L.; de Messias Reason, I.J. Autoimmunity in Chronic Chagas Disease: A Road of Multiple Pathways to Cardiomyopathy? Front. Immunol. 2018, 9, 1842. [Google Scholar] [CrossRef] [Green Version]
- Gironès, N.; Cuervo, H.; Fresno, M. Trypanosoma Cruzi-Induced Molecular Mimicry and Chagas’ Disease. In Molecular Mimicry: Infection-Inducing Autoimmune Disease; Oldstone, M.B.A., Ed.; Current Topics in Microbiology and Immunology; Springer: Berlin/Heidelberg, Germany, 2005; Volume 296, pp. 89–123. ISBN 978-3-540-25597-0. [Google Scholar]
- Gironès, N.; Fresno, M. Etiology of Chagas Disease Myocarditis: Autoimmunity, Parasite Persistence, or Both? Trends Parasitol. 2003, 19, 19–22. [Google Scholar] [CrossRef]
- Medei, E.H.; Nascimento, J.H.M.; Pedrosa, R.C. Role of Autoantibodies in the Physiopathology of Chagas’ Disease. Arq. Bras. Cardiol. 2008, 91, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Rossi, M.A.; Tanowitz, H.B.; Malvestio, L.M.; Celes, M.R.; Campos, E.C.; Blefari, V.; Prado, C.M. Coronary Microvascular Disease in Chronic Chagas Cardiomyopathy Including an Overview on History, Pathology, and Other Proposed Pathogenic Mechanisms. PLoS Negl. Trop. Dis. 2010, 4, e674. [Google Scholar] [CrossRef]
- Marin-Neto, J.A.; Simões, M.V.; Ayres-Neto, E.M.; Attab-Santos, J.L.; Gallo, L., Jr.; Amorim, D.S.; Maciel, B.C. Studies of the Coronary Circulation in Chagas’ Heart Disease. Sao Paulo Med. J. 1995, 113, 826–834. [Google Scholar] [CrossRef] [Green Version]
- Marin-Neto, J.; Marzullo, P.; Marcassa, C.; Gallo, L.; Maciel, B.C.; Bellina, C.R.; L’Abbate, A. Myocardial Perfusion Abnormalities in Chronic Chagas’ Disease as Detected by Thallium-201 Scintigraphy. Am. J. Cardiol. 1992, 69, 780–784. [Google Scholar] [CrossRef]
- Duran-Crane, A.; Rojas, C.A.; Cooper, L.T.; Medina, H.M. Cardiac Magnetic Resonance Imaging in Chagas’ Disease: A Parallel with Electrophysiologic Studies. Int. J. Cardiovasc. Imaging 2020, 36, 2209–2219. [Google Scholar] [CrossRef]
- Regueiro, A.; García-Álvarez, A.; Sitges, M.; Ortiz-Pérez, J.T.; De Caralt, M.T.; Pinazo, M.J.; Posada, E.; Heras, M.; Gascón, J.; Sanz, G. Myocardial Involvement in Chagas Disease: Insights from Cardiac Magnetic Resonance. Int. J. Cardiol. 2013, 165, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Simões, M.V.; Pintya, A.O.; Bromberg-Marin, G.; Sarabanda, Á.V.; Antloga, C.M.; Pazin-Filho, A.; Maciel, B.C.; Marin-Neto, J.A. Relation of Regional Sympathetic Denervation and Myocardial Perfusion Disturbance to Wall Motion Impairment in Chagas’ Cardiomyopathy. Am. J. Cardiol. 2000, 86, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Hagar, J.M.; Rahimtoola, S.H. Chagas’ heart disease in the United States. N. Engl. J. Med. 1991, 325, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Marin-Neto, J.A.; Simoes, M.V.; Rassi Junior, A. Pathogenesis of Chronic Chagas Cardiomyopathy: The Role of Coronary Microvascular Derangements. Rev. Soc. Bras. Med. Trop. 2013, 46, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Corral, R.S.; Guerrero, N.A.; Cuervo, H.; Gironès, N.; Fresno, M. Trypanosoma Cruzi Infection and Endothelin-1 Cooperatively Activate Pathogenic Inflammatory Pathways in Cardiomyocytes. PLoS Negl. Trop. Dis. 2013, 7, e2034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashton, A.W.; Mukherjee, S.; Nagajyothi, F.; Huang, H.; Braunstein, V.L.; Desruisseaux, M.S.; Factor, S.M.; Lopez, L.; Berman, J.W.; Wittner, M.; et al. Thromboxane A2 Is a Key Regulator of Pathogenesis during Trypanosoma Cruzi Infection. J. Exp. Med. 2007, 204, 929–940. [Google Scholar] [CrossRef]
- Roffê, E.; Souza, A.L.S.; Machado, P.P.; Barcelos, L.S.; Romanha, A.J.; Mariano, F.S.; Silva, J.S.; Machado, C.R.; Tanowitz, H.B.; Teixeira, M.M. Endothelin-1 Receptors Play a Minor Role in the Protection against Acute Trypanosoma Cruzi Infection in Mice. Braz. J. Med. Biol. Res. 2007, 40, 391–399. [Google Scholar] [CrossRef]
- Bonney, K.M.; Engman, D.M. Autoimmune Pathogenesis of Chagas Heart Disease. Am. J. Pathol. 2015, 185, 1537–1547. [Google Scholar] [CrossRef] [Green Version]
- Soares, M.B.P.; Pontes-De-Carvalho, L.; Ribeiro-Dos-Santos, R. The Pathogenesis of Chagas’ Disease: When Autoimmune and Parasite-Specific Immune Responses Meet. An. Acad. Bras. Ciênc. 2001, 73, 547–559. [Google Scholar] [CrossRef] [Green Version]
- Dávila, D.F.; Donis, J.H.; Arata de Bellabarba, G.; Villarroel, V.; Sanchez, F.; Berrueta, L.; Salmen, S.; Das Neves, B. Cardiac Autonomic Control Mechanisms in the Pathogenesis of Chagas’ Heart Disease. Interdiscip. Perspect. Infect. Dis. 2012, 2012, 980739. [Google Scholar] [CrossRef]
- Amorim, D.D.S.; Marin Neto, J.A. Functional Alterations of the Autonomic Nervous System in Chagas’ Heart Disease. Sao Paulo Med. J. 1995, 113, 772–784. [Google Scholar] [CrossRef]
- de Cuba, M.B.; Ribeiro Machado, M.P.; Farnesi, T.S.; Alves, A.C.; Martins, L.A.; de Oliveira, L.F.; Capitelli, C.S.; Leite, C.F.; Vinícius Silva, M.; Machado, J.R.; et al. Effects of Cholinergic Stimulation with Pyridostigmine Bromide on Chronic Chagasic Cardiomyopathic Mice. Mediat. Inflamm. 2014, 2014, 475946. [Google Scholar] [CrossRef]
- Rassi, A.; Rassi, A.; Rassi, S.G. Predictors of Mortality in Chronic Chagas Disease: A Systematic Review of Observational Studies. Circulation 2007, 115, 1101–1108. [Google Scholar] [CrossRef] [Green Version]
- Dobarro, D.; Gomez-Rubin, C.; Sanchez-Recalde, A.; Olias, F.; Bret-Zurita, M.; Cuesta-Lopez, E.; Robles-Marhuenda, A.; Fraile-Vicente, J.M.; Paño-Pardo, J.R.; Lopez-Sendon, J. Chagas’ Heart Disease in Europe: An Emergent Disease? J. Cardiovasc. Med. 2008, 9, 1263–1267. [Google Scholar] [CrossRef]
- Rassi, A.; de Rezende, J.M.; Luquetti, A.O.; Rassi, A. Clinical Phases and Forms of Chagas Disease. In American Trypanosomiasis Chagas Disease; Elsevier: Amsterdam, The Netherlands, 2017; pp. 653–686. ISBN 978-0-12-801029-7. [Google Scholar]
- Punukollu, G.; Gowda, R.M.; Khan, I.A.; Navarro, V.S.; Vasavada, B.C. Clinical Aspects of the Chagas’ Heart Disease. Int. J. Cardiol. 2007, 115, 279–283. [Google Scholar] [CrossRef]
- Pérez-Molina, J.A.; Molina, I. Chagas Disease. Lancet 2018, 391, 82–94. [Google Scholar] [CrossRef]
- Schild, D.; Fankhauser, R.; Arenja, N.; Novak, J. A Rare Cause of Dilated Cardiomyopathy in Switzerland Chagas Heart Disease. Cardiovasc. Med. 2018, 21, 316–321. [Google Scholar] [CrossRef] [Green Version]
- Gascón, J.; Albajar, P.; Cañas, E.; Flores, M.; Gómez i Prat, J.; Herrera, R.N.; Lafuente, C.A.; Luciardi, H.L.; Moncayo, Á.; Molina, L.; et al. Diagnóstico, manejo y tratamiento de la cardiopatía chagásica crónica en áreas donde la infección por Trypanosoma cruzi no es endémica. Enferm. Infecc. Microbiol. Clínica 2008, 26, 99–106. [Google Scholar] [CrossRef]
- Hasslocher-Moreno, A.M.; Salles Xavier, S.; Magalhães Saraiva, R.; Conde Sangenis, L.H.; Teixeira de Holanda, M.; Horta Veloso, H.; Rodrigues da Costa, A.; de Souza Nogueira Sardinha Mendes, F.; Alvarenga Americano do Brasil, P.E.; Sperandio da Silva, G.M.; et al. Progression Rate from the Indeterminate Form to the Cardiac Form in Patients with Chronic Chagas Disease: Twenty-Two-Year Follow-Up in a Brazilian Urban Cohort. Trop. Med. 2020, 5, 76. [Google Scholar] [CrossRef]
- Nunes, M.C.P.; Dones, W.; Morillo, C.A.; Encina, J.J.; Ribeiro, A.L. Chagas Disease. J. Am. Coll. Cardiol. 2013, 62, 767–776. [Google Scholar] [CrossRef]
- Reis Lopes, E.; Chapadeiro, E.; Araújo Andrade, Z.; de Oliveira Almeida, H.; Rocha, A. Anatomo-pathology of heart of asymptomatic chagas’ patients who had a violent death. Mem. Ins. Oswaldo Cruz 1981, 76, 189–197. [Google Scholar] [CrossRef]
- Añez, N.; Carrasco, H.; Crisante, G.; Rojas, A.; Fuenmayor, C.; Gonzlaez, N.; Percoco, G.; Borges, R.; Guevara, P.; Ramirez, J.L. Myocardial Parasite Persistence in Chronic Chagasic Patients. Am. J. Trop. Med. Hyg. 1999, 60, 726–732. [Google Scholar] [CrossRef] [Green Version]
- Dias, J.C.P. The Indeterminate Form of Human Chronic Chagas’ Disease: A Clinical Epidemological Review. Rev. Soc. Bras. Med. Trop. 1989, 22, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.; Dias Romano, M.M.; Marin-Neto, J.A.; Rao-Melacini, P.; Rassi, A.; Mattos, A.; Avezum, Á.; Villena, E.; Sosa-Estani, S.; Bonilla, R.; et al. Effects of Trypanocidal Treatment on Echocardiographic Parameters in Chagas Cardiomyopathy and Prognostic Value of Wall Motion Score Index: A BENEFIT Trial Echocardiographic Substudy. J. Am. Soc. Echocardiogr. 2019, 32, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Marin-Neto, J.A.; de Almeida Filho, O.C.; Pazin-Filho, A.; Maciel, B.C. Forma Indeterminada da Moléstia de Chagas: Proposta de Novos Critérios de Caracterização e Perspectivas de Tratamento Precoce da Cardiomiopatia. Arq. Bras. Cardiol. 2002, 79, 623–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scanavacca, M. Epicardial Ablation for Ventricular Tachycardia in Chronic Chagas Heart Disease. Arq. Bras. Cardiol. 2014, 102, 524–528. [Google Scholar] [CrossRef]
- Ribeiro, A.L.; Nunes, M.P.; Teixeira, M.M.; Rocha, M.O.C. Diagnosis and Management of Chagas Disease and Cardiomyopathy. Nat. Rev. Cardiol. 2012, 9, 576–589. [Google Scholar] [CrossRef]
- de Andrade, J.P.; Neto, J.A.M.; Oliveira, G.M.M.; Bacal, F.; Bocchi, E.A.; Almeida, D.R.; Augusto, A.; Filho, F. I Latin American Guidelines for the Diagnosis and Treatment of Chagas’ Heart Disease. Executive Summary. Arq. Bras. Cardiol. 2011, 96, 434–442. [Google Scholar] [CrossRef] [Green Version]
- Luquetti, A.O.; Schmuñis, G.A. Diagnosis of Trypanosoma Cruzi Infection. In American Trypanosomiasis Chagas Disease; Elsevier: Amsterdam, The Netherlands, 2017; pp. 687–730. ISBN 978-0-12-801029-7. [Google Scholar]
- Angheben, A.; Gobbi, F.; Buonfrate, D.; Tais, S.; Degani, M.; Anselmi, M.; Bisoffi, Z. Notes on Rapid Diagnostic Tests for Chronic Chagas Disease. Bull. Soc. Pathol. Exot. 2017, 110, 9–12. [Google Scholar] [CrossRef]
- Figueredo, F.; Stolowicz, F.; Vojnov, A.; Coltro, W.K.T.; Larocca, L.; Carrillo, C.; Cortón, E. Towards a Versatile and Economic Chagas Disease Point-of-Care Testing System, by Integrating Loop-Mediated Isothermal Amplification and Contactless/Label-Free Conductivity Detection. PLoS Negl. Trop. Dis. 2021, 15, e0009406. [Google Scholar] [CrossRef]
- Jimenez-Coello, M.; Shelite, T.; Castellanos-Gonzalez, A.; Saldarriaga, O.; Rivero, R.; Ortega-Pacheco, A.; Acevedo-Arcique, C.; Amaya-Guardia, K.; Garg, N.; Melby, P.; et al. Efficacy of Recombinase Polymerase Amplification to Diagnose Trypanosoma Cruzi Infection in Dogs with Cardiac Alterations from an Endemic Area of Mexico. Vector-Borne Zoonotic Dis. 2018, 18, 417–423. [Google Scholar] [CrossRef]
- Celedon, P.A.F.; Leony, L.M.; Oliveira, U.D.; Freitas, N.E.M.; Silva, Â.A.O.; Daltro, R.T.; Santos, E.F.; Krieger, M.A.; Zanchin, N.I.T.; Santos, F.L.N. Stability Assessment of Four Chimeric Proteins for Human Chagas Disease Immunodiagnosis. Biosensors 2021, 11, 289. [Google Scholar] [CrossRef]
- Cortina, M.E.; Melli, L.J.; Roberti, M.; Mass, M.; Longinotti, G.; Tropea, S.; Lloret, P.; Serantes, D.A.R.; Salomón, F.; Lloret, M.; et al. Electrochemical Magnetic Microbeads-Based Biosensor for Point-of-Care Serodiagnosis of Infectious Diseases. Biosens. Bioelectron. 2016, 80, 24–33. [Google Scholar] [CrossRef]
- Abras, A.; Ballart, C.; Fernández-Arévalo, A.; Llovet, T.; Gállego, M.; Muñoz, C. ARCHITECT Chagas® as a Single Test Candidate for Chagas Disease Diagnosis: Evaluation of Two Algorithms Implemented in a Non-Endemic Setting. Clin. Microbiol. Infect. 2021, 27, 782.e1–782.e6. [Google Scholar] [CrossRef]
- Ghonim, S.; Voges, I.; Gatehouse, P.D.; Keegan, J.; Gatzoulis, M.A.; Kilner, P.J.; Babu-Narayan, S.V. Myocardial Architecture, Mechanics, and Fibrosis in Congenital Heart Disease. Front. Cardiovasc. Med. 2017, 4, 30. [Google Scholar] [CrossRef] [Green Version]
- Pane, S.; Giancola, M.L.; Piselli, P.; Corpolongo, A.; Repetto, E.; Bellagamba, R.; Cimaglia, C.; Carrara, S.; Ghirga, P.; Oliva, A.; et al. Serological Evaluation for Chagas Disease in Migrants from Latin American Countries Resident in Rome, Italy. BMC Infect. Dis. 2018, 18, 212. [Google Scholar] [CrossRef] [Green Version]
- Echeverría, L.E.; Rojas, L.Z.; Calvo, L.S.; Roa, Z.M.; Rueda-Ochoa, O.L.; Morillo, C.A.; Muka, T.; Franco, O.H. Profiles of Cardiovascular Biomarkers According to Severity Stages of Chagas Cardiomyopathy. Int. J. Cardiol. 2017, 227, 577–582. [Google Scholar] [CrossRef]
- Echeverría, L.E.; Rojas, L.Z.; Gómez-Ochoa, S.A.; Rueda-Ochoa, O.L.; Sosa-Vesga, C.D.; Muka, T.; Januzzi, J.L.; Marcus, R.; Morillo, C.A. Cardiovascular Biomarkers as Predictors of Adverse Outcomes in Chronic Chagas Cardiomyopathy. PLoS ONE 2021, 16, e0258622. [Google Scholar] [CrossRef]
- Strauss, D.G.; Cardoso, S.; Lima, J.A.C.; Rochitte, C.E.; Wu, K.C. ECG Scar Quantification Correlates with Cardiac Magnetic Resonance Scar Size and Prognostic Factors in Chagas’ Disease. Heart 2011, 97, 357–361. [Google Scholar] [CrossRef]
- Brito, B.O.D.F.; Ribeiro, A.L.P. Electrocardiogram in Chagas Disease. Rev. Soc. Bras. Med. Trop. 2018, 51, 570–577. [Google Scholar] [CrossRef]
- Guadalajara, J.F. Capítulo 27. Miocarditis. In Cardiología; Méndez Editores: Mexico City, Mexico, 2018; pp. 1048–1049. ISBN 978-607-7659-44-0. [Google Scholar]
- Nascimento, C.A.S.; Gomes, V.A.M.; Silva, S.K.; Santos, C.R.F.; Chambela, M.C.; Madeira, F.S.; Holanda, M.T.; Brasil, P.E.A.A.; Sousa, A.S.; Xavier, S.S.; et al. Left Atrial and Left Ventricular Diastolic Function in Chronic Chagas Disease. J. Am. Soc. Echocardiogr. 2013, 26, 1424–1433. [Google Scholar] [CrossRef] [PubMed]
- Braggion-Santos, M.F.; Moreira, H.T.; Volpe, G.J.; Koenigkam-Santos, M.; Marin-Neto, J.A.; Schmidt, A. Electrocardiogram Abnormalities in Chronic Chagas Cardiomyopathy Correlate with Scar Mass and Left Ventricular Dysfunction as Assessed by Cardiac Magnetic Resonance Imaging. J. Electrocardiol. 2022, 72, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, B.R.; Araújo, C.G.; Rocha, M.O.C.; Domingues, J.D.P.; Rodrigues, A.B.; Barros, M.V.L.; Ribeiro, A.L.P. The Prognostic Significance of Electrocardiographic Changes in Chagas Disease. J. Electrocardiol. 2012, 45, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Maguire, J.H.; Hoff, R.; Sherlock, I.; Guimarães, A.C.; Sleigh, A.C.; Ramos, N.B.; Mott, K.E.; Weller, T.H. Cardiac Morbidity and Mortality Due to Chagas’ Disease: Prospective Electrocardiographic Study of a Brazilian Community. Circulation 1987, 75, 1140–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salles, G.; Xavier, S.; Sousa, A.; Hasslocher-Moreno, A.; Cardoso, C. Prognostic Value of QT Interval Parameters for Mortality Risk Stratification in Chagas’ Disease: Results of a Long-Term Follow-Up Study. Circulation 2003, 108, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Salles, G.F.; Xavier, S.S.; Sousa, A.S.; Hasslocher-Moreno, A.; Cardoso, C.R.L. T-Wave Axis Deviation as an Independent Predictor of Mortality in Chronic Chagas’ Disease. Am. J. Cardiol. 2004, 93, 1136–1140. [Google Scholar] [CrossRef]
- Acquatella, H.; Asch, F.M.; Barbosa, M.M.; Barros, M.; Bern, C.; Cavalcante, J.L.; Echeverria Correa, L.E.; Lima, J.; Marcus, R.; Marin-Neto, J.A.; et al. Recommendations for Multimodality Cardiac Imaging in Patients with Chagas Disease: A Report from the American Society of Echocardiography in Collaboration with the InterAmerican Association of Echocardiography (ECOSIAC) and the Cardiovascular Imaging Department of the Brazilian Society of Cardiology (DIC-SBC). J. Am. Soc. Echocardiogr. 2018, 31, 3–25. [Google Scholar] [CrossRef] [Green Version]
- Acquatella, H. Echocardiography in Chagas Heart Disease. Circulation 2007, 115, 1124–1131. [Google Scholar] [CrossRef]
- Moll-Bernardes, R.J.; Rosado-de-Castro, P.H.; Camargo, G.C.; Mendes, F.S.N.S.; Brito, A.S.X.; Sousa, A.S. New Imaging Parameters to Predict Sudden Cardiac Death in Chagas Disease. Trop. Med. Infect. Dis. 2020, 5, 74. [Google Scholar] [CrossRef]
- Hiss, F.C.; Lascala, T.F.; Maciel, B.C.; Marin-Neto, J.A.; Simões, M.V. Changes in Myocardial Perfusion Correlate with Deterioration of Left Ventricular Systolic Function in Chronic Chagas’ Cardiomyopathy. JACC Cardiovasc. Imaging 2009, 2, 164–172. [Google Scholar] [CrossRef]
- Nunes, M.C.P.; Badano, L.P.; Marin-Neto, J.A.; Edvardsen, T.; Fernández-Golfín, C.; Bucciarelli-Ducci, C.; Popescu, B.A.; Underwood, R.; Habib, G.; Zamorano, J.L.; et al. Multimodality Imaging Evaluation of Chagas Disease: An Expert Consensus of Brazilian Cardiovascular Imaging Department (DIC) and the European Association of Cardiovascular Imaging (EACVI). Eur. Heart J.-Cardiovasc. Imaging 2018, 19, 459–460n. [Google Scholar] [CrossRef]
- Volpe, G.J.; Moreira, H.T.; Trad, H.S.; Wu, K.C.; Braggion-Santos, M.F.; Santos, M.K.; Maciel, B.C.; Pazin-Filho, A.; Marin-Neto, J.A.; Lima, J.A.C.; et al. Left Ventricular Scar and Prognosis in Chronic Chagas Cardiomyopathy. J. Am. Coll. Cardiol. 2018, 72, 2567–2576. [Google Scholar] [CrossRef]
- Hundley, W.G.; Bluemke, D.A.; Finn, J.P.; Flamm, S.D.; Fogel, M.A.; Friedrich, M.G.; Ho, V.B.; Jerosch-Herold, M.; Kramer, C.M.; Manning, W.J.; et al. ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance: A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J. Am. Coll. Cardiol. 2010, 55, 2614–2662. [Google Scholar] [CrossRef]
- Rochitte, C.E.; Oliveira, P.F.; Andrade, J.M.; Ianni, B.M.; Parga, J.R.; Ávila, L.F.; Kalil-Filho, R.; Mady, C.; Meneghetti, J.C.; Lima, J.A.C.; et al. Myocardial Delayed Enhancement by Magnetic Resonance Imaging in Patients with Chagas’ Disease. J. Am. Coll. Cardiol. 2005, 46, 1553–1558. [Google Scholar] [CrossRef] [Green Version]
- Moreira, H.T.; Volpe, G.J.; Marin-Neto, J.A.; Ambale-Venkatesh, B.; Nwabuo, C.C.; Trad, H.S.; Romano, M.M.D.; Pazin-Filho, A.; Maciel, B.C.; Lima, J.A.C.; et al. Evaluation of Right Ventricular Systolic Function in Chagas Disease Using Cardiac Magnetic Resonance Imaging. Circ. Cardiovasc. Imaging 2017, 10, e005571. [Google Scholar] [CrossRef] [Green Version]
- Simões, M.V.; Tanaka, D.M.; Marin-Neto, J.A. Nuclear Medicine Methods for Assessment of Chronic Chagas Heart Disease. Int. J. Cardiovasc. Sci. 2020, 33, 686–696. [Google Scholar] [CrossRef]
- Miranda, C.H.; Figueiredo, A.B.; Maciel, B.C.; Marin-Neto, J.A.; Simões, M.V. Sustained Ventricular Tachycardia Is Associated with Regional Myocardial Sympathetic Denervation Assessed with 123 I-Metaiodobenzylguanidine in Chronic Chagas Cardiomyopathy. J. Nucl. Med. 2011, 52, 504–510. [Google Scholar] [CrossRef] [Green Version]
- Busse, A.; Rajagopal, R.; Yücel, S.; Beller, E.; Öner, A.; Streckenbach, F.; Cantré, D.; Ince, H.; Weber, M.-A.; Meinel, F.G. Cardiac MRI—Update 2020. Radiologe 2020, 60, 33–40. [Google Scholar] [CrossRef]
- Apt, W. Treatment of Chagas Disease. In American Trypanosomiasis Chagas Disease; Elsevier: Amsterdam, The Netherlands, 2017; pp. 751–771. ISBN 978-0-12-801029-7. [Google Scholar]
- Monge-Maillo, B.; López-Vélez, R. Challenges in the Management of Chagas Disease in Latin-American Migrants in Europe. Clin. Microbiol. Infect. 2017, 23, 290–295. [Google Scholar] [CrossRef] [Green Version]
- Villar, J.C.; Herrera, V.M.; Pérez Carreño, J.G.; Váquiro Herrera, E.; Castellanos Domínguez, Y.Z.; Vásquez, S.M.; Cucunubá, Z.M.; Prado, N.G.; Hernández, Y. Nifurtimox versus Benznidazole or Placebo for Asymptomatic Trypanosoma Cruzi Infection (Equivalence of Usual Interventions for Trypanosomiasis–EQUITY): Study Protocol for a Randomised Controlled Trial. Trials 2019, 20, 431. [Google Scholar] [CrossRef] [Green Version]
- Morillo, C.A.; Marin-Neto, J.A.; Avezum, A.; Sosa-Estani, S.; Rassi, A.; Rosas, F.; Villena, E.; Quiroz, R.; Bonilla, R.; Britto, C.; et al. Randomized Trial of Benznidazole for Chronic Chagas’ Cardiomyopathy. N. Engl. J. Med. 2015, 373, 1295–1306. [Google Scholar] [CrossRef] [PubMed]
- Camandaroba, E.L.P.; Reis, E.A.G.; Gonçalves, M.S.; Reis, M.G.; Andrade, S.G. Trypanosoma Cruzi: Susceptibility to Chemotherapy with Benznidazole of Clones Isolated from the Highly Resistant Colombian Strain. Rev. Soc. Bras. Med. Trop. 2003, 36, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Veloso, V.; Carneiro, C.; Toledo, M.; Lana, M.; Chiari, E.; Tafuri, W.; Bahia, M. Variation in Susceptibility to Benznidazole in Isolates Derived from Trypanosoma Cruzi Parental Strains. Mem. Inst. Oswaldo Cruz 2001, 96, 1005–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zingales, B.; Miles, M.A.; Moraes, C.B.; Luquetti, A.; Guhl, F.; Schijman, A.G.; Ribeiro, I. Drug Discovery for Chagas Disease Should Consider Trypanosoma Cruzi Strain Diversity. Mem. Inst. Oswaldo Cruz 2014, 109, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.D.F.; Nagao-Dias, A.T.; Oliveira de Pontes, V.M.; de Souza Júnior, A.S.; Luna Coelho, H.L.; Branco Coelho, I.C. Tratamento etiológico da doença de Chagas no Brasil. Rev. Patol. Trop. 2008, 37, 209–228. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Ayala, A.; Pérez-Molina, J.A.; Norman, F.; Navarro, M.; Monge-Maillo, B.; Díaz-Menéndez, M.; Peris-García, J.; Flores, M.; Cañavate, C.; López-Vélez, R. Chagas Disease in Latin American Migrants: A Spanish Challenge. Clin. Microbiol. Infect. 2011, 17, 1108–1113. [Google Scholar] [CrossRef] [Green Version]
- Viotti, R.; Vigliano, C.; Lococo, B.; Alvarez, M.G.; Petti, M.; Bertocchi, G.; Armenti, A. Side Effects of Benznidazole as Treatment in Chronic Chagas Disease: Fears and Realities. Expert Rev. Anti-Infect. Ther. 2009, 7, 157–163. [Google Scholar] [CrossRef]
- Morillo, C.A.; Waskin, H.; Sosa-Estani, S.; del Carmen Bangher, M.; Cuneo, C.; Milesi, R.; Mallagray, M.; Apt, W.; Beloscar, J.; Gascon, J.; et al. Benznidazole and Posaconazole in Eliminating Parasites in Asymptomatic T. Cruzi Carriers. J. Am. Coll. Cardiol. 2017, 69, 939–947. [Google Scholar] [CrossRef]
- Torrico, F.; Gascón, J.; Ortiz, L.; Pinto, J.; Rojas, G.; Palacios, A.; Barreira, F.; Blum, B.; Schijman, A.G.; Vaillant, M.; et al. A Phase 2, Randomized, Multicenter, Placebo-Controlled, Proof-of-Concept Trial of Oral Fexinidazole in Adults with Chronic Indeterminate Chagas Disease. Clin. Infect. Dis. 2022, 8, ciac579. [Google Scholar] [CrossRef]
- Urbina, J.A. Ergosterol Biosynthesis and Drug Development for Chagas Disease. Mem. Inst. Oswaldo Cruz 2009, 104, 311–318. [Google Scholar] [CrossRef] [Green Version]
- Mazzeti, A.L.; Diniz, L.D.F.; Gonçalves, K.R.; WonDollinger, R.S.; Assíria, T.; Ribeiro, I.; Bahia, M.T. Synergic Effect of Allopurinol in Combination with Nitroheterocyclic Compounds against Trypanosoma Cruzi. Antimicrob. Agents Chemother. 2019, 63, e02264-18. [Google Scholar] [CrossRef]
- Apt, W.; Arribada, A.; Zulantay, I.; Sanchez, G.; Vargas, S.L.; Rodriguez, J. Itraconazole or Allopurinol in the Treatment of Chronic American Trypanosomiasis: The Regression and Prevention of Electrocardiographic Abnormalities during 9 Years of Follow-Up. Ann. Trop. Med. Parasitol. 2003, 97, 23–29. [Google Scholar] [CrossRef]
- Rassi, A.; Luquetti, A.O.; Rassi, A., Jr.; Rassi, G.G.; Rassi, S.G.; Silva, I.G.D.; Rassi, A.G. Short report: Specific treatment for Trypanosoma Cruzi: Lack of efficacy of allopurinol in the human chronic phase of chagas disease. Am. J. Trop. Med. Hyg. 2007, 76, 4. [Google Scholar] [CrossRef] [Green Version]
- Moraes, C.B.; Giardini, M.A.; Kim, H.; Franco, C.H.; Araujo-Junior, A.M.; Schenkman, S.; Chatelain, E.; Freitas-Junior, L.H. Nitroheterocyclic Compounds Are More Efficacious than CYP51 Inhibitors against Trypanosoma Cruzi: Implications for Chagas Disease Drug Discovery and Development. Sci. Rep. 2015, 4, 4703. [Google Scholar] [CrossRef] [Green Version]
- Weniger, B.; Robledo, S.; Arango, G.J.; Deharo, E.; Aragón, R.; Muñoz, V.; Callapa, J.; Lobstein, A.; Anton, R. Antiprotozoal Activities of Colombian Plants. J. Ethnopharmacol. 2001, 78, 193–200. [Google Scholar] [CrossRef]
- Meira, C.S.; Guimarães, E.T.; dos Santos, J.A.F.; Moreira, D.R.M.; Nogueira, R.C.; Tomassini, T.C.B.; Ribeiro, I.M.; de Souza, C.V.C.; Ribeiro dos Santos, R.; Soares, M.B.P. In Vitro and in Vivo Antiparasitic Activity of Physalis Angulata, L. Concentrated Ethanolic Extract against Trypanosoma Cruzi. Phytomedicine 2015, 22, 969–974. [Google Scholar] [CrossRef]
- Sosa, A.; Salamanca Capusiri, E.; Amaya, S.; Bardón, A.; Giménez-Turba, A.; Vera, N.; Borkosky, S. Trypanocidal Activity of South American Vernonieae (Asteraceae) Extracts and Its Sesquiterpene Lactones. Nat. Prod. Res. 2021, 35, 5224–5228. [Google Scholar] [CrossRef]
- Abe, F.; Nagafuji, S.; Okawa, M.; Kinjo, J.; Akahane, H.; Ogura, T.; Martinez-Alfaro, M.A.; Reyes-Chilpa, R. Trypanocidal Constituents in Plants 5. Evaluation of Some Mexican Plants for Their Trypanocidal Activity and Active Constituents in the Seeds of Persea Americana. Biol. Pharm. Bull. 2005, 28, 1314–1317. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Coello, M.; Guzman-Marín, E.; Ortega-Pacheco, A.; Perez-Gutiérrez, S.; Acosta-Viana, K. Assessment of the Anti-Protozoal Activity of Crude Carica Papaya Seed Extract against Trypanosoma Cruzi. Molecules 2013, 18, 12621–12632. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, M.P.T.; do Carmo, A.A.L.; Rocha, M.O.D.C.; Ribeiro, A.L.P. Ventricular Arrhythmias in Chagas Disease. Rev. Soc. Bras. Med. Trop. 2015, 48, 4–10. [Google Scholar] [CrossRef] [Green Version]
- McMurray, J.J.V.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin–Neprilysin Inhibition versus Enalapril in Heart Failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Ramires, F.J.A.; Martinez, F.; Gómez, E.A.; Demacq, C.; Gimpelewicz, C.R.; Rouleau, J.L.; Solomon, S.D.; Swedberg, K.; Zile, M.R.; Packer, M.; et al. Post Hoc Analyses of SHIFT and PARADIGM-HF Highlight the Importance of Chronic Chagas’ Cardiomyopathy Comment on: “Safety Profile and Efficacy of Ivabradine in Heart Failure Due to Chagas Heart Disease: A Post Hoc Analysis of the SHIFT Trial” by Bocchi et: Correspondence. ESC Heart Fail. 2018, 5, 1069–1071. [Google Scholar] [CrossRef] [PubMed]
- Bocchi, E.A.; Rassi, S.; Veiga Guimarães, G. Argentine, Chile, and Brazil SHIFT Investigators Reply: Sacubitril/Valsartan for Chagas’ Heart Disease Heart Failure? Reply: Sacubitril/Valsartan for Chagas’ Heart Disease Heart Failure? ESC Heart Fail. 2018, 5, 1072–1073. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo, C.S.; Melo, R.M.V.; Viana, T.T.; Jesus, A.G.Q.; Silva, T.C.; Silva, V.M.; Carvalho, W.N.; Silva, D.N.V.; Passos, L.C.S. Clinical and Echocardiographic Characteristics after Six Months of Sacubitril/Valsartan in Chagas Heart Disease–A Case Series. Brit. J. Clin. Pharma. 2022, 88, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, S.S.; Felizardo, A.A.; Caldas, I.S.; Gonçalves, R.V.; Novaes, R.D. Challenges of Immunosuppressive and Antitrypanosomal Drug Therapy after Heart Transplantation in Patients with Chronic Chagas Disease: A Systematic Review of Clinical Recommendations. Transplant. Rev. 2018, 32, 157–167. [Google Scholar] [CrossRef]
- Magarakis, M.; Macias, A.E.; Tompkins, B.A.; Reis, V.; Loebe, M.; Batista, R.; Salerno, T.A. Cardiac Surgery for Chagas Disease. J. Card. Surg. 2018, 33, 597–602. [Google Scholar] [CrossRef]
- Moreira, M.D.C.V.; Renan Cunha-Melo, J. Chagas Disease Infection Reactivation after Heart Transplant. Trop. Med. Infect. Dis. 2020, 5, 106. [Google Scholar] [CrossRef]
- Rodríguez-Morales, O.; Monteón-Padilla, V.; Carrillo-Sánchez, S.C.; Rios-Castro, M.; Martínez-Cruz, M.; Carabarin-Lima, A.; Arce-Fonseca, M. Experimental Vaccines against Chagas Disease: A Journey through History. J. Immunol. Res. 2015, 2015, 489758. [Google Scholar] [CrossRef]
- Barbosa, M.P.T.; da Costa Rocha, M.O.; de Oliveira, A.B.; Lombardi, F.; Ribeiro, A.L.P. Efficacy and Safety of Implantable Cardioverter-Defibrillators in Patients with Chagas Disease. EP Eur. 2013, 15, 957–962. [Google Scholar] [CrossRef] [Green Version]
- Arce-Fonseca, M.; Rios-Castro, M.; Carrillo-Sánchez, S.; Martínez-Cruz, M.; Rodríguez-Morales, O. Prophylactic and Therapeutic DNA Vaccines against Chagas Disease. Parasites Vectors 2015, 8, 121. [Google Scholar] [CrossRef] [Green Version]
- Arce-Fonseca, M.; Carbajal-Hernández, A.C.; Lozano-Camacho, M.; Carrillo-Sánchez, S.D.C.; Roldán, F.-J.; Aranda-Fraustro, A.; Rosales-Encina, J.L.; Rodríguez-Morales, O. DNA Vaccine Treatment in Dogs Experimentally Infected with Trypanosoma Cruzi. J. Immunol. Res. 2020, 2020, 9794575. [Google Scholar] [CrossRef]
- Rodríguez-Morales, O.; Roldán, F.-J.; Vargas-Barrón, J.; Parra-Benítez, E.; Medina-García, M.D.L.; Vergara-Bello, E.; Arce-Fonseca, M. Echocardiographic Findings in Canine Model of Chagas Disease Immunized with DNA Trypanosoma Cruzi Genes. Animals 2020, 10, 648. [Google Scholar] [CrossRef] [Green Version]
- Arce-Fonseca, M.; González-Vázquez, M.C.; Rodríguez-Morales, O.; Graullera-Rivera, V.; Aranda-Fraustro, A.; Reyes, P.A.; Carabarin-Lima, A.; Rosales-Encina, J.L. Recombinant Enolase of Trypanosoma Cruzi as a Novel Vaccine Candidate against Chagas Disease in a Mouse Model of Acute Infection. J. Immunol. Res. 2018, 2018, 8964085. [Google Scholar] [CrossRef] [Green Version]
- Salgado-Jiménez, B.; Arce-Fonseca, M.; Baylón-Pacheco, L.; Talamás-Rohana, P.; Rosales-Encina, J.L. Differential Immune Response in Mice Immunized with the A, R or C Domain from TcSP Protein of Trypanosoma Cruzi or with the Coding DNAs. Parasite Immunol. 2013, 35, 32–41. [Google Scholar] [CrossRef]
- Arce-Fonseca, M.; Ramos-Ligonio, A.; López-Monteón, A.; Salgado-Jiménez, B.; Talamás-Rohana, P.; Rosales-Encina, J.L. A DNA Vaccine Encoding for Tc SSP4 Induces Protection against Acute and Chronic Infection in Experimental Chagas Disease. Int. J. Biol. Sci. 2011, 7, 1230–1238. [Google Scholar] [CrossRef] [Green Version]
- Arce-Fonseca, M.; Ballinas-Verdugo, M.A.; Zenteno, E.R.A.; Suárez-Flores, D.; Carrillo-Sánchez, S.C.; Alejandre-Aguilar, R.; Rosales-Encina, J.L.; Reyes, P.A.; Rodríguez-Morales, O. Specific Humoral and Cellular Immunity Induced by Trypanosoma Cruzi DNA Immunization in a Canine Model. Vet. Res. 2013, 44, 15. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Morales, O.; Pérez-Leyva, M.M.; Ballinas-Verdugo, M.A.; Carrillo-Sánchez, S.C.; Rosales-Encina, J.L.; Alejandre-Aguilar, R.; Reyes, P.A.; Arce-Fonseca, M. Plasmid DNA Immunization with Trypanosoma Cruzi Genes Induces Cardiac and Clinical Protection against Chagas Disease in the Canine Model. Vet. Res. 2012, 43, 79. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Morales, O.; Carrillo-Sánchez, S.C.; García-Mendoza, H.; Aranda-Fraustro, A.; Ballinas-Verdugo, M.A.; Alejandre-Aguilar, R.; Rosales-Encina, J.L.; Vallejo, M.; Arce-Fonseca, M. Effect of the Plasmid-DNA Vaccination on Macroscopic and Microscopic Damage Caused by the Experimental Chronic Trypanosoma Cruzi Infection in the Canine Model. BioMed. Res. Int. 2013, 2013, 826570. [Google Scholar] [CrossRef] [Green Version]
- Nogueira, R.T.; Nogueira, A.R.; Pereira, M.C.S.; Rodrigues, M.M.; Neves, P.C.D.C.; Galler, R.; Bonaldo, M.C. Recombinant Yellow Fever Viruses Elicit CD8+ T Cell Responses and Protective Immunity against Trypanosoma Cruzi. PLoS ONE 2013, 8, e59347. [Google Scholar] [CrossRef]
- Dumonteil, E.; Bottazzi, M.E.; Zhan, B.; Heffernan, M.J.; Jones, K.; Valenzuela, J.G.; Kamhawi, S.; Ortega, J.; Rosales, S.P.D.L.; Lee, B.Y.; et al. Accelerating the Development of a Therapeutic Vaccine for Human Chagas Disease: Rationale and Prospects. Expert Rev. Vaccines 2012, 11, 1043–1055. [Google Scholar] [CrossRef] [Green Version]
- Aparicio-Burgos, J.E.; Ochoa-García, L.; Zepeda-Escobar, J.A.; Gupta, S.; Dhiman, M.; Martínez, J.S.; de Oca-Jiménez, R.M.; Arreola, M.V.; Barbabosa-Pliego, A.; Vázquez-Chagoyán, J.C.; et al. Testing the Efficacy of a Multi-Component DNA-Prime/DNA-Boost Vaccine against Trypanosoma Cruzi Infection in Dogs. PLoS Negl. Trop. Dis. 2011, 5, e1050. [Google Scholar] [CrossRef] [PubMed]
- Rigato, P.O.; de Alencar, B.C.; de Vasconcelos, J.R.C.; Dominguez, M.R.; Araújo, A.F.; Machado, A.V.; Gazzinelli, R.T.; Bruna-Romero, O.; Rodrigues, M.M. Heterologous Plasmid DNA Prime-Recombinant Human Adenovirus 5 Boost Vaccination Generates a Stable Pool of Protective Long-Lived CD8 + T Effector Memory Cells Specific for a Human Parasite, Trypanosoma Cruzi. Infect. Immun. 2011, 79, 2120–2130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cazorla, S.I.; Becker, P.D.; Frank, F.M.; Ebensen, T.; Sartori, M.J.; Corral, R.S.; Malchiodi, E.L.; Guzmán, C.A. Oral Vaccination with Salmonella Enterica as a Cruzipain-DNA Delivery System Confers Protective Immunity against Trypanosoma Cruzi. Infect. Immun. 2008, 76, 324–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatia, V.; Garg, N.J. Previously Unrecognized Vaccine Candidates Control Trypanosoma Cruzi Infection and Immunopathology in Mice. Clin. Vaccine Immunol. 2008, 15, 1158–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Burgos, G.; Mezquita-Vega, R.G.; Escobedo-Ortegon, J.; Ramirez-Sierra, M.J.; Arjona-Torres, A.; Ouaissi, A.; Rodrigues, M.M.; Dumonteil, E. Comparative Evaluation of Therapeutic DNA Vaccines against Trypanosoma Cruzi in Mice. FEMS Immunol. Med. Microbiol. 2007, 50, 333–341. [Google Scholar] [CrossRef] [Green Version]
- Mussalem, J.S.; Vasconcelos, J.R.C.; Squaiella, C.C.; Ananias, R.Z.; Braga, E.G.; Rodrigues, M.M.; Longo-Maugéri, I.M. Adjuvant Effect of the Propionibacterium Acnes and Its Purified Soluble Polysaccharide on the Immunization with Plasmidial DNA Containing a Trypanosoma Cruzi Gene. Microbiol. Immunol. 2006, 50, 253–263. [Google Scholar] [CrossRef]
- García, G.A.; Arnaiz, M.R.; Laucella, S.A.; Esteva, M.I.; Ainciart, N.; Riarte, A.; Garavaglia, P.A.; Fichera, L.E.; Ruiz, A.M. Immunological and Pathological Responses in BALB/c Mice Induced by Genetic Administration of Tc 13 Tul Antigen of Trypanosoma Cruzi. Parasitology 2006, 132, 855–866. [Google Scholar] [CrossRef]
- Morell, M.; Thomas, M.C.; Caballero, T.; Alonso, C.; López, M.C. The Genetic Immunization with Paraflagellar Rod Protein-2 Fused to the HSP70 Confers Protection against Late Trypanosoma Cruzi Infection. Vaccine 2006, 24, 7046–7055. [Google Scholar] [CrossRef]
- Roffê, E.; Souza, A.L.S.; Caetano, B.C.; Machado, P.P.; Barcelos, L.S.; Russo, R.C.; Santiago, H.C.; Souza, D.G.; Pinho, V.; Tanowitz, H.B.; et al. A DNA Vaccine Encoding CCL4/MIP-1β Enhances Myocarditis in Experimental Trypanosoma Cruzi Infection in Rats. Microbes Infect. 2006, 8, 2745–2755. [Google Scholar] [CrossRef]
- Zapata-Estrella, H.; Hummel-Newell, C.; Sanchez-Burgos, G.; Escobedo-Ortegon, J.; Ramirez-Sierra, M.J.; Arjona-Torres, A.; Dumonteil, E. Control of Trypanosoma Cruzi Infection and Changes in T-Cell Populations Induced by a Therapeutic DNA Vaccine in Mice. Immunol. Lett. 2006, 103, 186–191. [Google Scholar] [CrossRef]
- Miyahira, Y.; Takashima, Y.; Kobayashi, S.; Matsumoto, Y.; Takeuchi, T.; Ohyanagi-Hara, M.; Yoshida, A.; Ohwada, A.; Akiba, H.; Yagita, H.; et al. Immune Responses against a Single CD8+-T-Cell Epitope Induced by Virus Vector Vaccination Can Successfully Control Trypanosoma Cruzi Infection. Infect. Immun. 2005, 73, 10. [Google Scholar] [CrossRef]
- Dumonteil, E.; Escobedo-Ortegon, J.; Reyes-Rodriguez, N.; Arjona-Torres, A.; Ramirez-Sierra, M.J. Immunotherapy of Trypanosoma Cruzi Infection with DNA Vaccines in Mice. Infect. Immun. 2004, 72, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Fralish, B.H.; Tarleton, R.L. Genetic Immunization with LYT1 or a Pool of Trans-Sialidase Genes Protects Mice from Lethal Trypanosoma Cruzi Infection. Vaccine 2003, 21, 3070–3080. [Google Scholar] [CrossRef]
- Miyahira, Y.; Katae, M.; Takeda, K.; Yagita, H.; Okumura, K.; Kobayashi, S.; Takeuchi, T.; Kamiyama, T.; Fukuchi, Y.; Aoki, T. Activation of Natural Killer T Cells by α-Galactosylceramide Impairs DNA Vaccine-Induced Protective Immunity against Trypanosoma Cruzi. Infect. Immun. 2003, 71, 1234–1241. [Google Scholar] [CrossRef] [Green Version]
- Boscardin, S.B.; Kinoshita, S.S.; Fujimura, A.E.; Rodrigues, M.M. Immunization with CDNA Expressed by Amastigotes of Trypanosoma Cruzi Elicits Protective Immune Response against Experimental Infection. Infect. Immun 2003, 71, 2744–2757. [Google Scholar] [CrossRef] [Green Version]
- Garg, N.; Tarleton, R.L. Genetic Immunization Elicits Antigen-Specific Protective Immune Responses and Decreases Disease Severity in Trypanosoma Cruzi Infection. Infect. Immun. 2002, 70, 5547–5555. [Google Scholar] [CrossRef] [Green Version]
- Schnapp, A.R.; Eickhoff, C.S.; Scharfstein, J.; Hoft, D.F. Induction of B- and T-Cell Responses to Cruzipain in the Murine Model of Trypanosoma Cruzi Infection. Microbes Infect. 2002, 4, 805–813. [Google Scholar] [CrossRef]
- Diaz-Hernandez, A.; Gonzalez-Vazquez, M.C.; Arce-Fonseca, M.; Rodríguez-Morales, O.; Cedillo-Ramirez, M.L.; Carabarin-Lima, A. Consensus Enolase of Trypanosoma Cruzi: Evaluation of Their Immunogenic Properties Using a Bioinformatics Approach. Life 2022, 12, 746. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A | B | C | D | |
|---|---|---|---|---|
| Asymptomatic form (indeterminate): no data of cardiac or structural damage (normal ECG and chest X-ray). | Asymptomatic patients with structural or functional cardiomyopathy defined by electrocardiographic or echocardiographic findings | Symptomatic patients with data of previous or current HF. Significant LVEF impairment. | The presence of refractory symptoms secondary to HF, without response to treatment. NYHA (New York Heart Association) functional class IV. Specialized treatment | |
| B 1 | B 2 | |||
| Structural heart disease: mild changes by echocardiogram and ECG (arrhythmias or conduction disorders) Preservation of global ventricular function | Functional heart disease: decreased left ventricular ejection fraction (LVEF) Previously no signs or symptoms of heart failure | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montalvo-Ocotoxtle, I.G.; Rojas-Velasco, G.; Rodríguez-Morales, O.; Arce-Fonseca, M.; Baeza-Herrera, L.A.; Arzate-Ramírez, A.; Meléndez-Ramírez, G.; Manzur-Sandoval, D.; Lara-Romero, M.L.; Reyes-Ortega, A.; et al. Chagas Heart Disease: Beyond a Single Complication, from Asymptomatic Disease to Heart Failure. J. Clin. Med. 2022, 11, 7262. https://doi.org/10.3390/jcm11247262
Montalvo-Ocotoxtle IG, Rojas-Velasco G, Rodríguez-Morales O, Arce-Fonseca M, Baeza-Herrera LA, Arzate-Ramírez A, Meléndez-Ramírez G, Manzur-Sandoval D, Lara-Romero ML, Reyes-Ortega A, et al. Chagas Heart Disease: Beyond a Single Complication, from Asymptomatic Disease to Heart Failure. Journal of Clinical Medicine. 2022; 11(24):7262. https://doi.org/10.3390/jcm11247262
Chicago/Turabian StyleMontalvo-Ocotoxtle, Isis G., Gustavo Rojas-Velasco, Olivia Rodríguez-Morales, Minerva Arce-Fonseca, Luis A. Baeza-Herrera, Arturo Arzate-Ramírez, Gabriela Meléndez-Ramírez, Daniel Manzur-Sandoval, Mayra L. Lara-Romero, Antonio Reyes-Ortega, and et al. 2022. "Chagas Heart Disease: Beyond a Single Complication, from Asymptomatic Disease to Heart Failure" Journal of Clinical Medicine 11, no. 24: 7262. https://doi.org/10.3390/jcm11247262