
Long-Term Follow-Up after Testicular Torsion: Prospective Evaluation of Endocrine and Exocrine Testicular Function, Fertility, Oxidative Stress and Erectile Function
 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Ethics Approval
2.2. Statistics
2.2.1. Comparisons of Two Subgroups
2.2.2. Comparisons of More Than Two Subgroups
3. Results
3.1. Demographic Data—Descriptive Statistics
3.1.1. Family Planning
3.1.2. Erectile Function
3.1.3. Incidental Findings during the Physical Examination
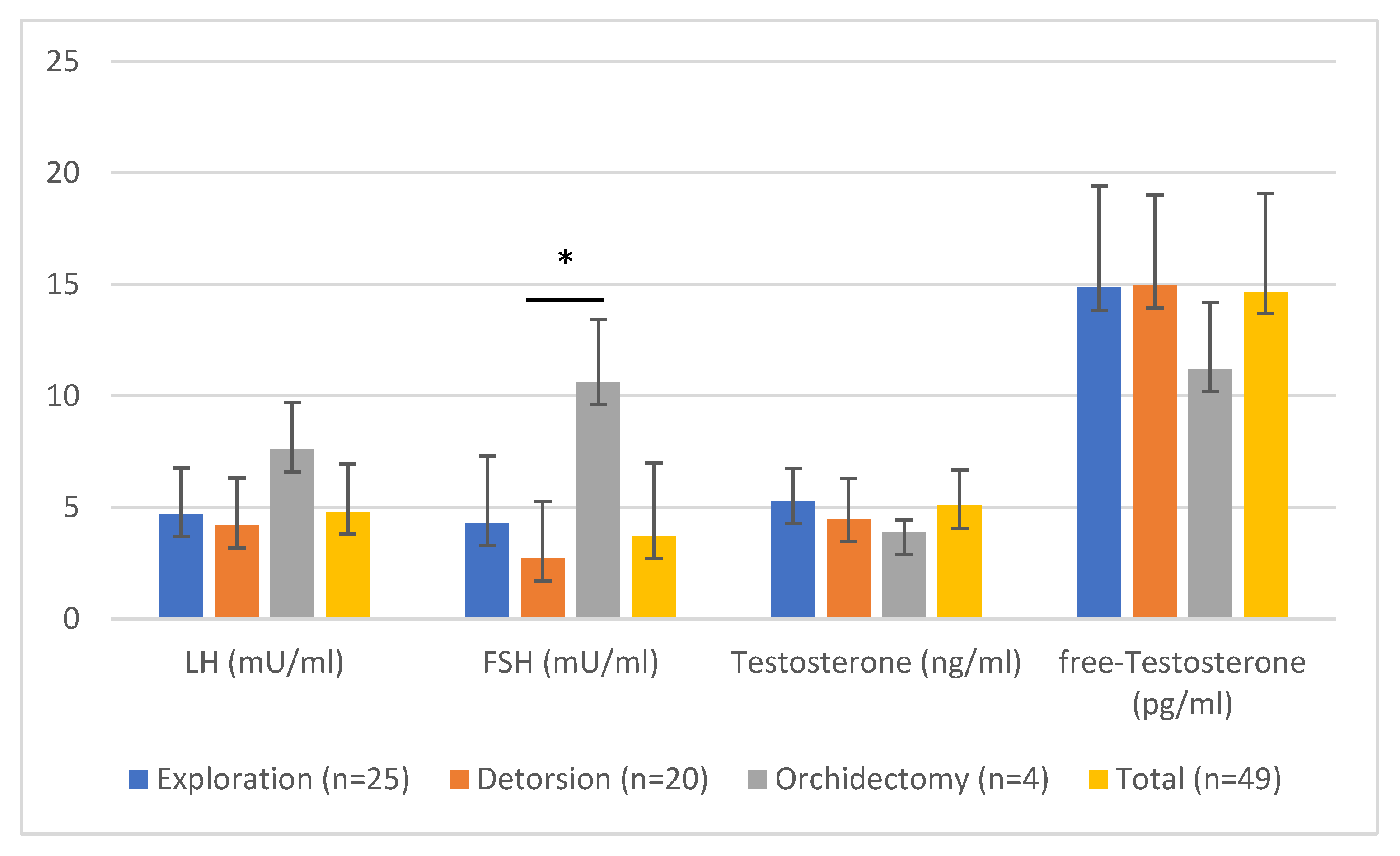
3.1.4. Laboratory Parameters
3.1.5. Semen Parameters
3.2. Comparison of Exploration, Detorsion, and Orchiectomy
Correlation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASA | Anti-sperm antibodies |
| BMI | Body mass index |
| BTB | Blood-testis barrier |
| FSH | Follicle-stimulating hormone |
| fT | Free testosterone |
| IIEF-5 | International Index of Erectile Function |
| LH | Luteinizing hormone |
| MAR-test | Mixed antigen reaction test |
| MyOxSIS | Male infertility Oxidative System |
| OS | Oxidative stress |
| ROS | Reactive oxygen species |
| SD | Standard deviation |
| TT | Testicular torsion |
| WHO | World Health Organization |
References
- Williamson, R.C. Torsion of the testis and allied conditions. Br. J. Surg. 1976, 63, 465–476. [Google Scholar] [CrossRef]
- Yecies, T.; Bandari, J.; Schneck, F.; Cannon, G. Direction of Rotation in Testicular Torsion and Identification of Predictors of Testicular Salvage. Urology 2018, 114, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Watkin, N.A.; Reiger, N.A.; Moisey, C.U. Is the conservative management of the acute scrotum justified on clinical grounds? Br. J. Urol. 1996, 78, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Arap, M.A.; Vicentini, F.C.; Cocuzza, M.; Hallak, J.; Athayde, K.; Lucon, A.M.; Arap, S.; Srougi, M. Late hormonal levels, semen parameters, and presence of antisperm antibodies in patients treated for testicular torsion. J. Androl. 2007, 28, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, G.; Frank, S.; Marberger, H.; Mikuz, G. Testicular torsion: Late results with special regard to fertility and endocrine function. J. Urol. 1980, 124, 375–378. [Google Scholar] [CrossRef]
- Cuckow, P.M.; Frank, J.D. Torsion of the testis. BJU Int. 2000, 86, 349–353. [Google Scholar] [CrossRef]
- Miller, S.R.; Cherrington, N.J. Transepithelial transport across the blood-testis barrier. Reproduction 2018, 156, R187–R194. [Google Scholar] [CrossRef]
- Turner, T.T.; Brown, K.J. Spermatic cord torsion: Loss of spermatogenesis despite return of blood flow. Biol. Reprod. 1993, 49, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Turner, T.T.; Bang, H.J.; Lysiak, J.L. The molecular pathology of experimental testicular torsion suggests adjunct therapy to surgical repair. J. Urol. 2004, 172, 2574–2578. [Google Scholar] [CrossRef]
- Agarwal, A.; Saleh, R.A.; Bedaiwy, M.A. Role of reactive oxygen species in the pathophysiology of human reproduction. Fertil. Steril. 2003, 79, 829–843. [Google Scholar] [CrossRef]
- Cocuzza, M.; Athayde, K.S.; Agarwal, A.; Pagani, R.; Sikka, S.C.; Lucon, A.M.; Srougi, M.; Hallak, J. Impact of clinical varicocele and testis size on seminal reactive oxygen species levels in a fertile population: A prospective controlled study. Fertil. Steril. 2008, 90, 1103–1108. [Google Scholar] [CrossRef]
- Ko, E.Y.; Sabanegh, E.S.; Agarwal, A. Male infertility testing: Reactive oxygen species and antioxidant capacity. Fertil. Steril. 2014, 102, 1518–1527. [Google Scholar] [CrossRef] [PubMed]
- Kavoussi, P.K.; Gilkey, M.S.; Machen, G.L.; Kavoussi, S.K.; Dorsey, C. Varicocele Repair Improves Static Oxidation Reduction Potential as a Measure of Seminal Oxidative Stress Levels in Infertile Men: A Prospective Clinical Trial Using the MiOXSYS System. Urology 2022, 165, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Pasqualotto, F.F.; Sharma, R.K.; Nelson, D.R.; Thomas, A.J.; Agarwal, A. Relationship between oxidative stress, semen characteristics, and clinical diagnosis in men undergoing infertility investigation. Fertil. Steril. 2000, 73, 459–464. [Google Scholar] [CrossRef]
- Romeo, C.; Impellizzeri, P.; Arrigo, T.; Antonuccio, P.; Valenzise, M.; Mirabelli, S.; Borruto, F.A.; Scalfari, G.; Arena, F.; De Luca, F. Late hormonal function after testicular torsion. J. Pediatr. Surg 2010, 45, 411–413. [Google Scholar] [CrossRef]
- Thomas, W.E.; Cooper, M.J.; Crane, G.A.; Lee, G.; Williamson, R.C. Testicular exocrine malfunction after torsion. Lancet 1984, 2, 1357–1360. [Google Scholar] [CrossRef]
- Goldwasser, B.; Weissenberg, R.; Lunenfeld, B.; Nativ, O.; Many, M. Semen quality and hormonal status of patients following testicular torsion. Andrologia 1984, 16, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.J.; Dunn, J.K.; Lipshultz, L.I.; Coburn, M. Semen quality and endocrine parameters after acute testicular torsion. J. Urol. 1992, 147, 1545–1550. [Google Scholar] [CrossRef]
- Gielchinsky, I.; Suraqui, E.; Hidas, G.; Zuaiter, M.; Landau, E.H.; Simon, A.; Duvdevani, M.; Gofrit, O.N.; Pode, D.; Rosenberg, S. Pregnancy Rates after Testicular Torsion. J. Urol. 2016, 196, 852–855. [Google Scholar] [CrossRef]
- Jacobsen, F.M.; Rudlang, T.M.; Fode, M.; Østergren, P.B.; Sønksen, J.; Ohl, D.A.; Jensen, C.F.S.; Collaborative, C. The Impact of Testicular Torsion on Testicular Function. World J. Mens Health 2020, 38, 298–307. [Google Scholar] [CrossRef]
- Mäkelä, E.P.; Roine, R.P.; Taskinen, S. Paternity, erectile function, and health-related quality of life in patients operated for pediatric testicular torsion. J. Pediatr. Urol. 2020, 16, 44.e41–44.e44. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Sharma, R.; Roychoudhury, S.; Du Plessis, S.; Sabanegh, E. MiOXSYS: A novel method of measuring oxidation reduction potential in semen and seminal plasma. Fertil. Steril. 2016, 106, 566–573.e510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigman, M.J.J. Male Infertility in Campbell Walsh Wein Handbook of Urology; Wein, J.A., Ed.; Elsevier: Amsterdam, The Netherlands, 2007; p. 57. [Google Scholar]
- Howe, A.S.; Vasudevan, V.; Kongnyuy, M.; Rychik, K.; Thomas, L.A.; Matuskova, M.; Friedman, S.C.; Gitlin, J.S.; Reda, E.F.; Palmer, L.S. Degree of twisting and duration of symptoms are prognostic factors of testis salvage during episodes of testicular torsion. Transl. Androl. Urol. 2017, 6, 1159–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mellick, L.B.; Sinex, J.E.; Gibson, R.W.; Mears, K. A Systematic Review of Testicle Survival Time After a Torsion Event. Pediatr. Emerg. Care 2019, 35, 821–825. [Google Scholar] [CrossRef]
- Yang, C.; Song, B.; Tan, J.; Liu, X.; Wei, G.H. Testicular torsion in children: A 20-year retrospective study in a single institution. ScientificWorldJournal 2011, 11, 362–368. [Google Scholar] [CrossRef] [Green Version]
- Wilbert, D.M.; Schaerfe, C.W.; Stern, W.D.; Strohmaier, W.L.; Bichler, K.H. Evaluation of the acute scrotum by color-coded Doppler ultrasonography. J. Urol. 1993, 149, 1475–1477. [Google Scholar] [CrossRef]
- Shteynshlyuger, A.; Yu, J. Familial testicular torsion: A meta analysis suggests inheritance. J. Pediatr Urol. 2013, 9, 683–690. [Google Scholar] [CrossRef]
- Van Welie, M.; Qu, L.G.; Adam, A.; Lawrentschuk, N.; Laher, A.E. Recurrent testicular torsion post orchidopexy—An occult emergency: A systematic review. ANZ J. Surg. 2022, 92, 2043–2052. [Google Scholar] [CrossRef]
- Sigman, M.; Jarow, J.P. Ipsilateral testicular hypotrophy is associated with decreased sperm counts in infertile men with varicoceles. J. Urol. 1997, 158, 605–607. [Google Scholar] [CrossRef]
- Condorelli, R.; Calogero, A.E.; La Vignera, S. Relationship between Testicular Volume and Conventional or Nonconventional Sperm Parameters. Int. J. Endocrinol. 2013, 2013, 145792. [Google Scholar] [CrossRef]
- Corsini, C.; Boeri, L.; Candela, L.; Pozzi, E.; Belladelli, F.; Capogrosso, P.; Fallara, G.; Schifano, N.; Cignoli, D.; Ventimiglia, E.; et al. Is There a Relevant Clinical Impact in Differentiating Idiopathic versus Unexplained Male Infertility? World J. Mens Health 2022, 40, e63. [Google Scholar] [CrossRef] [PubMed]
- Fedder, J. Nonsperm cells in human semen: With special reference to seminal leukocytes and their possible influence on fertility. Arch Androl 1996, 36, 41–65. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, J.; Cai, Z.; Wang, X.; Lu, W.; Li, H. Effect of unilateral testicular torsion at different ages on male fertility. J. Int. Med. Res. 2020, 48, 300060520918792. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, A.; Leisegang, K.; Majzoub, A.; Henkel, R.; Finelli, R.; Panner Selvam, M.K.; Tadros, N.; Parekh, N.; Ko, E.Y.; Cho, C.L.; et al. Utility of Antioxidants in the Treatment of Male Infertility: Clinical Guidelines Based on a Systematic Review and Analysis of Evidence. World J. Mens Health 2021, 39, 233–290. [Google Scholar] [CrossRef]
- Jensen, N.B.; Justesen, S.D.; Larsen, A.; Ernst, E.; Pedersen, L.H. A systematic overview of the spermatotoxic and genotoxic effects of methotrexate, ganciclovir and mycophenolate mofetil. Acta Obstet. Gynecol. Scand. 2021, 100, 1557–1580. [Google Scholar] [CrossRef]
- Rao, M.; Zhao, X.L.; Yang, J.; Hu, S.F.; Lei, H.; Xia, W.; Zhu, C.H. Effect of transient scrotal hyperthermia on sperm parameters, seminal plasma biochemical markers, and oxidative stress in men. Asian J. Androl. 2015, 17, 668–675. [Google Scholar] [CrossRef]
- Rehman, R.; Zahid, N.; Amjad, S.; Baig, M.; Gazzaz, Z.J. Relationship Between Smoking Habit and Sperm Parameters Among Patients Attending an Infertility Clinic. Front. Physiol. 2019, 10, 1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tvrda, E.; Lovisek, D.; Galova, E.; Schwarzova, M.; Kovacikova, E.; Kunova, S.; Ziarovska, J.; Kacaniova, M. Possible Implications of Bacteriospermia on the Sperm Quality, Oxidative Characteristics, and Seminal Cytokine Network in Normozoospermic Men. Int. J. Mol. Sci. 2022, 23, 8678. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Exploration Group 1 | Detorsion Group 2 | Orchiectomy Group 3 | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Investigated Parameter | n | % | n | % | n | % | n | % | |
| Side of the affected testis | Left | 10 | 40 | 7 | 35 | 0 | 0 | 17 | 35 |
| Right | 15 | 60 | 13 | 65 | 4 | 100 | 32 | 65 | |
| Total | 25 | 100 | 20 | 100 | 4 | 100 | 49 | 100 | |
| Activity at the onset of Symptoms | Resting | 9 | 42.9 | 3 | 25 | 1 | 33.3 | 13 | 36 |
| Sleeping | 8 | 38.1 | 7 | 58.3 | 1 | 33.3 | 16 | 44 | |
| Doing sports | 4 | 19 | 2 | 16.7 | 1 | 33.3 | 7 | 19 | |
| Total | 21 | 100 | 12 | 100 | 3 | 100 | 36 b | 100 | |
| Undescended testis in the hashish | No | 21 | 84 | 19 | 95 | 3 | 75 | 43 | 88 |
| Yes | 4 | 16 | 1 | 5 | 1 | 25 | 6 | 12 | |
| Total | 25 | 100 | 20 | 100 | 4 | 100 | 49 | 100 | |
| Positive family history of TT a | No | 23 | 92 | 18 | 90 | 4 | 100 | 45 | 92 |
| Yes | 2 | 8 | 2 | 10 | 0 | 0 | 4 | 8.2 | |
| Total | 25 | 100 | 20 | 100 | 4 | 100 | 49 | 100 | |
| Smoking | No | 13 | 52 | 16 | 80 | 3 | 75 | 32 | 65 |
| Yes | 12 | 48 | 4 | 20 | 1 | 25 | 17 | 35 | |
| Total | 25 | 100 | 20 | 100 | 4 | 100 | 49 | 100 | |
| Alcohol Consumption | No | 8 | 32 | 9 | 45 | 1 | 25 | 18 | 37 |
| Yes | 17 | 68 | 11 | 55 | 3 | 75 | 31 | 64 | |
| Total | 25 | 100 | 20 | 100 | 4 | 100 | 49 | 100 | |
| Exploration (n = 26) Group 1 | Detorsion (n = 19) Group 2 | Orchiectomy (n = 4) Group 3 | Total (n = 49) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD a | Mean | SD | Mean | SD | Mean | SD | ||
| Medical History | Age at surgery (years) | 21 | 7.42 | 18 | 4.24 | 15.5 | 8.54 | 19 | 6.46 |
| Age at control (years) | 28 | 6.54 | 27 | 5.28 | 32.5 | 6.66 | 28 | 5.98 | |
| Time from the onset of symptoms to surgery (hours) | 8 | 11.93 | 3 | 1.71 | 50 | 37.9 | 5 | 15.34 | |
| Follow-up (months) | 83 | 66.25 | 106.5 | 66.6 | 137.5 | 98.83 | 101 | 69.08 | |
| Height of patients (meter) | 1.8 | 0.08 | 1.8 | 0.07 | 1.79 | 0.08 | 1.8 | 0.08 | |
| Weight of patients (kg) | 75 | 16.5 | 79 | 20.15 | 82 | 18.12 | 77.5 | 17.92 | |
| BMI b (kg/m2) | 24.02 | 4.52 | 23.41 | 6.36 | 25.64 | 8.65 | 23.42 | 5.64 | |
| IIEF-5 c | 25 | 3.95 | 24 | 1.58 | 25 | 3.46 | 24.5 | 3.17 | |
| Size of the affected testicle (mL) | 18 | 4.26 | 20 | 3.33 | n.a. | n.a. | 20 | 3.91 | |
| Size of the unaffected testicle (mL) | 20 | 4.51 | 20 | 4.09 | 16.5 | 3.5 | 20 | 4.29 | |
| Grade of torsion (°) | 0 | 0 | 360 | 207.04 | 540 | 236.7 | 0 | 241.61 | |
| Fitness scale from 1 to 5 (the best is 5) | 4 | 0.94 | 4 | 0.74 | 4.5 | 0.96 | 4 | 0.86 | |
| Laboratory parameters | FSH d (mU/mL) | 4.3 | 3.01 | 2.7 | 2.57 | 10.6 | 2.83 | 3.7 | 3.31 |
| LH e (mU/mL) | 4.7 | 2.07 | 4.2 | 2.13 | 7.6 | 2.12 | 4.8 | 2.17 | |
| Testosterone (ng/mL) | 5.29 | 1.45 | 4.47 | 1.82 | 3.89 | 0.56 | 5.08 | 1.6 | |
| Free testosterone (pg/mL) | 14.85 | 4.57 | 14.95 | 4.07 | 11.21 | 3.01 | 14.68 | 4.4 | |
| Prolactin (µU/mL) | 304 | 125.73 | 331 | 132.17 | 194 | 87.09 | 300 | 129.14 | |
| SHBG f (nmol/L) | 34 | 13.98 | 30.4 | 17.65 | 32.3 | 11.03 | 31.6 | 15.13 | |
| Albumin (g/dL) | 4.6 | 0.24 | 4.7 | 0.19 | 4.45 | 0.17 | 4.6 | 0.22 | |
| TSH g (mU/L) | 1.88 | 2.68 | 2.02 | 0.82 | 2.15 | 0.85 | 1.88 | 2 | |
| Semen analysis h | Sperm concentration (million/mL) | 52 | 45.35 | 50.2 | 70.87 | 34 | 10.88 | 50.7 | 56.05 |
| Total sperm count (million) | 158.88 | 238.47 | 235.44 | 296.71 | 159.35 | 15.48 | 172.5 | 255.45 | |
| Vitality (%) | 68 | 10.12 | 65 | 14.52 | 70.5 | 2.06 | 68 | 11.99 | |
| Progressive motility (a+b) (%) | 53 | 8.01 | 55 | 13.23 | 55 | 18.78 | 54.5 | 11.17 | |
| Overall motility (a+b+c+) (%) | 65 | 7.62 | 62 | 11.57 | 66.5 | 13.67 | 64.5 | 9.88 | |
| Fast progressive motility (a; %) | 19 | 12.24 | 19 | 13.88 | 22 | 18.57 | 19 | 13.29 | |
| Slow progressive motility (b; %) | 35 | 12.65 | 31 | 10.99 | 26.5 | 12.07 | 31.5 | 11.92 | |
| Non-progressive motility (c; %) | 8 | 5.93 | 8 | 6.3 | 11.5 | 5.8 | 8.5 | 5.98 | |
| Immotility (d; %) | 35 | 7.7 | 38 | 11.57 | 33.5 | 13.67 | 35.5 | 9.92 | |
| Semen pH | 7.5 | 0.23 | 7.5 | 0.2 | 7.65 | 0.35 | 7.5 | 0.23 | |
| Morphology (%) | 11 | 6.85 | 12 | 4.83 | 12 | 4.9 | 11 | 5.94 | |
| Round cell count (million/mL) | 1 | 4.02 | 2.4 | 15.01 | 0.7 | 0.43 | 1.8 | 10.04 | |
| Leukocytes (million) | 0 | 0.36 | 0.2 | 0.94 | 0 | 0 | 0.05 | 0.66 | |
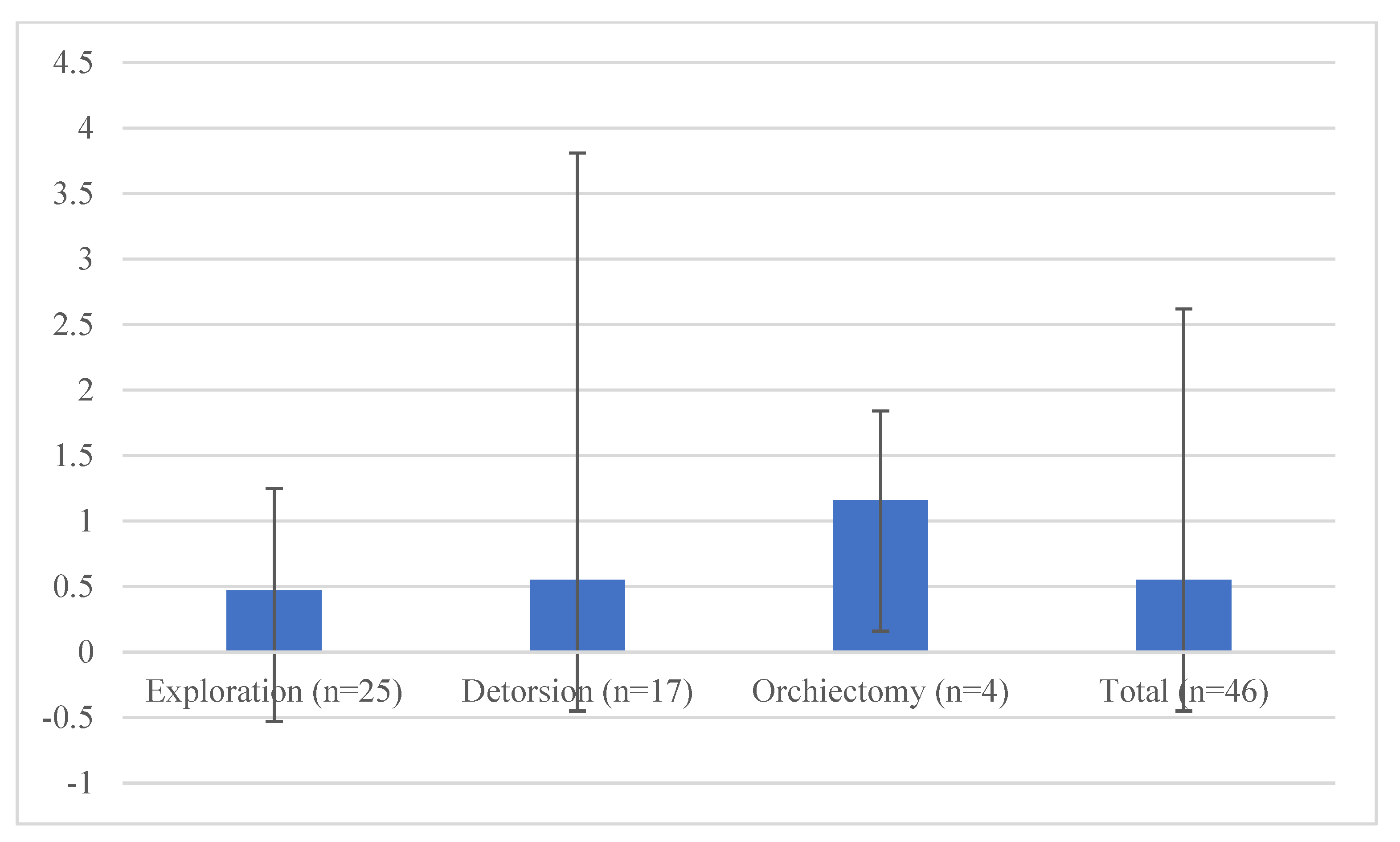
| Oxidative stress i (mV/106 mL) | 0.47 | 0.78 | 0.55 | 3.26 | 1.16 | 0.68 | 0.55 | 2.07 | |
| Exploration Group 1 | Detorsion Group 2 | Orchiectomy Group 3 | Total | |||||
|---|---|---|---|---|---|---|---|---|
| N | % | n | % | n | % | n | % | |
| Normozoospermia | 23 | 92 | 15 | 78.9 | 4 | 100 | 42 | 87.5 |
| Oligozoospermia | 1 | 4 | 4 | 21.1 | 0 | 0 | 5 | 10.4 |
| Asthenozoospermia | 1 | 4 | 0 | 0 | 0 | 0 | 1 | 2.1 |
| Total | 25 | 100 | 19 | 100 | 4 | 100 | 48 | 100 |
| Investigated Parameter | Test | Overall p-Value |
|---|---|---|
| Time from the onset of symptoms to surgery (hours) | KW | <0.001 |
| FSH a (mU/mL) | KW | 0.003 |
| Round cell count (million/mL) | KW | 0.002 |
| Leukocytes (million) | KW | 0.040 |
| Age at surgery (years) | KW | 0.167 |
| Age at control (years) | KW | 0.704 |
| Follow-up (months) | KW | 0.441 |
| Height of the patient (m) | KW | 0.455 |
| Weight of the patient (kg) | KW | 0.535 |
| BMI b (kg/m2) | KW | 0.973 |
| IIEF-5 c | KW | 0.985 |
| Size of the unaffected testicle (mL) | KW | 0.318 |
| Fitness scale from 1 to 5 (5 denotes the best) | KW | 0.691 |
| LH d (mU/mL) | KW | 0.094 |
| Testosterone (ng/mL) | KW | 0.073 |
| Free testosterone (pg/mL) | KW | 0.123 |
| Prolactin (µU/mL) | KW | 0.092 |
| SHBG e (nmol/L) | KW | 0.737 |
| Albumin (g/dL) | KW | 0.084 |
| TSH f (mU/L) | KW | 0.895 |
| Sperm concentration (million/mL) | KW | 0.466 |
| Total sperm count (million) | KW | 0.593 |
| Vitality (%) | KW | 0.239 |
| Progressive motility (a+b) (%) | KW | 0.885 |
| Overall motility (a+b+c+) (%) | KW | 0.465 |
| Fast progressive motility (a; %) | KW | 0.798 |
| Slow progressive motility (b; %) | KW | 0.391 |
| Non-progressive motility (c; %) | KW | 0.559 |
| Immotility (d; %) | KW | 0.455 |
| Semen-pH | KW | 0.385 |
| Morphology (%) | KW | 0.773 |
| Oxidative stress g (mV/106 mL) | KW | 0.764 |
| Spermiogram categories | KW | 0.183 |
| Side of the affected testis | Chi | 0.356 |
| Children fathered after testicular torsion | Chi | 0.453 |
| Smoking (yes/no) | Chi | 0.126 |
| Alcohol consumption (yes/no) | Chi | 0.604 |
| Medication history (yes/no) | Chi | 0.399 |
| Drug use (yes/no) | Chi | 0.464 |
| Symptoms in the operated testis | Chi | 0.884 |
| Sports activities (yes/no) | Chi | 0.026 |
| Family history of testicular torsion | Chi | >0.999 |
| Fitness status (yes or no) | Chi | 0.575 |
| Activity at the onset of symptoms | Chi | 0.807 |
| Investigated Parameter | Overall p-Value | Exploration vs. Detorsion | Exploration vs. Orchiectomy | Detorsion vs.Orchiectomy |
|---|---|---|---|---|
| Time from the onset of symptoms to surgery | <0.001 ** | <0.001 ** | 0.831 | 0.048 * |
| FSH a (mU/mL) | 0.003 ** | 0.156 | 0.08 | 0.005 ** |
| Round cell count (million/mL) | 0.002 ** | 0.013 * | 0.49 | 0.019 * |
| Leukocytes (million) | 0.040 * | 0.296 | 0.399 | 0.091 |
| Parameter | Correlations Coefficient | p | n | Test | p | Eta-Coefficient ŋ2 | |
|---|---|---|---|---|---|---|---|
| Oxidative stress a | Age at control (years) | −0.315 | 0.033 | 46 | |||
| Height of patient (m) | 0.337 | 0.025 | 44 | ||||
| Sperm concentration (million/mL) | −0.573 | <0.001 | 46 | ||||
| Total sperm count (million) | −0.402 | 0.006 | 46 | ||||
| Spermiogram category | 0.337 | 0.022 | 46 | ||||
| Medication history | 0.32 | 0.039 | 42 | ||||
| Erectile function b | Weight of the patient (kg) | 0.364 | 0.015 | 44 | |||
| BMI (kg/m2) | 0.3 | 0.048 | 44 | ||||
| Physical status | 0.439 | 0.002 | 46 | ||||
| Sports activities | 0.301 | 0.042 | 46 | ||||
| Size of the affected testicle | Size of the normal testicle (mL) | 0.755 | <0.001 | 44 | |||
| Sperm concentration (million/mL) | 0.391 | 0.009 | 44 | ||||
| Total sperm count (million) | 0.416 | 0.005 | 44 | ||||
| Round cell count (million/mL) | 0.391 | 0.009 | 44 | ||||
| Children after torsion | 0.566 | 0.035 | 14 | ||||
| Medication history | −0.324 | 0.039 | 41 | ||||
| Activity at the onset of symptoms | - | - | - | KW | 0.047 | 0.267 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Törzsök, P.; Steiner, C.; Pallauf, M.; Abenhardt, M.; Milinovic, L.; Plank, B.; Rückl, A.; Sieberer, M.; Lusuardi, L.; Deininger, S. Long-Term Follow-Up after Testicular Torsion: Prospective Evaluation of Endocrine and Exocrine Testicular Function, Fertility, Oxidative Stress and Erectile Function. J. Clin. Med. 2022, 11, 6507. https://doi.org/10.3390/jcm11216507
Törzsök P, Steiner C, Pallauf M, Abenhardt M, Milinovic L, Plank B, Rückl A, Sieberer M, Lusuardi L, Deininger S. Long-Term Follow-Up after Testicular Torsion: Prospective Evaluation of Endocrine and Exocrine Testicular Function, Fertility, Oxidative Stress and Erectile Function. Journal of Clinical Medicine. 2022; 11(21):6507. https://doi.org/10.3390/jcm11216507
Chicago/Turabian StyleTörzsök, Peter, Christopher Steiner, Maximilian Pallauf, Michael Abenhardt, Ljiljana Milinovic, Bethseba Plank, Alena Rückl, Manuela Sieberer, Lukas Lusuardi, and Susanne Deininger. 2022. "Long-Term Follow-Up after Testicular Torsion: Prospective Evaluation of Endocrine and Exocrine Testicular Function, Fertility, Oxidative Stress and Erectile Function" Journal of Clinical Medicine 11, no. 21: 6507. https://doi.org/10.3390/jcm11216507