1. Introduction
Total thyroidectomy (TT) is one of the most performed operations in the world. In neck surgery, it is among the most important interventions, as it is complex and very common [
1].
Despite innovative approaches in surgery and innovations in surgical instruments, bleeding after TT remains a rare event affecting early postoperative morbidity, occurring in 0.3% to 4.2% of cases [
2]. Post-TT bleeding is not only due to the neck’s anterolateral region’s complex anatomy, which is richly vascularised, but also to the strategies adopted to achieve perfect haemostasis in an operative field where contiguous anatomical structures must be preserved [
3,
4].
Intraoperative bleeding is an unpleasant complication that is usually easily manageable and resolvable, although it engages the surgeon and may lengthen operating time. In contrast, postoperative bleeding can represent a life-threatening condition for the patient; therefore, all known methods and strategies need to be used to minimise postoperative bleeding. Over time, the use of new instruments, the collagen-fibrinogen-thrombin patch (CFTP), cellulose gauze, and other hemostatic agents have made it possible to reduce the incidence of postoperative bleeding and reinterventions; however, it cannot be completely avoided [
5,
6].
The purpose of our study was to clarify whether the routine intraoperative execution of a Valsalva manoeuvre (VM) affected the detection of bleeding that would otherwise remain occult and possibly manifest in the postoperative period.
2. Methods
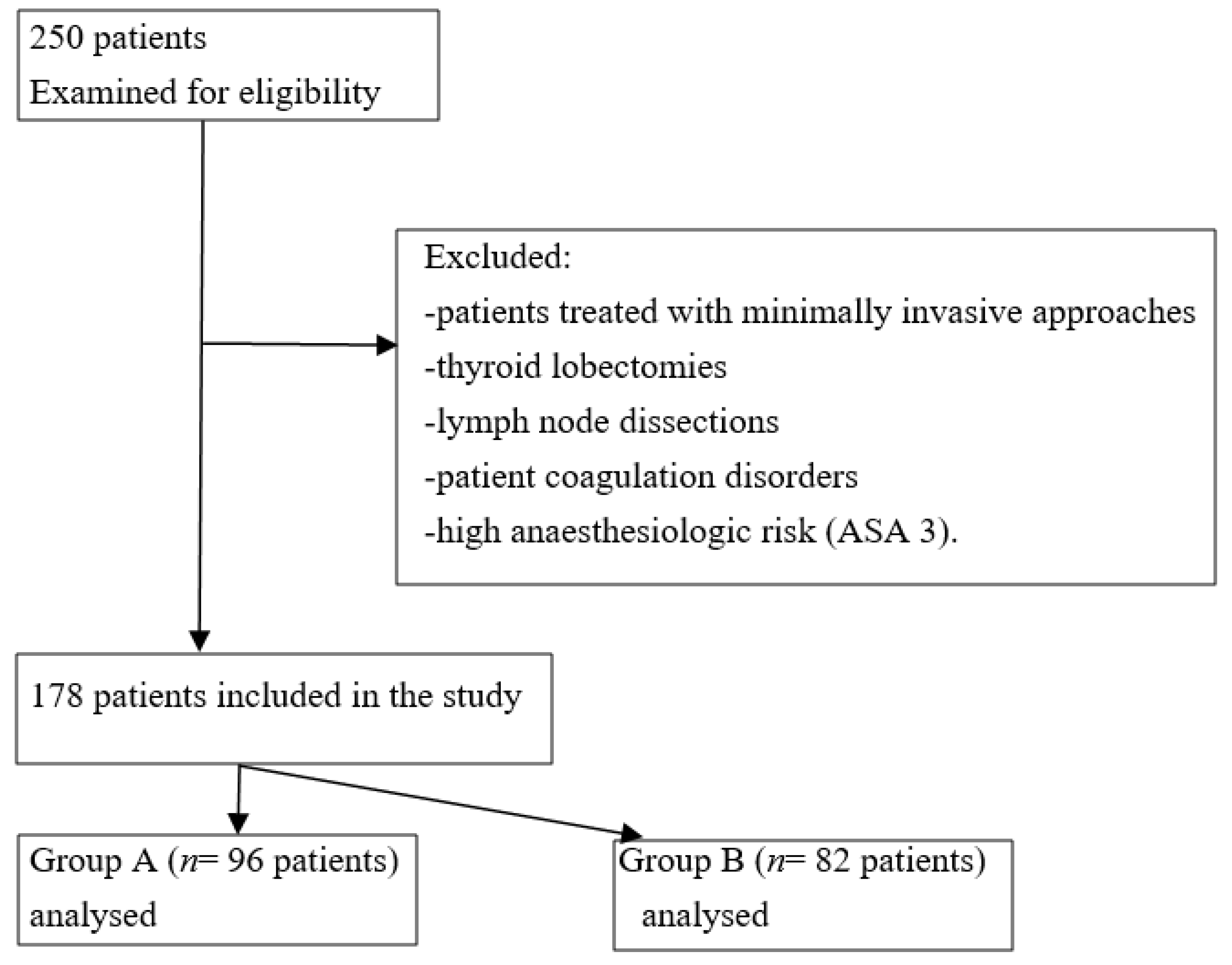
Between January 2019 to February 2022, 250 consecutive patients were listed for thyroid surgery at our surgical department. To evaluate the role of the VM, all patients treated using minimally invasive video-assisted thyroidectomy (MIVAT) or robot-assisted transaxillary thyroid surgery (RATS) were excluded from the study. Other exclusion criteria included thyroid lobectomies, the need for lymph node dissections, patient coagulation disorders, and high anaesthesiologic risk (ASA 3). We chronologically divided our cohort of 178 patients into 2 groups. MV was not performed in Group A (
n = 96 patients); MV was performed at the end of the TT in Group B (
n = 82 patients). This study was conducted according to STROBE guidelines (
Figure 1) [
7].
The VM was performed after thyroid excision and first revision of hemostasis on the operative field. The VM was achieved by applying an incremental PEEP (positive end expiratory pressure) up to 30 cm H2O for 30 s, followed by a new shorter VM performed by setting the mechanical ventilator to manual mode through the APL (adjustable pressure-limiting) valve and using the bag of the manual breathing unit (MBU).
All patients were treated using the same surgical approach by a team with extensive experience in neck surgery; therefore, all procedures were standardised.
The two groups had comparable demographic and clinical-pathological data (
Table 1). Post hoc power was calculated to evaluate sample size (73.9% α 0.05).
Hemostasis was achieved using monopolar or bipolar coagulators, and LigaSure ™ (LSJ Medtronic, Covidien product, Minneapolis, MN, USA) was used to achieve better sealing of vessels in both groups. In dangerous areas, vessels’ ligation and application of small surgical clips was preferred to avoid recurrent laryngeal nerve injury.
At the end of the operation (after a VM execution in Group B), a human fibrinogen and human thrombin (CFTP) patch was always applied, and two suction surgical drains were placed in the thyroid lodges. A CFTP was also applied in Group A.
After the surgery, and anaesthesiologic awakening, patients were kept for 2 h in the recovery room, with personnel assigned to check clinical features and drainage outputs. Sometimes a longer observation time was required. If drains filled rapidly, or symptoms such as dyspnoea, a feeling of neck compression and smoothing of the jugule appeared, then the patient quickly underwent new surgery for haemostasis revision.
Primary outcomes considered included drainage volume, reoperation rates in the first 6 h, and in the first 24 h. The duration of the operation and the occurrence of complications other than bleeding were also evaluated.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed written consent was obtained from all individual participants included in the study.
The study was registered on Clinicaltrial with the following ID: NCT05474261.
Statistical Analysis
Data were analysed using the Statistical Package for the Social Sciences (SPSS) 28.0 (IBM Corp., Armonk, NY, USA). T tests for numerical variables and chi-square tests for categorical variables were performed to accomplish statistical comparison between groups. Phi Coefficients were calculated to determine the association between dichotomous variables. Point-biserial correlations were calculated to correlate between dichotomous and continuous variables. A binary logistic regression model was employed to determine the role of VMs in influencing postoperative bleeding (drainage volume). A p value less than 0.05 was considered statistically significant.
3. Results
The cohort was composed of 178 patients, divided into two groups based on the use of the VM. No statistically significant differences in age, sex, BMI (Body Mass Index), or ASA score (American Society of Anesthesiologists) between the two groups (
p value > 0.05 for all;
Table 1) were found.
Surgical and postoperative data are shown and analysed in
Table 2. No difference in the duration of surgery between the two groups was recorded. Notably, Group B expressed fewer cases of both early (<6 h) and late re-intervention within the 24 h following the operation. These results were not statistically significant. The average period of stay under observation in the recovery room was also slightly shorter in Group B, but was not statistically significant. The results show that Group A was characterised by a significantly greater volume of drainage output in comparison with Group B, and that Group A patients were more frequently kept in place even on the second postoperative day. All patients had double suction drains placed in the right and left thyroid lodges.
Correlation tests (phi coefficients between dichotomous variables and point-biserial correlations between dichotomous and continuous variables) were used to evaluate the real contribution of the VM during TT. The results showed no significant correlation with early or late reoperation or persistence of drainage beyond the first postoperative day. In contrast, correlation with the overall volume of drainage output was statistically significant (
Table 3). Postoperative bleeding (drainage volume) was further investigated using binary logistic regression to analyse the role of the VM (
Table 4).
Finally, we analysed the incidence of major complications during TT (postoperative hypoparathyroidism, recurrent laryngeal nerve palsy, and wound infection). The two groups were homogeneous; no significant differences between the groups were found. These complications were not related to the VM application (
Table 5). All patients included in this study had a 30-day follow-up period after surgery. All cases of hypoparathyroidism and recurrent laryngeal nerve palsy resolved during follow-up; as a result, they were deemed as transient.
4. Discussion
Total thyroidectomy and neck lymph node dissections are among the most frequent surgery performed at the cervical level and have low rates of morbidity and mortality. Bleeding after thyroidectomy is a well-known complication, but thanks to improvements in haemostasis, it has become a rare occurrence. However, despite its rarity, if bleeding is not diagnosed early and correctly managed it can become a potentially life-threatening condition [
8,
9,
10].
In fact, patients with postoperative cervical haematoma are required to undergo a new surgery and lengthier hospital monitoring [
11]. Symptoms arising include respiratory distress, choking, dysphagia, and a feeling of neck constriction. In 72% of cases, postoperative haematoma occurred within 6 h after surgery, and in 89% of cases, within 12 h [
12,
13]. The risk of bleeding was affected not only by patients’ features, but also by the underlying thyroid disease and the haemostatic techniques employed.
In our unit, all patients undergoing TT are routinely subjected to the placement of a drain in the right thyroid lodge and the left thyroid lodge; these drains are subsequently placed on suction. Drains are removed on the first postoperative day or later in cases of abnormal drainage output.
Traditionally, the main purpose of drains is to prevent postoperative complications when evacuating postoperative haematomas or lymphatic fluids and to notify the surgeon as soon as possible. However, drains usage may be omitted as unnecessary in uncomplicated cases because the drained volume is frequently very low, or because haemostasis was adequate during surgery [
14,
15]. In light of improvements in haemostatic techniques and increasing surgical skills, the value of drainage in thyroid surgery may again be questioned; using energy devices and advanced hemostatic agents could reduce drain output, making the use of drainage tubes less useful [
16,
17,
18,
19,
20]. However, we believe that life-threatening complications (such as postoperative bleeding, haematoma, compression of the airways, or suffocation) can be more promptly signaled by the presence of drains, and can guarantee the surgeon a timelier diagnosis and a less rapid onset of symptoms associated with haematoma for patients [
21,
22].
The VM is a common procedure for detecting bleeding points during thyroidectomy procedures. During a VM, increased intrathoracic and intra-abdominal pressures cause internal jugular vein distension and an increase in internal jugular venous pressure. Venous hypertension involving the large veins causes an increase in blood flow to the vessels of the thyroid lodge, forcing any bleeding, and its detection [
23,
24].
Tokaç et al. suggest that intraoperative application of the VM has no positive effects on postoperative hemorrhagic complication [
25]. In 2020, Beyoglu recommended maintaining airway pressure at 50 cm H
2O for 22.5 s to achieve a more reliable intraoperative detection of bleeding points in patients undergoing total thyroidectomies [
26]. Ozdemir affirms that the VM helps to detect bleeding points after Trendelenburg positioning and, given his experience, argues that manual compression is less effective [
27].
In our study, we considered how the VM could help surgeons practicing TT. To reduce postoperative bleeding at the end of the haemostatic phase, we performed double VMs by applying an incremental PEEP up to 30 cm H2O for 30 s, followed by a new VM implemented by setting the mechanical ventilator to manual mode. The second shot was shorter and more energetic, and often identified a new bleeding point, allowing the surgeons to reach a clean and dry surgical field. All bleeding points found after the VMs were treated using monopolar or bipolar coagulators. Ties or stitching were preferred near the RLN. Revision of haemostasis after the VM was performed in 28 cases, or 34.15% of Group B cases. The average time required for re-hemostasis was negligible; it did not affect the overall operating time in our study.
The results reported herein should be considered in light of some limitations. Lymph node dissections increase the risk of postoperative bleeding [
28]. The 178 patients enlisted for this study were suffering from benign and malignant pathologies. Forty-seven patients, accounting for 26% of the study sample, were treated for suspected malignant disease, and were therefore eligible for eventual lymph node dissection. The choice to execute total thyroidectomies without lymph nodal dissection was determined by the information gathered from patients’ clinical histories, US imaging features, the substantial uncertainty of malignant disease deriving from preoperative cytologic investigations. Further studies, including all thyroidectomies with lymph node dissections in the sample, are needed. The sample size was not sufficiently elevated, so the statistical power is less than 80%; it was not a double-blind study, so cultural and/or personal bias may have occurred. However, this procedure allowed us to have fewer re-operations both in the first 6 postoperative hours and in the following 24 h. Notably, many of the early reoperations (<6 h) were performed before the patient left the operating room or recovery room. The numerical increase in the reoperation rate in Group A might be explained by the exiguity of the sample and the patients’ selection criteria, the involvement of different surgeons despite their common experience, and/or rapidly filling surgical drains, any of which may have influenced the choice to re-operate.
These data were not statistically significant in our study, whereas a significant difference was recorded when quantifying the reduction in drainage volume and the lower incidence of drains’ permanence beyond the first postoperative day. The VM did not affect any of the other complications examined.
5. Conclusions
Haematoma manifestation may be life threatening, causing a severe compression of the airways; therefore, assertive bleeding control is crucial. Technological progress and using new haemostatic agents have contributed to a reduction in the incidence of this phenomenon. However, using a simple, economical, and safe manoeuvre such as the VM can improve the postoperative course with a significant reduction in drainage output, although it does not prevent the risk of reoperation.
Author Contributions
M.P. and N.T. wrote and critically revised the first draft; G.P., A.G. and A.F. contributed substantially to data acquisition, analysis, and interpretation; A.A. approved the final version for publication. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent Statement
Informed consent was obtained from all study participants. All participants agreed to participate in the study, which was approved by our institute.
Data Availability Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gil, Z.; Patel, S.G. Surgery for Thyroid Cancer. Surg. Oncol. Clin. North Am. 2008, 17, 93–120. [Google Scholar] [CrossRef] [PubMed]
- Harding, J.; Sebag, F.; Sierra, M.; Palazzo, F.F.; Henry, J.-F. Thyroid surgery: Postoperative hematoma—Prevention and treatment. Langenbeck’s Arch. Surg. 2006, 391, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Cannizzaro, M.A.; Borzì, L.; Bianco, S.L.; Okatyeva, V.; Cavallaro, A.S.; Buffone, A. Comparison between Focus Harmonic scalpel and other hemostatic techniques in open thyroidectomy: A systematic review and meta-analysis. Head Neck 2016, 38, 1571–1578. [Google Scholar] [CrossRef] [PubMed]
- Pacilli, M.; Tartaglia, N.; Gerundo, A.; Pavone, G.; Fersini, A.; Ambrosi, A. Energy Based Vessel Sealing Devices in Thyroid Surgery: A Systematic Review to Clarify the Relationship with Recurrent Laryngeal Nerve Injuries. Medicina 2020, 56, 651. [Google Scholar] [CrossRef] [PubMed]
- Khadra, H.; Bakeer, M.; Hauch, A.; Hu, T.; Kandil, E. Hemostatic agent use in thyroid surgery: A meta-analysis. Gland Surg. 2018, 7, S34–S41. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, N.; Di Lascia, A.; Lizzi, V.; Cianci, P.; Fersini, A.; Ambrosi, A.; Neri, V. Haemostasis in Thyroid Surgery: Collagen-Fibrinogen-Thrombin Patch versus Cellulose Gauze—Our Experience. Surg. Res. Pract. 2016, 2016, 3058754. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Materazzi, G.; Ambrosini, C.E.; Fregoli, L.; De Napoli, L.; Frustaci, G.; Matteucci, V.; Papini, P.; Bakkar, S.; Miccoli, P. Prevention and management of bleeding in thyroid surgery. Gland Surg. 2017, 6, 510–515. [Google Scholar] [CrossRef]
- Graceffa, G.; Orlando, G.; Cocorullo, G.; Mazzola, S.; Vitale, I.; Proclamà, M.; Amato, C.; Saputo, F.; Rollo, E.; Corigliano, A.; et al. Predictors of Central Compartment Involvement in Patients with Positive Lateral Cervical Lymph Nodes According to Clinical and/or Ultrasound Evaluation. J. Clin. Med. 2021, 10, 3407. [Google Scholar] [CrossRef]
- Dolidze, D.D.; Shabunin, A.V.; Mumladze, R.B.; Vardanyan, A.V.; Covantsev, S.D.; Shulutko, A.M.; Semikov, V.I.; Isaev, K.M.; Kazaryan, A.M. A Narrative Review of Preventive Central Lymph Node Dissection in Patients with Papillary Thyroid Cancer—A Necessity or an Excess. Front. Oncol. 2022, 12, 906695. [Google Scholar] [CrossRef]
- Tartaglia, N.; Di Lascia, A.; Vovola, F.; Cianci, P.; Fersini, A.; Pacilli, M.; Pavone, G.; Ambrosi, A. Bilateral central neck dissection in the treatment of early unifocal papillary thyroid carcinomas with poor risk factors A mono-institutional experience. Ann. Ital. Chir. 2020, 91, 161–165. [Google Scholar] [PubMed]
- Lang, B.H.-H.; Yih, P.C.-L.; Lo, C.-Y. A Review of Risk Factors and Timing for Postoperative Hematoma After Thyroidectomy: Is Outpatient Thyroidectomy Really Safe? World J. Surg. 2012, 36, 2497–2502. [Google Scholar] [CrossRef] [PubMed]
- Jeppesen, K.; Moos, C.; Holm, T.; Pedersen, A.K.; Skjøt-Arkil, H. Risk of hematoma after hemithyroidectomy in an outpatient setting: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2022, 279, 3755–3767. [Google Scholar] [CrossRef] [PubMed]
- Abboud, B.; Sleilaty, G.; Rizk, H.; Abadjian, G.; Ghorra, C. Safety of thyroidectomy and cervical neck dissection without drains. Can. J. Surg. 2012, 55, 199–203. [Google Scholar] [CrossRef]
- Ha, E.J.; Lee, J. The effect of fibrin glue on the quantity of drainage after thyroidectomy: A randomized controlled pilot trial. Ann. Surg. Treat. Res. 2022, 102, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, F.; Giuliani, A.; Sorrenti, S.; Tromba, L.; Carbotta, S.; Maturo, A.; Carbotta, G.; De Anna, L.; Merola, R.; Livadoti, G.; et al. Early discharge after total thyroidectomy: A retrospective feasibility study. G Chir. 2016, 37, 250–256. [Google Scholar] [CrossRef]
- Soh, T.C.F.; Ong, Q.J.; Yip, H.M. Complications of Neck Drains in Thyroidectomies: A Systematic Review and Meta-Analysis. Laryngoscope 2020, 131, 690–700. [Google Scholar] [CrossRef]
- Docimo, G.; Tolone, S.; Conzo, G.; Limongelli, P.; Del Genio, G.; Parmeggiani, D.; De Palma, M.; Lupone, G.; Avenia, N.; Lucchini, R.; et al. A Gelatin–Thrombin Matrix Topical Hemostatic Agent (Floseal) in Combination with Harmonic Scalpel Is Effective in Patients Undergoing Total Thyroidectomy. Surg. Innov. 2015, 23, 23–29. [Google Scholar] [CrossRef]
- Canu, G.L.; Medas, F.; Cappellacci, F.; Casti, F.; Bura, R.; Erdas, E.; Calò, P.G. The Use of Harmonic Focus and Thunderbeat Open Fine Jaw in Thyroid Surgery: Experience of a High-Volume Center. J. Clin. Med. 2022, 11, 3062. [Google Scholar] [CrossRef]
- Li, L.; Liu, W.; Tao, H.; Chen, H.; Li, W.; Huang, T.; Zhao, E. Efficacy and safety of negative pressure versus natural drainage after thyroid surgery: A systematic review and meta-analysis. Medicine 2018, 97, e11576. [Google Scholar] [CrossRef]
- Portinari, M.; Carcoforo, P. The application of drains in thyroid surgery. Gland Surg. 2017, 6, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, N.; Iadarola, R.; Di Lascia, A.; Cianci, P.; Fersini, A.; Ambrosi, A. What is the treatment of tracheal lesions associated with traditional thyroidectomy? Case report and systematic review. World J. Emerg. Surg. 2018, 13, 15. [Google Scholar] [CrossRef] [PubMed]
- Moumoulidis, I.; Del Pero, M.M.; Brennan, L.; Jani, P. Haemostasis in head and neck surgical procedures: Valsalva manoeuvre versus Trendelenburg tilt. Ann. R. Coll. Surg. Engl. 2010, 92, 292–294. [Google Scholar] [CrossRef] [PubMed]
- Di Lascia, A.; Tartaglia, N.; Petruzzelli, F.; Pacilli, M.; Maddalena, F.; Fersini, A.; Pavone, G.; Vovola, F.; Ambrosi, A. Right hemicolectomy: Laparoscopic versus robotic approach. Ann. Ital. Chir. 2020, 91, 478–485. [Google Scholar]
- Tokaç, M.; Dumlu, E.G.; Bozkurt, B.; Öcal, H.; Aydın, C.; Yalçın, A.; Çakır, B.; Kılıç, M. Effect of Intraoperative Valsalva Maneuver Application on Bleeding Point Detection and Postoperative Drainage After Thyroidectomy Surgeries. Int. Surg. 2015, 100, 994–998. [Google Scholar] [CrossRef]
- Beyoglu, C.A.; Teksoz, S.; Ozdilek, A.; Akcivan, M.; Erbabacan, E.; Altindas, F.; Koksal, G. A comparison of the efficacy of three different peak airway pressures on intraoperative bleeding point detection in patients undergoing thyroidectomy: A randomized, controlled, clinical trial. BMC Surg. 2020, 20, 69. [Google Scholar] [CrossRef]
- Ozdemir, M.; Makay, O.; Icoz, G.; Akyildiz, M. What adds Valsalva maneuver to hemostasis after Trendelenburg’s positioning during thyroid surgery? Gland Surg. 2017, 6, 433–436. [Google Scholar] [CrossRef]
- de Carvalho, A.Y.; Gomes, C.C.; Chulam, T.C.; Vartanian, J.G.; Carvalho, G.B.; Lira, R.B.; Kohler, H.F.; Kowalski, L.P. Risk Factors and Outcomes of Postoperative Neck Hematomas: An Analysis of 5,900 Thyroidectomies Performed at a Cancer Center. Int. Arch. Otorhinolaryngol. 2020, 25, e421–e427. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 

{kind=link}