
Durlobactam in the Treatment of Multidrug-Resistant Acinetobacter baumannii Infections: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
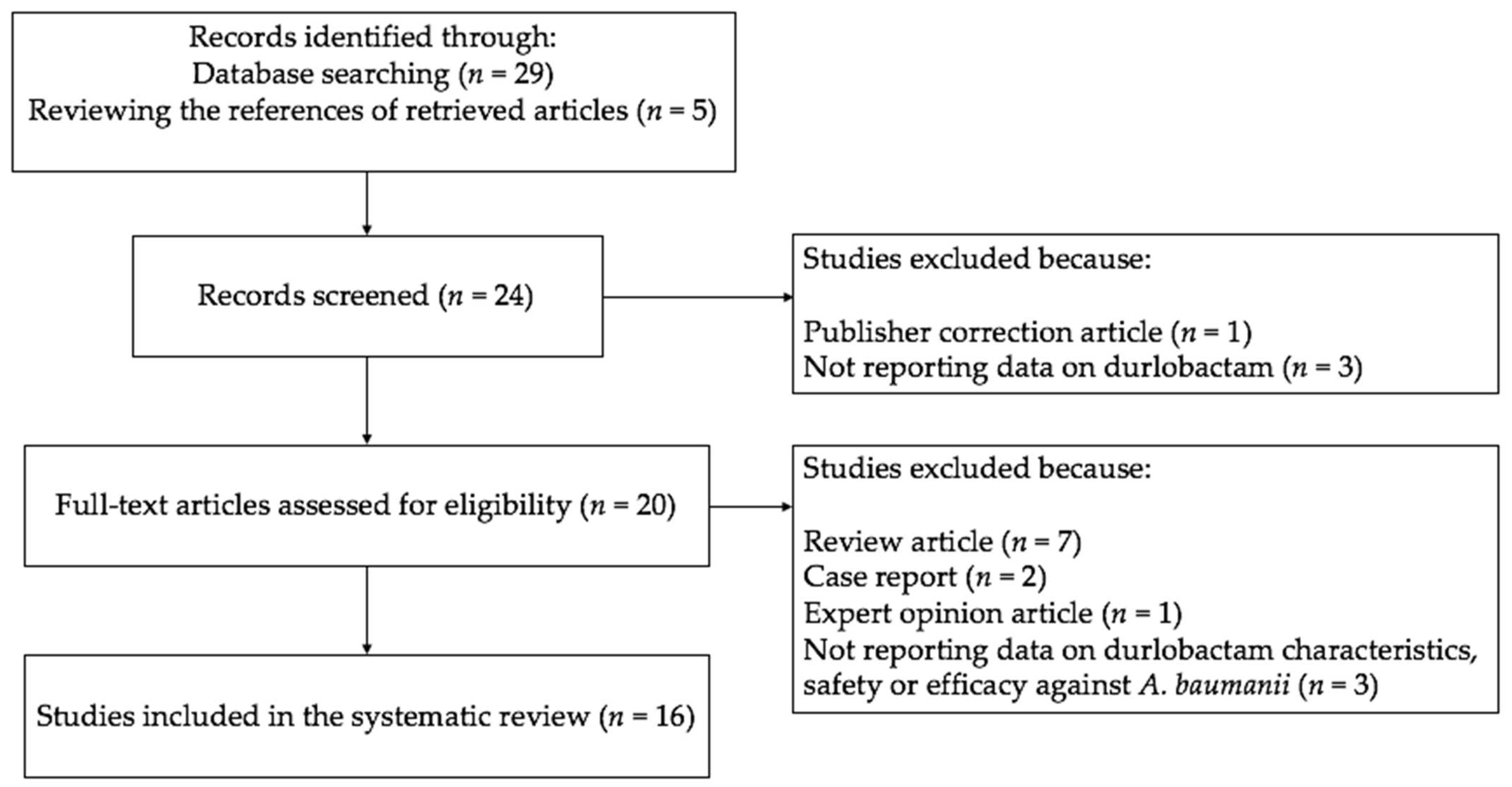
2.1. Search Strategy and Article Identification
2.2. Eligibility Criteria
2.3. Study Selection and Data Extraction
2.4. Data Synthesis
2.5. Assessment of Bias
3. Results
3.1. Studies Description
3.2. Durlobactam Characteristics
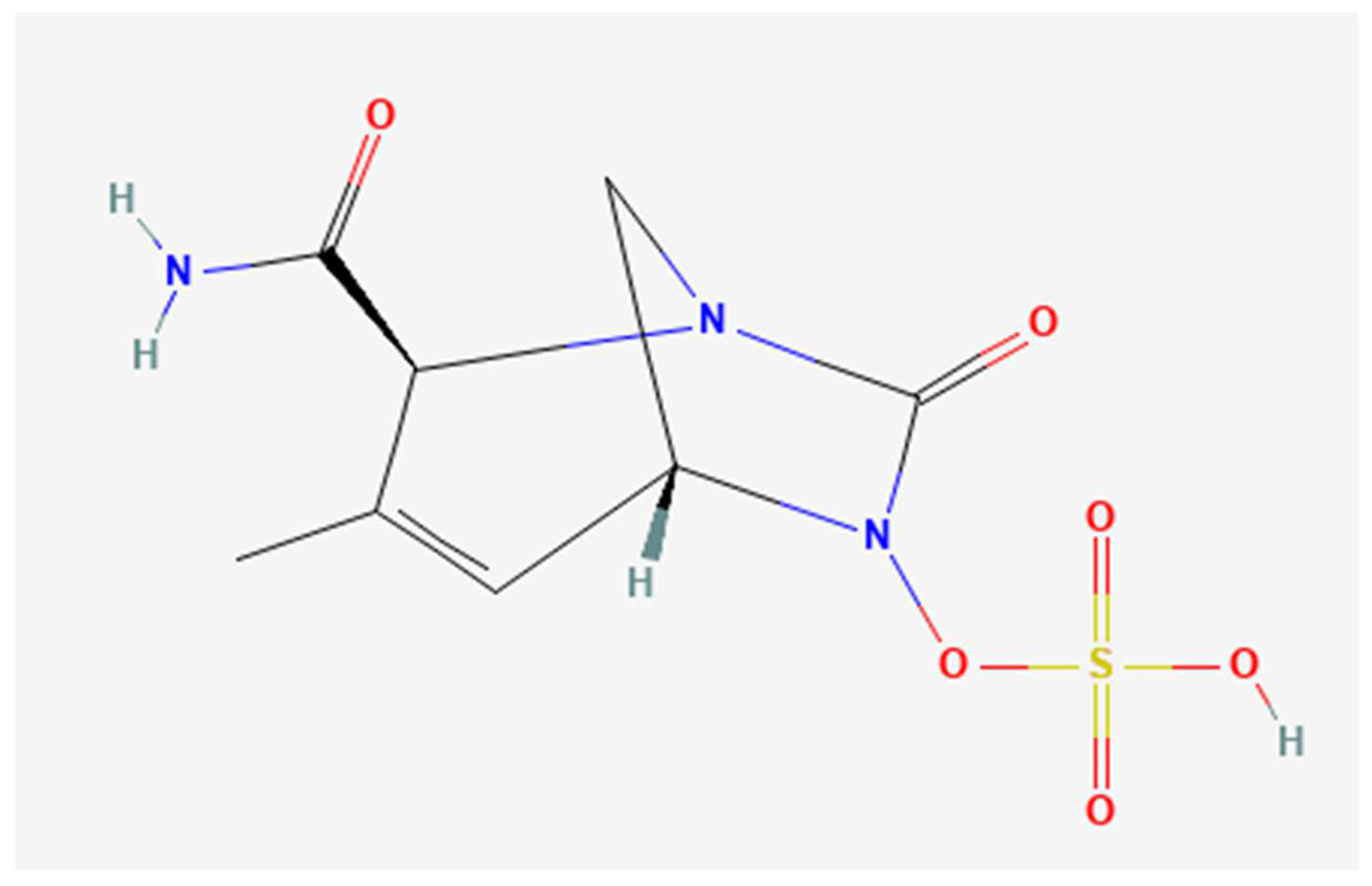
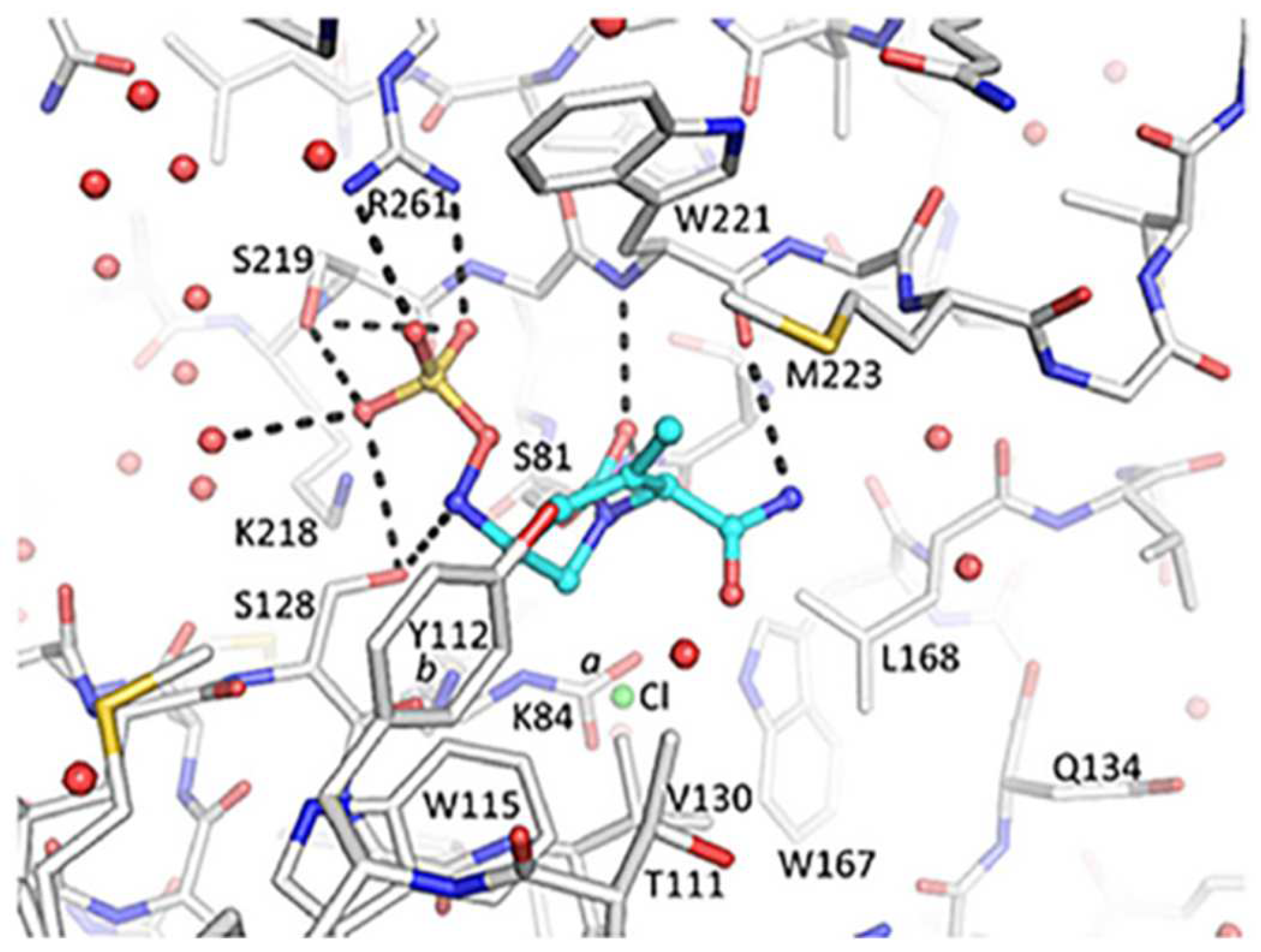
3.2.1. Durlobactam Molecular Structure and Pharmacodynamics
3.2.2. Durlobactam Pharmacokinetics
3.3. In Vitro Studies on the Activity of Durlobactam/Sulbactam against A. baumannii
Durlobactam and Sulbactam Synergistic Bactericidal Activity
3.4. In Vivo Studies on the Efficacy of Durlobactam/Sulbactam to Treat A. baumannii Infections
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sugden, R.; Kelly, R.; Davies, S. Combatting antimicrobial resistance globally. Nat. Microbiol. 2016, 1, 16187. [Google Scholar] [CrossRef]
- Sherry, N.; Howden, B. Emerging Gramnegative resistance to last-line antimicrobial agents fosfomycin, colistin and ceftazidime-avibactam—Epidemiology, laboratory detection and treatment implications. Expert Rev. Anti. Infect. Ther. 2018, 16, 289–306. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Labate, L.; Russo, C.; Vena, A.; Giacobbe, D.R. Therapeutic options for difficult-to-treat Acinetobacter baumannii infections: A 2020 perspective. Expert Opin. Pharmacother. 2021, 22, 167–177. [Google Scholar] [CrossRef]
- Harding, C.M.; Hennon, S.W.; Feldman, M.F. Uncovering the mechanisms of Acinetobacter baumannii virulence. Nat. Rev. Microbiol. 2018, 16, 91–102. [Google Scholar] [CrossRef]
- Giannella, M.; Bussini, L.; Pascale, R.; Bartoletti, M.; Malagrinò, M.; Pancaldi, L.; Toschi, A.; Ferraro, G.; Marconi, L.; Ambretti, S.; et al. Prognostic Utility of the New Definition of Difficult-to-Treat Resistance Among Patients With Gram-Negative Bloodstream Infections. Open Forum Infect. Dis. 2019, 6, ofz505. [Google Scholar] [CrossRef] [PubMed]
- Kadri, S.S.; Adjemian, J.; Lai, Y.L.; Spaulding, A.B.; Ricotta, E.; Prevots, D.R.; Palmore, T.N.; Rhee, C.; Klompas, M.; Dekker, J.P.; et al. Difficult-to-Treat Resistance in Gram-negative Bacteremia at 173 US Hospitals: Retrospective Cohort Analysis of Prevalence, Predictors, and Outcome of Resistance to All First-line Agents. Clin. Infect. Dis. 2018, 67, 1803–1814. [Google Scholar] [CrossRef] [Green Version]
- Vrancianu, C.O.; Gheorghe, I.; Czobor, I.B.; Chifiriuc, M.C. Antibiotic Resistance Profiles, Molecular Mechanisms and Innovative Treatment Strategies of Acinetobacter baumannii. Microorganisms 2020, 8, 935. [Google Scholar] [CrossRef]
- Asif, M.; Alvi, I.A.; Rehman, S.U. Insight into Acinetobacter baumannii: Pathogenesis, global resistance, mechanisms of resistance, treatment options, and alternative modalities. Infect. Drug Resist. 2018, 11, 1249–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viehman, J.A.; Nguyen, M.H.; Doi, Y. Treatment options for carbapenem-resistant and extensively drug-resistant Acinetobacter baumannii infections. Drugs 2014, 74, 1315–1333. [Google Scholar] [CrossRef] [Green Version]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Abdul-Mutakabbir, J.C.; Griffith, N.C.; Shields, R.K.; Tverdek, F.P.; Escobar, Z.K. Contemporary Perspective on the Treatment of Acinetobacter baumannii Infections: Insights from the Society of Infectious Diseases Pharmacists. Infect. Dis. Ther. 2021, 10, 2177–2202. [Google Scholar] [CrossRef] [PubMed]
- Yahav, D.; Giske, C.G.; Grāmatniece, A.; Abodakpi, H.; Tam, V.H.; Leibovici, L. New β-Lactam-β-Lactamase Inhibitor Combinations. Clin. Microbiol. Rev. 2020, 34, e00115-20. [Google Scholar] [CrossRef]
- Durand-Réville, T.F.; Guler, S.; Comita-Prevoir, J.; Chen, B.; Bifulco, N.; Huynh, H.; Lahiri, S.; Shapiro, A.B.; McLeod, S.M.; Carter, N.M.; et al. ETX2514 is a broad-spectrum β-lactamase inhibitor for the treatment of drug-resistant Gram-negative bacteria including Acinetobacter baumannii. Nat. Microbiol. 2017, 2, 17104. [Google Scholar] [CrossRef]
- McLeod, S.M.; Moussa, S.H.; Hackel, M.A.; Miller, A.A. In Vitro Activity of Sulbactam-Durlobactam against Acinetobacter baumannii-calcoaceticus Complex Isolates Collected Globally in 2016 and 2017. Antimicrob. Agents Chemother. 2020, 64, e02534-19. [Google Scholar] [CrossRef]
- Shapiro, A.B.; Gao, N.; Jahić, H.; Carter, N.M.; Chen, A.; Miller, A.A. Reversibility of Covalent, Broad-Spectrum Serine β-Lactamase Inhibition by the Diazabicyclooctenone ETX2514. ACS Infect. Dis. 2017, 3, 833–844. [Google Scholar] [CrossRef] [PubMed]
- Lickliter, J.D.; Lawrence, K.; O’Donnell, J.; Isaacs, R. Safety, Pharmacokinetics, and Drug-Drug Interaction Potential of Intravenous Durlobactam, a β-Lactamase Inhibitor, in Healthy Subjects. Antimicrob. Agents Chemother. 2020, 64, e00071-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodvold, K.A.; Gotfried, M.H.; Isaacs, R.D.; O’Donnell, J.P.; Stone, E. Plasma and Intrapulmonary Concentrations of ETX2514 and Sulbactam following Intravenous Administration of ETX2514SUL to Healthy Adult Subjects. Antimicrob. Agents Chemother. 2018, 62, e01089-18. [Google Scholar] [CrossRef] [Green Version]
- Sagan, O.; Yakubsevitch, R.; Yanev, K.; Fomkin, R.; Stone, E.; Hines, D.; O’Donnell, J.; Miller, A.; Isaacs, R.; Srinivasan, S. Pharmacokinetics and Tolerability of Intravenous Sulbactam-Durlobactam with Imipenem-Cilastatin in Hospitalized Adults with Complicated Urinary Tract Infections, Including Acute Pyelonephritis. Antimicrob. Agents Chemother. 2020, 64, e01506-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, J.; Preston, R.A.; Mamikonyan, G.; Stone, E.; Isaacs, R. Pharmacokinetics, Safety, and Tolerability of Intravenous Durlobactam and Sulbactam in Subjects with Renal Impairment and Healthy Matched Control Subjects. Antimicrob. Agents Chemother. 2019, 63, e00794-19. [Google Scholar] [CrossRef] [Green Version]
- McLeod, S.M.; Shapiro, A.B.; Moussa, S.H.; Johnstone, M.; McLaughlin, R.E.; De Jonge, B.L.M.; Miller, A.A. Frequency and Mechanism of Spontaneous Resistance to Sulbactam Combined with the Novel β-Lactamase Inhibitor ETX2514 in Clinical Isolates of Acinetobacter baumannii. Antimicrob. Agents Chemother. 2018, 62, e01576-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seifert, H.; Müller, C.; Stefanik, D.; Higgins, P.G.; Miller, A.; Kresken, M. In vitro activity of sulbactam/durlobactam against global isolates of carbapenem-resistant Acinetobacter baumannii. J. Antimicrob. Chemother. 2020, 75, 2616–2621. [Google Scholar] [CrossRef]
- Yang, Q.; Xu, Y.; Jia, P.; Zhu, Y.; Zhang, J.; Zhang, G.; Deng, J.; Hackel, M.; Bradford, P.A.; Reinhart, H. In vitro activity of sulbactam/durlobactam against clinical isolates of Acinetobacter baumannii collected in China. J. Antimicrob. Chemother. 2020, 75, 1833–1839. [Google Scholar] [CrossRef]
- Naha, A.; Vijayakumar, S.; Lal, B.; Shankar, B.A.; Chandran, S.; Ramaiah, S.; Veeraraghavan, B.; Anbarasu, A. Genome sequencing and molecular characterisation of XDR Acinetobacter baumannii reveal complexities in resistance: Novel combination of sulbactam-durlobactam holds promise for therapeutic intervention. J. Cell. Biochem. 2021, 122, 1946–1957. [Google Scholar] [CrossRef]
- Nodari, C.S.; Santos, F.F.; Kurihara, M.N.L.; Valiatti, T.B.; Cayô, R.; Gales, A.C. In vitro activity of sulbactam/durlobactam against extensively drug-resistant Acinetobacter baumannii isolates belonging to South American major clones. J. Glob. Antimicrob. Resist. 2021, 25, 363–366. [Google Scholar] [CrossRef]
- Barnes, M.D.; Kumar, V.; Bethel, C.R.; Moussa, S.H.; O’Donnell, J.; Rutter, J.D.; Good, C.E.; Hujer, K.M.; Hujer, A.M.; Marshall, S.H.; et al. Targeting Multidrug-Resistant Acinetobacter spp.: Sulbactam and the Diazabicyclooctenone β-Lactamase Inhibitor ETX2514 as a Novel Therapeutic Agent. mBio 2019, 10, e00159-19. [Google Scholar] [CrossRef] [Green Version]
- Iyer, R.; Moussa, S.H.; Durand-Réville, T.F.; Tommasi, R.; Miller, A. Acinetobacter baumannii OmpA Is a Selective Antibiotic Permeant Porin. ACS Infect. Dis. 2018, 4, 373–381. [Google Scholar] [CrossRef]
- O’Donnell, J.; Maloney, K.; Steidler, M.; Morrison, R.; Isaacs, R. A randomized, double-blind, placebo- and positive-controlled crossover study of the effects of durlobactam on cardiac repolarization in healthy subjects. Clin. Transl. Sci. 2021, 14, 1423–1430. [Google Scholar] [CrossRef]
- ATTACK Trial. Available online: https://investors.entasistx.com/news-releases/news-release-details/entasis-therapeutics-announces-positive-topline-results (accessed on 1 May 2022).
- Tsuji, B.T.; Pogue, J.M.; Zavascki, A.P.; Paul, M.; Daikos, G.L.; Forrest, A.; Giacobbe, D.R.; Viscoli, C.; Giamarellou, H.; Karaiskos, I.; et al. International Consensus Guidelines for the Optimal Use of the Polymyxins: Endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy 2019, 39, 10–39. [Google Scholar]
- Panidis, D.; Markantonis, S.L.; Boutzouka, E.; Karatzas, S.; Baltopoulos, G. Penetration of gentamicin into the alveolar lining fluid of critically ill patients with ventilator-associated pneumonia. Chest 2005, 128, 545–552. [Google Scholar] [CrossRef] [Green Version]
- Tooke, C.L.; Hinchliffe, P.; Bragginton, E.C.; Colenso, C.K.; Hirvonen, V.H.A.; Takebayashi, Y.; Spencer, J. β-Lactamases and β-Lactamase Inhibitors in the 21st Century. J. Mol. Biol. 2019, 431, 3472–3500. [Google Scholar] [CrossRef]
- Portsmouth, S.; Van Veenhuyzen, D.; Echols, R.; Machida, M.; Ferreira, J.C.A.; Ariyasu, M.; Tenke, P.; Nagata, T.D. Cefiderocol versus imipenem-cilastatin for the treatment of complicated urinary tract infections caused by Gram-negative uropathogens: A phase 2, randomised, double-blind, non-inferiority trial. Lancet Infect. Dis. 2018, 18, 1319–1328. [Google Scholar] [CrossRef]
- Solomkin, J.; Evans, D.; Slepavicius, A.; Lee, P.; Marsh, A.; Tsai, L.; Sutcliffe, J.A.; Horn, P. Assessing the Efficacy and Safety of Eravacycline vs Ertapenem in Complicated Intra-abdominal Infections in the Investigating Gram-Negative Infections Treated With Eravacycline (IGNITE 1) Trial: A Randomized Clinical Trial. JAMA Surg. 2017, 152, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Echols, R.; Matsunaga, Y.; Ariyasu, M.; Doi, Y.; Ferrer, R.; Lodise, T.P.; Naas, T.; Niki, Y.; Paterson, D.L.; et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-negative bacteria (CREDIBLE-CR): A randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet Infect. Dis. 2021, 21, 226–240. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author & Country | Year | Study Aim | Study Design & Setting | Methods | Study Results | ||
|---|---|---|---|---|---|---|---|
| Durand-Réville TF et al. [13] US | 2017 | To modify the diazabicyclooctanone scaffold shared by traditional beta-lactamase inhibitors to extend its spectrum of activity to include a broad range of class D, A and C beta-lactamases | In vitro study Laboratory | Reverse phase chromatographies | Durlobactam was discovered. A novel broad-spectrum serine beta-lactamase inhibitor to be combined with a beta-lactam to treat patients infected by Gram-negative bacteria | ||
| Iyer R et al. [26] US | 2018 | To study the permeation characteristics of the A. baumannii outer membrane porin “OmpA” of substrates including durlobactam | In vitro study Laboratory | A specific whole-cell approach called titrable outer membrane permeability assay system was used to characterize the structure porin-permeation relationships. Antibacterial assays used a standard MIC format in Mueller-Hinton cation-adjusted broth. Contribution of OmpA to bacterial fitness was evaluated using a murine thigh model of infection | Durlobactam and sulbactam are substrates of OmpA, with a potential for structure-porin- permeation relationships | ||
| Shapiro AB et al. [15] US | 2017 | To assess the reversibility of durlobactam acylation of a set of beta-lactamases | In vitro study Laboratory | “Jump Dilution” to measure beta-lactamases off-rate constants; Mass spectrometry to assess durlobactam degradation | Durlobactam recyclized and dissociated intact from beta-lactamases AmpC, CTX-M-15, P99, SHV-5 and TEM-1 | ||
| Author & Country | Year | Study aim | Setting | Antimicrobial susceptibility testing | Bacterial isolates | Infection source | Study result and minimum inhibitory concentration |
| McLeod SM et al. [14] US | 2020 | To report the in vitro activity of durlobactam/ sulbactam and comparator antibiotics against clinical isolates of A. baumanni- calcoaceticus complex | Isolates collected in 2016 and 2017 from 209 medical centers in 31 different countries | In-house broth microdilution panels | 1722 Acinetobacter baumannii- calcoaceticus complex 1420 A. baumannii isolates | bloodstream (13.9%), intra- abdominal (3.8%), respiratory tract (61.2%), urinary tract (18.3%), skin and soft tissue (0.8%), other (2.0%) | Durlobactam/sulbactam had a MIC50/MIC90 of 1 and 4 mg/L, respectively, compared to a MIC50/MIC90 of 16/64 mg/L for sulbactam alone |
| McLeod SM et al. [20] US | 2018 | To determine spontaneous resistance to sulbactam in the presence of 4 mg/L durlobactam | Pharmaceutical industry laboratory | Susceptibility testing was performed in cation-adjusted Mueller–Hinton broth | 4 A. baumannii clinical isolates | - | Durlobactam/sulbactam had MICs between 0.5 and 1 mg/L. The frequency of resistance to durlobactam/sulbactam (4xMIC) was lower than 9.0 × 1010 |
| Seifert H et al. [21] US, Germany | 2020 | To evaluate the activity of durlobactam/sulbactam against global isolates of carbapenem- resistant A. baumannii | Isolates collected between 2012 and 2016 from 94 hospitals in 37 different countries | Broth microdilution | 246 carbapenem-resistant A. baumannii isolates | The isolates were collected from various body sites | Durlobactam/sulbactam MIC50 and MIC90 values were 0.25 and 0.5 mg/L, respectively |
| Yang Q et al. [22] China | 2020 | To determine the in vitro activity of durlobactam/sulbactam against A. baumannii isolates | A. baumannii clinical isolates were collected from 22 sites across China between 2016 and 2018 | Frozen microbroth dilution panels | 982 A. baumannii clinical isolates. (831 (84.6%) were imipenem resistant) | Lower respiratory tract (715 isolates, 72.8%), intra- abdominal (170 isolates, 17.3%), urinary tract (59 isolates, 6.0%), skin and soft tissue (35 isolates, 3.6%) and blood (3 isolates, 0.3%) | Sulbactam/durlobactam was equally active against A. baumannii isolates from all infection types: the MIC90 was 2 mg/L for isolates from lower respiratory tract, intraabdominal and skin infections and 1 mg/L for urinary tract isolates. The MIC90 of sulbactam/durlobactam was 0.5 and 2 mg/L for carbapenem-susceptible and -resistant A. baumannii isolates, respectively |
| Nodari CS et al. [24] Brazil | 2021 | To evaluate the antimicrobial activity of durlobactam/sulbactam against a collection of MDR A. baumannii isolates | Isolates collected between 2000 and 2019 in Brazil | Broth microdilution method using durlobactam at a fixed concentration of 4 mg/L | 112 MDR A. baumannii clinical isolates | - | Durlobactam/sulbactam MIC90 values of 4 mg/L |
| Barnes MD et al. [25] US | 2019 | To test the susceptibility of A. baumannii isolates to durlobactam/sulbactam and characterize the ability of durlobactam to inhibit class C and class D beta lactamases Acinetobacter spp. | Isolates collected in at four medical centers in US | Strains were phenotypically characterized using Mueller–Hinton agar dilution | 98 A. baumannii clinical isolates. (43 were carbapenem resistant) | - | The MIC90 of the sole sulbactam was 32 mg/L, in comparison to a durlobactam/sulbactam MIC90 of 2 mg/L |
| Naha et al. [23] India | 2021 | To evaluate the efficacy of the durlobactam/sulbactam against clinical isolates of A. baumannii | Isolates collected between 2018 and 2019 in Indian hospital | Kirby–Bauer disc-diffusion method and broth micro-dilution. The efficacy of durlobactam was assessed through in silico intermolecular interaction analysis | 28 A. baumannii clinical isolates | The 28 clinical strains were isolated from blood (n: 21) and sputum (n: 7) | 93% of isolates expressed carbapenemases. Presence of carbapenemase genes resulted in sulbactam resistance (MIC: 16–256 mg/L) in all isolates. The intermolecular interactions of durlobactam and sulbactam with their respective targets displayed strong binding affinities against the strains of MDR A. baumannii |
| Author, Year &Country | Study Population | Study Design | Study Aim | Setting | Methods | Study Results |
|---|---|---|---|---|---|---|
| Lickliter JD et al. [16] 2020 US, Australia | 124 | Randomized, double-blind, placebo- controlled phase I clinical trial | To evaluate the safety and pharmacokinetics of durlobactam, durlobactam/sulbactam and imipenem- cilastatin in healthy subjects | A single clinical site in Australia, between 2016 and 2017 | 4-part study. Part A was a single- ascending-dose escalation phase. Part B was a multiple-ascending-dose escalation phase. In parts C and D, the drug–drug interaction potential and the safety of durlobactam/sulbactam was investigated after single and multiple doses | On a total of 124 subjects, durlobactam was generally safe and well tolerated when it was administered either alone or in combination with sulbactam or imipenem–cilastatin. Renal excretion was the predominant clearance mechanism |
| Rodvold KA et al. [17] 2018 US | 30 | Phase I, multiple-dose open-label pharmacokinetic study in healthy adults | To determine and compare plasma, epithelial lining fluid and alveolar macrophage concentrations of durlobactam and sulbactam following intravenous administration | A single private facility in US, during 2017 | Liquid chromatography-tandem mass spectrometry following repeated dosing of 1 g of durlobactam and 1 g of sulbactam every 6 h, for a total of 3 doses. A bronchoalveolar lavage was performed once in each subject | In 30 healthy adults subjects, durlobactam/sulbactam was safe and tolerated. Following the third infusion, durlobactam showed values of AUC 0–6 of 109.05 ± 23.44 mg/h/L, the half-life of 1.40 ± 0.18 h and a volume of distribution at steady state of 16.7 ± 3.0 L. Durlobactam AUC 0–6 based on mean epithelial lining fluid concentrations resulted 40.1 mg/h/L |
| O’Donnel J et al. [27] 2021 US | 32 | Placebo- controlled, single-infusion, phase I clinical trial | To evaluate the effect of a single supratherapeutic dose of durlobactam on the heart rate corrected QT interval in healthy volunteers | Private clinical pharmacology center | 32 healthy volunteers were randomized to 1 of 6 sequences that included a single infusion of durlobactam 4 g, a single infusion of placebo, and a single infusion of placebo plus a single oral dose of moxifloxacin 400 mg given open-label at the end of the infusions. In each treatment period, Holter electrocardiogram measurements were obtained | No significant change was observed with durlobactam in comparison to placebo. A concentration-QT analysis demonstrated no significant effect of durlobactam on electrocardiogram parameters, including QT interval prolongation |
| O’Donnell J et al. [19] 2019 US | 34 | Phase I open-label, non-randomized study | To evaluate the effects of various degrees of renal impairment, including subjects with end-stage renal disease on hemodialysis, on the pharmacokinetics and tolerability of durlobactam and sulbactam | Three clinical sites in the United States between 2017 and 2018 | Study included 8 patients with normal renal function, 26 patients with renal impairment. For healthy subjects and those with mild or moderate renal impairment, single 1 g dose each of durlobactam and sulbactam via 3 h infusion was administered, and for severe renal impairment, 500 mg doses were administered. For subjects on hemodialysis, 500 mg doses each of durlobactam and sulbactam were administered post-hemodialysis and pre-hemodialysis, with a 1-week washout between doses | Renal impairment had no effect of the safety profile of durlobactam and sulbactam. Decreasing renal function increased peak plasma concentration and AUC to durlobactam and sulbactam in a generally linear manner. Durlobactam exposure doubled in patients with renal impairment with creatinine clearance lower than 30 mL/min/1.73 m2. Hemodialysis was effective at removing both durlobactam and sulbactam from plasma |
| Sagan O et al. [18] 2020 Ukraine, Belarus, Bulgaria, Russia, US | 80 | Phase II double-blind, randomized, placebo- controlled trial | To evaluate the tolerability and pharmacokinetic of durlobactam/sulbactam in patients with complicated urinary tract infections | 20 clinical sites in Belarus, Bulgaria, Russia, and Ukraine between January 2018 and May 2018 | All the included patients received background therapy with imipenem, in addition to either durlobactam/sulbactam or placebo | The mean steady-state clearance and VD of durlobactam were 10.3 L/h and 31.6 liters, respectively. The microbiological intent-to-treat population were similar in the two groups, 36 (76.6%) and 17 (81.0%) patients in the durlobactam/sulbactam and in the placebo group, respectively |
| ATTACK trial [28] 2021 US | 207 | Open label, randomized phase III clinical trial | To evaluate the efficacy and safety of durlobactam/sulbactam in the treatment of patients with infections caused by A. Baumannii- calcoaceticus Complex | 17 countries in the world, 95 clinical sites between 2019 and 2021 | 2-part study, with Part A being the randomized, controlled portion of the study in patients with A. baumannii hospital- acquired bacterial pneumonia or bacteremia. Part B is the single-group portion of the study and includes A. baumannii infections that are resistant to colistin. Part A contemplated two treatment arms: durlobactam/sulbactam (1 g/1 g qid) plus imipenem/cilastin (1 g/1 g qid) Versus colistin (2.5 mg/kg bid) plus imipenem/cilastin (1 g/1 g qid) | This clinical trial is ongoing. Recruitment phase ended with 207 participants. Durlobactam/sulbactam met the primary efficacy endpoint of 28-day all-cause mortality compared to colistin in the carbapenem- resistant Acinetobacter microbiologically modified intent-to-treat population (125 patients). Durlobactam/sulbactam mortality was 19.0% (12/63) compared to 32.3% (20/62) in the colistin arm (treatment difference of −13.2%; 95% CI: −30.0, 3.5). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Granata, G.; Taglietti, F.; Schiavone, F.; Petrosillo, N. Durlobactam in the Treatment of Multidrug-Resistant Acinetobacter baumannii Infections: A Systematic Review. J. Clin. Med. 2022, 11, 3258. https://doi.org/10.3390/jcm11123258
Granata G, Taglietti F, Schiavone F, Petrosillo N. Durlobactam in the Treatment of Multidrug-Resistant Acinetobacter baumannii Infections: A Systematic Review. Journal of Clinical Medicine. 2022; 11(12):3258. https://doi.org/10.3390/jcm11123258
Chicago/Turabian StyleGranata, Guido, Fabrizio Taglietti, Francesco Schiavone, and Nicola Petrosillo. 2022. "Durlobactam in the Treatment of Multidrug-Resistant Acinetobacter baumannii Infections: A Systematic Review" Journal of Clinical Medicine 11, no. 12: 3258. https://doi.org/10.3390/jcm11123258