
Nitrates vs. Other Types of Vasodilators and Clinical Outcomes in Patients with Vasospastic Angina: A Propensity Score-Matched Analysis

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
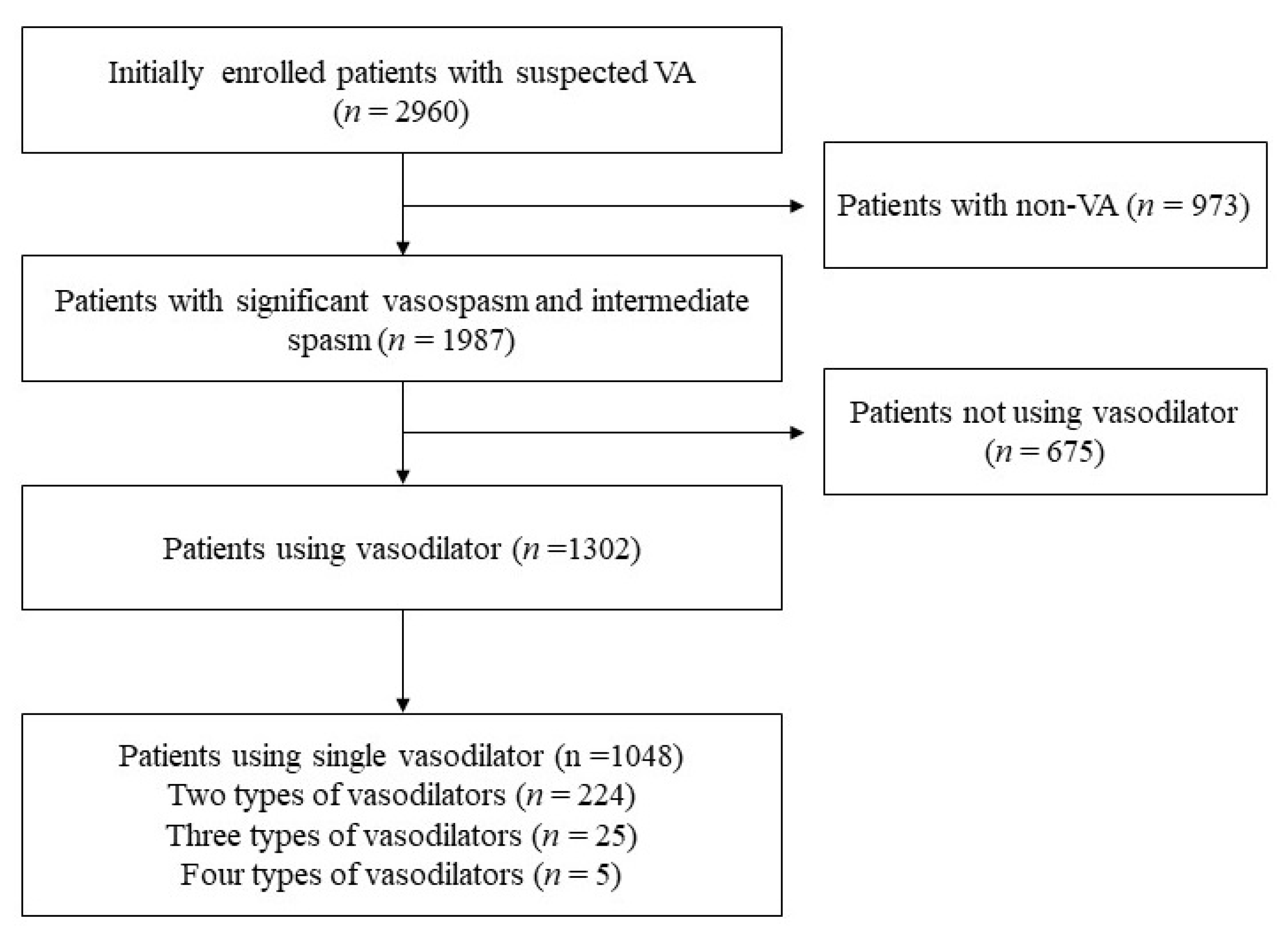
2.1. Study Population
2.2. Data Collection
2.3. Invasive CAG and EG Provocation Test
2.4. Study Outcomes
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
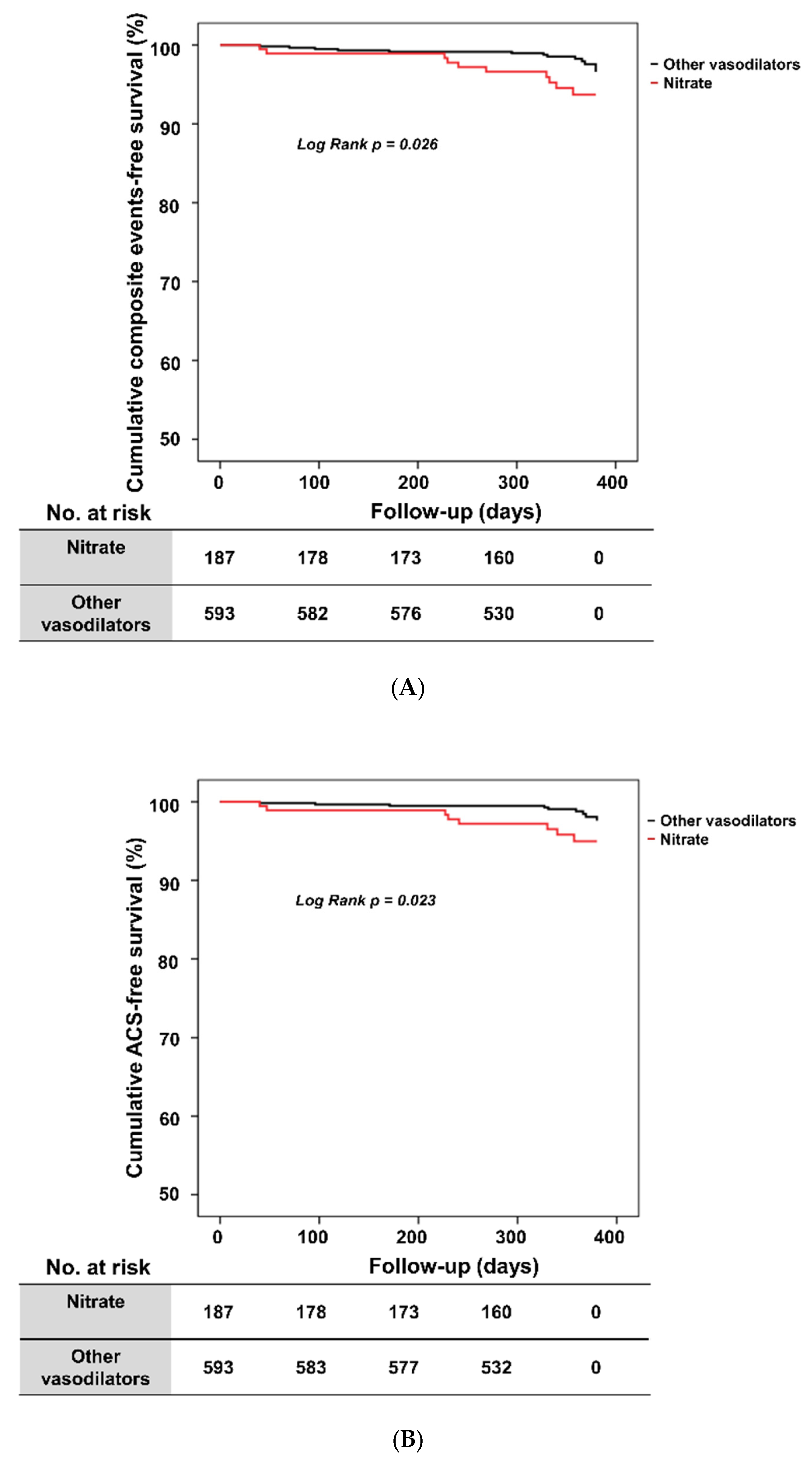
3.2. Clinical Outcomes according to Vasodilator Type
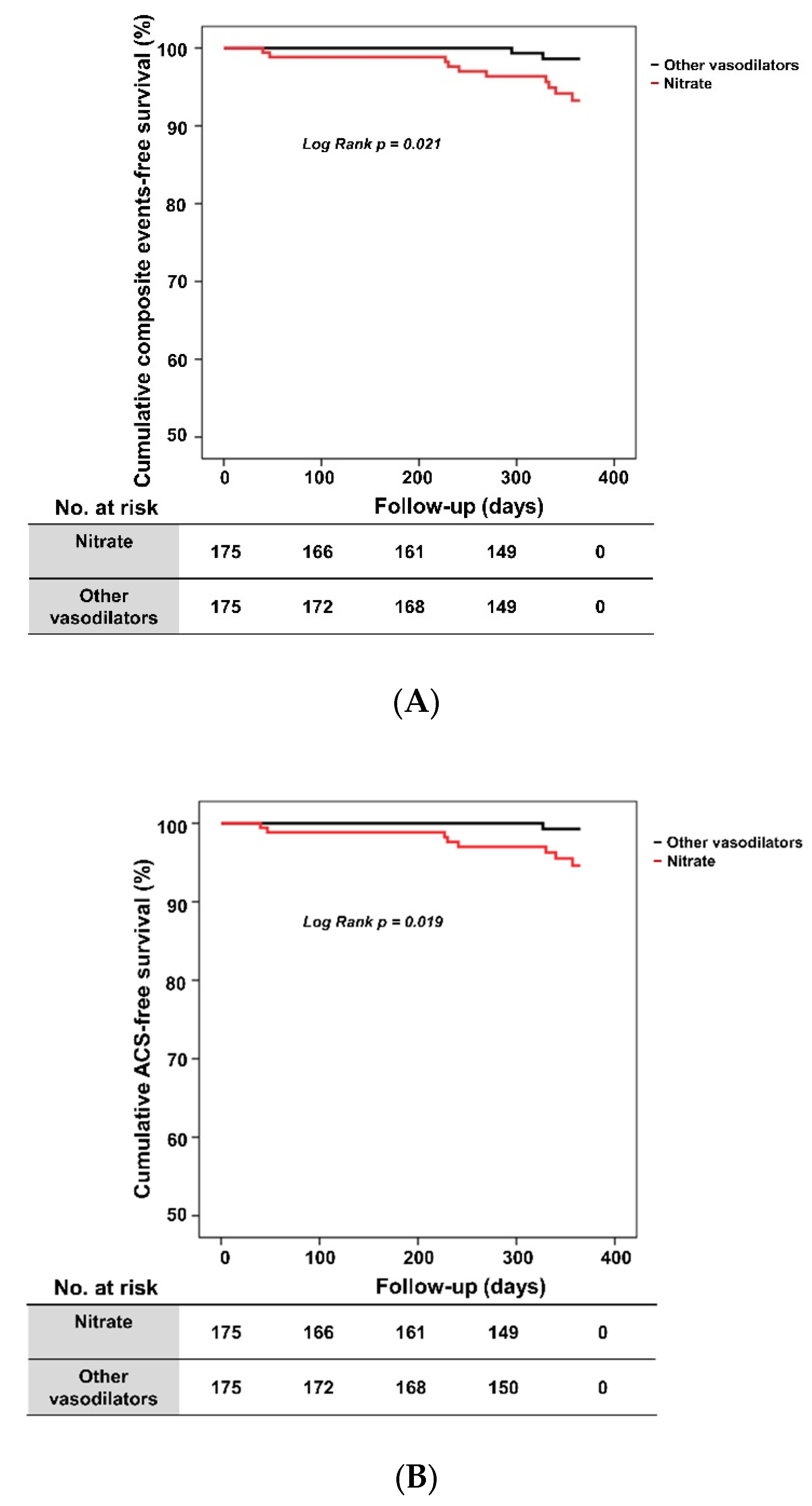
3.3. Clinical Outcomes in Propensity Score-Matched Population
3.4. Effect of Nitrate Type on One-Year ACS Rate in VA Patients
3.5. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- JCS Joint Working Group. Guidelines for diagnosis and treatment of patients with vasospastic angina (Coronary Spastic Angina) (JCS 2013). Circ. J. 2014, 78, 2779–2801. [Google Scholar] [CrossRef] [Green Version]
- Yamagishi, M.; Tamaki, N.; Akasaka, T.; Ikeda, T.; Ueshima, K.; Uemura, S.; Otsuji, Y.; Kihara, Y.; Kimura, K.; Kimura, T.; et al. JCS 2018 Guideline on Diagnosis of Chronic Coronary Heart Diseases. Circ. J. 2021, 85, 402–572. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.I.; Baek, S.H.; Her, S.H.; Han, S.H.; Ahn, Y.; Park, K.H.; Kim, D.S.; Yang, T.H.; Choi, D.J.; Suh, J.W.; et al. The 24-Month Prognosis of Patients With Positive or Intermediate Results in the Intracoronary Ergonovine Provocation Test. JACC Cardiovasc. Interv. 2015, 8, 914–923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsue, Y.; Suzuki, M.; Nishizaki, M.; Hojo, R.; Hashimoto, Y.; Sakurada, H. Clinical implications of an implantable cardioverter-defibrillator in patients with vasospastic angina and lethal ventricular arrhythmia. J. Am. Coll. Cardiol. 2012, 60, 908–913. [Google Scholar] [CrossRef] [Green Version]
- Ong, P.; Athanasiadis, A.; Borgulya, G.; Voehringer, M.; Sechtem, U. 3-year follow-up of patients with coronary artery spasm as cause of acute coronary syndrome: The CASPAR (coronary artery spasm in patients with acute coronary syndrome) study follow-up. J. Am. Coll. Cardiol. 2011, 57, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Parker, J.D.; Parker, J.O. Nitrate therapy for stable angina pectoris. N. Engl. J. Med. 1998, 338, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, T.; Ogasawara, K.; Nakamura, F.; Hirosaka, A.; Sakuma, T.; Nagashima, K.; Kato, K. Effect of nicorandil on coronary spasm. Am. J. Cardiol. 1989, 63, 75J–79J. [Google Scholar] [CrossRef]
- Krumenacker, M.; Roland, E. Clinical profile of nicorandil: An overview of its hemodynamic properties and therapeutic efficacy. J. Cardiovasc. Pharmacol. 1992, 20 (Suppl. S3), S93–S102. [Google Scholar]
- Majid, P.A.; DeFeyter, P.J.; Van der Wall, E.E.; Wardeh, R.; Roos, J.P. Molsidomine in the treatment of patients with angina pectoris. N. Engl. J. Med. 1980, 302, 1–6. [Google Scholar] [CrossRef]
- Gori, T.; Parker, J.D. Nitrate-induced toxicity and preconditioning: A rationale for reconsidering the use of these drugs. J. Am. Coll. Cardiol. 2008, 52, 251–254. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, J.; Nihei, T.; Takagi, Y.; Miyata, S.; Odaka, Y.; Tsunoda, R.; Seki, A.; Sumiyoshi, T.; Matsui, M.; Goto, T.; et al. Prognostic impact of chronic nitrate therapy in patients with vasospastic angina: Multicentre registry study of the Japanese coronary spasm association. Eur. Heart J. 2015, 36, 228–237. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.W.; Her, S.H.; Ahn, Y.; Shin, D.I.; Han, S.H.; Kim, D.S.; Choi, D.J.; Kwon, H.M.; Gwon, H.C.; Jo, S.H.; et al. Clinical outcome according to spasm type of single coronary artery provoked by intracoronary ergonovine tests in patients without significant organic stenosis. Int. J. Cardiol. 2018, 252, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.H.; Jo, S.H.; Kwon, S.; Park, B.W.; Bang, D.W.; Hyon, M.S.; Baek, S.H.; Han, S.H.; Her, S.H.; Shin, D.I.; et al. Impact of Overweight/Obesity on Clinical Outcomes of Patient with Vasospastic Angina: From the Vasospastic Angina in Korea Registry. Sci. Rep. 2020, 10, 4954. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.S.; Jo, S.H.; Han, S.H.; Lee, K.Y.; Her, S.H.; Lee, M.H.; Seo, W.W.; Kim, S.E.; Yang, T.H.; Park, K.H.; et al. Clopidogrel plus Aspirin Use is Associated with Worse Long-Term Outcomes, but Aspirin Use Alone is Safe in Patients with Vasospastic Angina: Results from the VA-Korea Registry, A Prospective Multi-Center Cohort. Sci. Rep. 2019, 9, 17783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takagi, Y.; Yasuda, S.; Takahashi, J.; Tsunoda, R.; Ogata, Y.; Seki, A.; Sumiyoshi, T.; Matsui, M.; Goto, T.; Tanabe, Y.; et al. Clinical implications of provocation tests for coronary artery spasm: Safety, arrhythmic complications, and prognostic impact: Multicentre registry study of the Japanese Coronary Spasm Association. Eur. Heart J. 2013, 34, 258–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarkin, J.M.; Kaski, J.C. Vasodilator Therapy: Nitrates and Nicorandil. Cardiovasc. Drugs Ther. 2016, 30, 367–378. [Google Scholar] [CrossRef]
- Conti, C.R.; Hill, J.A.; Feldman, R.L.; Conti, J.B.; Pepine, C.J. Isosorbide dinitrate and nifedipine in variant angina pectoris. Am. Heart J. 1985, 110, 251–256. [Google Scholar] [CrossRef]
- Munzel, T.; Gori, T. Nitrate therapy and nitrate tolerance in patients with coronary artery disease. Curr. Opin. Pharmacol. 2013, 13, 251–259. [Google Scholar] [CrossRef]
- Thadani, U. Challenges with nitrate therapy and nitrate tolerance: Prevalence, prevention, and clinical relevance. Am. J. Cardiovasc. Drugs 2014, 14, 287–301. [Google Scholar] [CrossRef]
- Munzel, T.; Mollnau, H.; Hartmann, M.; Geiger, C.; Oelze, M.; Warnholtz, A.; Yehia, A.H.; Forstermann, U.; Meinertz, T. Effects of a nitrate-free interval on tolerance, vasoconstrictor sensitivity and vascular superoxide production. J. Am. Coll. Cardiol. 2000, 36, 628–634. [Google Scholar] [CrossRef] [Green Version]
- Munzel, T.; Kurz, S.; Heitzer, T.; Harrison, D.G. New insights into mechanisms underlying nitrate tolerance. Am. J. Cardiol. 1996, 77, 24C–30C. [Google Scholar] [CrossRef]
- O’Rourke, S.T. KATP channel activation mediates nicorandil-induced relaxation of nitrate-tolerant coronary arteries. J. Cardiovasc. Pharmacol. 1996, 27, 831–837. [Google Scholar] [CrossRef]
- Rosenkranz, B.; Winkelmann, B.R.; Parnham, M.J. Clinical pharmacokinetics of molsidomine. Clin. Pharm. 1996, 30, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Messin, R.; Opolski, G.; Fenyvesi, T.; Carreer-Bruhwyler, F.; Dubois, C.; Famaey, J.P.; Geczy, J. Efficacy and safety of molsidomine once-a-day in patients with stable angina pectoris. Int. J. Cardiol. 2005, 98, 79–89. [Google Scholar] [CrossRef]
- Kosugi, M.; Nakagomi, A.; Shibui, T.; Kato, K.; Kusama, Y.; Atarashi, H.; Mizuno, K. Effect of long-term nitrate treatment on cardiac events in patients with vasospastic angina. Circ. J. 2011, 75, 2196–2205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.H.; Park, T.K.; Cho, S.W.; Oh, M.S.; Lee, D.H.; Seong, C.S.; Gwag, H.B.; Lim, A.Y.; Yang, J.H.; Song, Y.B.; et al. Impact of different nitrate therapies on long-term clinical outcomes of patients with vasospastic angina: A propensity score-matched analysis. Int. J. Cardiol. 2018, 252, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.; Kim, M.C.; Ahn, Y.; Cho, K.H.; Sim, D.S.; Hong, Y.J.; Kim, J.H.; Jeong, M.H.; Baek, S.H.; Her, S.H.; et al. Prognostic Impact of Chronic Vasodilator Therapy in Patients With Vasospastic Angina. J. Am. Heart Assoc. 2022, 11, e023776. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All (n = 1048) | Nitrates (n = 239) | Other Types of Vasodilator (n = 809) | p Value | |
|---|---|---|---|---|
| Age, years | 54.8 ± 11.2 | 52.6 ± 11.4 | 55.5 ± 11.1 | 0.001 |
| Male, n (%) | 666 (63.5) | 160 (66.9) | 5056 (62.5) | 0.214 |
| BMI, kg/m2 | 24.7 ± 3.3 | 24.9 ± 4.1 | 24.7 ± 3.1 | 0.450 |
| SBP, mmHg | 126.0 ± 18.0 | 126.8 ± 18.7 | 125.7 ± 17.8 | 0.404 |
| DBP, mmHg | 77.2 ± 12.2 | 78.3 ± 13.3 | 76.9 ± 11.8 | 0.118 |
| Previous CAD, n (%) | 108 (10.3) | 19 (7.9) | 89 (11.0) | 0.171 |
| Diabetes mellitus, n (%) | 101 (9.6) | 20 (8.4) | 81 (10.0) | 0.446 |
| Hypertension, n (%) | 386 (36.9) | 98 (41.0) | 288 (35.6) | 0.131 |
| Dyslipidemia, n (%) | 183 (17.5) | 46 (19.4) | 137 (17.0) | 0.382 |
| Alcohol drinking, n (%) | 455 (43.4) | 137 (57.3) | 318 (39.3) | <0.001 |
| Current smoking, n (%) | 304 (29.5) | 91 (38.1) | 213 (26.9) | 0.001 |
| Laboratory finding | ||||
| Hemoglobin, g/dL | 13.9 ± 1.9 | 13.9 ± 1.8 | 13.9 ± 1.9 | 0.945 |
| Creatinine, mg/dL | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.294 |
| Glucose, mg/dL | 111.3 ± 35.8 | 112.8 ± 46.4 | 110.9 ± 32.1 | 0.565 |
| hs-CRP, mg/dL | 0.9 ± 5.8 | 1.1 ± 7.0 | 0.8 ± 5.3 | 0.453 |
| Total cholesterol, mg/dL | 173.6 ± 35.6 | 175.3 ± 35.2 | 173.0 ± 35.7 | 0.406 |
| LDL cholesterol, mg/dL | 103.1 ± 31.8 | 103.6 ± 31.4 | 103.0 ± 31.9 | 0.811 |
| Triglyceride, mg/dL | 145.7 ± 105.4 | 151.5 ± 94.7 | 143.9 ± 108.6 | 0.349 |
| HDL cholesterol, mg/dL | 46.3 ±12.7 | 42.2 ± 11.9 | 46.7 ± 13.0 | 0.126 |
| LV EF, % | 64.6 ± 6.6 | 65.1 ± 6.1 | 64.4 ± 6.8 | 0.167 |
| Previous cardiovascular medication | ||||
| Antiplatelet, n (%) | 222 (21.3) | 37 (15.5) | 186 (23.0) | 0.042 |
| Statin, n (%) | 163 (15.6) | 26 (10.9) | 137 (16.9) | 0.025 |
| CCB, n (%) | 191 (18.2) | 40 (16.7) | 151 (18.7) | 0.166 |
| Discharge medication | ||||
| CCB, n (%) | 959 (91.5) | 220 (92.1) | 739 (91.3) | 0.732 |
| Clinical diagnosis before ergonovine | ||||
| Angina, n (%) | 962 (92.1) | 226 (94.6) | 736 (91.4) | 0.114 |
| Myocardial infarction, n (%) | 18 (1.7) | 3 (1.3) | 15 (1.9) | 0.777 |
| Cardiac arrest, n (%) | 11 (1.1) | 6 (2.5) | 5 (0.6) | 0.022 |
| Syncope, n (%) | 11 (1.1) | 4 (1.7) | 7 (0.9) | 0.286 |
| VT or VF, n (%) | 5 (0.5) | 1 (0.4) | 4 (0.5) | 1.000 |
| AV block, n (%) | 1 (0.1) | 0 (0.0) | 1 (0.1) | 1.000 |
| All (n = 780) | Nitrates (n = 187) | Other Types of Vasodilator (n = 593) | p Value | |
|---|---|---|---|---|
| Composite events | 23 (2.9) | 10 (5.3) | 13 (2.2) | 0.026 |
| ACS | 17 (2.2) | 8 (4.3) | 9 (1.5) | 0.024 |
| Cardiac death | 1 (0.1) | 0 (0.0) | 1 (0.1) | 0.567 |
| VT or VF | 2 (0.3) | 1 (0.5) | 1 (0.2) | 0.422 |
| AV block | 3 (0.4) | 1 (0.5) | 2 (0.3) | 0.561 |
| All-cause death | 3 (0.4) | 1 (0.5) | 2 (0.3) | 0.561 |
| Readmission or emergency room visits due to angina | 88 (11.3) | 23 (12.3) | 65 (11.0) | 0.614 |
| All (n = 348) | Nitrates (n = 174) | Other Types of Vasodilator (n = 174) | p Value | |
|---|---|---|---|---|
| Composite events | 12 (3.4) | 10 (5.7) | 2 (1.1) | 0.035 |
| ACS | 9 (2.6) | 8 (4.6) | 1 (0.6) | 0.037 |
| Cardiac death | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| VT or VF | 1 (0.3) | 1 (0.6) | 0 (0.0) | 1.000 |
| AV block | 2 (0.6) | 1 (0.6) | 1 (0.6) | 1.000 |
| All-cause death | 2 (0.6) | 1 (0.6) | 1 (0.6) | 1.000 |
| Readmission or emergency room visits due to angina | 43 (12.4) | 22 (12.6) | 21 (12.1) | 0.871 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| Nitrate | 2.86 | 1.104–7.420 | 0.031 | 2.69 | 1.035–6.979 | 0.042 |
| Nicorandil | 1.10 | 0.424–2.847 | 0.847 | - | - | - |
| Molsidomine | 0.04 | 0.000–11.521 | 0.263 | - | - | - |
| Trimetazidine | 0.04 | 0.000–41.670 | 0.368 | - | - | - |
| Age | 0.96 | 0.914–1.000 | 0.049 | 0.96 | 0.915–1.003 | 0.067 |
| Previous CAD | 1.06 | 0.242–4.641 | 0.938 | - | - | - |
| Hypertension | 0.85 | 0.315–2.307 | 0.754 | - | - | - |
| Diabetes | 1.43 | 0.328–6.276 | 0.632 | - | - | - |
| Current smoking | 1.51 | 0.665–3.406 | 0.327 | - | - | - |
| Alcohol drinking | 1.01 | 0.452–2.242 | 0.987 | - | - | - |
| LDL-cholesterol | 1.01 | 0.995–1.026 | 0.193 | - | - | - |
| CCB at index admission | 1.49 | 0.198–11.268 | 0.697 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-J.; Jo, S.-H.; Lee, M.-H.; Seo, W.-W.; Kim, H.-L.; Lee, K.Y.; Yang, T.-H.; Her, S.-H.; Lee, B.-K.; Park, K.-H.; et al. Nitrates vs. Other Types of Vasodilators and Clinical Outcomes in Patients with Vasospastic Angina: A Propensity Score-Matched Analysis. J. Clin. Med. 2022, 11, 3250. https://doi.org/10.3390/jcm11123250
Kim H-J, Jo S-H, Lee M-H, Seo W-W, Kim H-L, Lee KY, Yang T-H, Her S-H, Lee B-K, Park K-H, et al. Nitrates vs. Other Types of Vasodilators and Clinical Outcomes in Patients with Vasospastic Angina: A Propensity Score-Matched Analysis. Journal of Clinical Medicine. 2022; 11(12):3250. https://doi.org/10.3390/jcm11123250
Chicago/Turabian StyleKim, Hyun-Jin, Sang-Ho Jo, Min-Ho Lee, Won-Woo Seo, Hack-Lyoung Kim, Kwan Yong Lee, Tae-Hyun Yang, Sung-Ho Her, Byoung-Kwon Lee, Keun-Ho Park, and et al. 2022. "Nitrates vs. Other Types of Vasodilators and Clinical Outcomes in Patients with Vasospastic Angina: A Propensity Score-Matched Analysis" Journal of Clinical Medicine 11, no. 12: 3250. https://doi.org/10.3390/jcm11123250