
Potential of Hematologic Parameters in Predicting Mortality of Patients with Traumatic Brain Injury

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
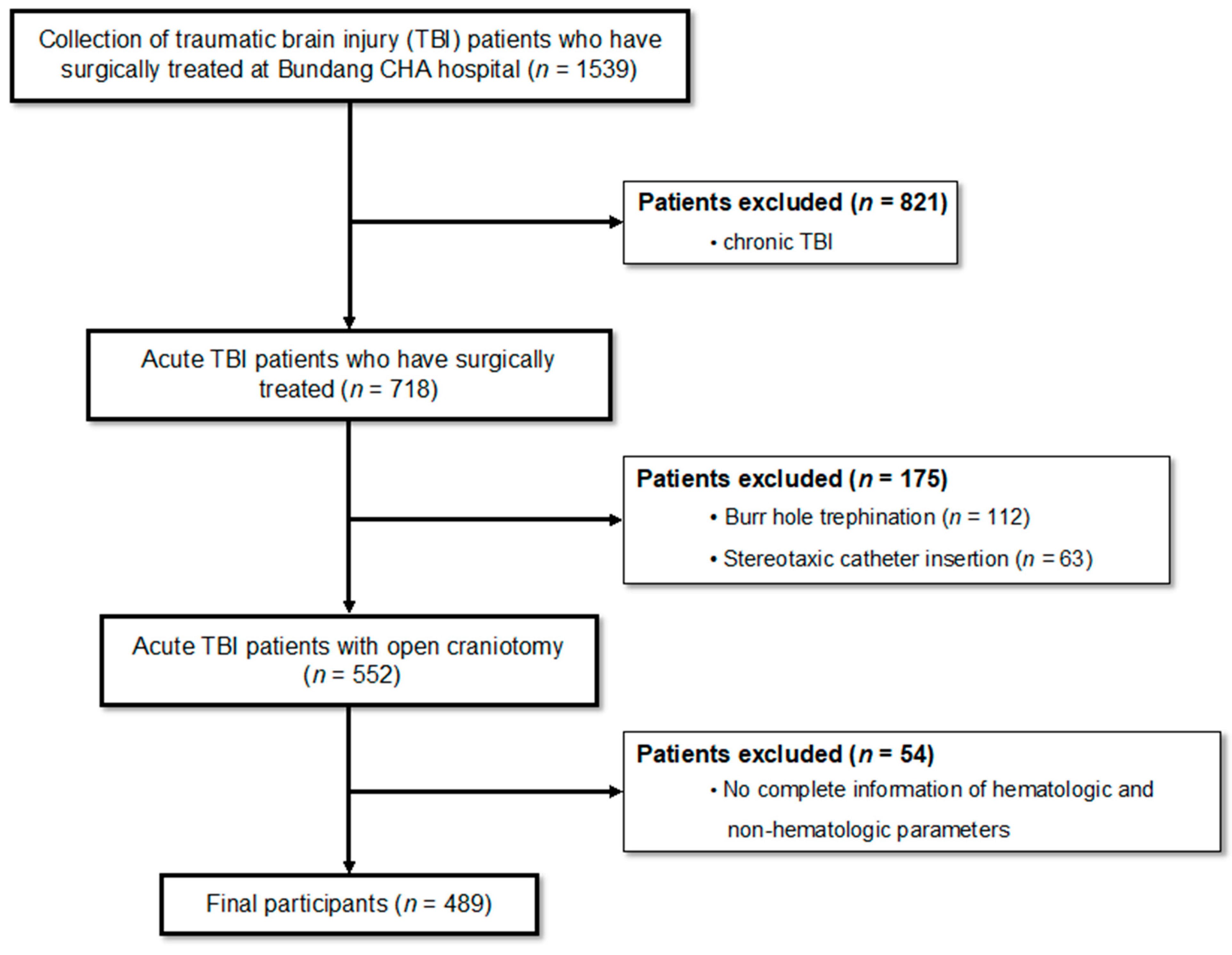
2.1. Inclusion and Exclusion Criteria of Participants
2.2. Clinical Information and Relevance
2.3. Statistical Analysis and Model Development
2.4. Model Validation
3. Results
3.1. Non-Hematologic Parameters on 30-Day Mortality
3.2. Hematologic Parameters on 30-Day Mortality
3.3. Prediction Model with Pre- and Postoperative Hematologic and Non-Hematologic Parameters
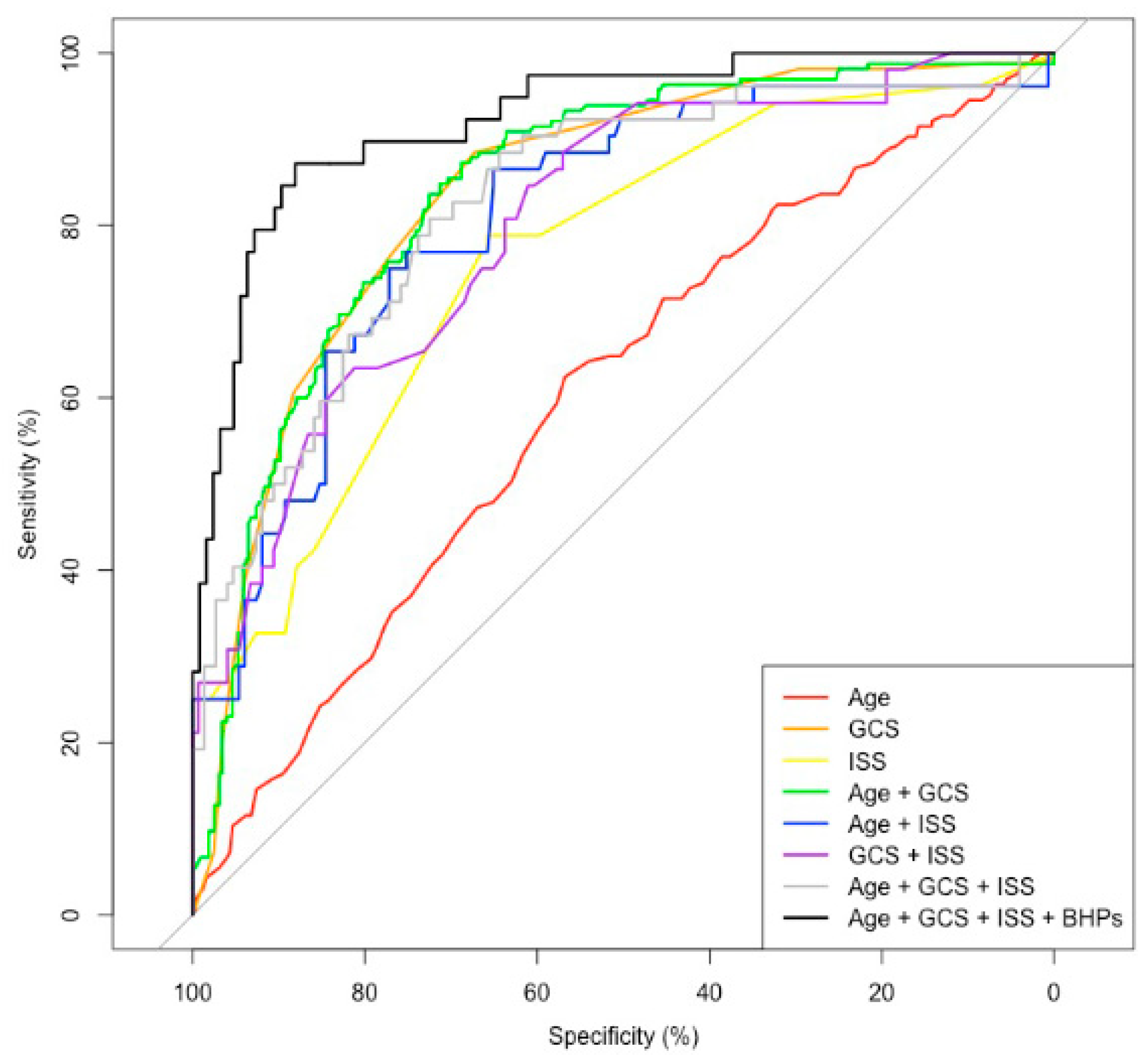
3.4. Performance of the Selected Prediction Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statements, Q. VA/DoD clinical practice guideline for management of concussion/mild traumatic brain injury. J. Rehabil. Res. Dev. 2009, 46, 1–60. [Google Scholar]
- Shafi, S.; Nathens, A.B.; Parks, J.; Cryer, H.M.; Fildes, J.J.; Gentilello, L.M. Trauma quality improvement using risk-adjusted outcomes. J. Trauma Acute Care Surg. 2008, 64, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Darby, J. Case Report: Takotsubo Cardiomyopathy After Traumatic Brain Injury. Front. Neurol. 2021, 12, 727754. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, N.; Santoro, G.; Marani, W.; Petrella, G. Posttraumatic synchronous double acute epidural hematomas: Two craniotomies, single skin incision. Surg. Neurol. Int. 2020, 11, 435. [Google Scholar] [CrossRef]
- Boyd, C.R.; Tolson, M.A.; Copes, W.S. Evaluating trauma care: The TRISS method. Trauma Score and the Injury Severity Score. J. Trauma 1987, 27, 370–378. [Google Scholar] [CrossRef]
- Champion, H.R.; Sacco, W.J.; Carnazzo, A.J.; Copes, W.; Fouty, W.J. Trauma score. Crit. Care Med. 1981, 9, 672–676. [Google Scholar] [CrossRef]
- Champion, H.R.; Sacco, W.J.; Hunt, T.K. Trauma severity scoring to predict mortality. World J. Surg. 1983, 7, 4–11. [Google Scholar] [CrossRef]
- Demetriades, D.; Chan, L.; Velmahos, G.; Berne, T.; Cornwell, E., III; Belzberg, H.; Asensio, J.; Murray, J.; Berne, J.; Shoemaker, W. TRISS methodology in trauma: The need for alternatives. J. Br. Surg. 1998, 85, 379–384. [Google Scholar] [CrossRef]
- Demetriades, D.; Chan, L.; Velmanos, G.V.; Sava, J.; Preston, C.; Gruzinski, G.; Berne, T.V. TRISS methodology: An inappropriate tool for comparing outcomes between trauma centers. J. Am. Coll. Surg. 2001, 193, 250–254. [Google Scholar] [CrossRef]
- Bai, W.; Zhu, W.-L.; Ning, Y.-L.; Li, P.; Zhao, Y.; Yang, N.; Chen, X.; Jiang, Y.-L.; Yang, W.-Q.; Jiang, D.-P. Dramatic increases in blood glutamate concentrations are closely related to traumatic brain injury-induced acute lung injury. Sci. Rep. 2017, 7, 5380. [Google Scholar] [CrossRef] [Green Version]
- Haltmeier, T.; Benjamin, E.; Gruen, J.P.; Shulman, I.A.; Lam, L.; Inaba, K.; Demetriades, D. Decreased mortality in patients with isolated severe blunt traumatic brain injury receiving higher plasma to packed red blood cells transfusion ratios. Injury 2018, 49, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Skaga, N.O.; Eken, T.; Jones, J.M.; Steen, P.A. Different definitions of patient outcome: Consequences for performance analysis in trauma. Injury 2008, 39, 612–622. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.E.; Anderson, K.L.; Hahn, D.R. Evaluating an inclusive trauma system using linked population-based data. J. Trauma Acute Care Surg. 2004, 57, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.E.; DeLorenzo, M.A.; Lucas, F.; Wennberg, D.E. Epidemiology and short-term outcomes of injured medicare patients. J. Am. Geriatr. Soc. 2004, 52, 2023–2030. [Google Scholar] [CrossRef]
- Kim, N.Y.; Lim, J.; Lee, S.; Kim, K.; Hong, J.H.; Chun, D.-H. Hematological factors predicting mortality in patients with traumatic epidural or subdural hematoma undergoing emergency surgical evacuation: A retrospective cohort study. Medicine 2020, 99, e22074. [Google Scholar] [CrossRef]
- Su, S.-H.; Xu, W.; Li, M.; Zhang, L.; Wu, Y.-F.; Yu, F.; Hai, J. Elevated C-reactive protein levels may be a predictor of persistent unfavourable symptoms in patients with mild traumatic brain injury: A preliminary study. Brain Behav. Immun. 2014, 38, 111–117. [Google Scholar] [CrossRef]
- Van Beek, J.G.; Mushkudiani, N.A.; Steyerberg, E.W.; Butcher, I.; McHugh, G.S.; Lu, J.; Marmarou, A.; Murray, G.D.; Maas, A.I. Prognostic value of admission laboratory parameters in traumatic brain injury: Results from the IMPACT study. J. Neurotrauma 2007, 24, 315–328. [Google Scholar] [CrossRef]
- Rainey, T.; Lesko, M.; Sacho, R.; Lecky, F.; Childs, C. Predicting outcome after severe traumatic brain injury using the serum S100B biomarker: Results using a single (24 h) time-point. Resuscitation 2009, 80, 341–345. [Google Scholar] [CrossRef]
- Salim, A.; Hadjizacharia, P.; DuBose, J.; Brown, C.; Inaba, K.; Chan, L.; Margulies, D.R. Role of anemia in traumatic brain injury. J. Am. Coll. Surg. 2008, 207, 398–406. [Google Scholar] [CrossRef]
- Rovlias, A.; Kotsou, S. The blood leukocyte count and its prognostic significance in severe head injury. Surg. Neurol. 2001, 55, 190–196. [Google Scholar] [CrossRef]
- Zhou, J.-K.; Zhang, Q.-S.; Chen, Y.-Q.; Li, M.; Xie, Y.; Ke, J.-J.; Lin, H.-Z.; Zhang, Y.-W. Use of Hematocrit for Short-Term Prognosis of Patients with Traumatic Brain Injury After Decompressive Craniectomy. World Neurosurg. 2019, 123, e141–e146. [Google Scholar] [CrossRef] [PubMed]
- Jeremitsky, E.; Omert, L.; Dunham, C.M.; Protetch, J.; Rodriguez, A. Harbingers of poor outcome the day after severe brain injury: Hypothermia, hypoxia, and hypoperfusion. J. Trauma Acute Care Surg. 2003, 54, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Carlson, A.P.; Schermer, C.R.; Lu, S.W. Retrospective evaluation of anemia and transfusion in traumatic brain injury. J. Trauma Acute Care Surg. 2006, 61, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Ziebell, J.M.; Morganti-Kossmann, M.C. Involvement of pro-and anti-inflammatory cytokines and chemokines in the pathophysiology of traumatic brain injury. Neurotherapeutics 2010, 7, 22–30. [Google Scholar] [CrossRef] [Green Version]
- Morganti-Kossmann, M.C.; Rancan, M.; Otto, V.I.; Stahel, P.F.; Kossmann, T. Role of cerebral inflammation after traumatic brain injury: A revisited concept. Shock 2001, 16, 165–177. [Google Scholar] [CrossRef]
- Gabbe, B.J.; Cameron, P.A.; Wolfe, R. TRISS: Does it get better than this? Acad. Emerg. Med. 2004, 11, 181–186. [Google Scholar] [CrossRef]
- Hannan, E.L.; Farrell, L.S.; Gorthy, S.-F.H.; Bessey, P.Q.; Cayten, C.G.; Cooper, A.; Mottley, L. Predictors of mortality in adult patients with blunt injuries in New York State: A comparison of the Trauma and Injury Severity Score (TRISS) and the International Classification of Disease, Ninth Revision-based Injury Severity Score (ICISS). J. Trauma Acute Care Surg. 1999, 47, 8–14. [Google Scholar] [CrossRef]
- Hannan, E.L.; Mendeloff, J.; Farrell, L.S.; Cayten, C.G.; Murphy, J.G. Validation of TRISS and ASCOT using a non-MTOS trauma registry. J. Trauma Acute Care Surg. 1995, 38, 83–88. [Google Scholar] [CrossRef]
- Garber, B.G.; Hebert, P.C.; Wells, G.; Yelle, J.-D. Validation of trauma and injury severity score in blunt trauma patients by using a Canadian trauma registry. J. Trauma Acute Care Surg. 1996, 40, 733–737. [Google Scholar] [CrossRef]
- Cayten, C.; Stahl, W.; Murphy, J.; Agarwal, N.; Byrne, D. Limitations of the TRISS method for interhospital comparisons: A multihospital study. J. Trauma 1991, 31, 471–481; discussion 481. [Google Scholar] [CrossRef]
- Davis, D.P.; Serrano, J.A.; Vilke, G.M.; Sise, M.J.; Kennedy, F.; Eastman, A.B.; Velky, T.; Hoyt, D.B. The predictive value of field versus arrival Glasgow Coma Scale score and TRISS calculations in moderate-to-severe traumatic brain injury. J. Trauma Acute Care Surg. 2006, 60, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Marion, D.W.; Carlier, P.M. Problems with initial Glasgow Coma Scale assessment caused by prehospital treatment of patients with head injuries: Results of a national survey. J. Trauma 1994, 36, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Arbabi, S.; Jurkovich, G.J.; Wahl, W.L.; Franklin, G.A.; Hemmila, M.R.; Taheri, P.A.; Maier, R.V. A comparison of prehospital and hospital data in trauma patients. J. Trauma Acute Care Surg. 2004, 56, 1029–1032. [Google Scholar] [CrossRef] [PubMed]
- Gill, M.R.; Reiley, D.G.; Green, S.M. Interrater reliability of Glasgow Coma Scale scores in the emergency department. Ann. Emerg. Med. 2004, 43, 215–223. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Long Survival Group | Short Survival Group | p-Value | |
|---|---|---|---|
| Age, n (mean) | 324 (46.69 years) | 165 (54.38 years) | <0.001 |
| Height, n (mean) | 324 (166.92 cm) | 165 (163.08 cm) | 0.4488 |
| Weight, n (mean) | 324 (60.29 kg) | 165 (61.04 kg) | 0.6028 |
| Sex (n) | |||
| Male | 248 | 119 | |
| Female | 76 | 46 | |
| 0.3381 | |||
| ISS, n (mean) | 149 (17.69) | 52 (34) | <0.001 |
| GCS, n (mean) | 324 (9.72) | 165 (6.28) | <0.001 |
| Long Survival Group | Short Survival Group | p-Value | p Adj | |
|---|---|---|---|---|
| Preoperative, n (Mean) | ||||
| RDW | 321 (13.58%) | 164 (14.02%) | 0.016 | 0.346 |
| MPV | 312 (8.75 fL) | 162 (8.48 fL) | 0.037 | 0.822 |
| WBC | 321 (13.36 × 103/uL) | 164 (13.93 × 103/uL) | 0.367 | 1.000 |
| Hemoglobin | 322 (12.98 g/dL) | 164(12.19 g/dL) | <0.001 | 0.012 |
| Hematocrit | 322 (37.87%) | 164 (35.8%) | 0.002 | 0.035 |
| Platelets | 321 (222.44 × 103/uL) | 164 (192.74 × 103/uL) | <0.001 | 0.017 |
| CRP | 288 (7.88 mg/dL) | 122 (12.25 mg/dL) | <0.001 | 0.009 |
| Creatinine | 322 (0.94 mg/dL) | 163 (1.13 mg/dL) | 0.046 | 1 |
| MCV | 321 (91 fL) | 164 (93.7 fL) | <0.001 | <0.001 |
| MCH | 321 (31.16 pg) | 164 (31.92 pg) | <0.001 | 0.015 |
| MCHC | 321 (34.24 g/dL) | 164 (34.06 g/dL) | 0.021 | 0.467 |
| Postoperative, n (Mean) | ||||
| RDW | 321 (13.87%)) | 162 (14.27%)) | 0.015 | 0.323 |
| MPV | 312 (8.7 fL) | 160 (8.35 fL) | 0.008 | 0.166 |
| WBC | 321 (14.02 × 103/uL) | 162 (14.19 × 103/uL) | 0.632 | 1.000 |
| Hemoglobin | 324 (11.98 g/dL) | 162 (11.17 g/dL) | <0.001 | 0.004 |
| Hematocrit | 324 (34.92%) | 162 (32.87%) | <0.001 | 0.021 |
| Platelets | 324 (183.84 × 103/uL) | 162 (139.11 × 103/uL) | <0.001 | <0.001 |
| CRP | 153 (8.09 mg/dL) | 62 (10.84 mg/dL) | 0.055 | 1.000 |
| Creatinine | 324 (0.86 mg/dL) | 160 (1.15 mg/dL) | 0.023 | 0.503 |
| MCV | 321 (90.69 fL) | 162 (92.14 fL) | 0.003 | 0.055 |
| MCH | 321 (31.1 pg) | 162 (31.44 pg) | 0.060 | 1.000 |
| MCHC | 321 (34.29 g/dL) | 162 (34.13 g/dL) | 0.039 | 0.867 |
| Parameter | Coefficient | Std. Error | Z-Statics | p-Value |
|---|---|---|---|---|
| Intercept | −7.621 | 3.293 | −2.314 | 0.021 |
| Age | 0.048 | 0.020 | 2.391 | 0.017 |
| GCS | −0.434 | 0.128 | −3.401 | 0.001 |
| ISS | 0.103 | 0.033 | 3.133 | 0.002 |
| Pre-Hct | 0.398 | 0.115 | 3.450 | 0.001 |
| Post-WBC | −0.115 | 0.061 | −1.904 | 0.057 |
| Pre-CRP | −0.111 | 0.069 | −1.605 | 0.108 |
| Post-Hgb | −0.815 | 0.272 | −2.996 | 0.003 |
| Post-CRP | 0.171 | 0.071 | 2.410 | 0.016 |
| Prediction Model | AUC (CI 95%) | Adj. AUC | AIC | AICc | HL (Statistic) | HL (p-Value) |
|---|---|---|---|---|---|---|
| Age | 60.32 (55.06–65.59) | 60.205 | 615.349 | 615.358 | 8.479 | 0.388 |
| GCS | 83.85 (80.16–87.54) | 83.815 | 465.127 | 465.135 | - | - |
| ISS | 76.06 (68.53–83.6) | 76.015 | 188.433 | 188.453 | 3.845 | 0.871 |
| Age + GCS | 84.2 (80.55–87.85) | 84.115 | 463.669 | 463.694 | 9.149 | 0.330 |
| Age + ISS | 80.96 (73.91–88.02) | 80.435 | 182.128 | 182.189 | 11.196 | 0.191 |
| GCS + ISS | 80.19 (73.32–87.07) | 79.900 | 182.356 | 182.417 | 11.622 | 0.169 |
| Age + GCS + ISS | 82.6 (75.83–89.38) | 81.825 | 177.760 | 177.882 | 8.937 | 0.348 |
| Age + GCS + ISS + BHPs | 92.53 (87.84–97.22) | 90.045 | 109.944 | 110.868 | 8.468 | 0.389 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.B.; Park, Y.; Ahn, J.W.; Sim, J.; Park, J.; Kim, Y.J.; Hwang, S.J.; Sung, K.S.; Lim, J. Potential of Hematologic Parameters in Predicting Mortality of Patients with Traumatic Brain Injury. J. Clin. Med. 2022, 11, 3220. https://doi.org/10.3390/jcm11113220
Kim SB, Park Y, Ahn JW, Sim J, Park J, Kim YJ, Hwang SJ, Sung KS, Lim J. Potential of Hematologic Parameters in Predicting Mortality of Patients with Traumatic Brain Injury. Journal of Clinical Medicine. 2022; 11(11):3220. https://doi.org/10.3390/jcm11113220
Chicago/Turabian StyleKim, Sol Bi, Youngjoon Park, Ju Won Ahn, Jeongmin Sim, Jeongman Park, Yu Jin Kim, So Jung Hwang, Kyoung Su Sung, and Jaejoon Lim. 2022. "Potential of Hematologic Parameters in Predicting Mortality of Patients with Traumatic Brain Injury" Journal of Clinical Medicine 11, no. 11: 3220. https://doi.org/10.3390/jcm11113220