
Health-Screening-Based Chronic Obstructive Pulmonary Disease and Its Effect on Cardiovascular Disease Risk

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
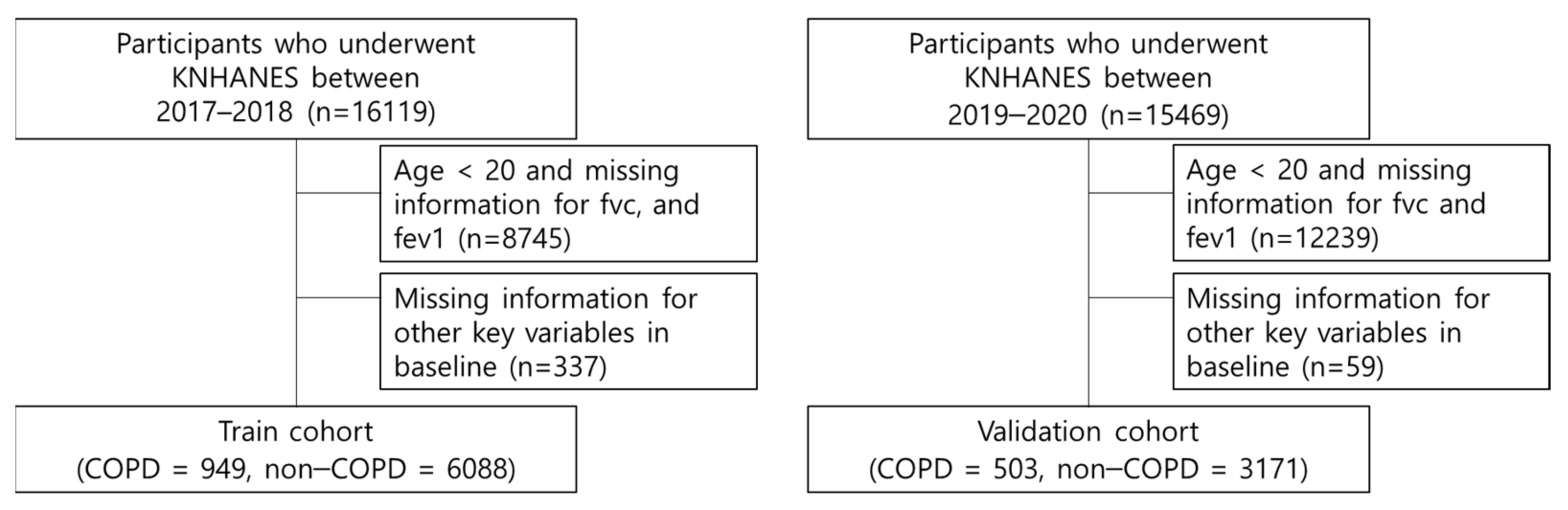
2.1. Study Population
2.2. Definition of Variables
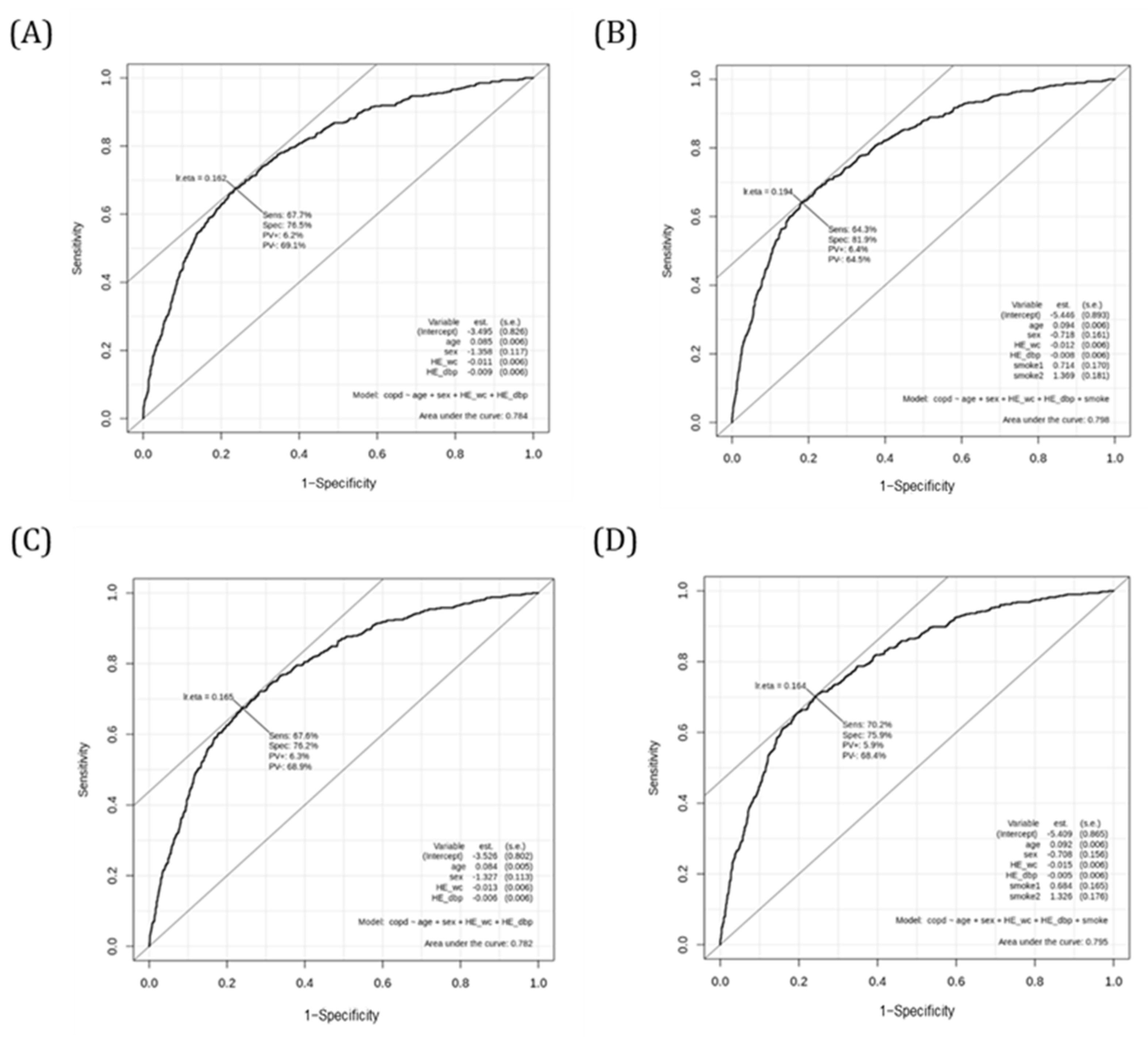
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, P.J.; Celli, B.R. Systemic manifestations and comorbidities of COPD. Eur. Respir. J. 2009, 33, 1165–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, A.R.; Hurst, J.R. Extrapulmonary comorbidities in chronic obstructive pulmonary disease: State of the art. Expert Rev. Respir. Med. 2011, 5, 647–662. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, N.; Muro, S.; Hirai, T.; Oguma, T.; Terada, K.; Marumo, S.; Kinose, D.; Ogawa, E.; Hoshino, Y.; Mishima, M. Impact of exacerbations on emphysema progression in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2011, 183, 1653–1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donaldson, G.C.; Seemungal, T.A.; Bhowmik, A.; Wedzicha, J.A. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax 2002, 57, 847–852. [Google Scholar] [CrossRef] [Green Version]
- Burden of Lung Disease Report. 2006. Available online: www.britthoracic.org.uk/copd/pubs_frameset.html (accessed on 15 April 2022).
- Mannino, D.M.; Buist, A.S. Global burden of COPD: Risk factors, prevalence, and future trends. Lancet 2007, 370, 765–773. [Google Scholar] [CrossRef]
- Lopez-Campos, J.L.; Tan, W.; Soriano, J.B. Global burden of COPD. Respirology 2016, 21, 14–23. [Google Scholar] [CrossRef]
- Cheng, S.L.; Chan, M.C.; Wang, C.C.; Lin, C.H.; Wang, H.C.; Hsu, J.Y.; Hang, L.W.; Chang, C.J.; Perng, D.W.; Yu, C.J. COPD in Taiwan: A National Epidemiology Survey. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 2459–2467. [Google Scholar] [CrossRef] [Green Version]
- Vestbo, J.; Hurd, S.S.; Agustí, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Berman, L.B.; Townsend, M.; Pugsley, S.O.; Chambers, L.W. A measure of quality of life for clinical trials in chronic lung disease. Thorax 1987, 42, 773–778. [Google Scholar] [CrossRef] [Green Version]
- Karloh, M.; Fleig Mayer, A.; Maurici, R.; Pizzichini, M.M.M.; Jones, P.W.; Pizzichini, E. The COPD Assessment Test: What Do We Know So Far?: A Systematic Review and Meta-Analysis About Clinical Outcomes Prediction and Classification of Patients Into GOLD Stages. Chest 2016, 149, 413–425. [Google Scholar] [CrossRef]
- Guerra, B.; Gaveikaite, V.; Bianchi, C.; Puhan, M.A. Prediction models for exacerbations in patients with COPD. Eur. Respir. Rev. 2017, 26, 160061. [Google Scholar] [CrossRef] [Green Version]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD statement. Ann. Intern. Med. 2015, 162, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- An, K.Y. Physical activity level in Korean adults: The Korea National Health and Nutrition Examination Survey 2017. Epidemiol. Health 2019, 41, e2019047. [Google Scholar] [CrossRef]
- Zhang, Z. Model building strategy for logistic regression: Purposeful selection. Ann. Transl. Med. 2016, 4, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogg, J.C. Pathophysiology of airflow limitation in chronic obstructive pulmonary disease. Lancet 2004, 364, 709–721. [Google Scholar] [CrossRef]
- Hogg, J.C.; Chu, F.; Utokaparch, S.; Woods, R.; Elliott, W.M.; Buzatu, L.; Cherniack, R.M.; Rogers, R.M.; Sciurba, F.C.; Coxson, H.O.; et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N. Engl. J. Med. 2004, 350, 2645–2653. [Google Scholar] [CrossRef] [PubMed]
- Galban, C.J.; Han, M.K.; Boes, J.L.; Chughtai, K.A.; Meyer, C.R.; Johnson, T.D.; Galbán, S.; Rehemtulla, A.; Kazerooni, E.A.; Martinez, F.J.; et al. Computed tomography-based biomarker provides unique signature for diagnosis of COPD phenotypes and disease progression. Nat. Med. 2012, 18, 1711–1715. [Google Scholar] [CrossRef]
- Di Stefano, A.; Caramori, G.; Oates, T.; Capelli, A.; Lusuardi, M.; Gnemmi, I.; Ioli, F.; Chung, K.F.; Donner, C.F.; Barnes, P.J.; et al. Increased expression of nuclear factor-kappaB in bronchial biopsies from smokers and patients with COPD. Eur. Respir. J. 2002, 20, 556–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mills, P.R.; Davies, R.J.; Devalia, J.L. Airway epithelial cells, cytokines, and pollutants. Am. J. Respir. Crit. Care Med. 1999, 160, S38–S43. [Google Scholar] [CrossRef] [PubMed]
- Marrack, P.; Kappler, J.; Kotzin, B.L. Autoimmune disease: Why and where it occurs. Nat. Med. 2001, 7, 899–905. [Google Scholar] [CrossRef]
- Curtis, J.L.; Freeman, C.M.; Hogg, J.C. The immunopathogenesis of chronic obstructive pulmonary disease: Insights from recent research. Proc. Am. Thorac. Soc. 2007, 4, 512–521. [Google Scholar] [CrossRef] [PubMed]
- Yanai, M.; Sekizawa, K.; Ohrui, T.; Sasaki, H.; Takishima, T. Site of airway obstruction in pulmonary disease: Direct measurement of intrabronchial pressure. J. Appl. Physiol. 1992, 72, 1016–1023. [Google Scholar] [CrossRef]
- Sevenoaks, M.J.; Stockley, R.A. Chronic Obstructive Pulmonary Disease, inflammation and co-morbidity—A common inflammatory phenotype? Respir. Res. 2006, 7, 70. [Google Scholar] [CrossRef] [Green Version]
- McLean, A.; Warren, P.M.; Gillooly, M.; MacNee, W.; Lamb, D. Microscopic and macroscopic measurements of emphysema: Relation to carbon monoxide gas transfer. Thorax 1992, 47, 144–149. [Google Scholar] [CrossRef] [Green Version]
- Weitzenblum, E.; Schrijen, F.; Mohan-Kumar, T.; Colas des Francs, V.; Lockhart, A. Variability of the pulmonary vascular response to acute hypoxia in chronic bronchitis. Chest 1988, 94, 772–778. [Google Scholar] [CrossRef] [Green Version]
- Stenmark, K.R.; Fagan, K.A.; Frid, M.G. Hypoxia-induced pulmonary vascular remodeling: Cellular and molecular mechanisms. Circ. Res. 2006, 99, 675–691. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, M.; Yuan, J.X. Hypoxic pulmonary vasoconstriction: Role of voltage-gated potassium channels. Respir. Res. 2000, 1, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Sin, D.D.; Wu, L.; Man, S.F. The relationship between reduced lung function and cardiovascular mortality: A population-based study and a systematic review of the literature. Chest 2005, 127, 1952–1959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barr, R.G.; Mesia-Vela, S.; Austin, J.H.; Basner, R.C.; Keller, B.M.; Reeves, A.P.; Shimbo, D.; Stevenson, L. Impaired flow-mediated dilation is associated with low pulmonary function and emphysema in ex-smokers: The Emphysema and Cancer Action Project (EMCAP) Study. Am. J. Respir. Crit. Care Med. 2007, 176, 1200–1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, S.; Arjomandi, M.; Tong, Y.; Liao, Z.C.; Luo, G. Developing a Machine Learning Model to Predict Severe Chronic Obstructive Pulmonary Disease Exacerbations: Retrospective Cohort Study. J. Med. Internet Res. 2022, 24, e28953. [Google Scholar] [CrossRef] [PubMed]
- Chmiel, F.P.; Burns, D.K.; Pickering, J.B.; Blythin, A.; Wilkinson, T.M.; Boniface, M.J. Prediction of Chronic Obstructive Pulmonary Disease Exacerbation Events by Using Patient Self-reported Data in a Digital Health App: Statistical Evaluation and Machine Learning Approach. JMIR Med. Inform. 2022, 10, e26499. [Google Scholar] [CrossRef]
- Takahashi, T.; Muro, S.; Tanabe, N.; Terada, K.; Kiyokawa, H.; Sato, S.; Hoshino, Y.; Ogawa, E.; Uno, K.; Naruishi, K.; et al. Relationship between periodontitis-related antibody and frequent exacerbations in chronic obstructive pulmonary disease. PLoS ONE 2012, 7, e40570. [Google Scholar] [CrossRef]
- Wouters, E.F. Economic analysis of the Confronting COPD survey: An overview of results. Respir. Med. 2003, 97 (Suppl. C), S3–S14. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Overall (n = 7037) | Non-COPD (n = 6088) | COPD (n = 949) | p-Value |
|---|---|---|---|---|
| Age, years | 58.4 (11.2) | 57.1 (10.9) | 66.6 (9.7) | <0.001 |
| Sex, female, n (%) | 3909 (55.5) | 3647 (59.9) | 262 (27.6) | <0.001 |
| Height, cm | 161.9 (8.8) | 161.6 (8.7) | 164.2 (8.8) | <0.001 |
| Weight, kg | 63.6 (11.0) | 63.6 (11.1) | 63.9 (10.3) | 0.482 |
| Body mass index, kg/m2 | 24.2 (3.2) | 24.3 (3.2) | 23.6 (2.8) | <0.001 |
| Waist circumference, cm | 83.3 (9.2) | 83.1 (9.3) | 84.8 (8.5) | <0.001 |
| Systolic blood pressure, mmHg | 121.2 (16.7) | 120.8 (16.8) | 123.7 (15.9) | <0.001 |
| Diastolic blood pressure, mmHg | 76.2 (10.1) | 76.6 (10.0) | 73.3 (10.2) | <0.001 |
| Fasting serum glucose, mg/dL | 104.0 (24.5) | 103.7 (24.2) | 106.1 (26.0) | 0.006 |
| Total cholesterol, mg/dL | 195.2 (39.1) | 196.7 (39.0) | 185.9 (38.0) | <0.001 |
| Triglyceride, mg/dL | 141.2 (106.4) | 141.2 (107.8) | 141.6 (97.4) | 0.905 |
| Aspartate aminotransferase, IU/L | 24.0 (11.5) | 23.9 (11.8) | 24.5 (9.1) | 0.100 |
| Alanine aminotransferase, IU/L | 22.6 (14.9) | 22.8 (15.3) | 21.5 (11.6) | 0.002 |
| Blood urea nitrogen, mg/dL | 15.6 (4.6) | 15.5 (4.5) | 16.7 (4.8) | <0.001 |
| Creatinine, mg/dL | 0.8 (0.2) | 0.8 (0.2) | 0.9 (0.3) | <0.001 |
| Urinary protein | ||||
| Negative 1 | 6085 (86.2) | 5271 (86.6) | 794 (83.7) | 0.082 |
| Positive 2 | 972 (13.8) | 817 (13.4) | 155 (16.3) | |
| Urinary glucose | ||||
| Negative 1 | 6671 (86.2) | 5782 (95.0) | 889 (93.7) | 0.056 |
| Positive 2 | 972 (13.8) | 306 (5.0) | 60 (6.3) | |
| Urinary pH | 5.9 (0.8) | 5.9 (0.8) | 5.9 (0.8) | 0.585 |
| Alcohol consumption, n (%) | ||||
| No | 4012 (57.0) | 3514 (57.7) | 498 (52.5) | 0.003 |
| Yes | 3025 (43.0) | 2574 (42.3) | 451 (47.5) | |
| Smoking, n (%) | ||||
| Never | 4131 (58.7) | 3821 (62.8) | 310 (32.7) | 0.633 |
| Past | 1722 (24.5) | 1353 (22.2) | 369 (38.9) | |
| Current | 1184 (16.8) | 914 (15.0) | 270 (28.5) | |
| Physical activity, n (%) | ||||
| No | 4347 (61.8) | 3731 (61.3) | 616 (64.9) | 0.036 |
| Yes | 2690 (38.2) | 2357 (38.7) | 333 (35.1) | |
| Cardiovascular disease | ||||
| No | 6686 (95.0) | 5823 (95.6) | 863 (90.9) | <0.001 |
| Yes | 351 (5.0) | 265 (4.4) | 86 (9.1) | |
| Chronic heart disease | ||||
| No | 6820 (96.9) | 5923 (97.3) | 897 (94.5) | <0.001 |
| Yes | 217 (3.1) | 165 (2.7) | 52 (5.5) | |
| Stroke | ||||
| No | 6883 (97.8) | 5975 (98.1) | 908 (95.7) | <0.001 |
| Yes | 154 (2.2) | 113 (1.9) | 41 (4.3) |
| Variable | Estimate | OR (95% CI) | p-Value | C-Index |
|---|---|---|---|---|
| Age, years | 0.081 | 1.080 (1.080–1.090) | <0.001 | 0.743 |
| Sex, female | −1.365 | 0.260 (0.220–0.300) | <0.001 | 0.661 |
| Height, cm | 0.034 | 1.030 (1.030–1.040) | 0.011 | 0.592 |
| Weight, kg | 0.002 | 1.002 (0.996–1.008) | 0.508 | 0.515 |
| Body mass index, kg/m2 | −0.067 | 0.940 (0.910–0.960) | <0.001 | 0.553 |
| Waist circumference, cm | 0.019 | 1.020 (1.010–1.030) | <0.001 | 0.557 |
| Alcohol consumption | ||||
| yes (vs. no) | 0.212 | 1.240 (1.080–1.420) | 0.002 | 0.526 |
| Smoking | <0.001 | 0.653 | ||
| Past vs. Never | 1.212 | 3.360 (2.860–3.960) | <0.001 | |
| Current vs. Never | 1.292 | 3.640 (3.050–4.350) | <0.001 | |
| Physical activity | ||||
| yes (vs. no) | −1.801 | 0.860 (0.740–0.990) | 0.032 | 0.518 |
| Blood pressure | ||||
| Systolic blood pressure, mmHg | 0.010 | 1.010 (1.010–1.010) | <0.001 | 0.557 |
| Diastolic blood pressure, mmHg | −0.034 | 0.970 (0.960–0.970) | <0.001 | 0.590 |
| Diabetes mellitus test | ||||
| Fasting serum glucose, mg/dL | 0.004 | 1.004 (1.001–1.006) | 0.006 | 0.544 |
| Dyslipidemia test | ||||
| Total cholesterol, mg/dL | −0.007 | 0.993 (0.991–0.995) | <0.001 | 0.579 |
| Triglyceride, mg/dL | 0.000 | 1.000 (0.999–1.001) | 0.911 | 0.515 |
| Liver function test | ||||
| Aspartate aminotransferase, IU/L | 0.004 | 1.004 (0.998–1.009) | 0.176 | 0.542 |
| Alanine aminotransferase, IU/L | −0.007 | 0.993 (0.998–0.999) | 0.013 | 0.509 |
| Kidney function test | ||||
| Blood urea nitrogen, mg/dL | 0.053 | 1.050 (1.040–1.070) | <0.001 | 0.574 |
| Creatinine, mg/dL | 1.663 | 5.280 (3.890–7.160) | <0.001 | 0.641 |
| Urine test | ||||
| Urinary protein (vs. Negative) | 0.169 | 1.180 (1.050–1.330) | 0.007 | 0.515 |
| Urinary glucose (vs. Negative) | 0.025 | 1.030 (0.940–1.120) | 0.590 | 0.506 |
| Urinary pH | 0.023 | 1.020 (0.940–1.110) | 0.579 | 0.504 |
| Covariate | Estimate | OR (95% CI) | p-Value |
|---|---|---|---|
| Intercept | −3.582 | <0.001 | |
| Age, years | 0.083 | 1.087 (1.075–1.095) | <0.001 |
| Sex, female | −1.636 | 0.195 (0.164–0.230) | <0.001 |
| Waist circumference, cm | −0.019 | 0.981 (0.972–0.990) | <0.001 |
| Diastolic blood pressure, mmHg | −0.015 | 0.985 (0.977–0.993) | <0.001 |
| COPD Score, Range | COPD, n (%) | OR (95% CI) | p-Value | |
|---|---|---|---|---|
| 1st quartile | −3.872 (−5.435–−3.273) | 918 (24.986) | 1.000 (reference) | |
| 2nd quartile | −2.852 (−3.272–−2.460) | 919 (25.014) | 1.838 (1.156–2.923) | 0.010 |
| 3rd quartile | −1.998 (−2.460–−1.509) | 919 (25.014) | 4.297 (2.827–6.534) | <0.001 |
| 4th quartile | −0.745 (−1.509–−1.026) | 918 (24.986) | 15.553 (10.484−23.071) | <0.001 |
| Estimate | OR (95% CI) | p-Value | C-Index | |
|---|---|---|---|---|
| CVD | 0.665 | 1.945(1.776–2.130) | <0.001 | 0.730 |
| CHD | 0.755 | 2.128(1.896–2.390) | <0.001 | 0.758 |
| Stroke | 0.507 | 1.661(1.459–1.890) | <0.001 | 0.683 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-J.; Yoon, S.-S.; Lee, M.-H.; Kim, H.-J.; Lim, Y.; Park, H.; Park, S.J.; Jeong, S.; Han, H.-W. Health-Screening-Based Chronic Obstructive Pulmonary Disease and Its Effect on Cardiovascular Disease Risk. J. Clin. Med. 2022, 11, 3181. https://doi.org/10.3390/jcm11113181
Lee S-J, Yoon S-S, Lee M-H, Kim H-J, Lim Y, Park H, Park SJ, Jeong S, Han H-W. Health-Screening-Based Chronic Obstructive Pulmonary Disease and Its Effect on Cardiovascular Disease Risk. Journal of Clinical Medicine. 2022; 11(11):3181. https://doi.org/10.3390/jcm11113181
Chicago/Turabian StyleLee, Sang-Jun, Sung-Soo Yoon, Myeong-Hoon Lee, Hye-Jun Kim, Yohwan Lim, Hyewon Park, Sun Jae Park, Seogsong Jeong, and Hyun-Wook Han. 2022. "Health-Screening-Based Chronic Obstructive Pulmonary Disease and Its Effect on Cardiovascular Disease Risk" Journal of Clinical Medicine 11, no. 11: 3181. https://doi.org/10.3390/jcm11113181