
Prognostic Value of 12-Leads Electrocardiogram at Emergency Department in Hospitalized Patients with Coronavirus Disease-19

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
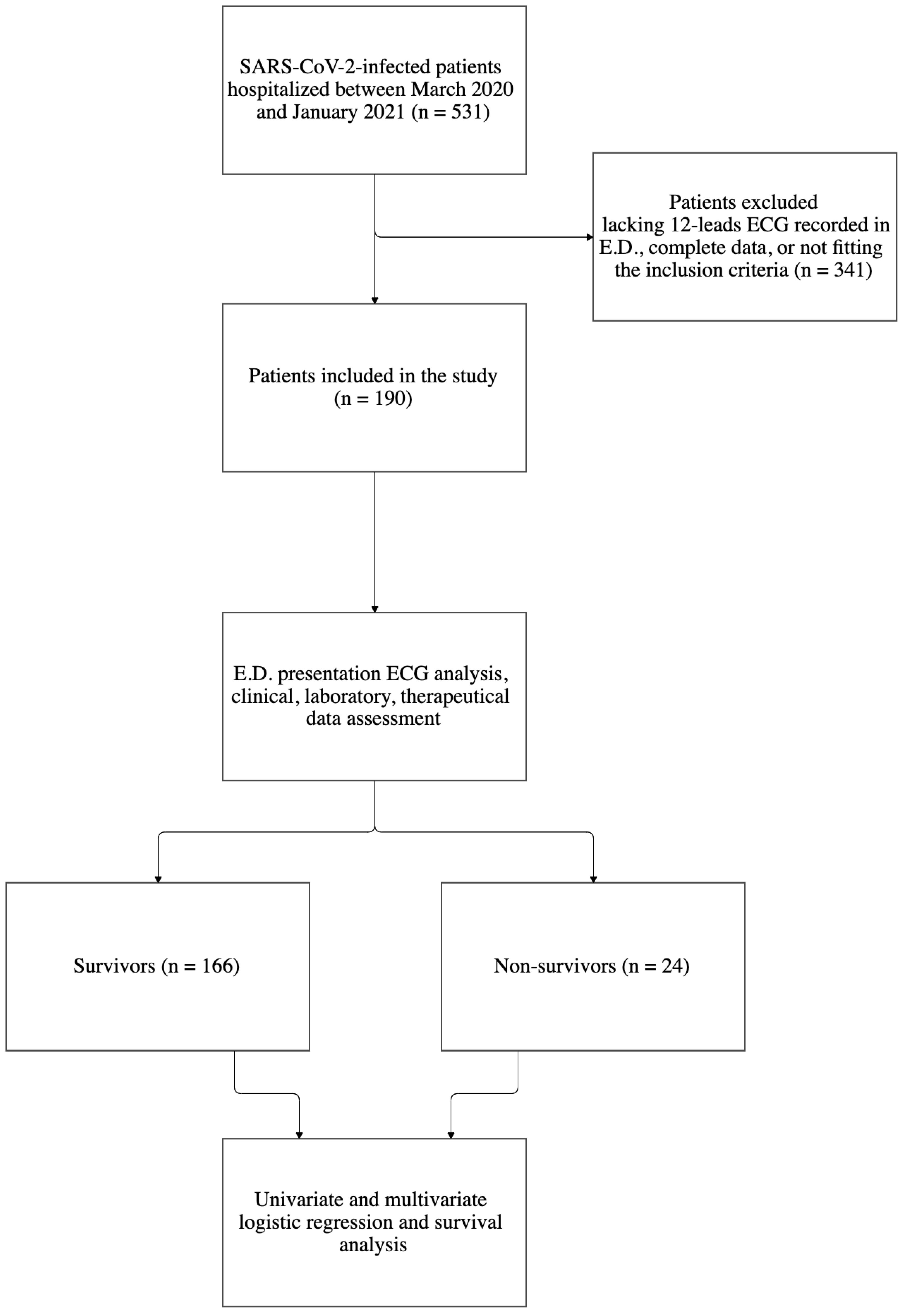
2.1. Study Design and Setting
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Definitions
2.4. ECG Analysis
2.5. Definitions
2.6. Statistical Analysis
3. Results
3.1. Demographics and Outcome
3.2. Baseline Comorbidities
3.3. Clinical Presentation and Characteristics at E.D.
3.4. ECG Findings on E.D. Admission
3.5. Arrhythmic Events during Hospitalization
3.6. Anti-SARS-CoV-2 Therapies
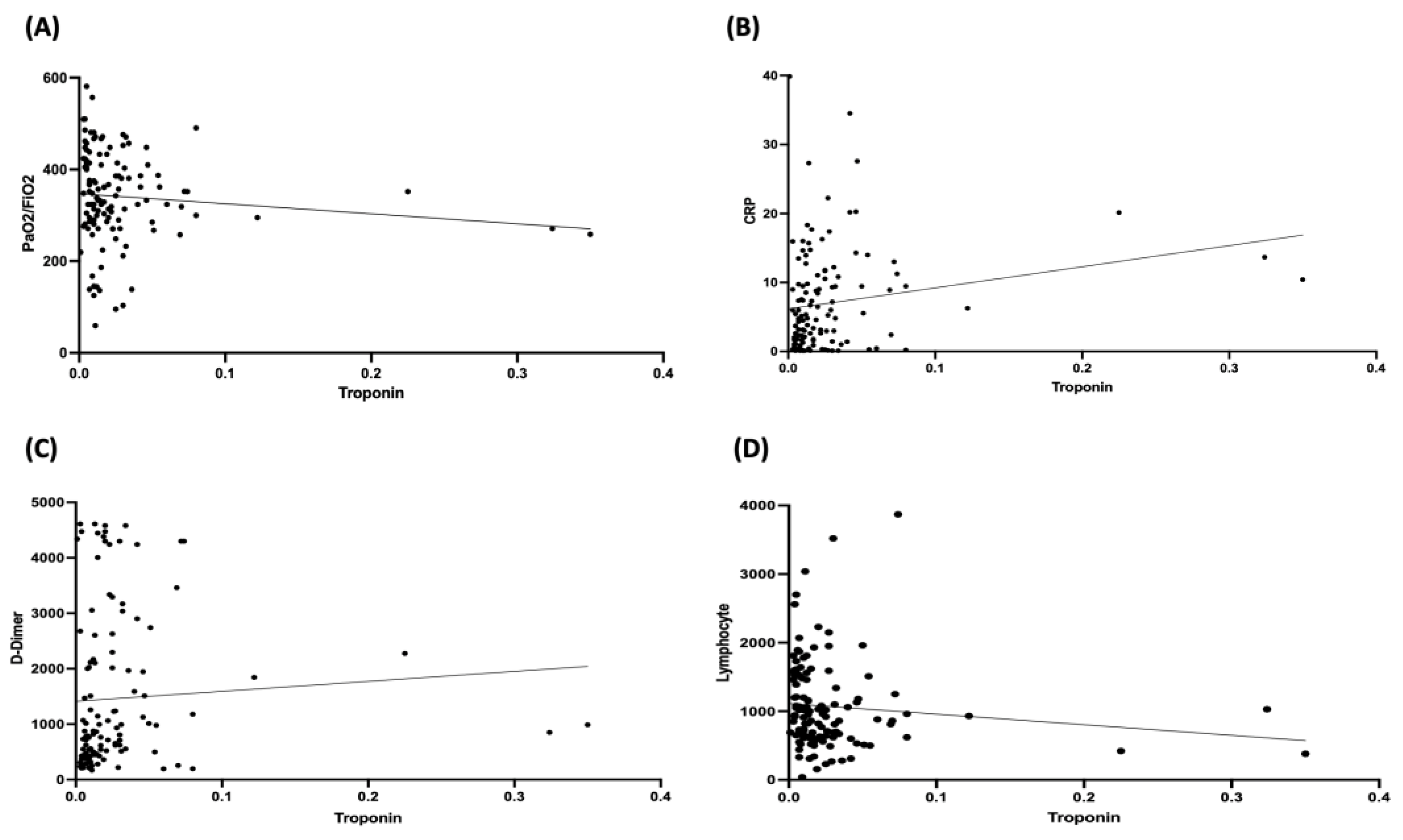
3.7. Troponin Levels and Correlation Analyses
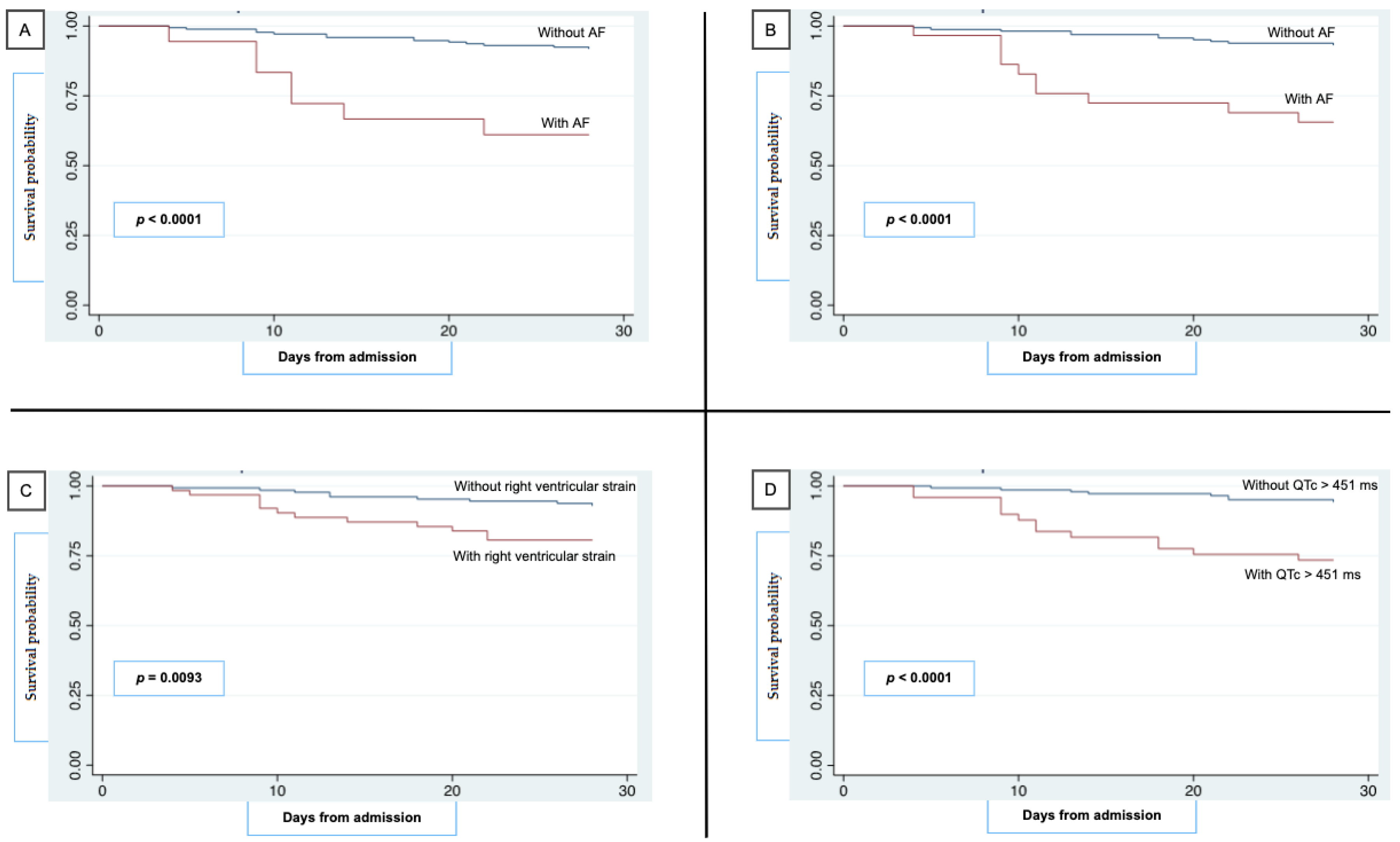
3.8. Kaplan–Meier Survival Curves for 28-Day Mortality
3.9. Multivariate Adjusted Cox Hazard Regression Model of Independent Factors Associated with 28-Day Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Available online: https://coronavirus.jhu.edu/ (accessed on 10 January 2022).
- Izcovich, A.; Ragusa, M.A.; Tortosa, F.; Marzio, M.A.L.; Agnoletti, C.; Bengolea, A.; Ceirano, A.; Espinosa, F.; Saavedra, E.; Sanguine, V.; et al. Prognostic factors for severity and mortality in patients infected with COVID-19: A systematic review. PLoS ONE 2020, 15, e0241955. [Google Scholar] [CrossRef] [PubMed]
- Jalali, F.; Hatami, F.; Saravi, M.; Jafaripour, I.; Hedayati, M.T.; Amin, K.; Pourkia, R.; Abroutan, S.; Javanian, M.; Ebrahimpour, S.; et al. Characteristics and outcomes of hospitalized patients with cardiovascular complications of COVID-19. J. Cardiovasc. Thorac. Res. 2021, 13, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Chammas, J.; Delaney, D.; Chabaytah, N.; Abdulkarim, S.; Schwertani, A. COVID-19 and the cardiovascular system: Insights into effects and treatments. Can. J. Physiol. Pharmacol. 2021, 99, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Bertini, M.; Ferrari, R.; Guardigli, G.; Malagù, M.; Vitali, F.; Zucchetti, O.; D’Aniello, E.; Volta, C.A.; Cimaglia, P.; Piovaccari, G.; et al. Electrocardiographic features of 431 consecutive, critically ill COVID-19 patients: An insight into the mechanisms of cardiac involvement. Europace 2020, 22, 1848–1854. [Google Scholar] [CrossRef]
- Long, B.; Brady, W.J.; Bridwell, R.E.; Ramzy, M.; Montrief, T.; Singh, M.; Gottlieb, M. Electrocardiographic manifestations of COVID-19. Am. J. Emerg. Med. 2021, 41, 96–103. [Google Scholar] [CrossRef]
- Raad, M.; Gorgis, S.; Dabbagh, M.; Chehab, O.; Parikh, S.; Singh, G. Right Heart Strain on Presenting 12-Lead Electrocardiogram Predicts Critical Illness in COVID-19. JACC Clin. Electrophysiol. 2021, 7, 485–493. [Google Scholar] [CrossRef]
- Ye, F.; Hatahet, M.; Youniss, M.A.; Toklu, H.Z.; Mazza, J.J.; Yale, S. The Clinical Significance of Relative Bradycardia. WMJ 2018, 117, 73–78. [Google Scholar]
- Oliva, A.; Franchi, C.; Gatto, M.C.; Galardo, G.; Pugliese, F.; Mastroianni, C. Prevalence and clinical significance of relative bradycardia at hospital admission in patients with coronavirus disease 2019 (COVID-19). Clin. Microbiol. Infect. 2021, 27, 1185–1187. [Google Scholar] [CrossRef]
- Bazett, H. An analysis of the time-relations of electrocardiograms. Heart 1920, 7, 353–370. [Google Scholar] [CrossRef]
- Rautaharju, P.M.; Zhang, Z.M.; Prineas, R.; Heiss, G. Assessment of prolonged QT and JT intervals in ventricular conduction defects. Am. J. Cardiol. 2004, 93, 1017–1021. [Google Scholar] [CrossRef]
- Day, C.P.; McComb, J.M.; Campbell, R.W. QT dispersion: An indication of arrhythmia risk in patients with long QT intervals. Br. Heart J. 1990, 63, 342–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yenerçağ, M.; Arslan, U.; Doğduş, M.; Günal, Ö.; Öztürk, Ç.E.; Aksan, G.; Erdoğan, G.; Gül, S.; Yontar, O.C.; Şen, A. Evaluation of electrocardiographic ventricular repolarization variables in patients with newly diagnosed COVID-19. J. Electrocardiol. 2020, 62, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://coronavirus.jhu.edu/data/mortality (accessed on 12 January 2022).
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- Bilinski, A.; Emanuel, E.J. COVID-19 and Excess All-Cause Mortality in the US and 18 Comparison Countries. JAMA 2020, 324, 2100–2102. [Google Scholar] [CrossRef] [PubMed]
- Hall, W.H.; Ramachandran, R.; Narayan, S.; Jani, A.B.; Vijayakumar, S. An electronic application for rapidly calculating Charlson comorbidity score. BMC Cancer 2004, 4, 94. [Google Scholar] [CrossRef] [Green Version]
- Zuin, M.; Rigatelli, G.; Zuliani, G.; Rigatelli, A.; Mazza, A.; Roncon, L. Arterial hypertension and risk of death in patients with COVID-19 infection: Systematic review and metaanalysis. J. Infect. 2020, 81, e84–e86. [Google Scholar] [CrossRef]
- Yarmohammadi, H.; Morrow, J.P.; Dizon, J.; Biviano, A.; Ehlert, F.; Saluja, D.; Waase, M.; Elias, P.; Poterucha, T.J.; Berman, J.; et al. Frequency of Atrial Arrhythmia in Hospitalized Patients With COVID-19. Am. J. Cardiol. 2021, 147, 52–57. [Google Scholar] [CrossRef]
- Romiti, G.F.; Corica, B.; Lip, G.Y.H.; Proietti, M. Prevalence and Impact of Atrial Fibrillation in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2490. [Google Scholar] [CrossRef]
- Zoni-Berisso, M.; Lercari, F.; Carazza, T.; Domenicucci, S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 2014, 6, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Chorin, E.; Wadhwani, L.; Magnani, S.; Dai, M.; Shulman, E.; Nadeau-Routhier, C.; Knotts, R.; Bar-Cohen, R.; Kogan, E.; Barbhaiya, C.; et al. QT interval prolongation and torsade de pointes in patients with COVID-19 treated with hydroxychloroquine/azithromycin. Heart Rhythm 2020, 17, 1425–1433. [Google Scholar] [CrossRef]
- Shopp, J.D.; Stewart, L.K.; Emmett, T.W.; Kline, J.A. Findings From 12-lead Electrocardiography That Predict Circulatory Shock From Pulmonary Embolism: Systematic Review and Meta-analysis. Acad. Emerg. Med. 2015, 22, 1127–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanni, S.; Polidori, G.; Vergara, R.; Pepe, G.; Nazerian, P.; Moroni, F.; Garbelli, E.; Daviddi, F.; Grifoni, S. Prognostic value of ECG among patients with acute pulmonary embolism and normal blood pressure. Am. J. Med. 2009, 122, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Elias, P.; Poterucha, T.J.; Jain, S.S.; Sayer, G.; Raikhelkar, J.; Fried, J.; Clerkin, K.; Griffin, J.; DeFilippis, E.M.; Gupta, A.; et al. The Prognostic Value of Electrocardiogram at Presentation to Emergency Department in Patients With COVID-19. Mayo Clin. Proc. 2020, 95, 2099–2109. [Google Scholar] [CrossRef] [PubMed]
- Marin, B.G.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Malik, P.; Patel, U.; Mehta, D.; Patel, N.; Kelkar, R.; Akrmah, M.; Gabrilove, J.L.; Sacks, H. Biomarkers and outcomes of COVID-19 hospitalisations: Systematic review and meta-analysis. BMJ Evid. Based Med. 2021, 26, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Polak, S.B.; Van Gool, I.C.; Cohen, D.; von der Thüsen, J.H.; van Paassen, J. A systematic review of pathological findings in COVID-19: A pathophysiological timeline and possible mechanisms of disease progression. Mod. Pathol. 2020, 33, 2128–2138. [Google Scholar] [CrossRef]
- Kumar, S.; Arcuri, C.; Chaudhuri, S.; Gupta, R.; Ms, M.A.; Barve, P.; Shah, S. A novel study on SARS-CoV-2 virus associated bradycardia as a predictor of mortality-retrospective multicenter analysis. Clin. Cardiol. 2021, 44, 857–862. [Google Scholar] [CrossRef]
- Bistrovic, P.; Manola, S.; Lucijanic, M. Bradycardia during remdesivir treatment might be associated with improved survival in patients with COVID-19: A retrospective cohort study on 473 patients from a tertiary centre. Postgrad. Med. J. 2021; ahead of print. [Google Scholar] [CrossRef]
- Pallotto, C.; Suardi, L.R.; Gabbuti, A.; Esperti, S.; Mecocci, L.; Blanc, P. Potential remdesivir-related transient bradycardia in patients with coronavirus disease 2019 (COVID-19). J. Med. Virol. 2021, 93, 2631–2634. [Google Scholar] [CrossRef]
- Fujii, T.; Mashimo, M.; Moriwaki, Y.; Misawa, H.; Ono, S.; Horiguchi, K.; Kawashima, K. Expression and Function of the Cholinergic System in Immune Cells. Front. Immunol. 2017, 8, 1085. [Google Scholar] [CrossRef] [Green Version]
- Gatto, M.C.; Persi, A.; Tung, M.; Masi, R.; Canitano, S.; Kol, A. Bradyarrhythmias in patients with SARS-CoV-2 infection: A narrative review and a clinical report. Pacing. Clin. Electrophysiol. 2021, 44, 1607–1615. [Google Scholar] [CrossRef]
- Hasty, F.; García, G.; Dávila, C.H.; Wittels, S.H.; Hendricks, S.; Chong, S. Heart Rate Variability as a Possible Predictive Marker for Acute Inflammatory Response in COVID-19 Patients. Mil. Med. 2020, 186, e34–e38. [Google Scholar] [CrossRef] [PubMed]
- Barizien, N.; Le Guen, M.; Russel, S.; Touche, P.; Huang, F.; Vallée, A. Clinical characterization of dysautonomia in long COVID-19 patients. Sci. Rep. 2021, 11, 14042. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall Population n (%) = 190 (100) | Survivors n (%) = 166 (87.4) | Non-Survivors n (%) = 24 (12.6) | p-Value |
|---|---|---|---|---|
| Demographics and outcome measures | ||||
| Age—median (IQR), years | 66 (55–80) | 64 (54–77) | 83.5 (79–88) | <0.0001 |
| Females—n (%) | 83 (44) | 72 (43) | 11 (46) | 0.820 |
| First wave—n (%) | 99 (52.1) | 89 (53.6) | 10 (41.7) | 0.273 |
| ICU stay—n (%) | 12 (6.4) | 10 (6) | 2 (8.3) | 0.676 |
| Length of stay—median (IQR), days | 18 (11–28) | 19 (12–28) | 13 (9–22) | 0.160 |
| Global deaths—n (%) | 24 (12.6) | N.A. | 24 (100) | N.A. |
| Within 48 h—n (%) | 0 (0) | 0 (0) | ||
| Within 7 days—n (%) | 4 (2.1) | 4 (16.7) | ||
| Within 14 days—n (%) | 14 (7.4) | 14 (58.3) | ||
| Within 28 days—n (%) | 21 (11) | 21 (87.5) | ||
| >28 days | 3 (1.7) | 3 (12.5) | ||
| Comorbidities | ||||
| CCI—median (IQR) | 4 (2–7) | 3 (1–6) | 8 (8–10) | <0.0001 |
| Stage III–IV CKD—n (%) | 60 (31.6) | 49 (29.5) | 11 (45.8) | 0.156 |
| Diabetes mellitus (I and II)—n (%) | 38 (20) | 35 (21) | 3 (12.5) | 0.412 |
| Periph. vascular disease—n (%) | 34 (18) | 25 (15) | 9 (37.5) | 0.005 |
| COPD—n (%) | 28 (14.9) | 23 (13.8) | 5 (20.8) | 0.325 |
| Myocardial infarction—n (%) | 27 (14.2) | 21 (13) | 6 (25) | 0.084 |
| Dementia—n (%) | 27 (14.3) | 11 (6.6) | 16 (66.7) | <0.0001 |
| Solid tumor—n (%) | 21 (11) | 14 (8.4) | 7 (29.2) | 0.015 |
| CVA/TIA—n (%) | 18 (9.5) | 9 (5.4) | 9 (37.5) | <0.0001 |
| Chronic heart failure—n (%) | 12 (6.3) | 9 (5.4) | 3 (12.5) | 0.160 |
| Hemiplegia—n (%) | 8 (4.2) | 3 (1.8) | 5 (20.8) | <0.0001 |
| Liver disease—n (%) | 7 (3.7) | 3 (1.8) | 4 (16.6) | <0.0001 |
| Hematologic malignancies—n (%) | 5 (2.6) | 1 (0.5) | 4 (16.7) | 0.001 |
| AIDS—n (%) | ||||
| Systemic hypertension—n (%) | 109 (57.3) | 95 (57.2) | 14 (58.3) | 0.741 |
| Atrial fibrillation *—n (%) | 20 (10.5) | 13 (7.8) | 7 (29.1) | <0.0001 |
| Asthma—n (%) | 10 (5.3) | 8 (4.8) | 2 (8.3) | 0.436 |
| Clinical and laboratory findings at E.D. | ||||
| Days from symptoms onset—median (IQR), days | 5.9 (2–9) | 6 (2–9) | 1.8 (0–5.5) | 0.039 |
| Vital signs | ||||
| BT—median (IQR), °C | 37 (36.2–37.95) | 37 (36.5–38) | 36.5 (36–37.45) | 0.252 |
| SpO2—median (IQR), % | 96 (94–98) | 96 (94–98) | 96 (93–97) | 0.356 |
| HR—median (IQR), bpm | 87 (80–100) | 86.5 (80–98) | 90 (79–110) | 0.191 |
| PaO2/FiO2—median (IQR), n | 352 (295–419) | 357 (314–424) | 302 (243–367) | 0.0007 |
| Relative bradycardia **—n (%) | 22 (11.6) | 21 (12.6) | 1 (4.1) | 0.225 |
| Reported symptoms | 37 (36.2–37.95) | 37 (36.5–38) | 36.5 (36–37.45) | 0.252 |
| Fever—n (%) | 149 (78.4) | 136 (82) | 13 (54.2) | 0.002 |
| Dyspnea—n (%) | 101 (53.1) | 85 (51.2) | 16 (66.7) | 0.164 |
| Cough—n (%) | 89 (46.8) | 84 (50.6) | 5 (20.8) | 0.009 |
| Weakness/osteoarticular—n (%) | 37 (19.6) | 29 (17.5) | 8 (33.3) | 0.069 |
| Gastrointestinal—n (%) | 25 (13.2) | 23 (13.8) | 2 (8.3) | 0.449 |
| Anosmia/dysgeusia—n (%) | 17 (8,9) | 16 (9.6) | 1 (4.1) | 0.380 |
| Laboratory tests | ||||
| Hb—median (IQR), g/dL | 13.8 (12.4–14.9) | 13.8 (12.7–14.9) | 11.3 (10.2–14.5) | 0.0004 |
| WBC—median (IQR), /μL | 5835 (4625–8220) | 5755 (4502–7790) | 7180 (5070–8820) | 0.009 |
| Neutrophils—median (IQR), /μL | 4310 (3160–6335) | 4150 (3110–5995) | 5465 (3647–7662) | 0.0038 |
| Lymphocytes—median (IQR), /μL | 895 (635–1285) | 920 (650–1367) | 795 (527–1120) | 0.130 |
| Serum albumin—median (IQR), g/L | 37 (34–40) | 38 (35–41) | 32 (30–35) | <0.0001 |
| LDH—median (IQR), UI/L | 280 (217–356) | 275 (213–349) | 330 (268–447) | 0.0001 |
| Serum TnT–median (IQR), μg/L § | 0.014 (0.007–0.028) | 0.012 (0.007–0.024) | 0.031 (0.021–0.04) | 0.084 |
| D-dimer—median (IQR), ng/mL | 822 (449–1947) | 777 (429–1469) | 1995 (1012–3198) | 0.0012 |
| CRP—median (IQR), mg/dL | ||||
| Serum creatinine—median (IQR), mg/dL | 3.93 (1.1–9.46) | 3.51 (0.95–9) | 7.57 (3.81–12.64) | 0.669 |
| Anti-SARS-CoV-2 therapies | ||||
| Remdesivir—n (%) | 35 (18.4) | 34 (20.5) | 1 (4.1) | 0.054 |
| Therapeutic dose LMWH—n (%) | 43 (22.6) | 33 (19.9) | 10 (41.7) | 0.0045 |
| VTE prophylaxis LMWH—n (%) | 92 (48.4) | 80 (48.2) | 12 (50) | 0.132 |
| Systemic steroids—n (%) | 89 (47.6) | 72 (43.4) | 17 (70.8) | 0.045 |
| Anti-IL6—n (%) | 36 (19.2) | 29 (17.5) | 7 (29.2) | 0.217 |
| Anti-JAK—n (%) | 1 (0.5) | 1 (0.6) | 0 (0) | N.A. |
| PI—n (%) | 32 (16.8) | 30 (18) | 2 (8.3) | 0.229 |
| Macrolides—n (%) | 105 (55.3) | 92 (55.4) | 13 (54.2) | 0.537 |
| HCQ—n (%) | 82 (43.4) | 74 (44.6) | 8 (33.3) | 0.288 |
| ECG Feature | Recordings n (%) = 190 (100) | Survivors n (%) = 166 (87.4) | Non-Survivors n (%) = 24 (12.6) | p-Value |
|---|---|---|---|---|
| Heart rhythm | ||||
| Sinus rhythm—n (%) | 172 (90.5) | 156 (94) | 16 (66.7) | <0.0001 |
| Atrial fibrillation—n (%) | 18 (10) | 10 (6) | 8 (33.3) | <0.0001 |
| Other arrhythmias *—n (%) | 18 (9.5) | 13 (7.8) | 5 (20.8) | 0.057 |
| Heart rate and cycle | ||||
| RR interval—median (IQR), ms | 752.5 (637.5–840) | 767 (664–875) | 637.5 (570–762) | 0.006 |
| RR interval SD—median (IQR), ms | 21.2 (14.1–35.3) | 20 (13.4–35) | 18 (11–30) | 0.414 |
| HR—median (IQR), bpm | 79.7 (71.4–94.1) | 81 (73–90) | 94 (79–105) | 0.015 |
| Ventricular conduction | ||||
| AVB—n (%) | 20 (10.6) | 15 (9) | 5 (20.8) | 0.081 |
| QRS duration—median (IQR), ms | 90 (84–102) | 89 (83–101) | 95 (90–110) | 0.119 |
| LAH—n (%) | 42 (22.2) | 28 (19.8) | 9 (37.5) | 0.0258 |
| LPH—n (%) | 2 (1) | 2 (1.2) | 0 (0) | 1 |
| RBBB—n (%) | 22 (11.6) | 18 (10.8) | 4 (16.7) | 0.407 |
| LBBB—n (%) | 6 (3.2) | 4 (2.4) | 2 (8.3) | 0.122 |
| Right ventricular strain | ||||
| S1Q3T3 sign—n (%) | 25 (13.2) | 18 (10.8) | 7 (29.1) | 0.013 |
| S1—n (%) | 39 (20) | 30 (18) | 9 (37.5) | 0.034 |
| Q3—n (%) | 39 (20) | 33 (19.9) | 6 (25) | 0.562 |
| T3—n (%) | 60 (31.6) | 45 (27.1) | 15 (62.5) | <0.0001 |
| Ventricular repolarization | ||||
| QTc duration—median (IQR), ms | 432.5 (412.2–452) | 428 (402–447) | 436.8 (435–487) | 0.0002 |
| QT maximum value, median (IQR), ms | 390 (320–480) | 390 (360–410) | 380 (357.5–412.5) | 0.987 |
| QT minimum value, median (IQR), ms | 370 (340–400) | 378 (350–396.5) | 360 (337.5–400) | 0.776 |
| QT dispersion, median (IQR), ms | 10 (10–20) | 10 (10–20) | 10 (10–20) | 0.397 |
| Prolonged QTc **—n (%) | 55 (28.9) | 39 (23.49) | 16 (66.6) | <0.0001 |
| Tp-e dispersion—median (IQR), ms | 20 (20–30) | 19 (19–27) | 20 (20–30) | 0.458 |
| Tp-e/QT—median (IQR) | 0.234 (0.214–0.253) | 0.236 (0.212–0.256) | 0.2 (0.209–0.238) | 0.126 |
| Tp-e/QTc—median (IQR) | 0.206 (0.182–0.218) | 0.22 (0.211–0.223) | 0.2 (0.158–0.198) | 0.0003 |
| Cardiovascular Events Registered during Hospitalization | Overall Population n (%) = 190 (100) | Survivors n (%) = 166 (87.4) | Non-Survivors n (%) = 24 (12.6) | p-Value |
|---|---|---|---|---|
| Daytime bradycardia—n (%) | 30 (15.8) | 28 (16.9) | 2 (8.3) | 0.284 |
| AF—n (%) | 11 (5.7) | 8 (4.8) | 3 (12.5) | 0.1477 |
| Overall AF (E.D. + in-hospital)—n (%) | 29 (15.3) | 18 (10.8) | 11 (45.8) | <0.0001 |
| PVC—n (%) | 6 (3.2) | 5 (3) | 1 (4.2) | 0.98 |
| PSVC—n (%) | 7 (3.7) | 5 (3) | 2 (8.3) | 0.32 |
| Simultaneous PVC and PSVC—n (%) | 2 (1) | 2 (1.2) | 0 (0) | N.A. |
| Myopericarditis—n (%) | 2 (1) | 2 (1.2) | 0 (0) | N.A. |
| Others §—n (%) | 4 (2) | 4 (2.4) | 0 (0) | N.A. |
| Multivariate Adjusted Cox Hazard Regression Model for 28-Day Mortality | Adjusted Hazard Ratio (aHR) * | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Age (>65 years) | 6.38 | 1.10–37.01 | 0.039 |
| Male Sex | 2.26 | 0.87–5.88 | 0.093 |
| D-dimer (>850 U/L) | 2.07 | 0.60–7.12 | 0.244 |
| AF ** | 3.02 | 1.03–8.81 | 0.042 |
| Right ventricular strain | 2.94 | 1.01–8.55 | 0.047 |
| QTc interval (>451 ms) | 3.24 | 1.09–9.62 | 0.033 |
| Tp-e/QTc (>0.20) | 0.79 | 0.28–2.20 | 0.662 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savelloni, G.; Gatto, M.C.; Cancelli, F.; Barbetti, A.; Cogliati Dezza, F.; Franchi, C.; Carnevalini, M.; Galardo, G.; Bucci, T.; Alessandroni, M.; et al. Prognostic Value of 12-Leads Electrocardiogram at Emergency Department in Hospitalized Patients with Coronavirus Disease-19. J. Clin. Med. 2022, 11, 2537. https://doi.org/10.3390/jcm11092537
Savelloni G, Gatto MC, Cancelli F, Barbetti A, Cogliati Dezza F, Franchi C, Carnevalini M, Galardo G, Bucci T, Alessandroni M, et al. Prognostic Value of 12-Leads Electrocardiogram at Emergency Department in Hospitalized Patients with Coronavirus Disease-19. Journal of Clinical Medicine. 2022; 11(9):2537. https://doi.org/10.3390/jcm11092537
Chicago/Turabian StyleSavelloni, Giulia, Maria Chiara Gatto, Francesca Cancelli, Anna Barbetti, Francesco Cogliati Dezza, Cristiana Franchi, Martina Carnevalini, Gioacchino Galardo, Tommaso Bucci, Maria Alessandroni, and et al. 2022. "Prognostic Value of 12-Leads Electrocardiogram at Emergency Department in Hospitalized Patients with Coronavirus Disease-19" Journal of Clinical Medicine 11, no. 9: 2537. https://doi.org/10.3390/jcm11092537