
High Levels of Sedentary Time in Patients with COVID-19 after Hospitalisation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
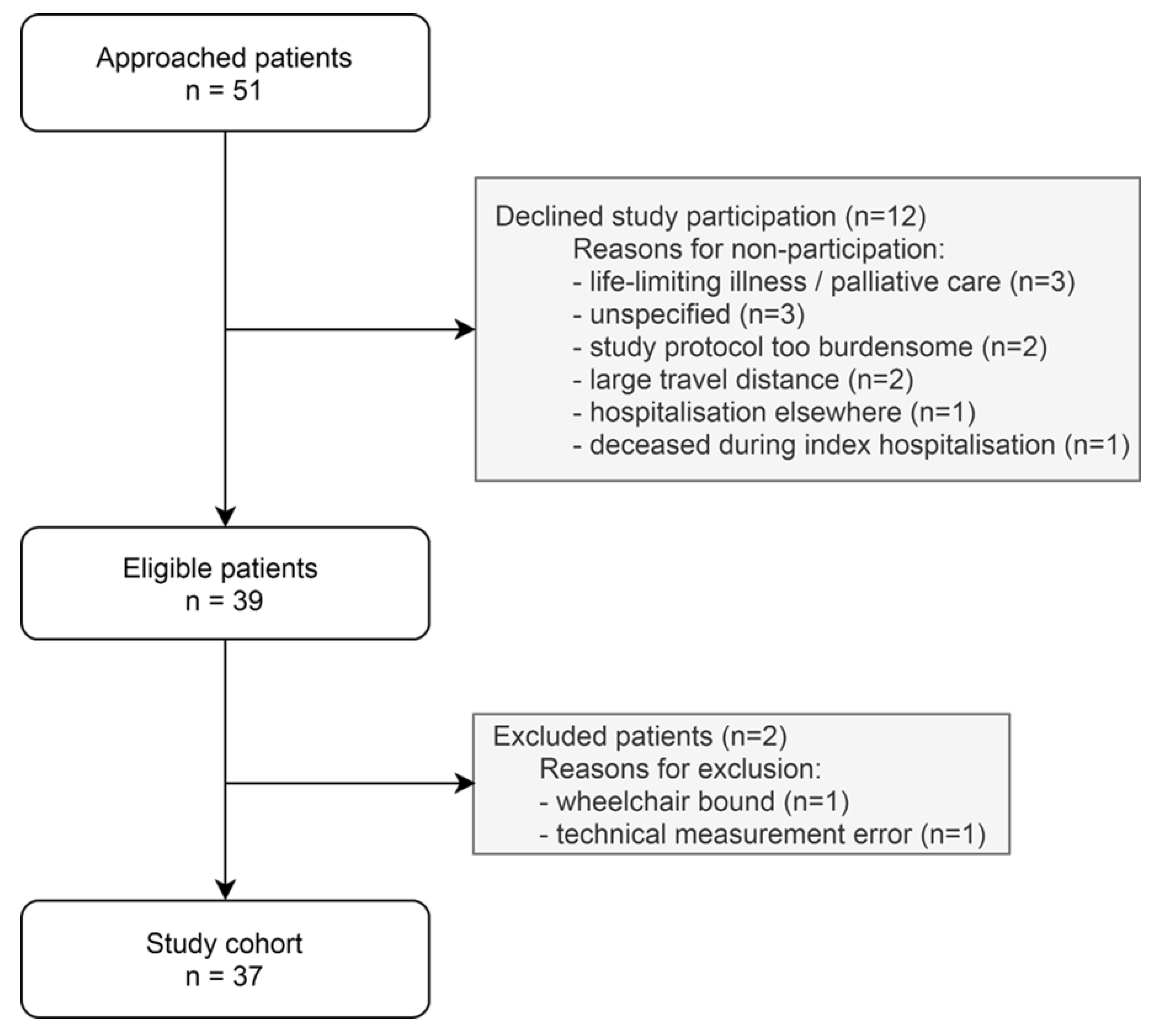
2.1. Population
2.2. Measurements
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Physical Activity and Sedentary Behaviour
3.3. Physical Activity Patterns across Subgroups
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mahajan, S.; Caraballo, C.; Li, S.X.; Dong, Y.; Chen, L.; Huston, S.K.; Srinivasan, R.; Redlich, C.A.; Ko, A.I.; Faust, J.S.; et al. SARS-CoV-2 Infection Hospitalization Rate and Infection Fatality Rate Among the Non-Congregate Population in Connecticut. Am. J. Med. 2021, 134, 812–816.e2. [Google Scholar] [CrossRef]
- del Rio, C.; Collins, L.F.; Malani, P. Long-term Health Consequences of COVID-19. JAMA 2020, 324, 1723–1724. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F.; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef]
- Heesakkers, H.; van der Hoeven, J.G.; Corsten, S.; Janssen, I.; Ewalds, E.; Simons, K.S.; Westerhof, B.; Rettig, T.C.D.; Jacobs, C.; van Santen, S.; et al. Clinical Outcomes among Patients With 1-Year Survival Following Intensive Care Unit Treatment for COVID-19. JAMA 2022, 327, 559–565. [Google Scholar] [CrossRef]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M.; Lancet Physical Activity Series 2 Executive, C.; Lancet Sedentary Behaviour Working, G. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef]
- Sallis, R.; Young, D.R.; Tartof, S.Y.; Sallis, J.F.; Sall, J.; Li, Q.; Smith, G.N.; Cohen, D.A. Physical inactivity is associated with a higher risk for severe COVID-19 outcomes: A study in 48 440 adult patients. Br. J. Sports Med. 2021, 55, 1099–1105. [Google Scholar] [CrossRef]
- Woods, J.A.; Hutchinson, N.T.; Powers, S.K.; Roberts, W.O.; Gomez-Cabrera, M.C.; Radak, Z.; Berkes, I.; Boros, A.; Boldogh, I.; Leeuwenburgh, C.; et al. The COVID-19 pandemic and physical activity. Sports Med. Health Sci. 2020, 2, 55–64. [Google Scholar] [CrossRef]
- Beauchamp, M.K.; Joshi, D.; McMillan, J.; Erbas Oz, U.; Griffith, L.E.; Basta, N.E.; Kirkland, S.; Wolfson, C.; Raina, P.; Canadian Longitudinal Study on Aging (CLSA) Team. Assessment of Functional Mobility After COVID-19 in Adults Aged 50 Years or Older in the Canadian Longitudinal Study on Aging. JAMA Network Open 2022, 5, e2146168. [Google Scholar] [CrossRef] [PubMed]
- van den Borst, B.; Peters, J.B.; Brink, M.; Schoon, Y.; Bleeker-Rovers, C.P.; Schers, H.; van Hees, H.W.H.; van Helvoort, H.; van den Boogaard, M.; van der Hoeven, H.; et al. Comprehensive Health Assessment 3 Months After Recovery From Acute Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2021, 73, e1089–e1098. [Google Scholar] [CrossRef]
- Belli, S.; Balbi, B.; Prince, I.; Cattaneo, D.; Masocco, F.; Zaccaria, S.; Bertalli, L.; Cattini, F.; Lomazzo, A.; Dal Negro, F.; et al. Low physical functioning and impaired performance of activities of daily life in COVID-19 patients who survived hospitalisation. Eur. Respir. J. 2020, 56, 2002096. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel, F.M.A.; Vos, J.L.; Koop, Y.; van Dijk, A.P.J.; Duijnhouwer, A.L.; de Mast, Q.; van de Veerdonk, F.L.; Bosch, F.; Kok, B.; Netea, M.G.; et al. Cardiac function in relation to myocardial injury in hospitalised patients with COVID-19. Neth. Heart J. 2020, 28, 410–417. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel, F.M.A.; Vos, J.L.; van Bakel, B.; Duijnhouwer, A.L.; van Dijk, A.P.J.; Dimitriu-Leen, A.C.; Koopmans, P.C.; de Mast, Q.; van de Veerdonk, F.L.; Bosch, F.H.; et al. Comparison between myocardial function assessed by echocardiography during hospitalization for COVID-19 and at 4 months follow-up. Int. J. Cardiovasc. Imaging 2021, 37, 3459–3467. [Google Scholar] [CrossRef] [PubMed]
- Edwardson, C.L.; Winkler, E.A.H.; Bodicoat, D.H.; Yates, T.; Davies, M.J.; Dunstan, D.W.; Healy, G.N. Considerations when using the activPAL monitor in field-based research with adult populations. J. Sport Health Sci. 2017, 6, 162–178. [Google Scholar] [CrossRef] [Green Version]
- Edwardson, C.L.; Rowlands, A.V.; Bunnewell, S.; Sanders, J.; Esliger, D.W.; Gorely, T.; O’Connell, S.; Davies, M.J.; Khunti, K.; Yates, T. Accuracy of Posture Allocation Algorithms for Thigh- and Waist-Worn Accelerometers. Med. Sci. Sports Exerc. 2016, 48, 1085–1090. [Google Scholar] [CrossRef] [Green Version]
- Winkler, E.A.; Bodicoat, D.H.; Healy, G.N.; Bakrania, K.; Yates, T.; Owen, N.; Dunstan, D.W.; Edwardson, C.L. Identifying adults’ valid waking wear time by automated estimation in activPAL data collected with a 24 h wear protocol. Physiol. Meas. 2016, 37, 1653–1668. [Google Scholar] [CrossRef] [Green Version]
- Lyden, K.; Keadle, S.K.; Staudenmayer, J.; Freedson, P.S. The activPALTM Accurately Classifies Activity Intensity Categories in Healthy Adults. Med. Sci. Sports Exerc. 2017, 49, 1022–1028. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [Green Version]
- Bakker, E.A.; van Bakel, B.M.A.; Aengevaeren, W.R.M.; Meindersma, E.P.; Snoek, J.A.; Waskowsky, W.M.; van Kuijk, A.A.; Jacobs, M.M.L.M.; Hopman, M.T.E.; Thijssen, D.H.J.; et al. Sedentary behaviour in cardiovascular disease patients: Risk group identification and the impact of cardiac rehabilitation. Int. J. Cardiol. 2021, 326, 194–201. [Google Scholar] [CrossRef]
- Prince, S.A.; Roberts, K.C.; Melvin, A.; Butler, G.P.; Thompson, W. Gender and education differences in sedentary behaviour in Canada: An analysis of national cross-sectional surveys. BMC Public Health 2020, 20, 1170. [Google Scholar] [CrossRef] [PubMed]
- van Bakel, B.M.A.; Bakker, E.A.; de Vries, F.; Thijssen, D.H.J.; Eijsvogels, T.M.H. Impact of COVID-19 lockdown on physical activity and sedentary behaviour in Dutch cardiovascular disease patients. Neth. Heart J. 2021, 29, 273–279. [Google Scholar] [CrossRef] [PubMed]
- van Bakel, B.M.A.; Bakker, E.A.; de Vries, F.; Thijssen, D.H.J.; Eijsvogels, T.M.H. Changes in Physical Activity and Sedentary Behaviour in Cardiovascular Disease Patients during the COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 11929. [Google Scholar] [CrossRef] [PubMed]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.N.; Eggelbusch, M.; Naddaf, E.; Gerrits, K.H.L.; van der Schaaf, M.; van den Borst, B.; Wiersinga, W.J.; van Vugt, M.; Weijs, P.J.M.; Murray, A.J.; et al. Skeletal muscle alterations in patients with acute COVID-19 and post-acute sequelae of COVID-19. J. Cachexia Sarcopenia Muscle 2022, 13, 11–22. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Patrucco, F.; Zeppegno, P.; Baricich, A.; Gramaglia, C.M.; Balbo, P.E.; Falaschi, Z.; Carriero, A.; Cuneo, D.; Pirisi, M.; Bellan, M. Long-lasting consequences of Coronavirus disease 19 pneumonia: A systematic review. Minerva Med. 2021; Online ahead of print. [Google Scholar] [CrossRef]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022; Online ahead of print. [Google Scholar] [CrossRef]
- Dogra, S.; Copeland, J.L.; Altenburg, T.M.; Heyland, D.K.; Owen, N.; Dunstan, D.W. Start with reducing sedentary behavior: A stepwise approach to physical activity counseling in clinical practice. Patient Educ. Couns. 2021; in press. [Google Scholar] [CrossRef]
- Jensen, M.T.; Treskes, R.W.; Caiani, E.G.; Casado-Arroyo, R.; Cowie, M.R.; Dilaveris, P.; Duncker, D.; Di Rienzo, M.; Frederix, I.; De Groot, N.; et al. ESC working group on e-cardiology position paper: Use of commercially available wearable technology for heart rate and activity tracking in primary and secondary cardiovascular prevention—in collaboration with the European Heart Rhythm Association, European Association of Preventive Cardiology, Association of Cardiovascular Nursing and Allied Professionals, Patient Forum, and the Digital Health Committee. Eur. Heart J. Digit. Health 2021, 2, 49–59. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristics | n = 37 | Missing Values |
|---|---|---|
| Age (years) | 60 (±10) | 0 (0%) |
| Sex (male) | 29 (78%) | 0 (0%) |
| Body mass index (kg/m2) | 26.8 [23.5, 29.6] | 0 (0%) |
| Smoking | 2 (2%) | 0 (0%) |
| Comorbidities | 0 (0%) | |
| Hypertension | 15 (41%) | |
| Diabetes mellitus | 6 (16%) | |
| Myocardial infarction | 5 (14%) | |
| Heart failure | 0 (0%) | |
| Cerebrovascular disease | 1 (3%) | |
| Chronic renal failure (eGFR < 30 mL/min/1.73 m2 or dialysis) | 1 (3%) | |
| Chronic respiratory disease (COPD or asthma) | 5 (14%) | |
| COVID-19 hospitalisation | ||
| Laboratory findings at admission | ||
| Haemoglobin (mmol/L) | 8.4 [7.8, 9.1] | 0 (0%) |
| Leucocytes (109/L) | 6.9 [5.0, 9.9] | 0 (0%) |
| C-reactive protein (mg/L) | 85.0 [44.5, 179.0] | 0 (0%) |
| Procalcitonin (µg/L) | 0.20 [0.08, 1.08] | 13 (35%) |
| eGFR (ml/min/1.73 m2) | 79 [65, 90] | 0 (0%) |
| Lactate (mmol/L) | 1.3 [1.2, 1.7] | 14 (38%) |
| pH | 7.47 (±0.05) | 6 (16%) |
| Cardiac biomarker release during hospitalisation | ||
| hs-cTnT (ng/L) | 13 [8, 21] | 3 (8%) |
| hs-cTnT > 14 ng/L | 16 (43%) | 3 (8%) |
| NT-proBNP (pg/mL) | 330 [77, 680] | 2 (5%) |
| NT-proBNP > 300 pg/mL | 18 (49%) | 2 (5%) |
| Treatment | ||
| Mechanical ventilation | 11 (30%) | 0 (0%) |
| Number of days | 16 (±7) | |
| Prone ventilation | 10 (27%) | |
| Intensive care unit admission | 13 (35%) | 0 (0%) |
| Medium care unit admission | 1 (3%) | 0 (0%) |
| Duration of hospitalisation (days) | 8 [7, 22] | 0 (0%) |
| In-hospital complications | 0 (0%) | |
| Pulmonary embolism | 6 (16%) | |
| Acute kidney failure | 2 (5%) | |
| Acute heart failure | 3 (8%) | |
| Myocardial infarction (type 2) | 1 (3%) | |
| CVA/TIA | 1 (3%) | |
| Ventricular arrhythmia | 0 (0%) | |
| Atrial fibrillation | 3 (8%) | |
| Myocarditis | 0 (0%) | |
| Follow-up—clinical outcomes | ||
| Days of follow-up after discharge | 194 [185, 203] | 0 (0%) |
| Emergency department visit | 1 (3%) | |
| Hospitalisation | 3 (8%) | |
| Pulmonary embolism | 1 (3%) | |
| Acute heart failure | 0 (0%) | |
| Myocardial infarction | 0 (0%) | |
| Atrial fibrillation | 1 (3%) | |
| Echocardiographic parameters | 0 (0%) | |
| Normal LV and RV volumes and function a | 28 (76%) | |
| Persistent symptoms post-discharge b | 0 (0%) | |
| Dyspnoea | 10 (27%) | |
| Chest pain | 3 (8%) | |
| Peripheral oedema | 7 (19%) | |
| Fatigue | 6 (16%) |
| n (%) | LIPA (h/Day) | MVPA (h/Day) | Sitting (h/Day) | Sleep (h/Day) | |||
|---|---|---|---|---|---|---|---|
| Patient characteristics | |||||||
| Age (years) | ≤62 | 19 (51%) | 4.5 ± 1.6 | 1.2 [0.9; 1.4] | 9.8 ± 1.8 | 8.5 ± 1.1 | |
| >62 | 18 (49%) | 4.2 ±1.3 | 1.0 [0.7; 1.4] | 9.9 ± 1.3 | 8.7 ± 0.7 | ||
| p-value | 0.52 | 0.43 | 0.94 | 0.49 | |||
| Sex | Females | 8 (22%) | 4.5 ± 1.1 | 1.0 [0.8; 1.3] | 9.3 ± 1.0 | 9.2 ± 1.0 | |
| Males | 29 (78%) | 4.3 ± 1.6 | 1.1 [0.8; 1.5] | 10.0 ± 1.6 | 8.5 ± 0.8 | ||
| p-value | 0.73 | 0.70 | 0.22 | 0.03 | |||
| Body mass index (kg/m2) | ≤26.8 | 18 (49%) | 4.7 ± 1.4 | 1.2 [0.8; 1.5] | 9.7 ± 1.5 | 8.5 ± 0.9 | |
| <26.8 | 19 (51%) | 4.1 ± 1.6 | 1.0 [0.7; 1.3] | 10.1 ± 1.6 | 8.8 ± 0.9 | ||
| p-value | 0.25 | 0.27 | 0.45 | 0.35 | |||
| Comorbidity a | Yes | 23 (62%) | 4.5 ± 1.6 | 1.0 [0.8; 1.5] | 9.6 ± 1.5 | 8.8 ± 1.0 | |
| No | 14 (38%) | 4.2 ± 1.4 | 1.2 [0.9; 1.4] | 10.3 ± 1.6 | 8.4 ± 0.6 | ||
| p-value | 0.63 | 0.75 | 0.19 | 0.19 | |||
| Disease characteristics | |||||||
| hs-cTnT (ng/L) | ≤14 | 18 (49%) | 4.1 ± 1.2 | 1.0 [0.7; 1.4] | 10.1 ± 1.1 | 8.7 ± 0.9 | |
| >14 | 16 (43%) | 4.5 ± 1.5 | 1.2 [1.0; 1.4] | 9.7 ± 1.7 | 8.6 ± 1.1 | ||
| p-value | 0.43 | 0.30 | 0.39 | 0.67 | |||
| NT-proBNP (pg/mL) | ≤300 | 17 (46%) | 4.6 ± 1.6 | 1.0 [0.8; 1.2] | 9.5 ± 1.5 | 8.9 ± 1.1 | |
| >300 | 18 (49%) | 4.1 ± 1.3 | 1.2 [0.8; 1.4] | 10.1 ± 1.5 | 8.5 ± 0.6 | ||
| p-value | 0.41 | 0.46 | 0.28 | 0.18 | |||
| Intensive care unit admission | Yes | 13 (35%) | 4.2 ± 1.4 | 1.2 [0.7; 1.3] | 9.9 ± 1.6 | 8.8 ± 1.3 | |
| No | 24 (65%) | 4.5 ± 1.5 | 1.0 [0.8; 1.4] | 9.8 ± 1.5 | 8.5 ± 0.6 | ||
| p-value | 0.58 | 1.0 | 0.83 | 0.45 | |||
| Duration of hospitalisation (days) | ≤8 | 19 (51%) | 4.7 ± 1.6 | 1.0 [0.8; 1.5] | 9.7 ± 1.5 | 8.4 ± 0.7 | |
| ≥8 | 18 (49%) | 4.1 ± 1.3 | 1.2 [0.8; 1.2] | 10.0 ± 1.6 | 8.9 ± 1.1 | ||
| p-value | 0.24 | 0.99 | 0.65 | 0.15 | |||
| Pulmonary embolism | Yes | 6 (16%) | 3.7 ± 1.2 | 1.3 [0.9; 1.6] | 10.5 ± 1.7 | 8.4 ± 1.3 | |
| No | 31 (84%) | 4.5 ± 1.5 | 1.0 [0.8; 1.3] | 9.7 ± 1.5 | 8.7 ± 0.8 | ||
| p-value | 0.24 | 0.27 | 0.26 | 0.60 | |||
| Cardiac dysfunction post-discharge | |||||||
| Normal TTE b | Yes | 28 (76%) | 4.5 ± 1.5 | 1.0 [0.8; 1.3] | 9.8 ± 1.6 | 8.6 ± 1.0 | |
| No | 9 (24%) | 3.9 ± 1.3 | 1.1 [0.8; 1.6] | 10.0 ± 1.3 | 8.7 ± 0.5 | ||
| p-value | 0.25 | 0.57 | 0.73 | 0.75 | |||
| Persistent symptoms post-discharge | |||||||
| Persistent symptoms c | Yes | 16 (43%) | 4.5 ± 1.4 | 1.0 [0.8; 1.2] | 9.4 ± 1.3 | 9.1 ± 1.1 | |
| No | 21 (57%) | 4.3 ± 1.6 | 1.2 [0.8; 1.6] | 10.2 ± 1.7 | 8.3 ± 0.6 | ||
| p-value | 0.64 | 0.16 | 0.15 | 0.02 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Bakel, B.M.A.; van den Heuvel, F.M.A.; Vos, J.L.; Rotbi, H.; Bakker, E.A.; Nijveldt, R.; Thijssen, D.H.J.; Eijsvogels, T.M.H. High Levels of Sedentary Time in Patients with COVID-19 after Hospitalisation. J. Clin. Med. 2022, 11, 1110. https://doi.org/10.3390/jcm11041110
van Bakel BMA, van den Heuvel FMA, Vos JL, Rotbi H, Bakker EA, Nijveldt R, Thijssen DHJ, Eijsvogels TMH. High Levels of Sedentary Time in Patients with COVID-19 after Hospitalisation. Journal of Clinical Medicine. 2022; 11(4):1110. https://doi.org/10.3390/jcm11041110
Chicago/Turabian Stylevan Bakel, Bram M. A., Frederik M. A. van den Heuvel, Jacqueline L. Vos, Hajar Rotbi, Esmée A. Bakker, Robin Nijveldt, Dick H. J. Thijssen, and Thijs M. H. Eijsvogels. 2022. "High Levels of Sedentary Time in Patients with COVID-19 after Hospitalisation" Journal of Clinical Medicine 11, no. 4: 1110. https://doi.org/10.3390/jcm11041110