
Hospital-Acquired Functional Decline and Clinical Outcomes in Older Cardiac Surgical Patients: A Multicenter Prospective Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Progression of Postoperative Rehabilitation
2.2. Clinical Outcomes
2.3. Definition of HAFD
2.4. Clinical Characteristics and Measurements of Physical Function
2.5. One-Year Follow-Up Data
Statistical Analysis
3. Results
3.1. Study Population and Incidence of HAFD
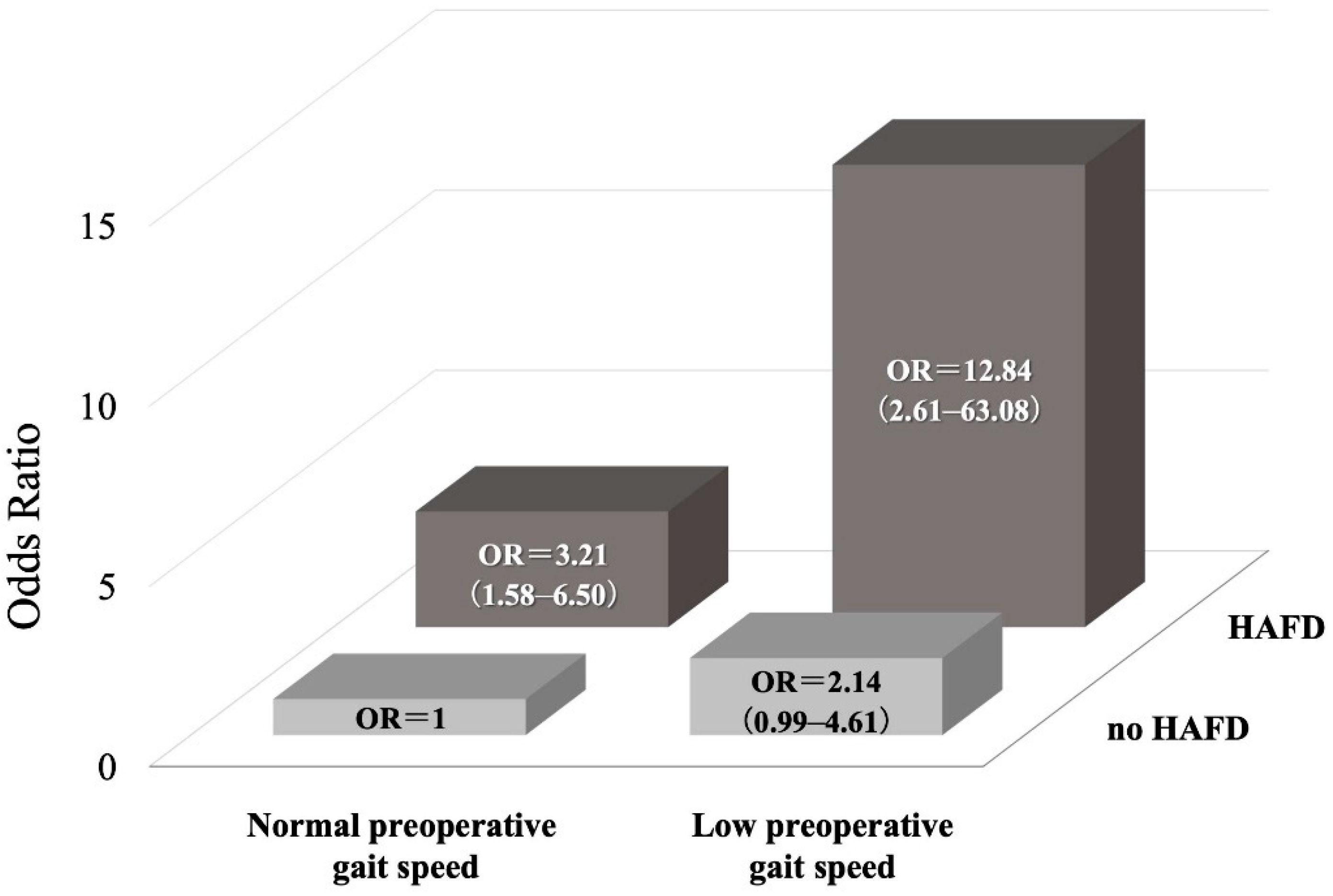
3.2. Association between HAFD and the Primary Outcome
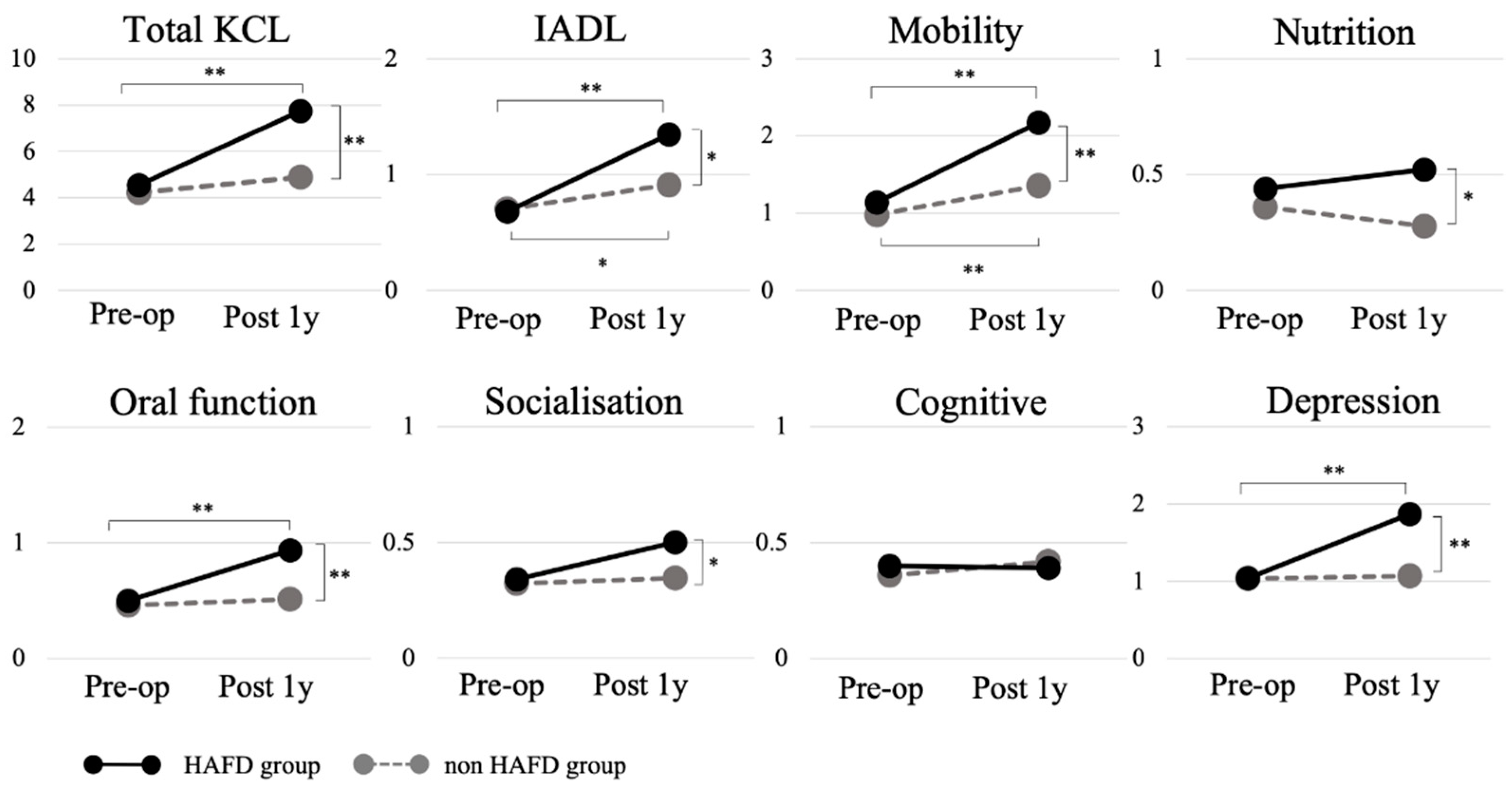
3.3. Changes in the Kihon Checklist Score among the HAFD and Non-HAFD Groups
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Afilalo, J.; Sharma, A.; Zhang, S.; Brennan, J.M.; Edwards, F.H.; Mack, M.J.; McClurken, J.B.; Cleveland, J.C.; Smith, P.K.; Shahian, D.M.; et al. Gait Speed and 1-Year Mortality Following Cardiac Surgery: A Landmark Analysis From the Society of Thoracic Surgeons Adult Cardiac Surgery Database. J. Am. Heart Assoc. 2018, 7, e010139. [Google Scholar] [CrossRef] [Green Version]
- Afilalo, J.; Eisenberg, M.J.; Morin, J.F.; Bergman, H.; Monette, J.; Noiseux, N.; Perrault, L.P.; Alexander, K.P.; Langlois, Y.; Dendukuri, N.; et al. Gait Speed as an Incremental Predictor of Mortality and Major Morbidity in Elderly Patients Undergoing Cardiac Surgery. J. Am. Coll. Cardiol. 2010, 56, 1668–1676. [Google Scholar] [CrossRef] [Green Version]
- Afilalo, J.; Kim, S.; O’Brien, S.; Brennan, J.M.; Edwards, F.H.; Mack, M.J.; McClurken, J.B.; Cleveland, J.C.; Smith, P.K.; Shahian, D.M.; et al. Gait Speed and Operative Mortality in Older Adults Following Cardiac Surgery. JAMA Cardiol. 2016, 1, 314–321. [Google Scholar] [CrossRef] [Green Version]
- Yanagawa, B.; Graham, M.M.; Afilalo, J.; Hassan, A.; Arora, R.C. Frailty as a Risk Predictor in Cardiac Surgery: Beyond the Eyeball Test. J. Thorac. Cardiovasc. Surg. 2018, 156, 172–176.e2. [Google Scholar] [CrossRef] [Green Version]
- Sepehri, A.; Beggs, T.; Hassan, A.; Rigatto, C.; Shaw-Daigle, C.; Tangri, N.; Arora, R.C. The Impact of Frailty on Outcomes after Cardiac Surgery: A Systematic Review. J. Thorac. Cardiovasc. Surg. 2014, 148, 3110–3117. [Google Scholar] [CrossRef] [Green Version]
- Okamura, H.; Kimura, N.; Tanno, K.; Mieno, M.; Matsumoto, H.; Yamaguchi, A.; Adachi, H. The Impact of Preoperative Sarcopenia, Defined Based on Psoas Muscle Area, on Long-Term Outcomes of Heart Valve Surgery. J. Thorac. Cardiovasc. Surg. 2019, 157, 1071–1079.e3. [Google Scholar] [CrossRef]
- Satake, S.; Arai, H. The Revised Japanese Version of the Cardiovascular Health Study Criteria (Revised J-CHS Criteria). Geriatr. Gerontol. Int. 2020, 20, 992–993. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus Report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Hirsch, C.H.; Sommers, L.; Olsen, A.; Mullen, L.; Winograd, C.H. The Natural History of Functional Morbidity in Hospitalized Older Patients. J. Am. Geriatr. Soc. 1990, 38, 1296–1303. [Google Scholar] [CrossRef]
- Zisberg, A.; Shadmi, E.; Gur-Yaish, N.; Tonkikh, O.; Sinoff, G. Hospital-Associated Functional Decline: The Role of Hospitalization Processes Beyond Individual Risk Factors. J. Am. Geriatr. Soc. 2015, 63, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Saitoh, M.; Saji, M.; Kozono-Ikeya, A.; Arimitsu, T.; Sakuyama, A.; Ueki, H.; Nagayama, M.; Isobe, M. Hospital-Acquired Functional Decline and Clinical Outcomes in Older Patients Undergoing Transcatheter Aortic Valve Implantation. Circ. J. 2020, 84, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Tasheva, P.; Vollenweider, P.; Kraege, V.; Roulet, G.; Lamy, O.; Marques-Vidal, P.; Méan, M. Association between Physical Activity Levels in the Hospital Setting and Hospital-Acquired Functional Decline in Elderly Patients. JAMA Netw. Open 2020, 3, e1920185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sleiman, I.; Rozzini, R.; Barbisoni, P.; Morandi, A.; Ricci, A.; Giordano, A.; Trabucchi, M. Functional Trajectories during Hospitalization: A Prognostic Sign for Elderly Patients. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2009, 64, 659–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortinsky, R.H.; Covinsky, K.E.; Palmer, R.M.; Landefeld, C.S. Effects of Functional Status Changes before and during Hospitalization on Nursing Home Admission of Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1999, 54, M521–M526. [Google Scholar] [CrossRef] [PubMed]
- JCS Joint Working Group. Guidelines for Rehabilitation in Patients With Cardiovascular Disease (JCS 2012). Circ. J. 2014, 78, 2022–2093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arai, H.; Satake, S. English Translation of the Kihon Checklist. Geriatr. Gerontol. Int. 2015, 15, 518–519. [Google Scholar] [CrossRef]
- Satake, S.; Shimokata, H.; Senda, K.; Kondo, I.; Toba, K. Validity of Total Kihon Checklist Score for Predicting the Incidence of 3-Year Dependency and Mortality in a Community-Dwelling Older Population. J. Am. Med. Dir. Assoc. 2017, 18, 552.e1–552.e6. [Google Scholar] [CrossRef]
- Yamada, M.; Arai, H. Predictive Value of Frailty Scores for Healthy Life Expectancy in Community-Dwelling Older Japanese Adults. J. Am. Med. Dir. Assoc. 2015, 16, 1002.e7–1002.e11. [Google Scholar] [CrossRef]
- Kojima, G.; Taniguchi, Y.; Kitamura, A.; Shinkai, S. Are the Kihon Checklist and the Kaigo-Yobo Checklist Compatible With the Frailty Index? J. Am. Med. Dir. Assoc. 2018, 19, 797–800.e2. [Google Scholar] [CrossRef]
- Satake, S.; Shimokata, H.; Senda, K.; Kondo, I.; Arai, H.; Toba, K. Predictive Ability of Seven Domains of the Kihon Checklist for Incident Dependency and Mortality. J. Frailty Aging. 2019, 8, 85–87. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Sato, Y.; Takahashi, T.; Tsuchihashi-Makaya, M.; Kotooka, N.; Ikegame, T.; Takura, T.; Yamamoto, T.; Nagayama, M.; Goto, Y.; et al. Multidisciplinary Cardiac Rehabilitation and Long-Term Prognosis in Patients With Heart Failure. Circ. Heart Fail. 2020, 13, e006798. [Google Scholar] [CrossRef]
- Matsue, Y.; Kamiya, K.; Saito, H.; Saito, K.; Ogasahara, Y.; Maekawa, E.; Konishi, M.; Kitai, T.; Iwata, K.; Jujo, K.; et al. Prevalence and Prognostic Impact of the Coexistence of Multiple Frailty Domains in Elderly Patients With Heart Failure: The FRAGILE-HF Cohort Study. Eur. J. Heart Fail. 2020, 22, 2112–2119. [Google Scholar] [CrossRef] [PubMed]
- Bock, J.O.; König, H.H.; Brenner, H.; Haefeli, W.E.; Quinzler, R.; Matschinger, H.; Saum, K.U.; Schöttker, B.; Heider, D. Associations of Frailty With Health Care Costs—Results of the Esther Cohort Study. BMC Health Serv. Res. 2016, 16, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldfarb, M.; Bendayan, M.; Rudski, L.G.; Morin, J.F.; Langlois, Y.; Ma, F.; Lachapelle, K.; Cecere, R.; DeVarennes, B.; Tchervenkov, C.I.; et al. Cost of Cardiac Surgery in Frail Compared with Nonfrail Older Adults. Can. J. Cardiol. 2017, 33, 1020–1026. [Google Scholar] [CrossRef] [PubMed]
- Morisawa, T.; Saitoh, M.; Takahashi, T.; Watanabe, H.; Mochizuki, M.; Kitahara, E.; Fujiwara, T.; Fujiwara, K.; Nishitani-Yokoyama, M.; Minamino, T.; et al. Association of Phase Angle With Hospital-Acquired Functional Decline in Older Patients Undergoing Cardiovascular Surgery. Nutrition. 2021, 91–92, 111402. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association With Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Freiberger, E.; de Vreede, P.; Schoene, D.; Rydwik, E.; Mueller, V.; Frändin, K.; Hopman-Rock, M. Performance-Based Physical Function in Older Community-Dwelling Persons: A Systematic Review of Instruments. Age Ageing. 2012, 41, 712–721. [Google Scholar] [CrossRef] [Green Version]
- Puthoff, M.L. Outcome Measures in Cardiopulmonary Physical Therapy: Short Physical Performance Battery. Cardiopulm. Phys. Ther. J. 2008, 19, 17–22. [Google Scholar] [CrossRef]
- Rinaldo, L.; Caligari, M.; Acquati, C.; Nicolazzi, S.; Paracchini, G.; Sardano, D.; Giordano, A.; Marcassa, C.; Corrà, U. Functional Capacity Assessment and Minimal Clinically Important Difference in Post-Acute Cardiac Patients: The Role of Short Physical Performance Battery. Eur. J. Prev. Cardiol. 2021, zwab044. [Google Scholar] [CrossRef]
- Katijjahbe, M.A.; Granger, C.L.; Denehy, L.; Royse, A.; Royse, C.; Clarke, S.; El-Ansary, D. Short Physical Performance Battery Can Be Utilized to Evaluate Physical Function in Patients after Cardiac Surgery. Cardiopulm. Phys. Ther. J. 2018, 29, 88–96. [Google Scholar] [CrossRef]
- Rutten, E.P.; Spruit, M.A.; McDonald, M.L.; Rennard, S.; Agusti, A.; Celli, B.; Miller, B.E.; Crim, C.; Calverley, P.M.; Hanson, C.; et al. Continuous Fat-Free Mass Decline in COPD: Fact or Fiction? Eur. Respir. J. 2015, 46, 1496–1498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAllister, D.A.; Wild, S.H.; MacLay, J.D.; Robson, A.; Newby, D.E.; MacNee, W.; Innes, J.A.; Zamvar, V.; Mills, N.L. Forced Expiratory Volume in One Second Predicts Length of Stay and in-Hospital Mortality in Patients Undergoing Cardiac Surgery: A Retrospective Cohort Study. PLoS ONE 2013, 8, e64565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, A.J.; Ahmad, T.; Phull, M.K.; Allard, S.; Gillies, M.A.; Pearse, R.M. Meta-Analysis of the Association between Preoperative Anaemia and Mortality after Surgery. Br. J. Surg. 2015, 102, 1314–1324. [Google Scholar] [CrossRef]
- Govers, A.C.; Buurman, B.M.; Jue, P.; de Mol, B.A.; Dongelmans, D.A.; de Rooij, S.E. Functional Decline of Older Patients 1 Year after Cardiothoracic Surgery Followed by Intensive Care Admission: A Prospective Longitudinal Cohort Study. Age Ageing. 2014, 43, 575–580. [Google Scholar] [CrossRef] [Green Version]
- Itagaki, A.; Saitoh, M.; Okamura, D.; Kawamura, T.; Otsuka, S.; Tahara, M.; Mori, Y.; Kamisaka, K.; Ochi, Y.; Yuguchi, S.; et al. Factors Related to Physical Functioning Decline after Cardiac Surgery in Older Patients: A Multicenter Retrospective Study. J. Cardiol. 2019, 74, 279–283. [Google Scholar] [CrossRef]
- Ortiz-Alonso, J.; Bustamante-Ara, N.; Valenzuela, P.L.; Vidán-Astiz, M.; Rodríguez-Romo, G.; Mayordomo-Cava, J.; Javier-González, M.; Hidalgo-Gamarra, M.; Lopéz-Tatis, M.; Valades-Malagón, M.I.; et al. Effect of a Simple Exercise Program on Hospitalization-Associated Disability in Older Patients: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2020, 21, 531–537.e1. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All (n = 247) | HAFD Group (n = 52) | Non-HAFD Group (n = 195) | p-Value | |
|---|---|---|---|---|
| Age, years | 74.0 (69, 79) | 75.0 (69, 80) | 75.0 (68, 80) | 0.231 |
| Sex, female, % (n) | 38 (95) | 50 (26) | 35 (69) | 0.040 * |
| Body mass index, kg/m2 | 23.1 (21.0, 25.3) | 23.1 (19.8, 25.4) | 23.6 (21.8, 25.6) | 0.222 |
| NYHA class, % (n) | 0.568 | |||
| Class I/ Class II/ Class III/ Class IV | 38 (94)/52 (129)/9 (21)/1 (3) | 44 (23)/46 (24)/10 (5)/0 (0) | 37 (71)/54 (105)/8 (16)/1 (3) | |
| LVEF, % | 63 (55, 70) | 64 (55, 71) | 64 (56, 71) | 0.640 |
| Comorbidity | ||||
| Diabetes mellitus, % (n) | 34 (84) | 44 (23) | 31 (61) | 0.058 |
| Chronic kidney disease, % (n) | 22 (55) | 25 (13) | 18 (35) | 0.323 |
| Chronic heart failure, % (n) | 39 (95) | 35 (18) | 40 (77) | 0.631 |
| Chronic obstructive pulmonary disease, % (%(n) | 6 (14) | 14 (7) | 4 (7) | 0.013 * |
| Cerebrovascular disease, % (n) | 15 (32) | 14 (7) | 13 (25) | 0.530 |
| Hemoglobin, g/dL | 12.9 (11.6, 14.1) | 12.5 (11.6, 13.6) | 13.3 (11.7, 14.5) | 0.025* |
| Albumin, g/dl | 4.0 (3.7, 4.2) | 4.1 (3.8, 4.2) | 4.0 (3.7, 4.2) | 0.787 |
| eGFR, ml/min/1.73 m2 | 59.3 (44.3, 70.1) | 56.0 (38.6, 65.9) | 59.3 (45.7, 70.8) | 0.117 |
| Preoperative SPPB score, points | 12 (10, 12) | 12 (11, 12) | 12 (11, 12) | 0.199 |
| Postoperative SPPB score, points | 12 (10, 12) | 10 (9, 11) | 12 (11, 12) | <0.001 * |
| Preoperative gait speed, m/s | 0.98 (0.83, 1.13) | 0.97 (0.82, 1.04) | 1.03 (0.88, 1.16) | 0.152 |
| Preoperative grip strength, kg | 23.7 (17.9, 31.0) | 20.2 (16.3, 26.7) | 25.0 (18.5, 32.1) | 0.002 * |
| Preoperative frailty, % (n) | 25 (61) | 29 (15) | 24 (46) | 0.470 |
| Type of Operation, % (n) | 0.441 | |||
| CABG/Valve surgery/ | 26 (64)/32 (80) | 27 (14)/31 (16) | 26 (50)/33 (64) | |
| Multiple valve surgery/ | 23 (56) | 17 (9) | 24 (47) | |
| CABG + valve surgery | 19 (47) | 25 (13) | 17 (34) | |
| Operation time, min | 300 (251, 351) | 288 (245, 332) | 302 (243, 365) | 0.691 |
| Bleeding, mL | 570 (320, 1218) | 471 (320, 970) | 610 (260, 1350) | 0.732 |
| Length of ICU stay, days | 4.0 (3.0, 5.0) | 4.0 (3.0, 5.0) | 3.0 (2, 4) | 0.142 |
| Postoperative day that rehabilitation was started, days | 1.0 (1.0, 1.0) | 1.0 (1.0, 1.0) | 1.0 (1, 1) | 0.370 |
| Postoperative day that ambulation was started, days | 3.0 (2.0, 4.0) | 3.0 (2.0, 4.0) | 3.0 (2, 4) | 0.229 |
| Postoperative day when ambulation independence was achieved, days | 5.0 (4.0, 6.3) | 5.0 (5.0, 7.0) | 5.0 (4, 7) | 0.180 |
| Length of hospital stay, days | 19.0 (16.0, 25.0) | 22.0 (15.0, 27.0) | 19.0 (16, 24) | 0.132 |
| Univariate Analysis | Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |||
| Age (every 1-year increase) | 1.035 | 0.989 | 1.084 | 0.137 | 1.027 | 0.975 | 1.082 | 0.317 |
| Female | 1.153 | 0.670 | 1.986 | 0.607 | 1.173 | 0.609 | 2.256 | 0.634 |
| BMI (every 1-kg/m2 increase) | 0.966 | 0.895 | 1.043 | 0.378 | 1.002 | 0.917 | 1.095 | 0.964 |
| NYHA class ≥ III (every degree increase) | 1.529 | 0.648 | 3.610 | 0.333 | ||||
| LVEF (every 1% increase) | 0.977 | 0.957 | 0.998 | 0.031 * | 0.982 | 0.959 | 1.005 | 0.129 |
| Diabetes mellitus | 1.220 | 0.700 | 2.127 | 0.483 | ||||
| CKD | 1.448 | 0.755 | 2.778 | 0.266 | ||||
| Hemoglobin | 0.805 | 0.687 | 0.942 | 0.007 * | 0.847 | 0.701 | 1.023 | 0.085 |
| Albumin | 0.670 | 0.349 | 1.285 | 0.228 | ||||
| Low preoperative gait speed | 2.318 | 1.200 | 4.479 | 0.012 * | 2.477 | 1.185 | 5.176 | 0.016 * |
| Low preoperative grip strength | 1.046 | 0.598 | 1.828 | 0.875 | ||||
| Preoperative SPPB score | 0.937 | 0.816 | 1.077 | 0.361 | ||||
| Bleeding | 1.000 | 1.000 | 1.000 | 0.357 | ||||
| Operative time | 1.003 | 1.000 | 1.006 | 0.093 | 1.004 | 1.000 | 1.007 | 0.051 |
| Postoperative ICU stay | 1.120 | 0.980 | 1.282 | 0.097 | ||||
| Postoperative hospital stay | 0.994 | 0.967 | 1.023 | 0.690 | ||||
| Hospital-acquired functional decline | 3.467 | 1.842 | 6.528 | <0.001 ** | 3.437 | 1.756 | 6.729 | <0.001 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morisawa, T.; Saitoh, M.; Otsuka, S.; Takamura, G.; Tahara, M.; Ochi, Y.; Takahashi, Y.; Iwata, K.; Oura, K.; Sakurada, K.; et al. Hospital-Acquired Functional Decline and Clinical Outcomes in Older Cardiac Surgical Patients: A Multicenter Prospective Cohort Study. J. Clin. Med. 2022, 11, 640. https://doi.org/10.3390/jcm11030640
Morisawa T, Saitoh M, Otsuka S, Takamura G, Tahara M, Ochi Y, Takahashi Y, Iwata K, Oura K, Sakurada K, et al. Hospital-Acquired Functional Decline and Clinical Outcomes in Older Cardiac Surgical Patients: A Multicenter Prospective Cohort Study. Journal of Clinical Medicine. 2022; 11(3):640. https://doi.org/10.3390/jcm11030640
Chicago/Turabian StyleMorisawa, Tomoyuki, Masakazu Saitoh, Shota Otsuka, Go Takamura, Masayuki Tahara, Yusuke Ochi, Yo Takahashi, Kentaro Iwata, Keisuke Oura, Koji Sakurada, and et al. 2022. "Hospital-Acquired Functional Decline and Clinical Outcomes in Older Cardiac Surgical Patients: A Multicenter Prospective Cohort Study" Journal of Clinical Medicine 11, no. 3: 640. https://doi.org/10.3390/jcm11030640