
Hemorrhagic Resuscitation Guided by Viscoelastography in Far-Forward Combat and Austere Civilian Environments: Goal-Directed Whole-Blood and Blood-Component Therapy Far from the Trauma Center


 , , , , add
Show full author list
, , , , add
Show full author list
Abstract
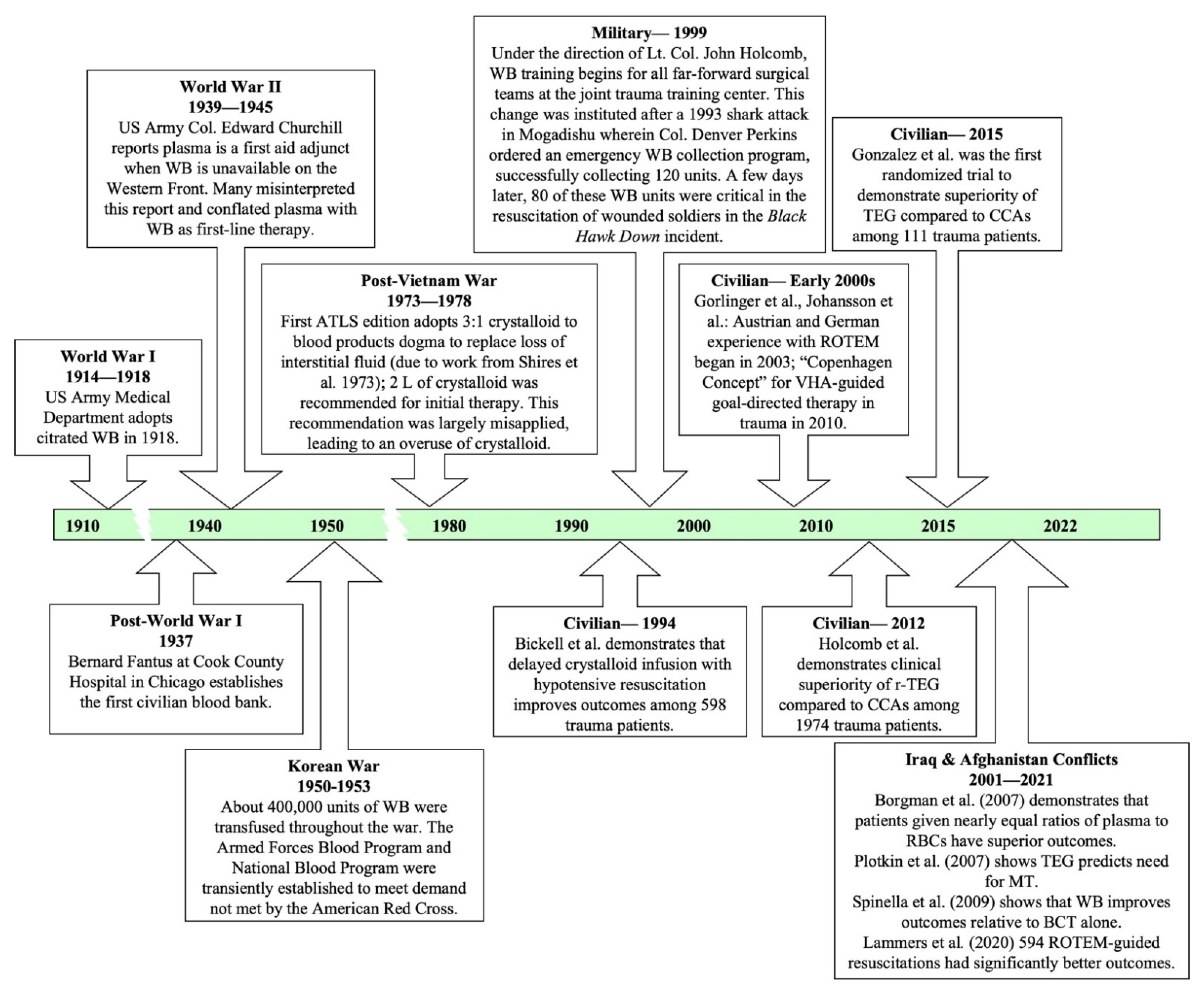
:1. Introduction

2. Modern Resuscitation in Civilian Environments
3. Thromboelastography (TEG®) and Rotational Thromboelastometry (ROTEM®)
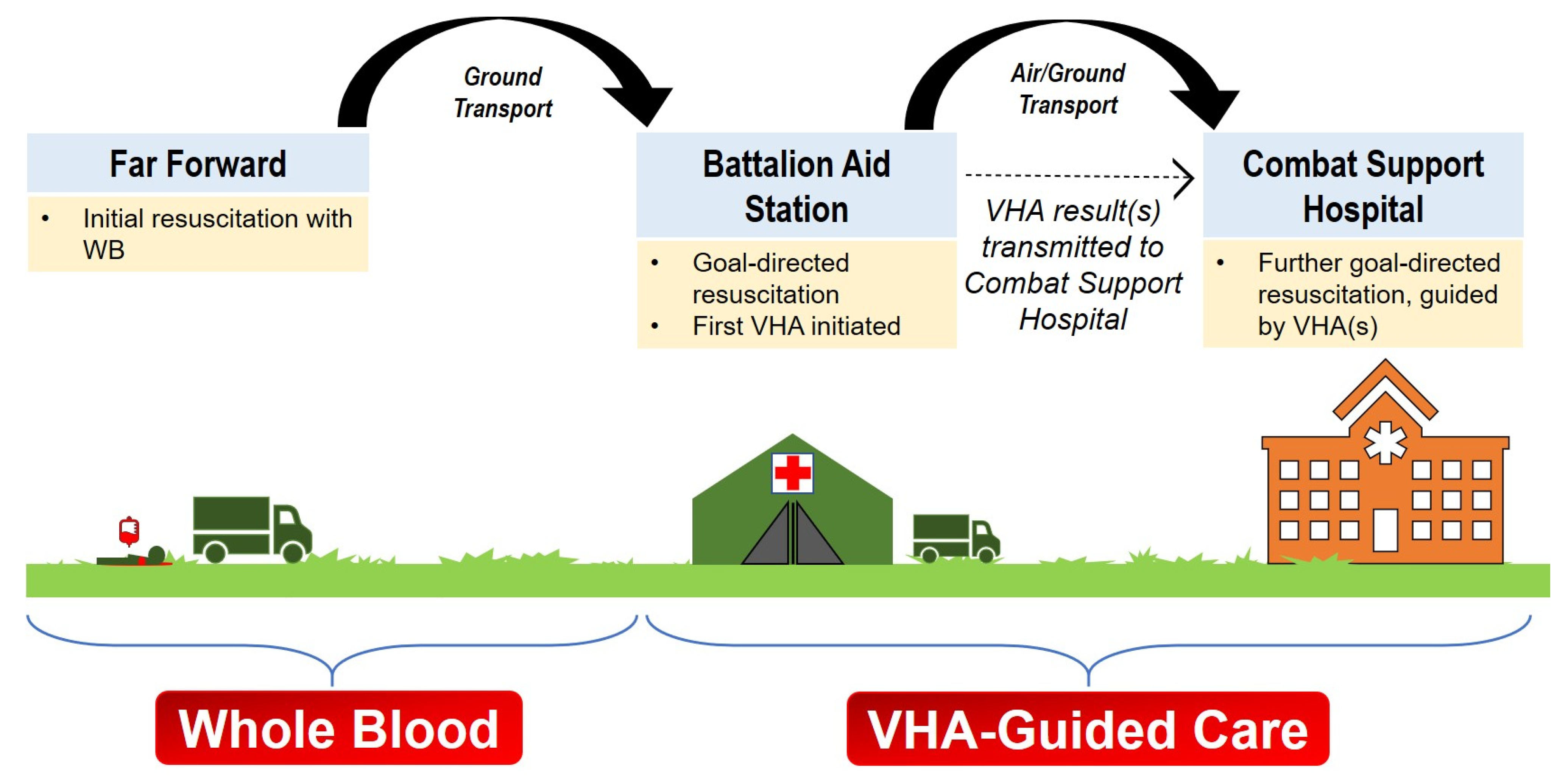
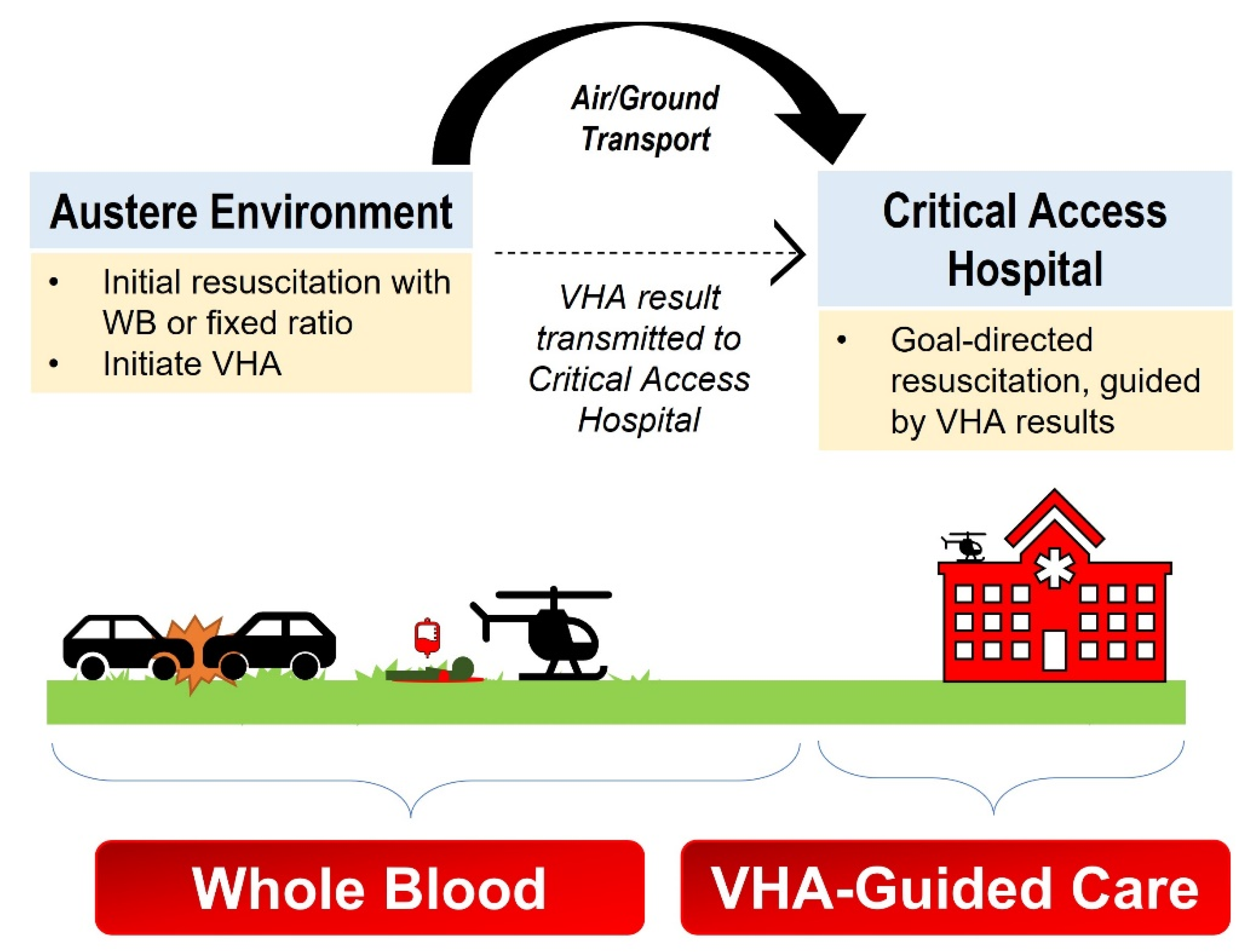
4. TEG®/ROTEM® in the Far-Forward and Austere Environment
5. Considerations for TEG®/ROTEM® Platforms in the Field
5.1. Transport

{kind=link}
{kind=link}
{kind=link}
| Article | Participants | Type of Study and Setting | Conclusions |
|---|---|---|---|
| Cundrle et al., 2013 [109] | 30 civilians treated with hypothermia for ROSC after cardiac arrest | Prospective Observational Setting: St. Anne’s University Hospital Brno, Czech Republic | Temperature adjustment for kaolin TEG® or r-TEG® are of little clinical utility due to low precision of TEG® measurements; in vivo temperature TEG® analysis is unnecessary. |
| Hunt et al., 2015 [61] | 430 military and civilian (3 total studies) | Systematic Review and Meta-analysis | Due to insufficient studies, the authors found no evidence on accuracy of TEG® and little evidence on accuracy of ROTEM® to diagnose TIC when compared to PT/INR. |
| Jeppesen et al., 2016 [110] | 40 civilians treated with hypothermia for ROSC after OHCA | Prospective Observational Setting: Aarhus University Hospital, Denmark | At 33 °C, ROTEM® demonstrated a slower initiation of coagulation compared to 37 °C. The authors recommended that VHA analyses be maintained at 37 °C regardless of the patient’s body temperature. |
| Gill et al., 2017 [97] | One healthy volunteer | Comparative Methodological Analysis Setting: Sydney Children’s Hospitals Network, New South Wales, Australia | With the TEG® 6 s, all measured parameters were significantly different while testing was subjected to motion. |
| Meledeo et al., 2018 [51] | 3 healthy donors | Prospective Observational Setting: US Army Institute Surgical Research Blood Bank, San Antonio, Fort Sam Houston, Texas | TEG® 6 s was more robust against motion and temperature stresses compared to the ROTEM® delta and TEG® 5000. TEG® 6 s may be useful in austere environments. |
| Scott et al., 2018 [96] | 148 TEG® 6 s samples (72 AW139 Helicopter flight simulators with CAE 3000-series, 76 ground) | Comparative Analysis Setting: Toll ACE Training Centre, Bankstown Airport, Sydney, NSW, Australia | TEG® 6 s was a reliable test in rotary wing flight conditions and demonstrated minimal variance compared to stable ground tests. |
| Roberts et al., 2019 [99] | 8 swine on venovenous ECMO | Comparative Analysis Setting: San Antonio Military Medical Center, Fort Sam Houston, Texas | TEG® 6 s during ground or aeromedical transport is feasible; however, method agreement was stronger at sea level and while stationary compared to mobile ground or altitude transport. |
| Bates et al., 2020 [102] | 8 healthy donors | Prospective Observational Setting: Gold Coast University Hospital ICU, Gold Coast, Queensland, Australia; and in a LifeFlight Retrieval Medicine operated Leonardo AW139 Helicopter | ROTEM® sigma and TEG® 6 s were unreliable during flight, however remained calibrated post-flight and provided sound results over time. |
| Boyé et al., 2020 [45] | 3 healthy donors 15 military ICU patients | Comparative Analysis Setting: ICU of the Military Medical Center Laveran (Marseille, France); simulated vibration at 100 Hz; simulated altitude of 8000 ft in a hypobaric chamber | TEG® 6 s parameters at simulated 0 ft and 8000 ft were consistent for 9 of 13 parameters. TEG® 6 s showed promise for aeromedical evacuation due to its ease of use and reliability. |
5.2. Altitude
5.3. Hypothermia
5.4. Time to Actionable Information
6. Future Direction
6.1. Towards a Common-Sense Approach to VHAs in the Far-Forward Setting
6.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| aPTT | Activated partial thromboplastin time |
| BCT | Blood-component therapy |
| CCA | Conventional coagulation assay |
| CFT | Clot formation time (ROTEM® parameter) |
| CRYO | Cryoprecipitate |
| CT | Clotting time (ROTEM® parameter) |
| DCR | Damage control resuscitation |
| ECMO | Extracorporeal membrane oxygenation |
| FFP | Fresh frozen plasma |
| INR | International normalized ratio |
| iTACTIC | implementing Treatment Algorithms for the Correction of Trauma-Induced Coagulopathy (clinical trial) |
| K | Clot formation time |
| LI30 | Lysis index at 30 min (ROTEM® parameter) |
| LY30 | Lysis at 30 min (TEG® parameter) |
| MA | Maximum amplitude (TEG® parameter) |
| MCF | Maximum clot firmness (ROTEM® parameter) |
| ML | Maximum lysis |
| MT | Massive transfusion |
| NATO | North Atlantic Treaty Organization |
| POC | Point-of-care |
| PPOWER | Pragmatic, Prehospital, Type O, Whole Blood Early Resuscitation (clinical trial) |
| PROPPER | Pragmatic Randomized Optimal Platelet and Plasma Ratios (clinical trial) |
| PT | Prothrombin time |
| R | Reaction time (TEG® parameter) |
| RBC | Red blood cells |
| ROTEM® | Rotational thromboelastometry® |
| r-TEG® | Rapid-thromboelastography® |
| STORHM | Sang Total dans les Hémorragies Massives (clinical trial) |
| SWAT | Shock Whole blood and Assessment of TBI (clinical trial) |
| TEG® | Thromboelastography® |
| THOR Network | Trauma Hemostasis and Oxygenation Research Network |
| TIC | Trauma-induced coagulopathy |
| TOWAR | Type O Whole Blood and Assessment of Age During Prehospital Resuscitation (clinical trial) |
| VHA | Viscoelastic hemostatic assay |
| WB | Whole blood |
| α-angle | Alpha angle |
References
- Remba, S.J.; Varon, J.; Rivera, A.; Sternbach, G.L. Dominique-Jean Larrey: The effects of therapeutic hypothermia and the first ambulance. Resuscitation 2010, 81, 268–271. [Google Scholar] [CrossRef]
- Ryan, K.L. Walter B. Cannon’s World War I experience: Treatment of traumatic shock then and now. Adv. Physiol. Educ. 2018, 42, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Cannon, W.B.; Fraser, J.; Cowell, E. The preventive treatment of wound shock. JAMA 1918, 70, 618–621. [Google Scholar]
- Thompson, P.; Strandenes, G. The History of Fluid Resuscitation for Bleeding. In Damage Control Resuscitation: Identification and Treatment of Life-Threatening Hemorrhage; Spinella, P.C., Ed.; Springer: Cham, Switzerland, 2020; pp. 3–29. [Google Scholar]
- Moore, H.B.; Moore, E.E.; Chin, T.L.; Gonzalez, E.; Chapman, M.P.; Walker, C.B.; Sauaia, A.; Banerjee, A. Activated clotting time of thrombelastography (T-ACT) predicts early postinjury blood component transfusion beyond plasma. Surgery 2014, 156, 564–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shires, G.T.; Canizaro, P.C. Fluid resuscitation in the severely injured. Surg. Clin. N. Am. 1973, 53, 1341–1366. [Google Scholar] [CrossRef]
- Spinella, P.C. Warm fresh whole blood transfusion for severe hemorrhage: US military and potential civilian applications. Crit. Care Med. 2008, 36, S340–S345. [Google Scholar] [CrossRef]
- Bowling, F.; Pennardt, A. The use of fresh whole blood transfusions by the SOF medic for hemostatic resuscitation in the austere environment. J. Spec. Oper. Med. 2010, 10, 25–35. [Google Scholar]
- Emergency War Surgery, 3rd ed.; Borden Institute, Walter Reed Army Medical Center: Washington, DC, USA, 2004.
- Bickell, W.H.; Wall, M.J., Jr.; Pepe, P.E.; Martin, R.R.; Ginger, V.F.; Allen, M.K.; Mattox, K.L. Immediate versus delayed fluid resuscitation for hypotensive patients with penetrating torso injuries. N. Engl. J. Med. 1994, 331, 1105–1109. [Google Scholar] [CrossRef]
- Revell, M.; Greaves, I.; Porter, K. Endpoints for fluid resuscitation in hemorrhagic shock. J. Trauma Acute Care Surg. 2003, 54, S63–S67. [Google Scholar]
- Borgman, M.A.; Spinella, P.C.; Perkins, J.G.; Grathwohl, K.W.; Repine, T.; Beekley, A.C.; Sebesta, J.; Jenkins, D.; Wade, C.E.; Holcomb, J.B. The ratio of blood products transfused affects mortality in patients receiving massive transfusions at a combat support hospital. J. Trauma Acute Care Surg. 2007, 63, 805–813. [Google Scholar] [CrossRef] [Green Version]
- Butler, F.K.; Holcomb, J.B.; Schreiber, M.A.; Kotwal, R.S.; Jenkins, D.A.; Champion, H.R.; Bowling, F.; Cap, A.P.; Dubose, J.J.; Dorlac, W.C. Fluid Resuscitation for Hemorrhagic Shock in Tactical Combat Casualty Care: TCCC Guidelines Change 14-01-2 June 2014; U.S. Army Institute of Surgical Research: Sam Houston, TX, USA, 2014. [Google Scholar]
- Holcomb, J.B.; Jenkins, D.; Rhee, P.; Johannigman, J.; Mahoney, P.; Mehta, S.; Cox, E.D.; Gehrke, M.J.; Beilman, G.J.; Schreiber, M.; et al. Damage control resuscitation: Directly addressing the early coagulopathy of trauma. J. Trauma Acute Care Surg. 2007, 62, 307–310. [Google Scholar] [CrossRef] [Green Version]
- Plotkin, A.J.; Wade, C.E.; Jenkins, D.H.; Smith, K.A.; Noe, J.C.; Park, M.S.; Perkins, J.G.; Holcomb, J.B. A reduction in clot formation rate and strength assessed by thrombelastography is indicative of transfusion requirements in patients with penetrating injuries. J. Trauma Acute Care Surg. 2008, 64, S64–S68. [Google Scholar] [CrossRef]
- Jobes, D.; Wolfe, Y.; O’Neill, D.; Calder, J.; Jones, L.; Sesok-Pizzini, D.; Zheng, X.L. Toward a definition of “fresh” whole blood: An in vitro characterization of coagulation properties in refrigerated whole blood for transfusion. Transfusion 2011, 51, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Nowadly, C.D.; Fisher, A.D.; Borgman, M.A.; Mdaki, K.S.; Hill, R.L.; Nicholson, S.E.; Bynum, J.A.; Schauer, S.G. The Use of Whole Blood Transfusion During Non-Traumatic Resuscitation. Mil. Med. 2021, usab128. [Google Scholar] [CrossRef] [PubMed]
- Curry, N.S.; Davenport, R. Transfusion strategies for major haemorrhage in trauma. Br. J. Haematol. 2019, 184, 508–523. [Google Scholar] [CrossRef] [Green Version]
- Spinella, P.C.; Perkins, J.G.; Grathwohl, K.W.; Beekley, A.C.; Holcomb, J.B. Warm fresh whole blood is independently associated with improved survival for patients with combat-related traumatic injuries. J. Trauma 2009, 66, S69. [Google Scholar] [CrossRef] [Green Version]
- Johansson, P.I. Goal-directed hemostatic resuscitation for massively bleeding patients: The Copenhagen concept. Transfus. Apher. Sci. 2010, 43, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Holcomb, J.B.; Minei, K.M.; Scerbo, M.L.; Radwan, Z.A.; Wade, C.E.; Kozar, R.A.; Gill, B.S.; Albarado, R.; McNutt, M.K.; Khan, S. Admission rapid thrombelastography can replace conventional coagulation tests in the emergency department: Experience with 1974 consecutive trauma patients. Ann. Surg. 2012, 256, 476–486. [Google Scholar] [CrossRef] [PubMed]
- Lammers, D.T.; Marenco, C.W.; Morte, K.R.; Bingham, J.R.; Martin, M.J.; Eckert, M.J. Viscoelastic testing in combat resuscitation: Is it time for a new standard? J. Trauma Acute Care Surg. 2020, 89, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Görlinger, K.; Fries, D.; Dirkmann, D.; Weber, C.F.; Hanke, A.A.; Schöchl, H. Reduction of fresh frozen plasma requirements by perioperative point-of-care coagulation management with early calculated goal-directed therapy. Transfus. Med. Hemotherapy 2012, 39, 104–113. [Google Scholar] [CrossRef] [Green Version]
- Strandenes, G.; De Pasquale, M.; Cap, A.P.; Hervig, T.A.; Kristoffersen, E.K.; Hickey, M.; Cordova, C.; Berseus, O.; Eliassen, H.S.; Fisher, L. Emergency whole-blood use in the field: A simplified protocol for collection and transfusion. Shock 2014, 41, 76–83. [Google Scholar] [CrossRef] [Green Version]
- McGinity, A.C.; Zhu, C.S.; Greebon, L.; Xenakis, E.; Waltman, E.; Epley, E.; Cobb, D.; Jonas, R.; Nicholson, S.E.; Eastridge, B.J. Prehospital low-titer cold-stored whole blood: Philosophy for ubiquitous utilization of O-positive product for emergency use in hemorrhage due to injury. J. Trauma Acute Care Surg. 2018, 84, S115–S119. [Google Scholar] [CrossRef]
- Seheult, J.; Bahr, M.; Spinella, P.; Triulzi, D.; Yazer, M. The Dead Sea needs salt water… massively bleeding patients need whole blood: The evolution of blood product resuscitation. Transfus. Clin. Biol. 2019, 26, 174–179. [Google Scholar] [CrossRef]
- Zielinski, M.D.; Stubbs, J.R.; Berns, K.S.; Glassberg, E.; Murdock, A.D.; Shinar, E.; Sunde, G.A.; Williams, S.; Yazer, M.H.; Zietlow, S. Prehospital blood transfusion programs: Capabilities and lessons learned. J. Trauma Acute Care Surg. 2017, 82, S70–S78. [Google Scholar] [CrossRef]
- Jenkins, D.H.; Rappold, J.F.; Badloe, J.F.; Berseus, O.; Blackbourne, L.; Brohi, K.H.; Butler, F.K.; Cap, A.P.; Cohen, M.J.; Davenport, R.; et al. Trauma hemostasis and oxygenation research position paper on remote damage control resuscitation: Definitions, current practice, and knowledge gaps. Shock 2014, 41 (Suppl. 1), 3–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooper, T.J.; De Pasquale, M.; Strandenes, G.; Sunde, G.; Ward, K.R. Challenges and possibilities in forward resuscitation. Shock 2014, 41, 13–20. [Google Scholar] [CrossRef]
- Stubbs, J.R.; Zielinski, M.D.; Jenkins, D. The state of the science of whole blood: Lessons learned at Mayo Clinic. Transfusion 2016, 56 (Suppl. 2), S173–S181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seheult, J.N.; Anto, V.; Alarcon, L.H.; Sperry, J.L.; Triulzi, D.J.; Yazer, M.H. Clinical outcomes among low-titer group O whole blood recipients compared to recipients of conventional components in civilian trauma resuscitation. Transfusion 2018, 58, 1838–1845. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, Z.G.; Chehab, M.; Nathens, A.B.; Joseph, B.; Bank, E.A.; Jansen, J.O.; Holcomb, J.B. Whole truths but half the blood: Addressing the gap between the evidence and practice of pre-hospital and in-hospital blood product use for trauma resuscitation. Transfusion 2021, 61 (Suppl. 1), S348–S353. [Google Scholar] [CrossRef]
- Martinaud, C.; Travers, S.; Pasquier, P.; Sailliol, A.; Ausset, S. Blood far forward program: Update on French armed forces policy. Transfusion 2021, 61 (Suppl. 1), S354–S355. [Google Scholar] [CrossRef]
- Walsh, M.; Moore, E.E.; Moore, H.B.; Thomas, S.; Kwaan, H.C.; Speybroeck, J.; Marsee, M.; Bunch, C.M.; Stillson, J.; Thomas, A.V.; et al. Whole Blood, Fixed Ratio, or Goal-Directed Blood Component Therapy for the Initial Resuscitation of Severely Hemorrhaging Trauma Patients: A Narrative Review. J. Clin. Med. 2021, 10, 320. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.; Thomas, S.; Kwaan, H.; Aversa, J.; Anderson, S.; Sundararajan, R.; Zimmer, D.; Bunch, C.; Stillson, J.; Draxler, D. Modern methods for monitoring hemorrhagic resuscitation in the United States: Why the delay? J. Trauma Acute Care Surg. 2020, 89, 1018–1022. [Google Scholar] [CrossRef] [PubMed]
- Sperry, J. Pragmatic Prehospital Group O Whole Blood Early Resuscitation (PPOWER) Trial: A Prospective, Interventional, Randomized, 3 Year, Pilot Clinical Trial; Lung, and Blood Institute (NHLBI): Bethesda, MD, USA, 2018.
- Hanna, K.; Bible, L.; Chehab, M.; Asmar, S.; Douglas, M.; Ditillo, M.; Castanon, L.; Tang, A.; Joseph, B. Nationwide Analysis of Whole Blood Hemostatic Resuscitation in Civilian Trauma. J. Trauma Acute Care Surg. 2020, 89, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.E.; Moore, H.B.; Chapman, M.P.; Gonzalez, E.; Sauaia, A. Goal-directed hemostatic resuscitation for trauma induced coagulopathy: Maintaining homeostasis. J. Trauma Acute Care Surg. 2018, 84, S35–S40. [Google Scholar] [CrossRef] [PubMed]
- Moore, H.B.; Moore, E.E.; Neal, M.D. Trauma Induced Coagulopathy, 2nd ed.; Spring Nature Switzerland AG: Cham, Switzerland, 2021. [Google Scholar]
- Cloonan, C.C. Treating traumatic bleeding in a combat setting. Mil. Med. 2004, 169, 8. [Google Scholar] [CrossRef] [Green Version]
- Sperry, J.L.; Early, B.; Buck, M.; Silfies, L. Shock, Whole Blood and Assessment of TBI (SWAT); University of Pittsburgh: Pittsburgh, PA, USA, 2018. [Google Scholar]
- Ausset, S.; Pouget, T.; Begué, S.; Gross, S.; Martinaud, C.; Tiberghien, P. La prise en charge transfusionnelle de l’hémorragie massive: Étude STORHM. Transfus. Clin. Biol. 2019, 26, S24. [Google Scholar] [CrossRef]
- Holcomb, J.B.; Gumbert, S. Potential value of protocols in substantially bleeding trauma patients. Curr. Opin. Anaesthesiol. 2013, 26, 215–220. [Google Scholar] [CrossRef]
- Spasiano, A.; Barbarino, C.; Marangone, A.; Orso, D.; Trillò, G.; Giacomello, R.; Bove, T.; Della Rocca, G. Early thromboelastography in acute traumatic coagulopathy: An observational study focusing on pre-hospital trauma care. Eur. J. Trauma Emerg. Surg. 2020, 1–9. [Google Scholar] [CrossRef]
- Boyé, M.; Boissin, J.; Poyat, C.; Pasquier, P.; Martinaud, C. Evaluation of the altitude impact on a point-of-care thromboelastography analyzer measurement: Prerequisites for use in airborne medical evacuation courses. Eur. J. Trauma Emerg. Surg. 2020, 1–7. [Google Scholar] [CrossRef]
- Maegele, M.; Lefering, R.; Yucel, N.; Tjardes, T.; Rixen, D.; Paffrath, T. Early Coagulopathy in mulitple injury: An analysis from the German Trauma Registry on 8724 patients. Injury 2007, 38, 298–304. [Google Scholar] [CrossRef]
- MacLeod, J.B.; Lynn, M.; McKenney, M.G.; Cohn, S.M.; Murtha, M. Early coagulopathy predicts mortality in trauma. J. Trauma Acute Care Surg. 2003, 55, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Davenport, R.; Manson, J.; De’Ath, H.; Platton, S.; Coates, A.; Allard, S.; Hart, D.; Pearse, R.; Pasi, K.J.; MacCallum, P.; et al. Functional definition and characterization of acute traumatic coagulopathy. Crit. Care Med. 2011, 39, 2652–2658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagemo, J.S.; Christiaans, S.C.; Stanworth, S.J.; Brohi, K.; Johansson, P.I.; Goslings, J.C.; Naess, P.A.; Gaarder, C. Detection of acute traumatic coagulopathy and massive transfusion requirements by means of rotational thromboelastometry: An international prospective validation study. Crit Care 2015, 19, 97. [Google Scholar] [CrossRef] [Green Version]
- Tauber, H.; Innerhofer, P.; Breitkopf, R.; Westermann, I.; Beer, R.; El Attal, R.; Strasak, A.; Mittermayr, M. Prevalence and impact of abnormal ROTEM(R) assays in severe blunt trauma: Results of the ‘Diagnosis and Treatment of Trauma-Induced Coagulopathy (DIA-TRE-TIC) study’. Br. J. Anaesth. 2011, 107, 378–387. [Google Scholar] [CrossRef] [Green Version]
- Meledeo, M.A.; Peltier, G.C.; McIntosh, C.S.; Voelker, C.R.; Bynum, J.A.; Cap, A.P. Functional stability of the TEG 6s hemostasis analyzer under stress. J. Trauma Acute Care Surg. 2018, 84, S83–S88. [Google Scholar] [CrossRef]
- Sachdeva, S.; Davis, R.W.; Saha, A.K. Microfluidic Point-of-Care Testing: Commercial Landscape and Future Directions. Front. Bioeng. Biotechnol. 2021, 8, 1537. [Google Scholar] [CrossRef]
- Chang, R.; Fox, E.E.; Greene, T.J.; Swartz, M.D.; DeSantis, S.M.; Stein, D.M.; Bulger, E.M.; Melton, S.M.; Goodman, M.D.; Schreiber, M.A. Abnormalities of laboratory coagulation tests versus clinically evident coagulopathic bleeding: Results from the prehospital resuscitation on helicopters study (PROHS). Surgery 2018, 163, 819–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pusateri, A.E.; Moore, E.E.; Moore, H.B.; Le, T.D.; Guyette, F.X.; Chapman, M.P.; Sauaia, A.; Ghasabyan, A.; Chandler, J.; McVaney, K. Association of prehospital plasma transfusion with survival in trauma patients with hemorrhagic shock when transport times are longer than 20 min: A post hoc analysis of the PAMPer and COMBAT clinical trials. JAMA Surg. 2020, 155, e195085. [Google Scholar] [CrossRef]
- Zong, Z.-W.; Chen, S.-X.; Qin, H.; Liang, H.-P.; Yang, L.; Zhao, Y.-F. Chinese expert consensus on echelons treatment of pelvic fractures in modern war. Mil. Med. Res. 2018, 5, 21. [Google Scholar] [CrossRef] [Green Version]
- Peng, H.; Nascimento, B.; Tien, B. A comparative analysis of functional fibrinogen assays using teg and rotem in trauma patients enrolled in the fiirst trial. Panam. J. Trauma Crit. Care Emerg. Surg. 2018, 7, 143–157. [Google Scholar]
- Tourtier, J.-P.; Palmier, B.; Tazarourte, K.; Raux, M.; Meaudre, E.; Ausset, S.; Sailliol, A.; Vivien, B.; Domanski, L.; Carli, P. The concept of damage control: Extending the paradigm in the prehospital setting. In Annales Francaises D’anesthesie et de Reanimation; Elsevier: Amsterdam, The Netherlands, 2013; pp. 520–526. [Google Scholar]
- Blackbourne, L.H.; Baer, D.G.; Eastridge, B.J.; Kheirabadi, B.; Kragh, J.F., Jr.; Cap, A.P.; Dubick, M.A.; Morrison, J.J.; Midwinter, M.J.; Butler, F.K. Military medical revolution: Prehospital combat casualty care. J. Trauma Acute Care Surg. 2012, 73, S372–S377, Correction in J. Trauma Acute Care Surg. 2013, 74, 705–705. [Google Scholar] [CrossRef] [PubMed]
- Deras, P.; Nouri, J.; Martinez, O.; Aubry, E.; Capdevila, X.; Charbit, J. Diagnostic performance of prothrombin time point-of-care to detect acute traumatic coagulopathy on admission: Experience of 522 cases in trauma center. Transfusion 2018, 58, 1781–1791. [Google Scholar] [CrossRef]
- Bouzat, P.; Guerin, R.; Boussat, B.; Nicolas, J.; Lambert, A.; Greze, J.; Maegele, M.; David, J.-S. Diagnostic performance of thromboelastometry in trauma-induced coagulopathy: A comparison between two level I trauma centres using two different devices. Eur. J. Trauma Emerg. Surg. 2021, 47, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Hunt, H.; Stanworth, S.; Curry, N.; Woolley, T.; Cooper, C.; Ukoumunne, O.; Zhelev, Z.; Hyde, C. Thromboelastography (TEG) and rotational thromboelastometry (ROTEM) for trauma-induced coagulopathy in adult trauma patients with bleeding. Cochrane Libr. 2015, 2015, CD010438. [Google Scholar] [CrossRef] [Green Version]
- Deng, Q.; Hao, F.; Wang, Y.; Guo, C. Rotation thromboelastometry (ROTEM) enables improved outcomes in the pediatric trauma population. J. Int. Med. Res. 2018, 46, 5195–5204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graff, J.T.; Cortez, A.R.; Dhar, V.K.; Wakefield, C.; Cuffy, M.C.; Shah, S.A.; Goodman, M.D. Perioperative thrombelastography serves as an important assessment tool of transfusion requirements during liver transplantation. Surg. Open Sci. 2020, 2, 70–74. [Google Scholar] [CrossRef]
- Meco, M.; Montisci, A.; Giustiniano, E.; Greco, M.; Pappalardo, F.; Mammana, L.; Panisi, P.; Roscitano, C.; Cirri, S.; Donatelli, F.; et al. Viscoelastic Blood Tests Use in Adult Cardiac Surgery: Meta-Analysis, Meta-Regression, and Trial Sequential Analysis. J. Cardiothorac. Vasc. Anesth. 2020, 34, 119–127. [Google Scholar] [CrossRef] [Green Version]
- Redfern, R.E.; Naimy, G.; Kuehne, M.; Fleming, K.; Bobulski, N.; Chen, J.T.; Moront, M.G. Retrospective Analysis of Thromboelastography-Directed Transfusion in Isolated CABG: Impact on Blood Product Use, Cost, and Outcomes. J. Extra-Corpor. Technol. 2020, 52, 103–111. [Google Scholar]
- Gratz, J.; Güting, H.; Thorn, S.; Brazinova, A.; Görlinger, K.; Schäfer, N.; Schöchl, H.; Stanworth, S.; Maegele, M. Protocolised thromboelastometric-guided haemostatic management in patients with traumatic brain injury: A pilot study. Anaesthesia 2019, 74, 883–890. [Google Scholar] [CrossRef]
- Bradbury, J.L.; Thomas, S.G.; Sorg, N.R.; Mjaess, N.; Berquist, M.R.; Brenner, T.J.; Langford, J.H.; Marsee, M.K.; Moody, A.N.; Bunch, C.M.; et al. Viscoelastic Testing and Coagulopathy of Traumatic Brain Injury. J. Clin. Med. 2021, 10, 5039. [Google Scholar] [CrossRef]
- Liew-Spilger, A.E.; Sorg, N.R.; Brenner, T.J.; Langford, J.H.; Berquist, M.; Mark, N.M.; Moore, S.H.; Mark, J.; Baumgartner, S.; Abernathy, M.P. Viscoelastic Hemostatic Assays for Postpartum Hemorrhage. J. Clin. Med. 2021, 10, 3946. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, C.; Chinna, S.; Um, J.Y.; Dias, J.D.; Hartmann, J.; Bradley, J.; Brooks, A. Site-Of-Care Viscoelastic Assay in Major Trauma Improves Outcomes and Is Cost Neutral Compared with Standard Coagulation Tests. Diagnostics 2020, 10, 486. [Google Scholar] [CrossRef] [PubMed]
- Baksaas-Aasen, K.; Gall, L.S.; Stensballe, J.; Juffermans, N.P.; Curry, N.; Maegele, M.; Brooks, A.; Rourke, C.; Gillespie, S.; Murphy, J.; et al. Viscoelastic haemostatic assay augmented protocols for major trauma haemorrhage (ITACTIC): A randomized, controlled trial. Intensive Care Med. 2021, 47, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Mitra, B.; Cameron, P.A.; Gruen, R.L.; Mori, A.; Fitzgerald, M.; Street, A. The definition of massive transfusion in trauma: A critical variable in examining evidence for resuscitation. Eur. J. Emerg. Med. 2011, 18, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Stettler, G.R.; Moore, E.E.; Nunns, G.R.; Chandler, J.; Peltz, E.; Silliman, C.C.; Banerjee, A.; Sauaia, A. Rotational thromboelastometry thresholds for patients at risk for massive transfusion. J. Surg. Res. 2018, 228, 154–159. [Google Scholar] [CrossRef]
- Stettler, G.R.; Moore, E.E.; Moore, H.B.; Nunns, G.R.; Silliman, C.C.; Banerjee, A.; Sauaia, A. Redefining postinjury fibrinolysis phenotypes using two viscoelastic assays. J. Trauma Acute Care Surg. 2019, 86, 679–685. [Google Scholar] [CrossRef]
- Hartert, H. Coagulation analysis with thromboelastography, a new method. Klin. Wochenschr. 1948, 26, 577–658. [Google Scholar] [CrossRef]
- Stettler, G.R.; Sumislawski, J.J.; Moore, E.E.; Nunns, G.R.; Kornblith, L.Z.; Conroy, A.S.; Callcut, R.A.; Silliman, C.C.; Banerjee, A.; Cohen, M.J. Citrated kaolin thrombelastography (TEG) thresholds for goal-directed therapy in injured patients receiving massive transfusion. J. Trauma Acute Care Surg. 2018, 85, 734. [Google Scholar] [CrossRef] [PubMed]
- Görlinger, K.; Dirkmann, D.; Hanke, A.A. Rotational Thromboelastometry (ROTEM®). In Trauma Induced Coagulopathy, 2nd ed.; Moore, H.B., Moore, E.E., Neal, M.D., Eds.; Spring Nature Switzerland AG: Cham, Switzerland, 2021; pp. 279–312. [Google Scholar]
- Vigneshwar, N.G.; Moore, E.E.; Moore, H.B.; Cotton, B.A.; Holcomb, J.B.; Cohen, M.J.; Sauaia, A. Precision medicine: Clinical tolerance to hyperfibrinolysis differs by shock and injury severity. Ann. Surg. 2020. [Google Scholar] [CrossRef]
- Regling, K.; Kakulavarapu, S.; Thomas, R.; Hollon, W.; Chitlur, M.B. Utility of thromboelastography for the diagnosis of von Willebrand disease. Pediatr. Blood Cancer 2019, 66, e27714. [Google Scholar] [CrossRef] [PubMed]
- Topf, H.G.; Weiss, D.; Lischetzki, G.; Strasser, E.; Rascher, W.; Rauh, M. Evaluation of a modified thromboelastography assay for the screening of von Willebrand disease. Thromb. Haemost. 2011, 105, 1091–1099. [Google Scholar] [CrossRef]
- Guzman-Reyes, S.; Osborne, C.; Pivalizza, E.G. Thrombelastography for perioperative monitoring in patients with von Willebrand disease. J. Clin. Anesth. 2012, 24, 166–167. [Google Scholar] [CrossRef]
- Li, R.; Elmongy, H.; Sims, C.; Diamond, S.L. Ex vivo recapitulation of trauma-induced coagulopathy and assessment of trauma patient platelet function under flow using microfluidic technology. J. Trauma Acute Care Surg. 2016, 80, 440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, D.E.; Chaireti, R.; Bruzelius, M.; Holmström, M.; Antovic, J.; Ågren, A. Correlation of thromboelastography and thrombin generation assays in warfarin-treated patients. Thromb. Res. 2019, 178, 34–40. [Google Scholar] [CrossRef]
- Gosselin, R.C.; Adcock, D.M.; Bates, S.M.; Douxfils, J.; Favaloro, E.J.; Gouin-Thibault, I.; Guillermo, C.; Kawai, Y.; Lindhoff-Last, E.; Kitchen, S. International Council for Standardization in Haematology (ICSH) recommendations for laboratory measurement of direct oral anticoagulants. Thromb. Haemost. 2018, 118, 437–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, J.D.; Lopez-Espina, C.G.; Ippolito, J.; Hsiao, L.H.; Zaman, F.; Muresan, A.A.; Thomas, S.G.; Walsh, M.; Jones, A.J.; Grisoli, A.; et al. Rapid point-of-care detection and classification of direct-acting oral anticoagulants with the TEG 6s: Implications for trauma and acute care surgery. J. Trauma Acute Care Surg. 2019, 87, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Craft, R.M.; Chavez, J.J.; Bresee, S.J.; Wortham, D.C.; Cohen, E.; Carroll, R.C. A novel modification of the Thrombelastograph assay, isolating platelet function, correlates with optical platelet aggregation. J. Lab Clin. Med. 2004, 143, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Bochsen, L.; Wiinberg, B.; Kjelgaard-Hansen, M.; Steinbruchel, D.A.; Johansson, P.I. Evaluation of the TEG platelet mapping assay in blood donors. Thromb. J. 2007, 5, 3. [Google Scholar] [CrossRef] [Green Version]
- Schenk, B.; Görlinger, K.; Treml, B.; Tauber, H.; Fries, D.; Niederwanger, C.; Oswald, E.; Bachler, M. A comparison of the new ROTEM® sigma with its predecessor, the ROTEMdelta. Anaesthesia 2019, 74, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Neal, M.D.; Moore, E.E.; Walsh, M.; Thomas, S.; Callcut, R.A.; Kornblith, L.Z.; Schreiber, M.; Ekeh, A.P.; Singer, A.J.; Lottenberg, L. A comparison between the TEG 6s and TEG 5000 analyzers to assess coagulation in trauma patients. J. Trauma Acute Care Surg. 2020, 88, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Morton, S.; Galea, J.; Uprichard, J.; Hudson, A. The practicalities and barriers of using TEG6s in code red traumas: An observational study in one London major trauma centre. Can. J. Emerg. Med. 2019, 21, 361–364. [Google Scholar] [CrossRef] [Green Version]
- Gurbel, P.A.; Bliden, K.P.; Tantry, U.S.; Monroe, A.L.; Muresan, A.A.; Brunner, N.E.; Lopez-Espina, C.G.; Delmenico, P.R.; Cohen, E.; Raviv, G.; et al. First report of the point-of-care TEG: A technical validation study of the TEG-6S system. Platelets 2016, 27, 642–649. [Google Scholar] [CrossRef]
- Duffield, C.; Davies, R.; Barclay, P. Advances in thromboelastograph technology. Anaesthesia 2018, 73, 398–399. [Google Scholar] [CrossRef]
- Howley, I.W.; Haut, E.R.; Jacobs, L.; Morrison, J.J.; Scalea, T.M. Is thromboelastography (TEG)-based resuscitation better than empirical 1: 1 transfusion? Trauma Surg. Acute Care Open 2018, 3, e000140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doran, C.M.; Woolley, T.; Midwinter, M.J. Feasibility of using rotational thromboelastometry to assess coagulation status of combat casualties in a deployed setting. J. Trauma Acute Care Surg. 2010, 69, S40–S48. [Google Scholar] [CrossRef]
- Prat, N.J.; Meyer, A.D.; Ingalls, N.K.; Trichereau, J.; DuBose, J.J.; Cap, A.P. Rotational thromboelastometry significantly optimizes transfusion practices for damage control resuscitation in combat casualties. J. Trauma Acute Care Surg. 2017, 83, 373. [Google Scholar] [CrossRef]
- Cohen, J.; Scorer, T.; Wright, Z.; Stewart, I.J.; Sosnov, J.; Pidcoke, H.; Fedyk, C.; Kwan, H.; Chung, K.K.; Heegard, K. A prospective evaluation of thromboelastometry (ROTEM) to identify acute traumatic coagulopathy and predict massive transfusion in military trauma patients in Afghanistan. Transfusion 2019, 59, 1601–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, R.; Burns, B.; Ware, S.; Oud, F.; Miller, M. The reliability of thromboelastography in a simulated rotary wing environment. Emerg. Med. J. 2018, 35, 739–742. [Google Scholar] [CrossRef] [PubMed]
- Gill, M. The TEG®6s on Shaky Ground? A Novel Assessment of the TEG®6s Performance under a Challenging Condition. J. Extra-Corpor. Technol. 2017, 49, 26–29. [Google Scholar]
- Lloyd-Donald, P.; Churilov, L.; Zia, F.; Bellomo, R.; Hart, G.; McCall, P.; Mårtensson, J.; Glassford, N.; Weinberg, L. Assessment of agreement and interchangeability between the TEG5000 and TEG6S thromboelastography haemostasis analysers: A prospective validation study. BMC Anesthesiol. 2019, 19, 45. [Google Scholar] [CrossRef] [PubMed]
- Roberts, T.R.; Jones, J.A.; Choi, J.-H.; Sieck, K.N.; Harea, G.T.; Wendorff, D.S.; Beely, B.M.; Karaliou, V.; Cap, A.P.; Davis, M.R. Thromboelastography on-the-go: Evaluation of the TEG 6s device during ground and high-altitude aeromedical evacuation with extracorporeal life support. J. Trauma Acute Care Surg. 2019, 87, S119–S127. [Google Scholar] [CrossRef] [PubMed]
- Wong, Q.; Byrne, K.P.; Robinson, S.C. Clinical agreement and interchangeability of TEG5000 and TEG6s during cardiac surgery. Anaesth. Intensive Care 2020, 48, 43–52. [Google Scholar] [CrossRef]
- Bialkower, M.; Garnier, G. Fibrinogen Diagnostics in Major Hemorrhage. Crit. Rev. Anal. Chem. 2020, 52, 194–209. [Google Scholar] [CrossRef]
- Bates, A.; Donohue, A.; McCullough, J.; Winearls, J. Viscoelastic haemostatic assays in aeromedical transport. Emerg. Med. Australas. 2020, 32, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Allan, P.F.; Osborn, E.C.; Bloom, B.B.; Wanek, S.; Cannon, J.W. The introduction of extracorporeal membrane oxygenation to aeromedical evacuation. Mil. Med. 2011, 176, 932–937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamm, M.S.; Sams, V.G.; DellaVolpe, M.J.D.; Lantry, J.H.; Mason, P.E. Case Report of Extracorporeal Membrane Oxygenation and Aeromedical Evacuation at a Deployed Military Hospital. Mil. Med. 2018, 183, 203–206. [Google Scholar] [CrossRef] [Green Version]
- Esper, S.A.; Levy, J.H.; Waters, J.H.; Welsby, I.J. Extracorporeal membrane oxygenation in the adult: A review of anticoagulation monitoring and transfusion. Anesth. Analg. 2014, 118, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Panigada, M.; Iapichino, G.E.; Brioni, M.; Panarello, G.; Protti, A.; Grasselli, G.; Occhipinti, G.; Novembrino, C.; Consonni, D.; Arcadipane, A.; et al. Thromboelastography-based anticoagulation management during extracorporeal membrane oxygenation: A safety and feasibility pilot study. Ann. Intensive Care 2018, 8, 7. [Google Scholar] [CrossRef] [Green Version]
- Colman, E.; Yin, E.B.; Laine, G.; Chatterjee, S.; Saatee, S.; Herlihy, J.P.; Reyes, M.A.; Bracey, A.W. Evaluation of a heparin monitoring protocol for extracorporeal membrane oxygenation and review of the literature. J. Thorac. Dis. 2019, 11, 3325–3335. [Google Scholar] [CrossRef]
- Chlebowski, M.M.; Baltagi, S.; Carlson, M.; Levy, J.H.; Spinella, P.C. Clinical controversies in anticoagulation monitoring and antithrombin supplementation for ECMO. Crit. Care 2020, 24, 19. [Google Scholar] [CrossRef] [Green Version]
- Cundrle, I., Jr.; Sramek, V.; Pavlik, M.; Suk, P.; Radouskova, I.; Zvonicek, V. Temperature corrected thromboelastography in hypothermia: Is it necessary? Eur. J. Anaesthesiol. 2013, 30, 85–89. [Google Scholar] [CrossRef]
- Jeppesen, A.N.; Kirkegaard, H.; Ilkjær, S.; Hvas, A.M. Influence of temperature on thromboelastometry and platelet aggregation in cardiac arrest patients undergoing targeted temperature management. Crit. Care 2016, 20, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, D.S.; Pate, J.S.; Vercueil, A.; Doyle, P.W.; Mythen, M.G.; Grocott, M.P. Reduced coagulation at high altitude identified by thromboelastography. Thromb. Haemost. 2012, 107, 1066–1071. [Google Scholar] [CrossRef] [PubMed]
- Rocke, A.S.; Paterson, G.G.; Barber, M.T.; Jackson, A.I.; Main, S.; Stannett, C.; Schnopp, M.F.; Baillie, J.K.; Horne, E.H.; Moores, C. Thromboelastometry and platelet function during acclimatization to high altitude. Thromb. Haemost. 2018, 118, 063–071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anand, A.C.; Jha, S.K.; Saha, A.; Sharma, V.; Adya, C.M. Thrombosis as a complication of extended stay at high altitude. Natl Med. J. India 2001, 14, 197–201. [Google Scholar] [PubMed]
- Trąbka-Zawicki, A.; Tomala, M.; Zeliaś, A.; Paszek, E.; Zajdel, W.; Stępień, E.; Żmudka, K. Adaptation of global hemostasis to therapeutic hypothermia in patients with out-of-hospital cardiac arrest: Thromboelastography study. Cardiol. J. 2019, 26, 77–86. [Google Scholar] [CrossRef] [Green Version]
- Forman, K.R.; Wong, E.; Gallagher, M.; McCarter, R.; Luban, N.L.; Massaro, A.N. Effect of temperature on thromboelastography and implications for clinical use in newborns undergoing therapeutic hypothermia. Pediatr. Res. 2014, 75, 663–669. [Google Scholar] [CrossRef] [Green Version]
- Luna, G.K.; Maier, R.V.; Pavlin, E.G.; Anardi, D.; Copass, M.K.; Oreskovich, M.R. Incidence and effect of hypothermia in seriously injured patients. J. Trauma 1987, 27, 1014–1018. [Google Scholar] [CrossRef]
- Klauke, N.; Gräff, I.; Fleischer, A.; Boehm, O.; Guttenthaler, V.; Baumgarten, G.; Meybohm, P.; Wittmann, M. Effects of prehospital hypothermia on transfusion requirements and outcomes: A retrospective observatory trial. BMJ Open 2016, 6, e009913. [Google Scholar] [CrossRef] [Green Version]
- Cotton, B.A.; Faz, G.; Hatch, Q.M.; Radwan, Z.A.; Podbielski, J.; Wade, C.; Kozar, R.A.; Holcomb, J.B. Rapid Thrombelastography Delivers Real-Time Results That Predict Transfusion Within 1 Hour of Admission. J. Trauma Acute Care Surg. 2011, 71, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Pressly, M.A.; Neal, M.D.; Waters, J.H.; Clermont, G.; Parker, R.S. Coupled Model of Blood Volume and Activated Clotting Factor Concentration during Childbirth. IFAC-PapersOnLine 2018, 51, 52–55. [Google Scholar] [CrossRef]
- Baksaas-Aasen, K.; Van Dieren, S.; Balvers, K.; Juffermans, N.P.; Næss, P.A.; Rourke, C.; Eaglestone, S.; Ostrowski, S.R.; Stensballe, J.; Stanworth, S.; et al. Data-driven Development of ROTEM and TEG Algorithms for the Management of Trauma Hemorrhage: A Prospective Observational Multicenter Study. Ann. Surg. 2019, 270, 1178–1185. [Google Scholar] [CrossRef] [PubMed]
- Pressly, M.A.; Parker, R.S.; Neal, M.D.; Sperry, J.L.; Clermont, G. Accelerating availability of clinically-relevant parameter estimates from thromboelastogram point-of-care device. J. Trauma Acute Care Surg. 2020, 88, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.D.; Miles, E.A.; Broussard, M.A.; Corley, J.B.; Knight, R.; Remley, M.A.; Cap, A.P.; Gurney, J.M.; Shackelford, S.A. Low titer group O whole blood resuscitation: Military experience from the point of injury. J. Trauma Acute Care Surg. 2020, 89, 834–841. [Google Scholar] [CrossRef] [PubMed]
- Brearton, C.; Rushton, A.; Parker, J.; Martin, H.; Hodgson, J. Performance Evaluation of a New Point of Care Viscoelastic Coagulation Monitoring System in Major Abdominal, Orthopaedic and Vascular Surgery. Platelets 2020, 31, 1052–1059. [Google Scholar] [CrossRef] [PubMed]


| Article | Participants | Type of Study and Setting | Conclusions |
|---|---|---|---|
| Plotkin et al., 2008 [15] | 44 military personnel with penetrating injuries | Retrospective Observational Setting: US Army Combat Support Hospital in Iraq | TEG® as an adjunct to platelet counts and hematocrit was more predictive of blood transfusion than PT, aPTT, and INR together. Specifically, a reduced MA on TEG® within 24 h of admission correlated with more administered blood products. |
| Doran et al., 2010 [93] | 31 military personnel (19/31 received MT) | Prospective Observational Setting: United Kingdom Military; Camp Bastion, Helmand province, Afghanistan | ROTEM® is feasible in the military setting and has a greater sensitivity for coagulation abnormalities compared to PT and aPTT. |
| Prat et al., 2017 [94] | 219 military personnel (85 received ROTEM®-guided transfusion) | Retrospective Observational Setting: US Craig Theater Hospital, Bagram Airfield in Afghanistan | ROTEM® did not significantly improve mortality or MT protocol activation. However, the ROTEM®-guided group received significant increases in PLT and CRYO transfusions (4× and 2×, respectively). ROTEM® increased adherence to DCR protocol. |
| Cohen et al., 2019 [95] | 40 military casualties | Prospective Observational Setting: NATO Hospitals in Afghanistan | ROTEM® detected hemorrhagic coagulopathy and need for MT with greater sensitivity than INR alone. ROTEM® should be included in MT protocols. |
| Lammers et al., 2020 [22] | 3320 military personnel (594 received VHA-guided initial resuscitation) | Retrospective Observational Setting: US-led NATO Role III Multinational Medical Unit | VHA-guided resuscitation was independently associated with a decreased mortality (OR, 0.63; p = 0.001) and a 57% reduction in overall mortality (7.3% vs. 13.1%, p = 0.001). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lantry, J.H.; Mason, P.; Logsdon, M.G.; Bunch, C.M.; Peck, E.E.; Moore, E.E.; Moore, H.B.; Neal, M.D.; Thomas, S.G.; Khan, R.Z.; et al. Hemorrhagic Resuscitation Guided by Viscoelastography in Far-Forward Combat and Austere Civilian Environments: Goal-Directed Whole-Blood and Blood-Component Therapy Far from the Trauma Center. J. Clin. Med. 2022, 11, 356. https://doi.org/10.3390/jcm11020356
Lantry JH, Mason P, Logsdon MG, Bunch CM, Peck EE, Moore EE, Moore HB, Neal MD, Thomas SG, Khan RZ, et al. Hemorrhagic Resuscitation Guided by Viscoelastography in Far-Forward Combat and Austere Civilian Environments: Goal-Directed Whole-Blood and Blood-Component Therapy Far from the Trauma Center. Journal of Clinical Medicine. 2022; 11(2):356. https://doi.org/10.3390/jcm11020356
Chicago/Turabian StyleLantry, James H., Phillip Mason, Matthew G. Logsdon, Connor M. Bunch, Ethan E. Peck, Ernest E. Moore, Hunter B. Moore, Matthew D. Neal, Scott G. Thomas, Rashid Z. Khan, and et al. 2022. "Hemorrhagic Resuscitation Guided by Viscoelastography in Far-Forward Combat and Austere Civilian Environments: Goal-Directed Whole-Blood and Blood-Component Therapy Far from the Trauma Center" Journal of Clinical Medicine 11, no. 2: 356. https://doi.org/10.3390/jcm11020356