
Intracranial Pressure Patterns and Neurological Outcomes in Out-of-Hospital Cardiac Arrest Survivors after Targeted Temperature Management: A Retrospective Observational Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
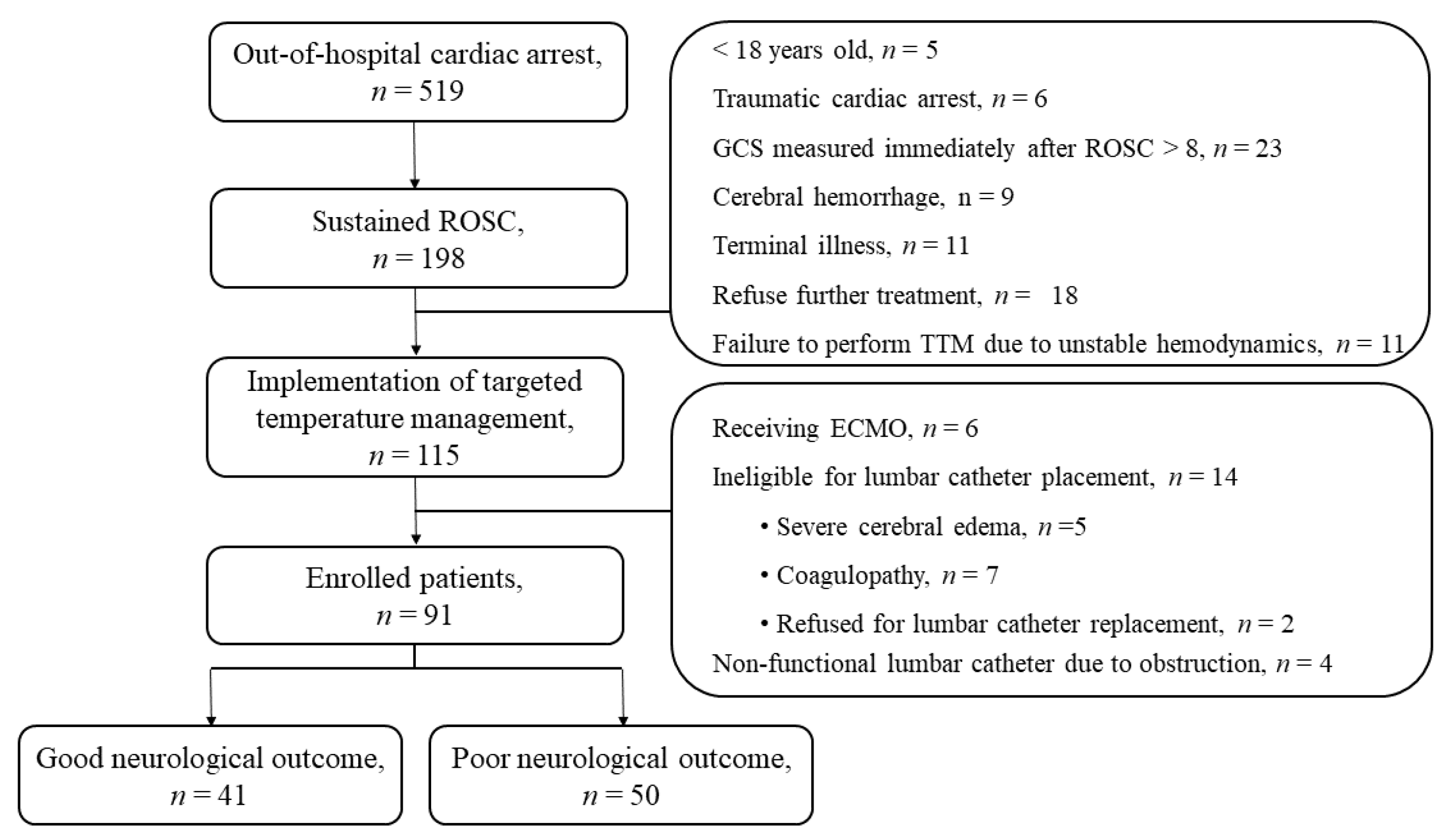
2.1. Study Design and Population
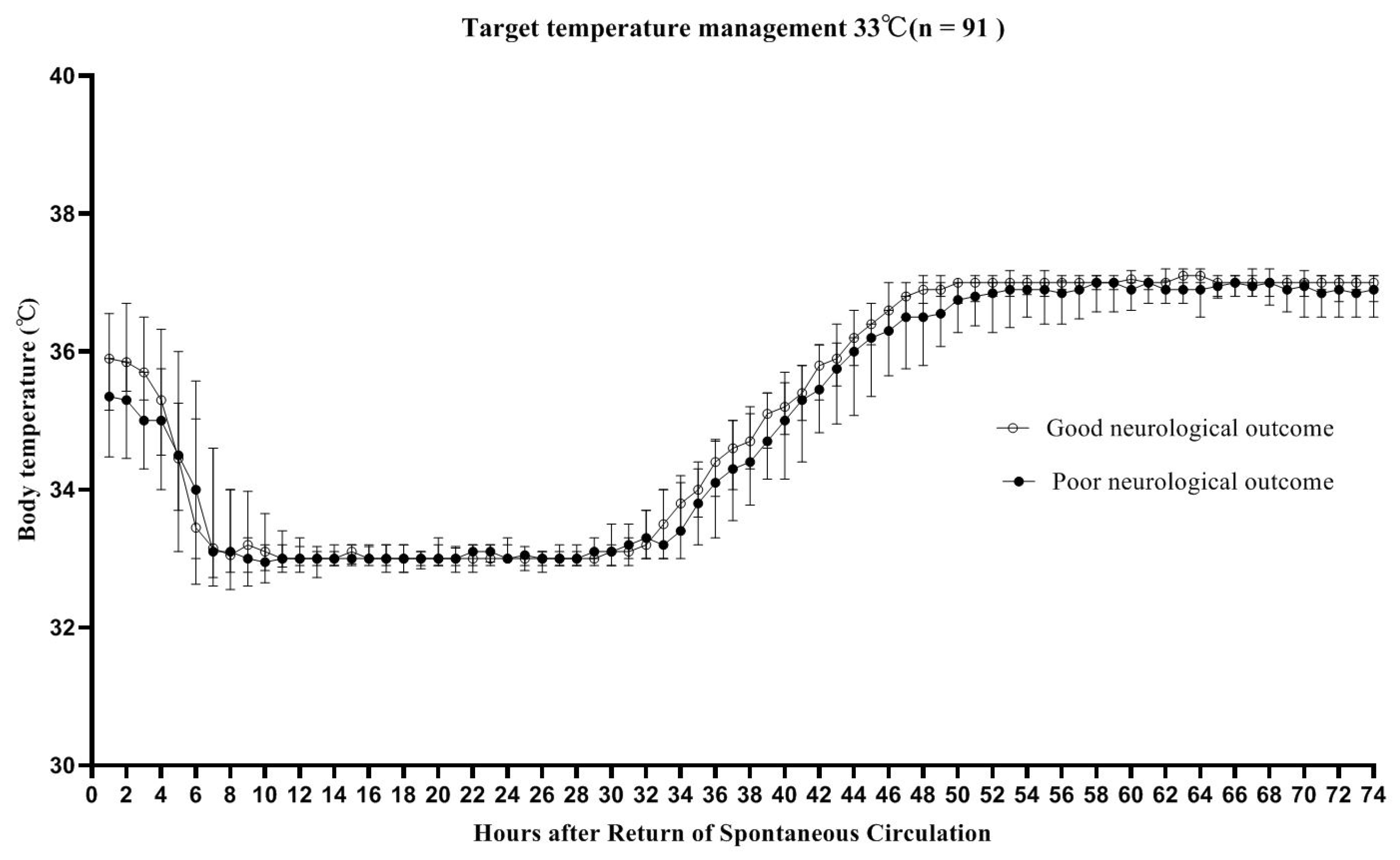
2.2. TTM and Sedatives
2.3. Data Collection
2.4. Measurement of ICP and QA
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
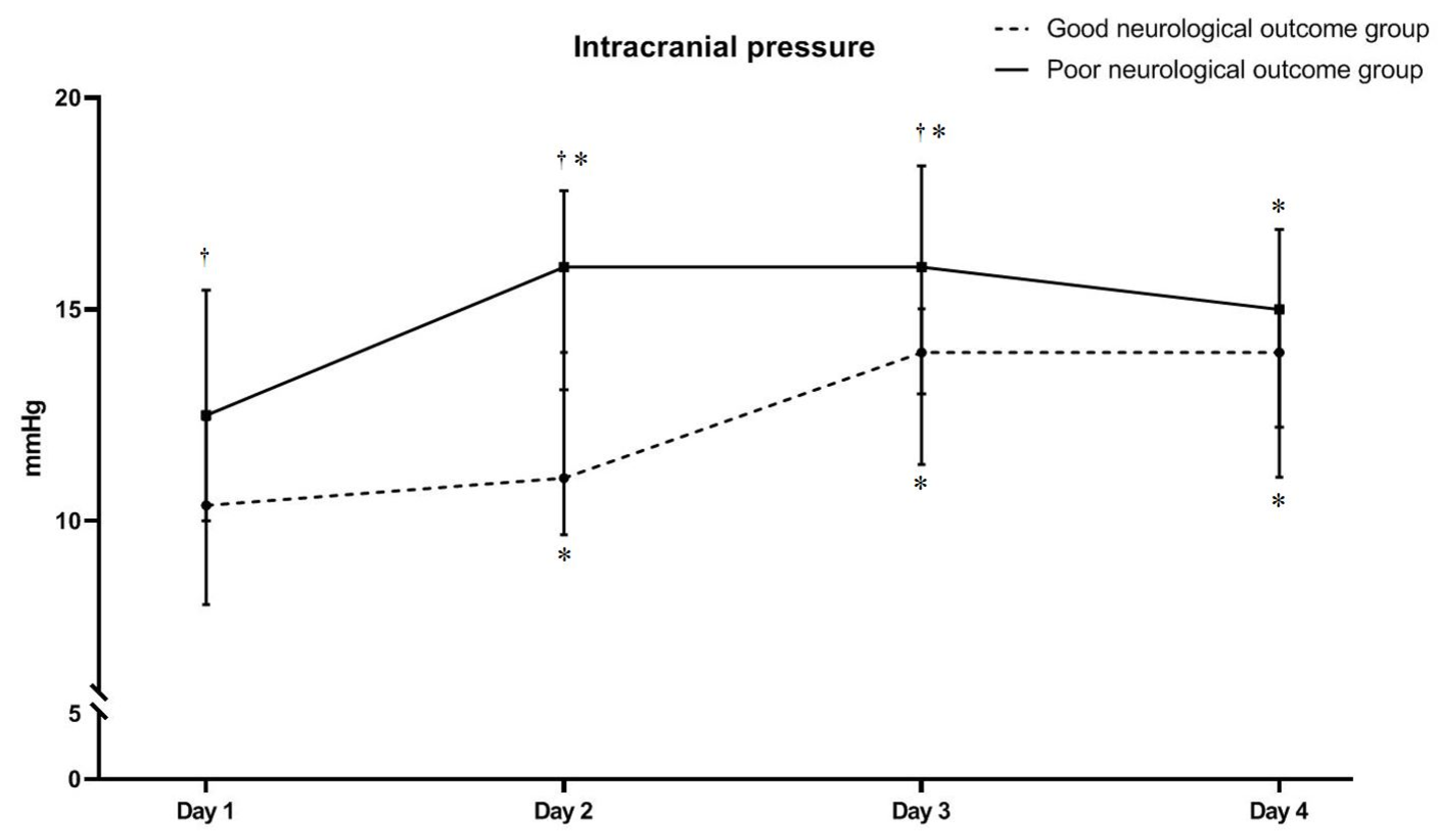
3.2. The Relationship between ICP and Neurological Outcome Groups
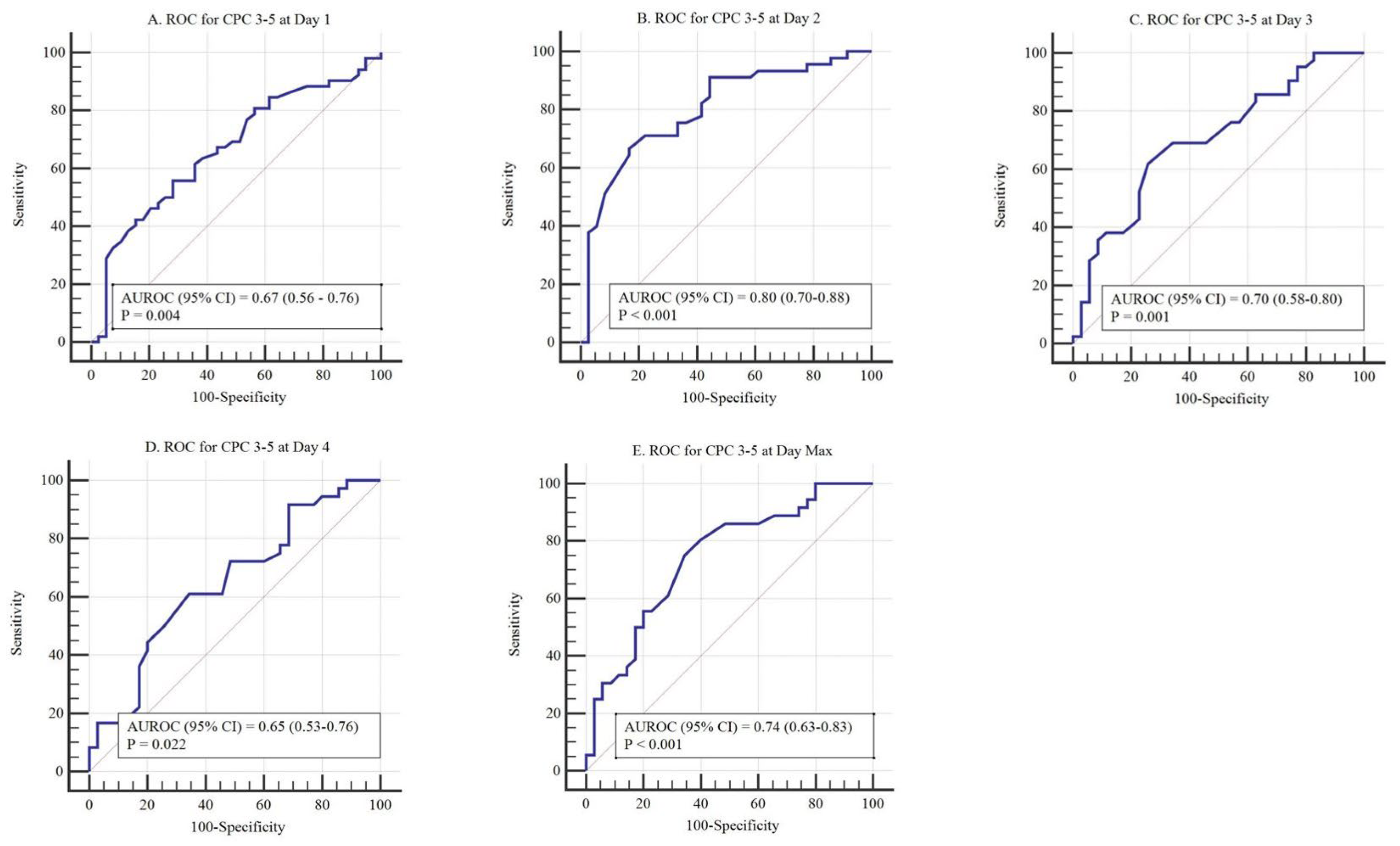
3.3. The Relationship between QA and Neurological Outcome Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2019 Update: A Report from the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Rungta, R.L.; Choi, H.B.; Tyson, J.R.; Malik, A.; Dissing-Olesen, L.; Lin, P.J.C.; Cain, S.M.; Cullis, P.R.; Snutch, T.P.; MacVicar, B.A. The cellular mechanisms of neuronal swelling underlying cytotoxic edema. Cell 2015, 161, 610–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keijzer, H.M.; Hoedemaekers, C.W.E.; Meijer, F.J.A.; Tonino, B.A.R.; Klijn, C.J.M.; Hofmeijer, J. Brain imaging in comatose survivors of cardiac arrest: Pathophysiological correlates and prognostic properties. Resuscitation 2018, 133, 124–136. [Google Scholar] [CrossRef]
- Czosnyka, M.; Pickard, J.D. Monitoring and interpretation of intracranial pressure. J. Neurol. Neurosurg. Psychiatry 2004, 75, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Sekhon, M.S.; Griesdale, D.E.; Ainslie, P.N.; Gooderham, P.; Foster, D.; Czosnyka, M.; Robba, C.; Cardim, D. Intracranial pressure and compliance in hypoxic ischemic brain injury patients after cardiac arrest. Resuscitation 2019, 141, 96–103. [Google Scholar] [CrossRef] [PubMed]
- You, Y.; Park, J.; Min, J.; Yoo, I.; Jeong, W.; Cho, Y.; Ryu, S.; Lee, J.; Kim, S.; Cho, S.; et al. Relationship between time related serum albumin concentration, optic nerve sheath diameter, cerebrospinal fluid pressure, and neurological prognosis in cardiac arrest survivors. Resuscitation 2018, 131, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Cho, Y.; You, Y.; Min, J.H.; Jeong, W.; Ahn, H.J.; Kang, C.; Yoo, I.; Ryu, S.; Lee, J.; et al. Optimal timing to measure optic nerve sheath diameter as a prognostic predictor in post-cardiac arrest patients treated with targeted temperature management. Resuscitation 2019, 143, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.; Min, J.H.; Park, J.S.; You, Y.; Yoo, I.; Cho, Y.C.; Jeong, W.; Ahn, H.J.; Ryu, S.; Lee, J.; et al. Relationship between optic nerve sheath diameter measured by magnetic resonance imaging, intracranial pressure, and neurological outcome in cardiac arrest survivors who underwent targeted temperature management. Resuscitation 2019, 145, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Jeon, G.R.; Ahn, H.J.; Park, J.S.; Yoo, I.; You, Y.; Cho, Y.C.; Jeong, W.; Kang, C.; Lee, B.K. The Association between Neurological Prognosis and the Degree of Blood-Brain Barrier Disruption in Cardiac Arrest Survivors Who Underwent Target Temperature Management. Neurocrit. Care epub ahead of print. 2021. [Google Scholar] [CrossRef]
- Nolan, J.P.; Sandroni, C.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: Post-resuscitation care. Intensive Care Med. 2021, 47, 369–421. [Google Scholar] [CrossRef]
- Lee, D.H.; Lee, S.H.; Oh, J.H.; Cho, I.S.; Lee, Y.H.; Han, C.; Choi, W.J.; Sohn, Y.D.; KORHN Investigators. Optic nerve sheath diameter measured using early unenhanced brain computed tomography shows no correlation with neurological outcomes in patients undergoing targeted temperature management after cardiac arrest. Resuscitation 2018, 128, 144–150. [Google Scholar] [CrossRef]
- Cardim, D.; Griesdale, D.E.; Ainslie, P.N.; Robba, C.; Calviello, L.; Czosnyka, M.; Smielewski, P.; Sekhon, M.S. A comparison of non-invasive versus invasive measures of intracranial pressure in hypoxic ischaemic brain injury after cardiac arrest. Resuscitation 2019, 137, 221–228. [Google Scholar] [CrossRef]
- Son, S.H.; Park, J.S.; Yoo, I.S.; You, Y.H.; Min, J.H.; Jeong, W.J.; Cho, Y.C.; Cho, S.U.; Oh, S.K.; Ahn, H.J.; et al. Usefulness of Intracranial Pressure and Mean Arterial Pressure for Predicting Neurological Prognosis in Cardiac Arrest Survivors Who Undergo Target Temperature Management. Hypothermia Temp. Manag. 2020, 10, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Hifumi, T.; Kawakita, K.; Yoda, T.; Okazaki, T.; Kuroda, Y. Association of brain metabolites with blood lactate and glucose levels with respect to neurological outcomes after out-of-hospital cardiac arrest: A preliminary microdialysis study. Resuscitation 2017, 110, 26–31. [Google Scholar] [CrossRef]
- Naito, H.; Isotani, E.; Callaway, C.W.; Hagioka, S.; Morimoto, N. Intracranial Pressure Increases During Rewarming Period After Mild Therapeutic Hypothermia in Postcardiac Arrest Patients. Target. Temp. Manag. 2016, 6, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Lenfeldt, N.; Koskinen, L.O.; Bergenheim, A.T.; Malm, J.; Eklund, A. CSF pressure assessed by lumbar puncture agrees with intracranial pressure. Neurology 2007, 68, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; You, Y.; Min, J.H.; Yoo, I.; Jeong, W.; Cho, Y.; Ryu, S.; Lee, J.; Kim, S.W.; Cho, S.U.; et al. Study on the timing of severe blood-brain barrier disruption using cerebrospinal fluid-serum albumin quotient in post cardiac arrest patients treated with targeted temperature management. Resuscitation 2019, 135, 118–123. [Google Scholar] [CrossRef]
- Blyth, B.J.; Farhavar, A.; Gee, C.; Hawthorn, B.; He, H.; Nayak, A.; Stöcklein, V.; Bazarian, J.J. Validation of serum markers for blood-brain barrier disruption in traumatic brain injury. J. Neurotrauma 2009, 26, 1497–1507. [Google Scholar] [CrossRef]
- Nordmark, J.; Rubertsson, S.; Mörtberg, E.; Nilsson, P.; Enblad, P. Intracerebral monitoring in comatose patients treated with hypothermia after a cardiac arrest. Acta Anaesthesiol. Scand. 2009, 53, 289–298. [Google Scholar] [CrossRef]
- Hayman, E.G.; Patel, A.P.; Kimberly, W.T.; Sheth, K.N.; Simard, J.M. Cerebral Edema after Cardiopulmonary Resuscitation: A Therapeutic Target Following Cardiac Arrest? Neurocrit. Care 2018, 28, 276–287. [Google Scholar] [CrossRef]
- Todd, M.M. Hyperosmolar therapy and the brain: A hundred years of hard-earned lessons. Anesthesiology 2013, 118, 777–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murad, A.; Ghostine, S.; Colohan, A.R. Role of controlled lumbar CSF drainage for ICP control in aneurysmal SAH. Acta Neurochir. Suppl. 2011, 110 Pt 2, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Tuettenberg, J.; Czabanka, M.; Horn, P.; Woitzik, J.; Barth, M.; Thomé, C.; Vajkoczy, P.; Schmiedek, P.; Muench, E. Clinical evaluation of the safety and efficacy of lumbar cerebrospinal fluid drainage for the treatment of refractory increased intracranial pressure. J. Neurosurg. 2009, 110, 1200–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Cohort (n = 91) | Good Neurological Outcome (n = 40) | Poor Neurological Outcome (n = 51) | p-Value |
|---|---|---|---|---|
| Age, years, median (IQR) | 57.0 (41.0–69.0) | 57.0 (39.5–68.0) | 57.0 (42.0–72.0) | 0.384 |
| Male sex, n (%) | 67 (73.6) | 32 (80.0) | 35 (68.6) | 0.242 |
| Charlson Comorbidity Index score, median (IQR) | 1.0 (0.0–5.0) | 2.0 (0.0–5.0) | 1.0 (0.0–5.0) | 0.609 |
| Arrest characteristics | ||||
| Witness, n (%) | 62 (68.1) | 32 (80) | 30 (58.8) | 0.032 |
| Location of arrest, public place, n (%) | 27 (29.7) | 13 (14.3) | 14 (15.4) | 0.256 |
| Bystander CPR, n (%) | 63 (69.2) | 33 (82.5) | 30 (58.8) | 0.016 |
| Shockable rhythm, n (%) | 26 (28.6) | 22 (55.0) | 4 (7.8) | <0.001 |
| Cardiac etiology, n (%) | 36 (39.6) | 24 (60.0) | 12 (23.5) | 0.001 |
| No flow time, min, median (IQR) | 2.0 (0–12.5) | 1.0 (0.0–5.0) | 6.5 (0.0–23.3) | 0.003 |
| Low flow time, min, median (IQR) | 19.0 (9.0–29.5) | 14.0 (8.0–19.0) | 27.5 (15.0–43.0) | <0.001 |
| Laboratory parameters immediately after ROSC | ||||
| pH, median (IQR) | 7.14 (7.00–7.32) | 7.14 (6.97–7.30) | 7.15 (7.00–7.30) | 0.542 |
| Lactate, mmol l−1, median (IQR) | 6.20 (3.60–10.80) | 4.50 (1.70–10.40) | 7.30 (4.08–11.00) | 0.038 |
| Albumin, g dl−1, median (IQR) | 3.2 (2.9–3.6) | 3.4 (2.7–3.7) | 3.1 (2.7–3.6) | 0.005 |
| Creatinine, mg dl−1, median (IQR) | 1.35 (1.02–7.11) | 1.56 (1.12–7.47) | 1.25 (0.96–2.65) | 0.786 |
| Troponin I, ng ml−1, median (IQR) | 0.66 (0.06–39.9) | 0.27 (0.03–30.4) | 5.53 (0.11–82.90) | 0.037 |
| Procalcitonin, ng ml−1, median (IQR) | 0.26 (0.05–0.66) | 0.19 (0.05–0.60) | 0.26 (0.05–2.01) | 0.092 |
| SOFA score | 10.0 (8.0–12.0) | 9.0 (7.5–11.0) | 11.0 (9.0–12.0) | 0.018 |
| Time-weighted average 24 h from ROSC, mmHg | ||||
| PaO2 | 142.2 (124.7–158.3) | 140.9 (116.2–157.3) | 142.9 (129.1–162.2) | 0.111 |
| PaCO2 | 39.2 (35.4–42.7) | 41.0 (36.7–43.5) | 38.2 (33.8–42.0) | 0.06 |
| MAP | 94.0 (86.6–99.9) | 98.5 (94.2–101.5) | 90.5 (82.1–95.9) | <0.001 |
| Time-weighted average 72 h from ROSC | ||||
| NMBA (Nimbex®), μg kg−1 min−1 | 3.00 (3.00–3.97) | 3.00 (3.00–4.00) | 3.00 (3.00–3.00) | 0.032 |
| Sedative (Midazolam®), mg kg−1 h−1 | 0.10 (0.06–0.15) | 0.10 (0.06–0.12) | 0.10 (0.05–0.19) | 0.666 |
| ROSC to LP time, hour (IQR) | 4.5 (3.2–6.0) | 4.1 (3.0–5.9) | 4.7 (4.0–6.0) | 0.150 |
| ROSC to induction time (33 °C), hour (IQR) | 6.0 (4.7–7.5) | 5.9 (4.6–8.1) | 5.9 (4.8–7.4) | 0.962 |
| Group | PGEE | Post Hoc Analysis | ||
|---|---|---|---|---|
| Bonferroni | ||||
| Day 1–2 | Day 2–3 | Day 3–4 | ||
| Good neurological outcome | <0.001 | 0.282 | 0.001 | 1.000 |
| Poor neurological outcome | <0.001 | 0.001 | 1.000 | 1.000 |
| Time | Cohort | Neurological Outcome at 3 Months after ROSC | p-Value | |
|---|---|---|---|---|
| Good | Poor | |||
| Day 1 | 0.008 (0.006–0.014), 91 * | 0.007 (0.005–0.009), 40 * | 0.01 (0.007–0.018), 51 * | 0.001 ** |
| Day 2 | 0.018 (0.007–0.054), 81 * | 0.008 (0.005–0.017), 36 * | 0.03 (0.015–0.137), 45 * | <0.001 ** |
| Day 3 | 0.015 (0.007–0.043), 78 * | 0.007 (0.006–0.013), 35 * | 0.029 (0.015–0.096), 43 * | <0.001 ** |
| Day 4 | 0.016 (0.007–0.031), 71 * | 0.007 (0.005–0.013), 35 * | 0.025 (0.016–0.068), 36 * | <0.001 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, H.; Kang, C.; Park, J.; You, Y.; In, Y.; Min, J.; Jeong, W.; Cho, Y.; Ahn, H.; Kim, D. Intracranial Pressure Patterns and Neurological Outcomes in Out-of-Hospital Cardiac Arrest Survivors after Targeted Temperature Management: A Retrospective Observational Study. J. Clin. Med. 2021, 10, 5697. https://doi.org/10.3390/jcm10235697
Song H, Kang C, Park J, You Y, In Y, Min J, Jeong W, Cho Y, Ahn H, Kim D. Intracranial Pressure Patterns and Neurological Outcomes in Out-of-Hospital Cardiac Arrest Survivors after Targeted Temperature Management: A Retrospective Observational Study. Journal of Clinical Medicine. 2021; 10(23):5697. https://doi.org/10.3390/jcm10235697
Chicago/Turabian StyleSong, Hogul, Changshin Kang, Jungsoo Park, Yeonho You, Yongnam In, Jinhong Min, Wonjoon Jeong, Yongchul Cho, Hongjoon Ahn, and Dongil Kim. 2021. "Intracranial Pressure Patterns and Neurological Outcomes in Out-of-Hospital Cardiac Arrest Survivors after Targeted Temperature Management: A Retrospective Observational Study" Journal of Clinical Medicine 10, no. 23: 5697. https://doi.org/10.3390/jcm10235697