
Frequency, Mortality, and Predictors of Adverse Outcomes for Endocarditis in Patients with Congenital Heart Disease: Results of a Nationwide Analysis including 2512 Endocarditis Cases

 , ,
, ,
Abstract
:1. Introduction
2. Methods
Statistical Analysis
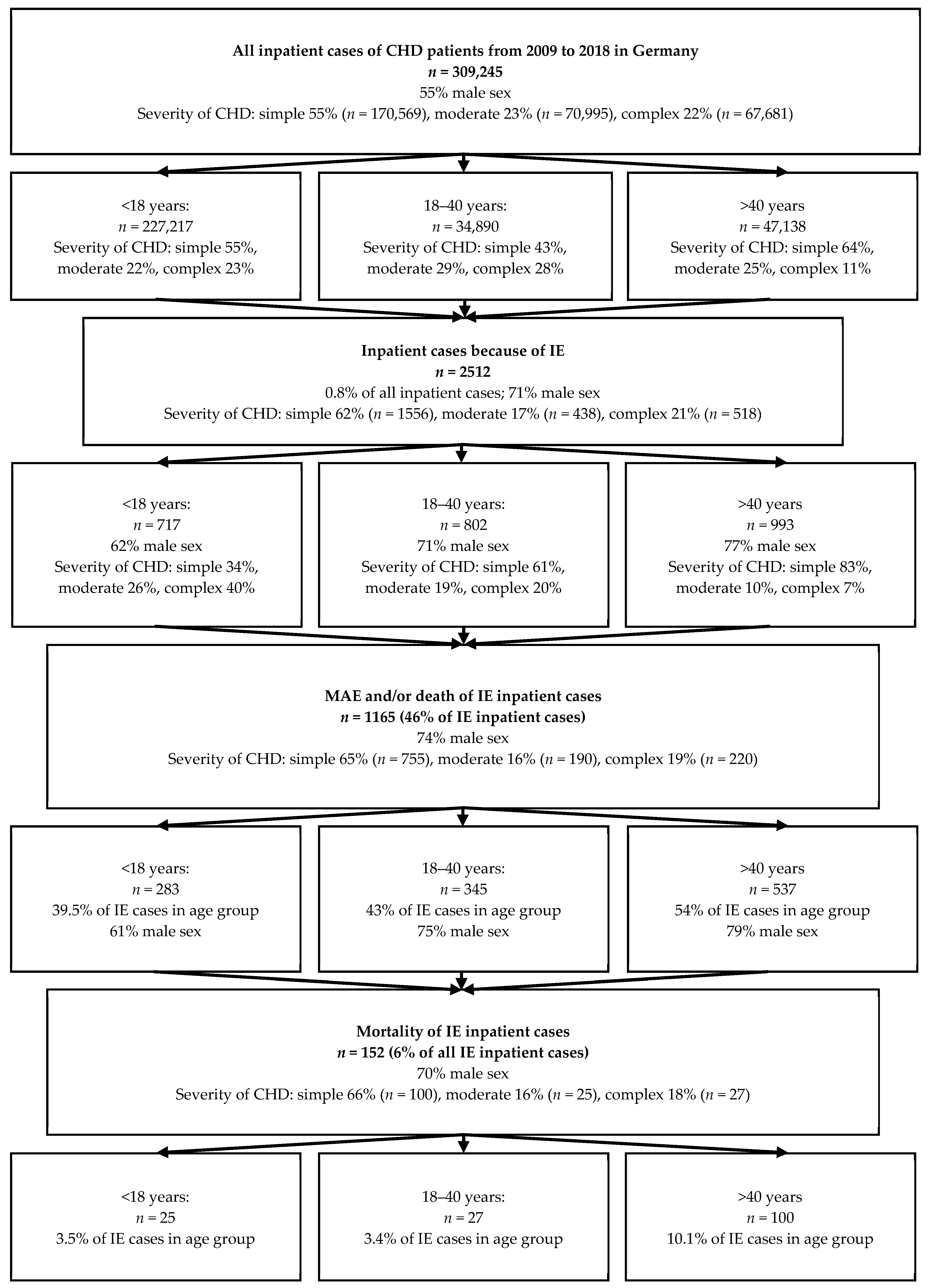
3. Results
4. Discussion
Strengths and Limitations of the Current Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [PubMed]
- Baltimore, R.S.; Gewitz, M.; Baddour, L.M.; Beerman, L.B.; Jackson, M.A.; Lockhart, P.B.; Pahl, E.; Schutze, G.E.; Shulman, S.T.; Willoughby, R., Jr. Infective Endocarditis in Childhood: 2015 Update: A Scientific Statement from the American Heart Association. Circulation 2015, 132, 1487–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgartner, H.; De Backer, J.; Babu-Narayan, S.V.; Budts, W.; Chessa, M.; Diller, G.P.; Lung, B.; Kluin, J.; Lang, I.M.; Meijboom, F.; et al. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur. Heart J. 2021, 42, 563–645. [Google Scholar] [CrossRef] [PubMed]
- Diller, G.P.; Arvanitaki, A.; Opotowsky, A.R.; Jenkins, K.; Moons, P.; Kempny, A.; Tandon, A.; Redington, A.; Khairy, P.; Mital, S.; et al. Lifespan Perspective on Congenital Heart Disease Research: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 77, 2219–2235. [Google Scholar] [CrossRef]
- Diller, G.-P.; Kempny, A.; Alonso-Gonzalez, R.; Swan, L.; Uebing, A.; Li, W.; Babu-Narayan, S.; Wort, S.J.; Dimopoulos, K.; Gatzoulis, M.A. Survival Prospects and Circumstances of Death in Contemporary Adult Congenital Heart Disease Patients Under Follow-Up at a Large Tertiary Centre. Circulation 2015, 132, 2118–2125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diller, G.-P.; Orwat, S.; Lammers, A.E.; Radke, R.M.; De-Torres-Alba, F.; Schmidt, R.; Marschall, U.; Bauer, U.M.; Enders, D.; Bronstein, L.; et al. Lack of specialist care is associated with increased morbidity and mortality in adult congenital heart disease: A population-based study. Eur. Heart J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Kuijpers, J.M.; Koolbergen, D.R.; Groenink, M.; Peels, K.C.; Reichert, C.L.; Post, M.C.; Bosker, H.A.; Wajon, E.M.; Zwinderman, A.H.; Mulder, B.J.; et al. Incidence, risk factors, and predictors of infective endocarditis in adult congenital heart disease: Focus on the use of prosthetic material. Eur. Heart J. 2017, 38, 2048–2056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Somerville, J. Infective endocarditis in the grown-up congenital heart (GUCH) population. Eur. Heart J. 1998, 19, 166–173. [Google Scholar] [CrossRef] [Green Version]
- Tutarel, O.; Alonso-Gonzalez, R.; Montanaro, C.; Schiff, R.; Uribarri, A.; Kempny, A.; Grübler, M.R.; Uebing, A.; Swan, L.; Diller, G.-P.; et al. Infective endocarditis in adults with congenital heart disease remains a lethal disease. Heart (Br. Card. Soc.) 2018, 104, 161–165. [Google Scholar] [CrossRef]
- Vincent, L.L.; Otto, C.M. Infective Endocarditis: Update on Epidemiology, Outcomes, and Management. Curr. Cardiol. Rep. 2018, 20, 86. [Google Scholar] [CrossRef]
- Webb, G.; Williams, R. Care of the Adult with Congenital Heart Disease. In Proceedings of the 32nd Bethesda Conference, Bethesda, ML, USA, 2–3 October 2000; pp. 1161–1198. [Google Scholar]
- Hoen, B.; Duval, X. Clinical practice. Infective endocarditis. N. Engl. J. Med. 2013, 368, 1425–1433. [Google Scholar] [CrossRef]
- Fortún, J.; Centella, T.; Martín-Dávila, P.; Lamas, M.J.; Pérez-Caballero, C.; Fernández-Pineda, L.; Otheo, E.; Cobo, J.; Navas, E.; Pintado, V.; et al. Infective endocarditis in congenital heart disease: A frequent community-acquired complication. Infection 2013, 41, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.J.; Enders, D.; Wasmer, K.; Marschall, U.; Baumgartner, H.; Diller, G.P. Impact of specialized electrophysiological care on the outcome of catheter ablation for supraventricular tachycardias in adults with congenital heart disease: Independent risk factors and gender aspects. Heart Rhythm. 2021, 18, 1852–1859. [Google Scholar] [CrossRef]
- Bauer, U.M.M.; Helm, P.C.; Diller, G.P.; Asfour, B.; Schlensak, C.; Schmitt, K.; Ewert, O.; Tutarel, O. Are adults with congenital heart disease informed about their risk for infective endocarditis and treated in accordance to current guidelines? Int. J. Cardiol. 2017, 245, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Gatzoulis, M.A. Adult congenital heart disease: Education, education, education. Nat. Clin. Pract. Cardiovasc. Med. 2006, 3, 2–3. [Google Scholar] [CrossRef]
- Kantoch, M.J.; Collins-Nakai, R.L.; Medwid, S.; Ungstad, E.; Taylor, D.A. Adult patients’ knowledge about their congenital heart disease. Can. J. Cardiol. 1997, 13, 641–645. [Google Scholar] [PubMed]
- Moons, P.; De Volder, E.; Budts, W.; De Geest, S.; Elen, J.; Waeytens, K.; Gewillig, M. What do adult patients with congenital heart disease know about their disease, treatment, and prevention of complications? A call for structured patient education. Heart (Br. Card. Soc.) 2001, 86, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Lammers, A.E.; Helm, P.C.; Bauer, U.M.; van Huelsen, A.-K.; Schneider, H.; Baumgartner, H.; Diller, G.-P. Optimizing Care for Adults with Congenital Heart Disease: Results of a Conjoint Analysis Based on a Nationwide Sample of Patients Included in the German National Register. J. Clin. Med. 2021, 10, 3483. [Google Scholar] [CrossRef]
- Eleyan, L.; Khan, A.A.; Musollari, G.; Chandiramani, A.S.; Shaikh, S.; Salha, A.; Tarmahomed, A.; Harky, A. Infective endocarditis in paediatric population. Eur. J. Pediatr. 2021, 180, 3089–3100. [Google Scholar] [CrossRef]
- Jortveit, J.; Eskedal, L.; Klcovansky, J.; Dohlen, G.; Holmstrom, H. Prevalence of infective endocarditis in children. Tidsskr. Nor. Laegeforen. 2019, 139. [Google Scholar] [CrossRef]
- Mahony, M.; Lean, D.; Pham, L.; Horvath, R.; Suna, J.; Ward, C.; Veerappan, S.; Versluis, K.; Nourse, C. Infective Endocarditis in Children in Queensland, Australia: Epidemiology, Clinical Features and Outcome. Pediatr. Infect. Dis. J. 2021, 40, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Chen, Y.; Xiao, T.; Niu, T.; Shi, Q.; Xiao, Y. Epidemiology and risk factors of infective endocarditis in a tertiary hospital in China from 2007 to 2016. BMC Infect Dis. 2020, 20, 428. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Munoz, D.R.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Condition | ICD-10/OPS Codes |
|---|---|
| Identification and classification of CHD | |
| Complex CHD | |
| Univentricular heart | Q20.1, Q20.2, Q20.4, Q22.6, Q23.4, (Q22.0 andNOT Q21.0) |
| Eisenmenger syndrome | I27.8 and additional Q code, Q21.88 |
| Transposition of the great arteries | Q20.3, Q20.5, Q25.8, Q25.9 |
| Other complex CHD lesions | Q20.0, Q26.2 |
| Moderate complexity CHD | |
| Tetralogy of Fallot including pulmonary atresia with ventricular septal defect | Q21.3, Q21.80, (Q22.0 and Q21.0) |
| Ebstein anomaly | Q22.5 |
| Aortic coarctation/interrupted aortic arch | Q25.1, Q25.2 |
| Atrioventricular septal defect | Q21.2 |
| Partial anomalous pulmonary venous drainage | Q26.3, Q26.4 |
| Simple CHD | |
| Ventricular septal defect | Q21.0 |
| Patent ductus arteriosus | Q25.0 |
| Valvular lesions | Q22.1, Q22.2, Q22.3, Q22.4, Q22.8, Q22.9, Q23.0, Q23.1, Q23.2, Q23.3 |
| Endocarditis | I33.-, I38, I39.- |
| Major adverse events: | |
| Death or | |
| Acute myocardial infarction | I21.- |
| Recurring myocardial infarction | I22.- |
| Pulmonary embolism | I26.-: O88.- |
| Resuscitation | 8–77 |
| Sepsis | A40.-. A41.-, B36.- |
| Stroke, cerebrovascular bleeding | I60–I69 |
| Renal dialysis Intubation/Ventilation | 8-853, 8-854, 8-855, 8-857 8-70, 8-71 |
| Operations | OPS-5-350, OPS-5-351, OPS-5-352, OPS-5-353, OPS-5-354, OPS-5-358 |
| All IE Cases > 18 Years of Age (with and without CHD) (Endpoint In-Hospital Mortality) | n = 153,776 | ||
|---|---|---|---|
| Parameter | OR | 95% CI | p-Value |
| Age (years) | 1.02 | 1.02–1.02 | <0.0001 |
| Male sex | 0.92 | 0.89–0.94 | <0.0001 |
| Simple complexity (vs. non-CHD) | 0.74 | 0.59–0.92 | 0.008 |
| Moderate complexity (vs. non-CHD) | 0.75 | 0.46–1.22 | 0.25 |
| High complexity (vs. non-CHD) | 0.91 | 0.55–1.52 | 0.72 |
| Diabetes | 1.20 | 1.17–1.24 | <0.0001 |
| Arterial hypertension | 0.56 | 0.55–0.58 | <0.0001 |
| Heart failure | 1.58 | 1.53–1.62 | <0.0001 |
| Renal dysfunction | 3.35 | 3.25–3.46 | <0.0001 |
| Coronary heart disease | 0.99 | 0.96–1.02 | 0.50 |
| Oncologic disease | 1.66 | 1.58–1.74 | <0.0001 |
| Lung disease | 1.10 | 1.05–1.14 | <0.0001 |
| IE cases > 18 Yars of Age with CHD (Endpoint In-Hospital Mortality) | n = 1795 | ||
|---|---|---|---|
| Parameter | OR | 95% CI | p-Value |
| Age (years) | 1.03 | 1.02–1.05 | <0.0001 |
| Male sex | 0.68 | 0.44–1.05 | 0.085 |
| Moderate complexity (vs. simple) | 0.97 | 0.55–1.72 | 0.91 |
| High complexity (vs. simple) | 1.42 | 0.78–2.59 | 0.25 |
| Diabetes | 1.04 | 0.59–1.84 | 0.89 |
| Arterial hypertension | 0.51 | 0.32–0.80 | 0.003 |
| Heart failure | 1.97 | 1.33–2.93 | 0.0008 |
| Renal dysfunction | 3.93 | 2.62–5.91 | <0.0001 |
| Coronary heart disease | 1.42 | 0.88–2.31 | 0.15 |
| Oncologic disease | 1.77 | 0.74–4.21 | 0.20 |
| Lung disease | 0.91 | 0.42–1.94 | 0.80 |
| All IE Cases < 18 Years of Age (with and without CHD) (Endpoint In-Hospital Mortality) | n = 1978 | ||
|---|---|---|---|
| Parameter | OR | 95% CI | p-Value |
| Age (years) | 0.97 | 0.92–1.02 | 0.18 |
| Male sex | 1.47 | 0.77–2.79 | 0.24 |
| Simple complexity (vs. non-CHD) | 1.54 | 0.64–3.67 | 0.33 |
| Moderate complexity (vs. non-CHD) | 1.28 | 0.48–3.41 | 0.62 |
| High complexity (vs. non-CHD) | 1.59 | 0.7–3.6 | 0.27 |
| Diabetes | 2.76 | 0.19–40.29 | 0.46 |
| Arterial hypertension | 0.27 | 0.03–2.17 | 0.22 |
| Heart failure | 5.76 | 3.07–10.78 | <0.0001 |
| Renal dysfunction | 9.27 | 3.97–21.62 | <0.0001 |
| Coronary heart disease | 24.57 | 3.35–180.07 | 0.002 |
| Oncologic disease | 10.33 | 3.25–32.85 | <0.0001 |
| IE cases < 18 Years of Age with CHD (Endpoint In-Hospital Mortality) | n = 717 | ||
|---|---|---|---|
| Parameter | OR | 95% CI | p-Value |
| Age (years) | 0.92 | 0.85–1.00 | 0.049 |
| Male sex | 2.26 | 0.83–6.20 | 0.11 |
| Moderate complexity (vs. simple) | 0.95 | 0.30–3.05 | 0.93 |
| High complexity (vs. simple) | 1.07 | 0.38–2.97 | 0.90 |
| Arterial hypertension | 0.73 | 0.09–6.31 | 0.78 |
| Heart failure | 4.32 | 1.83–10.21 | 0.0009 |
| Renal dysfunction | 8.26 | 2.19–31.15 | 0.0018 |
| Coronary heart disease | 66.47 | 5.86–753.88 | 0.0007 |
| All IE Cases (Children and Adults, with and without CHD) (Endpoint MAE or Death) | n = 155,754 | ||
|---|---|---|---|
| Parameter | OR | 95% CI | p-Value |
| Age (years) | 1.00 | 1.00–1.00 | 0.006 |
| Male sex | 1.12 | 1.09–1.14 | <0.0001 |
| Simple complexity (vs. non-CHD) | 1.04 | 0.93–1.15 | 0.51 |
| Moderate complexity (vs. non-CHD) | 0.88 | 0.72–1.07 | 0.20 |
| High complexity (vs. non-CHD) | 0.89 | 0.74–1.07 | 0.21 |
| Diabetes | 1.35 | 1.32–1.38 | <0.0001 |
| Arterial hypertension | 0.85 | 0.83–0.87 | <0.0001 |
| Heart failure | 1.54 | 1.50–1.57 | <0.0001 |
| Renal dysfunction | 2.95 | 2.88–3.02 | <0.0001 |
| Coronary heart disease | 1.26 | 1.23–1.29 | <0.0001 |
| Oncologic disease | 1.22 | 1.17–1.27 | <0.0001 |
| Lung disease | 1.07 | 1.03–1.11 | 0.0003 |
| All IE Cases with CHD (Children and Adults) (Endpoint MAE or Death) | n = 2512 | ||
|---|---|---|---|
| Parameter | OR | 95% CI | p-Value |
| Age (years) | 0.99 | 0.99–1.00 | 0.03 |
| Male sex | 1.13 | 0.94–1.37 | 1.20 |
| Moderate complexity (vs. simple) | 0.89 | 0.70–1.14 | 0.36 |
| High complexity (vs. simple) | 0.93 | 0.74–1.18 | 0.56 |
| Diabetes | 1.45 | 0.96–2.19 | 0.07 |
| Arterial hypertension | 1.12 | 0.89–1.41 | 0.35 |
| Heart failure | 2.22 | 1.83–2.69 | <0.0001 |
| Renal dysfunction | 4.39 | 3.39–5.69 | <0.0001 |
| Coronary artery disase | 1.90 | 1.37–2.62 | 0.0001 |
| Oncologic disease | 2.43 | 1.06–5.59 | 0.036 |
| Lung disease | 1.75 | 1.11–2.77 | 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maser, M.; Freisinger, E.; Bronstein, L.; Köppe, J.; Orwat, S.; Kaleschke, G.; Baumgartner, H.; Diller, G.-P.; Lammers, A. Frequency, Mortality, and Predictors of Adverse Outcomes for Endocarditis in Patients with Congenital Heart Disease: Results of a Nationwide Analysis including 2512 Endocarditis Cases. J. Clin. Med. 2021, 10, 5071. https://doi.org/10.3390/jcm10215071
Maser M, Freisinger E, Bronstein L, Köppe J, Orwat S, Kaleschke G, Baumgartner H, Diller G-P, Lammers A. Frequency, Mortality, and Predictors of Adverse Outcomes for Endocarditis in Patients with Congenital Heart Disease: Results of a Nationwide Analysis including 2512 Endocarditis Cases. Journal of Clinical Medicine. 2021; 10(21):5071. https://doi.org/10.3390/jcm10215071
Chicago/Turabian StyleMaser, Maarja, Eva Freisinger, Leo Bronstein, Jeanette Köppe, Stefan Orwat, Gerrit Kaleschke, Helmut Baumgartner, Gerhard-Paul Diller, and Astrid Lammers. 2021. "Frequency, Mortality, and Predictors of Adverse Outcomes for Endocarditis in Patients with Congenital Heart Disease: Results of a Nationwide Analysis including 2512 Endocarditis Cases" Journal of Clinical Medicine 10, no. 21: 5071. https://doi.org/10.3390/jcm10215071