
Discrepant End-Tidal Concentrations of Sevoflurane at the Same A-Line Autoregressive Index Level during Induction of General Anesthesia: An Observational Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Anesthetic Procedures
2.3. Data Acquisition
2.4. Data Analysis
3. Results
3.1. Participant Recruitment
3.2. General Characteristics of Participants
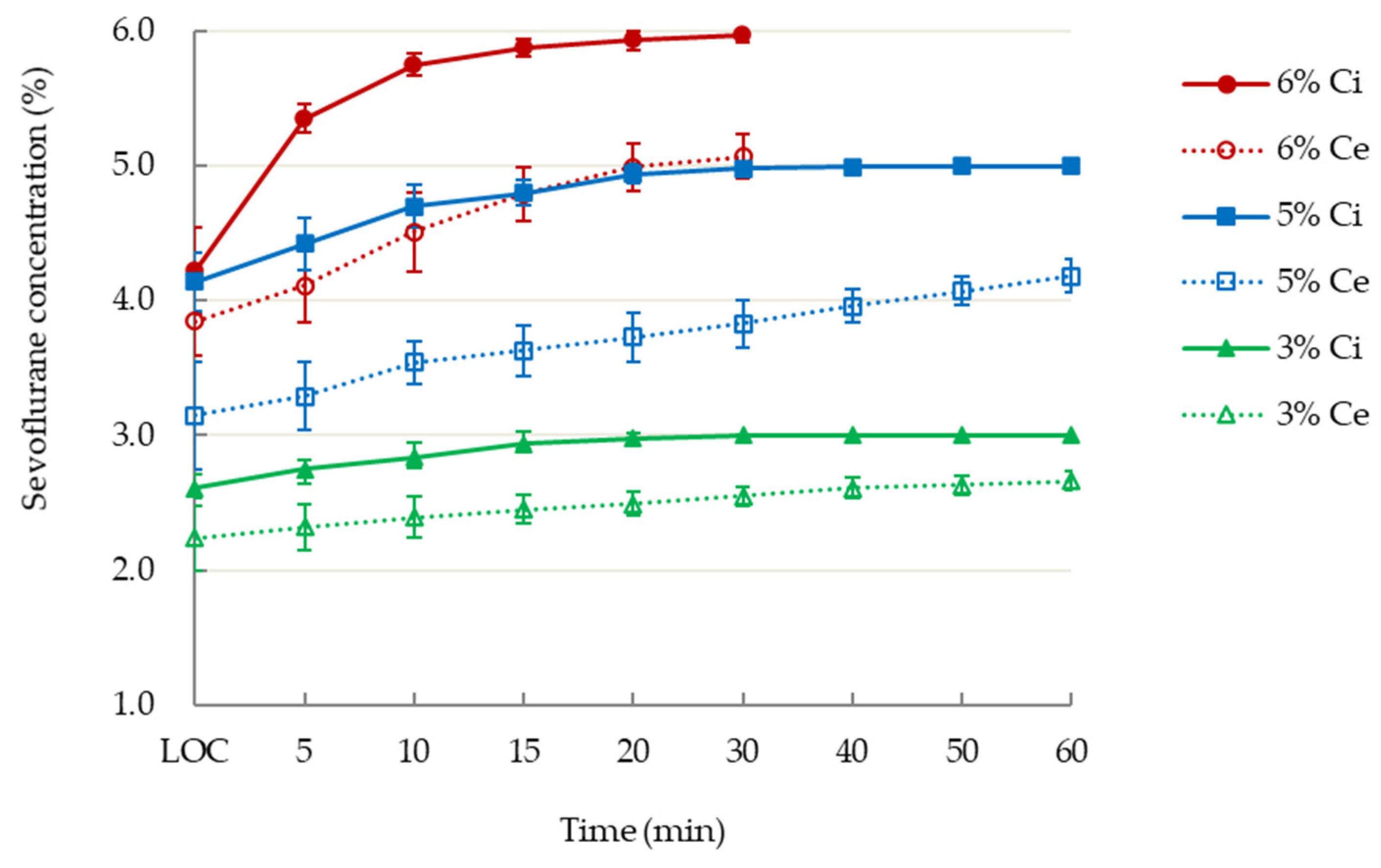
3.3. Iinspiratory and End-Tidal Concentrations of Sevoflurane
3.4. AAI Values and Sevoflurane Concentrations
3.5. Hemodynamic Variables during Induction
4. Discussion
4.1. Main Findings
4.2. Higher Inspiratory and End-Tidal Concentrations at the Same AAI Values during Wash-In
4.3. EEG Processing for Adjustment of Anesthesia Depth
4.4. AAI Values and MAC of Sevoflurane
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bell, S.L.; Smith, D.C.; Allen, R.; Lutman, M.E. Recording the middle latency response of the auditory evoked potential as a measure of depth of anaesthesia. A technical note. Br. J. Anaesth. 2004, 92, 442–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horn, B.; Pilge, S.; Kochs, E.F.; Stockmanns, G.; Hock, A.; Schneider, G. A combination of electroencephalogram and auditory evoked potentials separates different levels of anesthesia in volunteers. Anesth. Analg. 2009, 108, 1512–1521. [Google Scholar] [CrossRef] [PubMed]
- Feuerecker, M.; Lenk, M.; Flake, G.; Edelmann-Gahr, V.; Wiepcke, D.; Hornuss, C.; Daunderer, M.; Müller, H.H.; Kuhnle, G.E. Effects of increasing sevoflurane MAC levels on mid-latency auditory evoked potentials in infants, schoolchildren, and the elderly. Br. J. Anaesth. 2011, 107, 726–734. [Google Scholar] [CrossRef] [Green Version]
- Kreuer, S.; Bruhn, J.; Larsen, R.; Buchinger, H.; Wilhelm, W. A-line, bispectral index, and estimated effect-site concentrations: A prediction of clinical end-points of anesthesia. Anesth. Analg. 2006, 102, 1141–1146. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.E.; Barr, G.; Assareh, H.; Jakobsson, J. The AAI index, the BIS index and end-tidal concentration during wash in and wash out of sevoflurane. Anaesthesia 2003, 58, 531–535. [Google Scholar] [CrossRef]
- Lu, C.C.; Tsai, C.S.; Ho, S.T.; Chueng, C.M.; Wang, J.J.; Wong, C.S.; Chang, S.Y.; Lin, C.Y. Pharmacokinetics of desflurane uptake into the brain and body. Anaesthesia 2004, 59, 216–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, C.C.; Tsai, C.S.; Ho, S.T.; Chen, W.Y.; Wong, C.S.; Wang, J.J.; Hu, O.Y.; Lin, C.Y. Pharmacokinetics of sevoflurane uptake into the brain and body. Anaesthesia 2003, 58, 951–956. [Google Scholar] [CrossRef]
- Lu, C.C.; Ho, S.T.; Wang, J.J.; Wong, C.S.; Hu, O.Y.; Chang, S.Y.; Lin, C.Y. Pharmacokinetics of isoflurane: Uptake in the brain. Pharmacology 2003, 69, 102–107. [Google Scholar] [CrossRef]
- Lu, C.C.; Lin, T.C.; Hsu, C.H.; Tsai, C.S.; Sheen, M.J.; Hu, O.Y.; Ho, S.T. Pharmacokinetics of sevoflurane elimination from respiratory gas and blood after coronary artery bypass grafting surgery. J. Anesth. 2014, 28, 873–879. [Google Scholar] [CrossRef]
- Lin, T.C.; Lu, C.C.; Hsu, C.H.; Wu, G.J.; Lee, M.S.; Ho, S.T. Duration effect of desflurane anesthesia and its awakening time and arterial concentration in gynecologic patients. Clinics 2013, 68, 1305–1311. [Google Scholar] [CrossRef]
- Lin, T.C.; Lu, C.C.; Hsu, C.H.; Su, H.Y.; Lee, M.S.; Ho, S.T. Arterial blood and end-tidal concentrations of sevoflurane during the emergence from anesthesia in gynecologic patients. Clinics 2015, 70, 196–201. [Google Scholar] [CrossRef]
- Lin, T.C.; Lu, C.C.; Hsu, C.H.; Pergolizz, J.V., Jr.; Chang, C.C.; Lee, M.S.; Ho, S.T. Awakening arterial blood and end-tidal concentrations of isoflurane in female surgical patients. Medicine 2016, 95, e4370. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.C.; Lin, T.C.; Hsu, C.H.; Yu, M.H.; Ku, C.H.; Chen, T.L.; Chen, R.M.; Ho, S.T. Hyperventilation accelerates rise in arterial blood concentrations of sevoflurane in gynecologic patients. J. Anesth. 2013, 27, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.C.; Lu, C.C.; Li, C.Y.; Chang, C.C.; Ho, S.T. Arterial blood concentration of sevoflurane during single-breath induction and tracheal intubation in gynecologic patients. J. Clin. Anesth. 2008, 20, 496–500. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.; Koshy, T. Monitoring devices for measuring the depth of anaesthesia—An overview. Indian J. Anaesth. 2007, 51, 365. [Google Scholar]
- Eger, E.I., 2nd; Saidman, L.J.; Brandstater, B. Minimum alveolar anesthetic concentration: A standard of anesthetic potency. Anesthesiology 1965, 26, 756–763. [Google Scholar] [CrossRef]
- Rehberg, B.; Bouillon, T.; Zinserling, J.; Hoeft, A. Comparative pharmacodynamic modeling of the electroencephalography-slowing effect of isoflurane, sevoflurane, and desflurane. Anesthesiology 1999, 91, 397–405. [Google Scholar] [CrossRef]
- Yasuda, N.; Targ, A.G.; Eger, E.I., 2nd. Solubility of I-653, sevoflurane, isoflurane, and halothane in human tissues. Anesth. Analg. 1989, 69, 370–373. [Google Scholar] [CrossRef]
- Jeleazcov, C.; Schneider, G.; Daunderer, M.; Scheller, B.; Schuttler, J.; Schwilden, H. The discriminant power of simultaneous monitoring of spontaneous electroencephalogram and evoked potentials as a predictor of different clinical states of general anesthesia. Anesth. Analg. 2006, 103, 894–901. [Google Scholar] [CrossRef]
- Alpiger, S.; Helbo-Hansen, H.S.; Jensen, E.W. Effect of sevoflurane on the mid-latency auditory evoked potentials measured by a new fast extracting monitor. Acta Anaesthesiol. Scand. 2002, 46, 252–256. [Google Scholar] [CrossRef]
- Ironfield, C.M.; Davidson, A.J. AEP-monitor/2 derived, composite auditory evoked potential index (AAI-1.6) and bispectral index as predictors of sevoflurane concentration in children. Paediatr. Anaesth. 2007, 17, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Philip, J.H. Gas Man—An example of goal oriented computer-assisted teaching which results in learning. Int. J. Clin. Monit. Comput. 1986, 3, 165–173. [Google Scholar] [CrossRef]
- Mapleson, W.W. Effect of age on MAC in humans: A meta-analysis. Br. J. Anaesth. 1996, 76, 179–185. [Google Scholar] [CrossRef]
- Eger, E.I., 2nd; Laster, M.J.; Gregory, G.A.; Katoh, T.; Sonner, J.M. Women appear to have the same minimum alveolar concentration as men: A retrospective study. Anesthesiology 2003, 99, 1059–1061. [Google Scholar] [CrossRef] [PubMed]
- Schwender, D.; Conzen, P.; Klasing, S.; Finsterer, U.; Poppel, E.; Peter, K. The effects of anesthesia with increasing end-expiratory concentrations of sevoflurane on midlatency auditory evoked potentials. Anesth. Analg. 1995, 81, 817–822. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sevoflurane 3% | Sevoflurane 5% | Sevoflurane 6% | p Value | |
|---|---|---|---|---|
| Patient number | 10 males | 10 males | 10 males | |
| Age, year | 21.9 ± 1.2 | 21.7 ± 1.8 | 21.9 ± 1.4 | 0.956 |
| Height, cm | 175.3 ± 8.4 | 169.9 ± 2.7 | 171.3 ± 4.7 | 0.293 |
| Weight, kg | 71.2 ± 10.8 | 64.8 ± 12.1 | 62.8 ± 9.3 | 0.206 |
| Body mass index, kg/m2 | 23.2 ± 3.7 | 22.4 ± 4.1 | 21.3 ± 2.0 | 0.42 |
| Time to | 122.5 ± 35.0 | 89.5 ± 22.5 | 71.5 ± 12.5 | 0.002 |
| loss of consciousness, sec | (75–180) | (55–120) | (55–90) | |
| AAI values at | 31.7 ± 9.9 | 26.2 ± 7.0 | 28.6 ± 6.8 | 0.355 |
| loss of consciousness | (16–45) | (20-36) | (20–41) |
| Anesthesia Level | Sevoflurane Group | Time after Induction | Inspiratory Concentration (%) | End-Tidal Concentration (%) | Estimated Jugular Bulb Concentration (%) |
|---|---|---|---|---|---|
| Loss of consciousness | 3% | 122.5 ± 35.0 s | 2.6 ± 0.1 | 2.2 ± 0.2 | |
| 5% | 89.5 ± 22.5 s | 4.1 ± 0.2 | 3.2 ± 0.4 | ||
| 6% | 71.5 ± 12.5 s | 4.2 ± 0.3 | 3.9 ± 0.3 | ||
| AAI ≤ 20 | 3% | 5.9 ± 1.5 min | 2.8 ± 0.1 | 2.4 ± 0.1 | 0.9 ± 0.0 |
| 5% | 4.8 ± 3.0 min | 4.3 ± 0.2 | 3.4 ± 0.2 | 1.3 ± 0.1 | |
| 6% | 2.6 ± 2.0 min | 4.8 ± 0.6 | 4.1 ± 0.2 | 1.4 ± 0.1 | |
| AAI ≤ 10 | 5% | 21.4 ± 9.8 min | 4.9 ± 0.1 | 3.8 ± 0.2 | 1.9 ± 0.1 |
| 6% | 8.3 ± 2.9 min | 5.6 ± 0.2 | 4.5 ± 0.2 * | 1.9 ± 0.1 | |
| Start of burst suppression | 5% | 26.8 ± 11.1 min | 4.9 ± 0.1 | 3.9 ± 0.1 | 2.1 ± 0.1 |
| 6% | 9.9 ± 2.6 min | 5.7 ± 0.1 | 4.7 ± 0.1 # | 2.2 ± 0.1 | |
| At 30 min | 3% | 30 min | 3.0 ± 0.0 | 2.6 ± 0.1 | 1.4 ± 0.0 |
| 5% | 5.0 ± 0.0 | 3.8 ± 0.2 | 2.1 ± 0.1 | ||
| 6% | 6.0 ± 0.0 | 5.1 ± 0.2 | 2.8 ± 0.1 | ||
| At 60 min | 3% | 60 min | 3.0 ± 0.0 | 2.7 ± 0.1 | 1.7 ± 0.0 |
| 5% | 5.0 ± 0.0 | 4.2 ± 0.1 | 2.7 ± 0.1 |
| Group | Time | Heart Rate (beats per min) | Mean Blood Pressure (mmHg) | End-Tidal CO2 (mmHg) |
|---|---|---|---|---|
| 3% sevoflurane | Before induction | 65.2 ± 8.7 | 86.9 ± 7.0 | -- |
| Loss of consciousness | 64.7 ± 7.1 | 82.6 ± 8.2 | 40.4 ± 2.7 | |
| 5 min | 87.3 ± 22.2 | 89.1 ± 16.5 | 41.7 ± 3.1 | |
| 10 min | 71.4 ± 16.7 | 73.4 ± 12.6 | 42.3 ± 2.0 | |
| 15 min | 69.1 ± 13.8 | 71.6 ± 8.6 | 42.7 ± 1.8 | |
| 20 min | 66.1 ± 12.5 | 69.5 ± 8.8 | 43.0 ± 1.1 | |
| 30 min | 66.6 ± 11.8 | 68.9 ± 10.5 | 43.2 ± 1.4 | |
| 40 min | 66.6 ± 12.9 | 67.7 ± 10.4 | 43.4 ± 1.3 | |
| 50 min | 65.1 ±12.4 | 66.4 ± 8.5 | 43.9 ± 1.4 | |
| 60 min | 63.2 ± 12.4 | 65.9 ± 8.6 | 44.1 ± 2.0 | |
| 5% sevoflurane | Before induction | 72.9 ± 11.7 | 86.3 ± 9.9 | -- |
| Loss of consciousness | 69.1 ± 11.7 | 81.0 ± 10.4 | 35.0 ± 2.6 | |
| 5 min | 92.0 ± 20.4 | 79.7 ± 8.5 | 35.2 ± 2.7 | |
| 10 min | 82.7 ± 14.7 | 74.4 ± 8.8 | 35.6 ± 3.1 | |
| 15 min | 82.0 ± 17.6 | 70.6 ± 6.9 | 36.1 ± 3.4 | |
| 20 min | 79.0 ± 16.3 | 69.4 ± 6.0 | 37.6 ± 4.0 | |
| 30 min | 83.4 ± 20.0 | 69.6 ± 10.0 | 38.7 ± 4.5 | |
| 40 min | 83.7 ± 21.6 | 65.2 ± 3.3 | 39.4 ± 5.1 | |
| 50 min | 78.0 ± 20.4 | 63.0 ± 2.8 | 40.0 ± 5.2 | |
| 60 min | 73.4 ± 17.5 | 61.1 ± 2.8 | 41.5 ± 5.7 | |
| 6% sevoflurane | Before induction | 72.7 ± 14.7 | 86.8 ± 10.6 | -- |
| Loss of consciousness | 75.1 ± 22.4 | 80.6 ± 9.4 | 38.3 ± 3.4 | |
| 5 min | 93.6 ± 22.7 | 75.3 ± 13.9 | 36.7 ± 2.9 | |
| 10 min | 80.6 ± 14.0 | 69.4 ± 13.1 | 35.9 ± 2.0 | |
| 15 min | 81.4 ± 9.4 | 65.4 ± 5.0 | 36.1 ± 1.4 | |
| 20 min | 80.3 ± 12.0 | 62.8 ± 4.1 | 36.8 ± 2.3 | |
| 30 min | 79.4 ± 13.8 | 63.3 ± 6.5 | 38.0 ± 2.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-H.; Ho, S.-T.; Lu, C.-C.; Wang, J.-O.; Yeh, T.-C.; Lin, T.-C. Discrepant End-Tidal Concentrations of Sevoflurane at the Same A-Line Autoregressive Index Level during Induction of General Anesthesia: An Observational Study. J. Clin. Med. 2021, 10, 4526. https://doi.org/10.3390/jcm10194526
Hsu C-H, Ho S-T, Lu C-C, Wang J-O, Yeh T-C, Lin T-C. Discrepant End-Tidal Concentrations of Sevoflurane at the Same A-Line Autoregressive Index Level during Induction of General Anesthesia: An Observational Study. Journal of Clinical Medicine. 2021; 10(19):4526. https://doi.org/10.3390/jcm10194526
Chicago/Turabian StyleHsu, Che-Hao, Shung-Tai Ho, Chih-Cherng Lu, Ju-O Wang, Te-Chun Yeh, and Tso-Chou Lin. 2021. "Discrepant End-Tidal Concentrations of Sevoflurane at the Same A-Line Autoregressive Index Level during Induction of General Anesthesia: An Observational Study" Journal of Clinical Medicine 10, no. 19: 4526. https://doi.org/10.3390/jcm10194526