
PriME-PGx: La Princesa University Hospital Multidisciplinary Initiative for the Implementation of Pharmacogenetics

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Historical Achievements
3. Relevant Pharmacogenetic Tests
3.1. TPMT, NUDT15 and Thiopurines
3.2. HLA-B
3.3. IFNL3 (IL28B)
3.4. CYP2C19
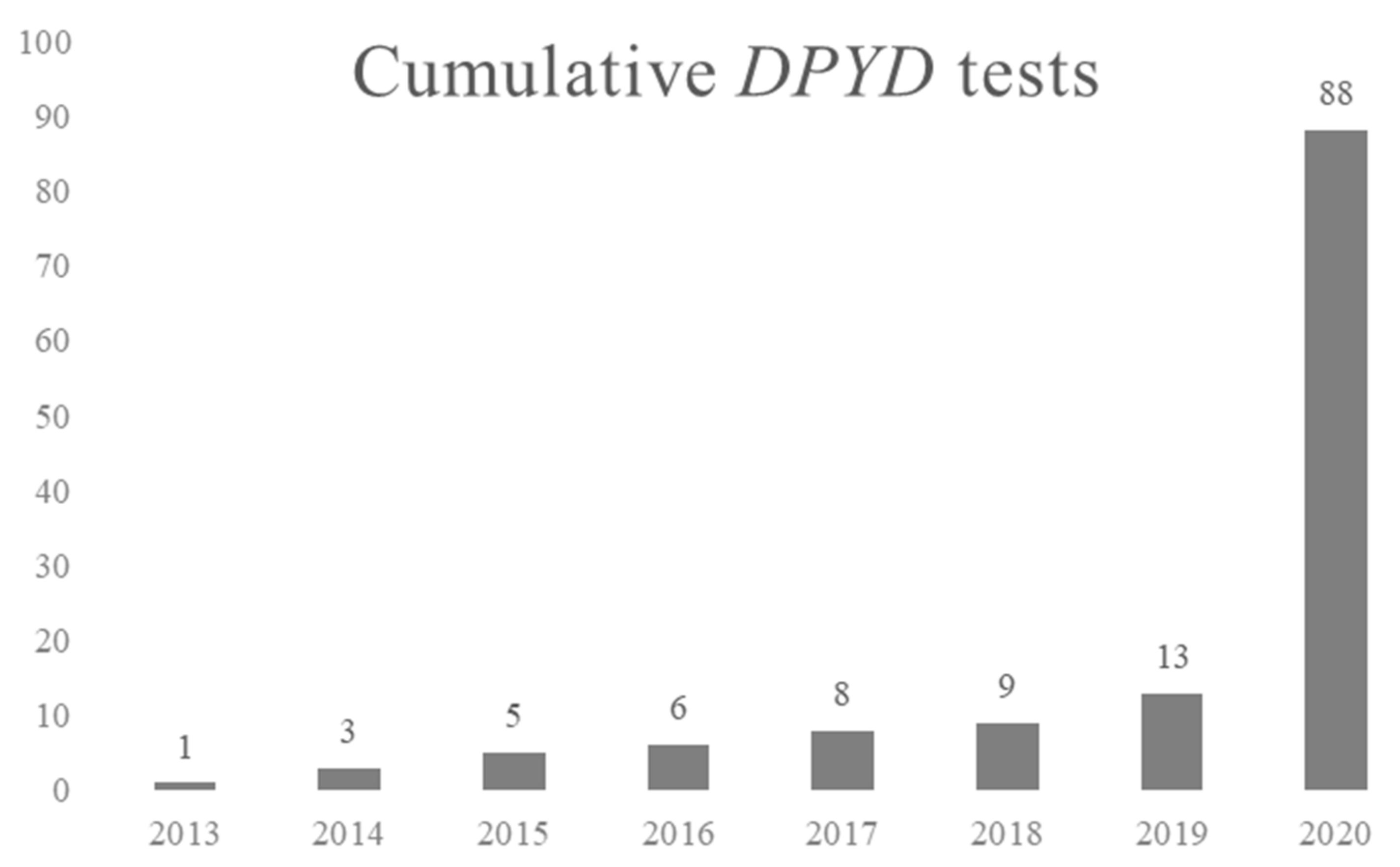
3.5. DPYD
3.6. Pain Management Unit: Towards Complete Pharmacogenetic Reports
4. The PROFILE Project
- Pain Management (PMU) profile: this profile includes evident drug-gene associations for anti-inflammatory and analgesic drugs (e.g., tramadol-CYP2D6 and NSAIDs-CYP2C9) and other less evident pairs: antidepressants, statins or antiepileptic drugs (Supplementary Table S1).
- Oncology (ONC) profile: this profile includes evident drug-gene associations for antineoplastic drugs (e.g., DPYD and 5-fluorouracil, CYP2D6 and tamoxifen or UGT1A1 and irinotecan), immunosuppressants (e.g., TPMT/NUDT15 for azathioprine and mercaptopurine and CYP3A5 for tacrolimus) and other less evident pairs: tramadol, codeine, ondansetron or tropisetron (Supplementary Table S1).
- Neurology-psychiatry (NEU) profile: this profile includes evident drug-gene associations for antipsychotics (e.g., CYP2D6 and aripiprazole), selective serotonin reuptake inhibitors (SSRIs) (e.g., CYP2D6 and fluvoxamine or CYP2C19 and citalopram), tricyclic antidepressants (e.g., CYP2D6 and desipramine or CYP2C19 and imipramine), CYP2C9-siponimod and antiepileptic drugs (e.g., HLA-B*15 and A*31 for carbamazepine) (Supplementary Table S1).
- Immunosuppressants (IMS) profile: this profile includes associations for immunosuppressants exclusively (e.g., TPMT/NUDT15 for azathioprine and mercaptopurine and CYP3A5 for tacrolimus) (Supplementary Table S1).
- Infectious Diseases (INF) profile: this profile includes evident drug-gene associations for anti-infectious agents (e.g., HLA-B for abacavir, DPYD for flucytosine, IFNL3 for ribavirin or peg-α-2a/2b interferon, UGT1A1 for atazanavir, CYP2B6 for efavirenz and CYP2C19 for voriconazole) (Supplementary Table S1).
- Gastroenterology (DIG) profile: this profile includes an evident drug-gene association, i.e., CYP2C19 and protein pump inhibitors (PPIs) (e.g., omeprazole) and other less evident drug-gene pairs (CYP2C19-clopidogrel, TPMT/NUDT15 for azathioprine and mercaptopurine or CYP2C9, CYP4F2 and VKORC1 for warfarin and acenocumarol) (Supplementary Table S1).
- Cardiovascular medicine (CAR) profile: this profile includes evident drug-gene associations for agents related to cardiovascular or blood function (e.g., SLCO1B1 for statins or CYP2C19 for clopidogrel and CYP2C9, CYP4F2 and VKORC1 for warfarin and acenocumarol) and other less evident drug-gene pairs (e.g., CYP2C19-PPIs) (Supplementary Table S1).
4.1. The GENOTRIAL Project
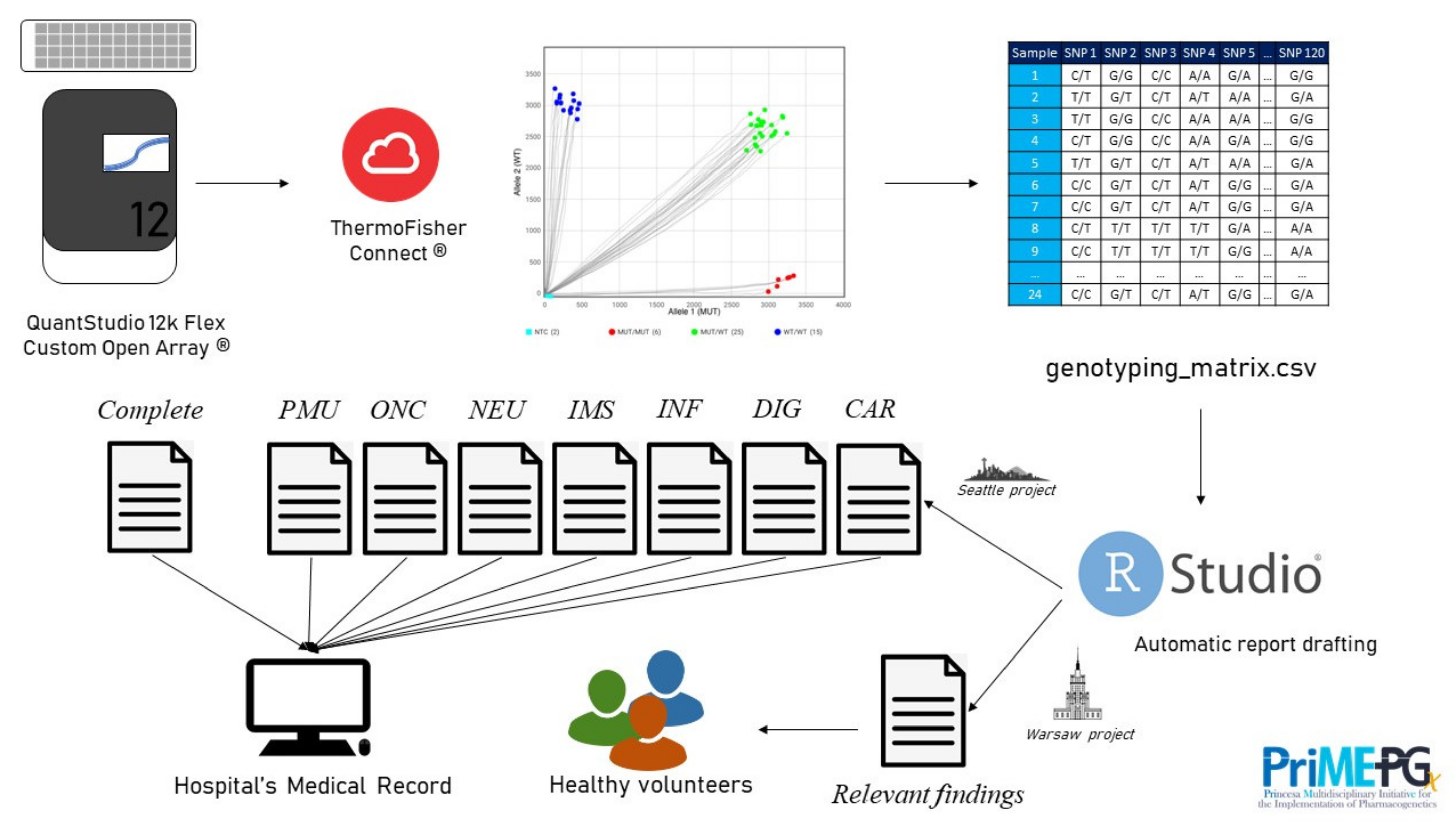
4.2. Automation
5. Conclusions and Future Perspective
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Motulsky, A.G.; Qi, M. Pharmacogenetics, Pharmacogenomics and Ecogenetics. J. Zhejiang Univ. Sci. B 2006, 7, 169–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Human Genome Research Institute. DNA Sequencing Costs: Data. Available online: https://www.genome.gov/about-genomics/fact-sheets/DNA-Sequencing-Costs-Data (accessed on 12 August 2021).
- Verbelen, M.; Weale, M.E.; Lewis, C.M. Cost-Effectiveness of Pharmacogenetic-Guided Treatment: Are We There Yet? Pharm. J. 2017, 17, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Van den Akker-van Marle, M.E.; Gurwitz, D.; Detmar, S.B.; Enzing, C.M.; Hopkins, M.M.; Gutierrez de Mesa, E.; Ibarreta, D. Cost-Effectiveness of Pharmacogenomics in Clinical Practice: A Case Study of Thiopurine Methyltransferase Genotyping in Acute Lymphoblastic Leukemia in Europe. Pharmacogenomics 2006, 7, 783–792. [Google Scholar] [CrossRef] [Green Version]
- Fragoulakis, V.; Roncato, R.; Fratte, C.D.; Ecca, F.; Bartsakoulia, M.; Innocenti, F.; Toffoli, G.; Cecchin, E.; Patrinos, G.P.; Mitropoulou, C. Estimating the Effectiveness of DPYD Genotyping in Italian Individuals Suffering from Cancer Based on the Cost of Chemotherapy-Induced Toxicity. Am. J. Hum. Genet. 2019, 104, 1158–1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toffoli, G.; Innocenti, F.; Polesel, J.; De Mattia, E.; Sartor, F.; Dalle Fratte, C.; Ecca, F.; Dreussi, E.; Palazzari, E.; Guardascione, M.; et al. The Genotype for DPYD Risk Variants in Patients With Colorectal Cancer and the Related Toxicity Management Costs in Clinical Practice. Clin. Pharmacol. Ther. 2019, 105, 994–1002. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Swanson, K.M.; Rojas, R.L.; Wang, Z.; St. Sauver, J.L.; Visscher, S.L.; Prokop, L.J.; Bielinski, S.J.; Wang, L.; Weinshilboum, R.; et al. Systematic Review of the Evidence on the Cost-Effectiveness of Pharmacogenomics-Guided Treatment for Cardiovascular Diseases. Genet. Med. 2020, 22, 475–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LLerena, A.; Peñas-Lledó, E.; de Andrés, F.; Mata-Martín, C.; Sánchez, C.L.; Pijierro, A.; Cobaleda, J. Clinical Implementation of Pharmacogenetics and Personalized Drug Prescription Based on E-Health: The MedeA Initiative. Drug Metabol. Pers. Ther. 2020, 20200143. [Google Scholar] [CrossRef]
- Van der Wouden, C.; Cambon-Thomsen, A.; Cecchin, E.; Cheung, K.; Dávila-Fajardo, C.; Deneer, V.; Dolžan, V.; Ingelman-Sundberg, M.; Jönsson, S.; Karlsson, M.; et al. Implementing Pharmacogenomics in Europe: Design and Implementation Strategy of the Ubiquitous Pharmacogenomics Consortium. Clin. Pharmacol. Ther. 2017, 101, 341–358. [Google Scholar] [CrossRef]
- Christensen, K.D.; Bell, M.; Zawatsky, C.L.B.; Galbraith, L.N.; Green, R.C.; Hutchinson, A.M.; Jamal, L.; LeBlanc, J.L.; Leonhard, J.R.; Moore, M.; et al. Precision Population Medicine in Primary Care: The Sanford Chip Experience. Front. Genet. 2021, 12, 626845. [Google Scholar] [CrossRef]
- Aquilante, C.L.; Kao, D.P.; Trinkley, K.E.; Lin, C.-T.; Crooks, K.R.; Hearst, E.C.; Hess, S.J.; Kudron, E.L.; Lee, Y.M.; Liko, I.; et al. Clinical Implementation of Pharmacogenomics via a Health System-Wide Research Biobank: The University of Colorado Experience. Pharmacogenomics 2020, 21, 375–386. [Google Scholar] [CrossRef] [Green Version]
- Borobia, A.M.; Dapia, I.; Tong, H.Y.; Arias, P.; Muñoz, M.; Tenorio, J.; Hernández, R.; García García, I.; Gordo, G.; Ramírez, E.; et al. Clinical Implementation of Pharmacogenetic Testing in a Hospital of the Spanish National Health System: Strategy and Experience Over 3 Years. Clin. Transl. Sci. 2018, 11, 189–199. [Google Scholar] [CrossRef] [Green Version]
- Nishimura, A.A.; Shirts, B.H.; Dorschner, M.O.; Amendola, L.M.; Smith, J.W.; Jarvik, G.P.; Tarczy-Hornoch, P. Development of Clinical Decision Support Alerts for Pharmacogenomic Incidental Findings from Exome Sequencing. Genet. Med. 2015, 17, 939–942. [Google Scholar] [CrossRef] [Green Version]
- Hicks, J.K.; Stowe, D.; Willner, M.A.; Wai, M.; Daly, T.; Gordon, S.M.; Lashner, B.A.; Parikh, S.; White, R.; Teng, K.; et al. Implementation of Clinical Pharmacogenomics within a Large Health System: From Electronic Health Record Decision Support to Consultation Services. Pharmacotherapy 2016, 36, 940–948. [Google Scholar] [CrossRef]
- Peterson, J.F.; Bowton, E.; Field, J.R.; Beller, M.; Mitchell, J.; Schildcrout, J.; Gregg, W.; Johnson, K.; Jirjis, J.N.; Roden, D.M.; et al. Electronic Health Record Design and Implementation for Pharmacogenomics: A Local Perspective. Genet. Med. 2013, 15, 833–841. [Google Scholar] [CrossRef] [Green Version]
- Pulley, J.M.; Denny, J.C.; Peterson, J.F.; Bernard, G.R.; Vnencak-Jones, C.L.; Ramirez, A.H.; Delaney, J.T.; Bowton, E.; Brothers, K.; Johnson, K.; et al. Operational Implementation of Prospective Genotyping for Personalized Medicine: The Design of the Vanderbilt PREDICT Project. Clin. Pharmacol. Ther. 2012, 92, 87–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roncato, R.; Dal Cin, L.; Mezzalira, S.; Comello, F.; De Mattia, E.; Bignucolo, A.; Giollo, L.; D’Errico, S.; Gulotta, A.; Emili, L.; et al. FARMAPRICE: A Pharmacogenetic Clinical Decision Support System for Precise and Cost-Effective Therapy. Genes 2019, 10, 276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinderer, M.; Boeker, M.; Wagner, S.A.; Lablans, M.; Newe, S.; Hülsemann, J.L.; Neumaier, M.; Binder, H.; Renz, H.; Acker, T.; et al. Integrating Clinical Decision Support Systems for Pharmacogenomic Testing into Clinical Routine—A Scoping Review of Designs of User-System Interactions in Recent System Development. BMC Med. Inform. Decis. Mak. 2017, 17, 81. [Google Scholar] [CrossRef] [Green Version]
- Muir, A.J.; Gong, L.; Johnson, S.G.; Lee, M.T.M.; Williams, M.S.; Klein, T.E.; Caudle, K.E.; Nelson, D.R. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines for IFNL3 (IL28B) Genotype and PEG Interferon-α–Based Regimens. Clin. Pharmacol. Ther. 2014, 95, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Relling, M.V.; Schwab, M.; Whirl-Carrillo, M.; Suarez-Kurtz, G.; Pui, C.-H.; Stein, C.M.; Moyer, A.M.; Evans, W.E.; Klein, T.E.; Antillon-Klussmann, F.G.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for Thiopurine Dosing Based on TPMT and NUDT15 Genotypes: 2018 Update. Clin. Pharmacol. Ther. 2019, 105, 1095–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, S.A.; Sangkuhl, K.; Stein, C.M.; Hulot, J.-S.; Mega, J.L.; Roden, D.M.; Klein, T.E.; Sabatine, M.S.; Johnson, J.A.; Shuldiner, A.R. Clinical Pharmacogenetics Implementation Consortium Guidelines for CYP2C19 Genotype and Clopidogrel Therapy: 2013 Update. Clin. Pharmacol. Ther. 2013, 94, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Amstutz, U.; Henricks, L.M.; Offer, S.M.; Barbarino, J.; Schellens, J.H.M.; Swen, J.J.; Klein, T.E.; McLeod, H.L.; Caudle, K.E.; Diasio, R.B.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for Dihydropyrimidine Dehydrogenase Genotype and Fluoropyrimidine Dosing: 2017 Update. Clin. Pharmacol. Ther. 2018, 103, 210–216. [Google Scholar] [CrossRef]
- Relling, M.V.; Klein, T.E. CPIC: Clinical Pharmacogenetics Implementation Consortium of the Pharmacogenomics Research Network. Clin. Pharmacol. Ther. 2011, 89, 464–467. [Google Scholar] [CrossRef] [PubMed]
- Relling, M.V.; Klein, T.E.; Gammal, R.S.; Whirl-Carrillo, M.; Hoffman, J.M.; Caudle, K.E. The Clinical Pharmacogenetics Implementation Consortium: 10 Years Later. Clin. Pharmacol. Ther. 2020, 107, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Pharmacogenetic Guidelines Issued by the Dutch Pharmacogenetics Working Group, Royal Dutch Pharmacists Association (KNMP). Available online: https://www.knmp.nl/patientenzorg/medicatiebewaking/farmacogenetica/pharmacogenetics-1/pharmacogenetics (accessed on 12 August 2021).
- Evans, W.E. Pharmacogenetics of Thiopurine S-Methyltransferase and Thiopurine Therapy. Ther. Drug Monit. 2004, 26, 186–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, M.A.; Klein, T.E.; Dong, B.J.; Pirmohamed, M.; Haas, D.W.; Kroetz, D.L. Clinical Pharmacogenetics Implementation Consortium Guidelines for HLA-B Genotype and Abacavir Dosing. Clin. Pharmacol. Ther. 2012, 91, 734–738. [Google Scholar] [CrossRef]
- Hughes, S.; Hughes, A.; Brothers, C.; Spreen, W.; Thorborn, D.; on behalf of the CNA106030 Study Team. PREDICT-1 (CNA106030): The First Powered, Prospective Trial of Pharmacogenetic Screening to Reduce Drug Adverse Events. Pharm. Stat. 2008, 7, 121–129. [Google Scholar] [CrossRef]
- Cristallo, A.F.; Schroeder, J.; Citterio, A.; Santori, G.; Ferrioli, G.M.; Rossi, U.; Bertani, G.; Cassano, S.; Gottardi, P.; Ceschini, N.; et al. A Study of HLA Class I and Class II 4-Digit Allele Level in Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Identification of HLA Markers in SJS and TEN. Int. J. Immunogenet. 2011, 38, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Phillips, E.J.; Sukasem, C.; Whirl-Carrillo, M.; Müller, D.J.; Dunnenberger, H.M.; Chantratita, W.; Goldspiel, B.; Chen, Y.; Carleton, B.C.; George, A.L.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for HLA Genotype and Use of Carbamazepine and Oxcarbazepine: 2017 Update. Clin. Pharmacol. Ther. 2018, 103, 574–581. [Google Scholar] [CrossRef] [Green Version]
- Zubiaur, P.; Saiz-Rodríguez, M.; Villapalos-García, G.; Navares-Gómez, M.; Koller, D.; Abad-Santos, F. HCP5 Rs2395029 Is a Rapid and Inexpensive Alternative to HLA-B*57:01 Genotyping to Predict Abacavir Hypersensitivity Reaction in Spain. Pharm. Genom. 2021, 31, 53–59. [Google Scholar] [CrossRef]
- Hershfield, M.S.; Callaghan, J.T.; Tassaneeyakul, W.; Mushiroda, T.; Thorn, C.F.; Klein, T.E.; Lee, M.T.M. Clinical Pharmacogenetics Implementation Consortium Guidelines for Human Leukocyte Antigen-B Genotype and Allopurinol Dosing. Clin. Pharmacol. Ther. 2013, 93, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, Y.; Nishida, N.; Sugiyama, M.; Kurosaki, M.; Matsuura, K.; Sakamoto, N.; Nakagawa, M.; Korenaga, M.; Hino, K.; Hige, S.; et al. Genome-Wide Association of IL28B with Response to Pegylated Interferon-α and Ribavirin Therapy for Chronic Hepatitis C. Nat. Genet. 2009, 41, 1105–1109. [Google Scholar] [CrossRef]
- Thomas, D.L.; Thio, C.L.; Martin, M.P.; Qi, Y.; Ge, D.; O’hUigin, C.; Kidd, J.; Kidd, K.; Khakoo, S.I.; Alexander, G.; et al. Genetic Variation in IL28B and Spontaneous Clearance of Hepatitis C Virus. Nature 2009, 461, 798–801. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.A.; Sangkuhl, K.; Shuldiner, A.R.; Hulot, J.-S.; Thorn, C.F.; Altman, R.B.; Klein, T.E. PharmGKB Summary: Very Important Pharmacogene Information for Cytochrome P450, Family 2, Subfamily C, Polypeptide 19. Pharm. Genom. 2012, 22, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Saiz-Rodríguez, M.; Romero-Palacián, D.; Villalobos-Vilda, C.; Caniego, J.L.; Belmonte, C.; Koller, D.; Bárcena, E.; Talegón, M.; Abad-Santos, F. Influence of CYP2C19 Phenotype on the Effect of Clopidogrel in Patients Undergoing a Percutaneous Neurointervention Procedure. Clin. Pharmacol. Ther. 2019, 105, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Saiz-Rodríguez, M.; Belmonte, C.; Caniego, J.L.; Koller, D.; Zubiaur, P.; Bárcena, E.; Romero-Palacián, D.; Eugene, A.R.; Ochoa, D.; Abad-Santos, F. Influence of CYP450 Enzymes, CES1, PON1, ABCB1, and P2RY12 Polymorphisms on Clopidogrel Response in Patients Subjected to a Percutaneous Neurointervention. Clin. Ther. 2019, 41, 1199–1212.e2. [Google Scholar] [CrossRef]
- Caudle, K.E.; Thorn, C.F.; Klein, T.E.; Swen, J.J.; McLeod, H.L.; Diasio, R.B.; Schwab, M. Clinical Pharmacogenetics Implementation Consortium Guidelines for Dihydropyrimidine Dehydrogenase Genotype and Fluoropyrimidine Dosing. Clin. Pharmacol. Ther. 2013, 94, 640–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crews, K.R.; Gaedigk, A.; Dunnenberger, H.M.; Klein, T.E.; Shen, D.D.; Callaghan, J.T.; Kharasch, E.D.; Skaar, T.C. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines for Codeine Therapy in the Context of Cytochrome P450 2D6 (CYP2D6) Genotype. Clin. Pharmacol. Ther. 2012, 91, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Theken, K.N.; Lee, C.R.; Gong, L.; Caudle, K.E.; Formea, C.M.; Gaedigk, A.; Klein, T.E.; Agúndez, J.A.G.; Grosser, T. Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and Nonsteroidal Anti-Inflammatory Drugs. Clin. Pharmacol. Ther. 2020, 108, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Koller, D.; Almenara, S.; Mejía, G.; Saiz-Rodríguez, M.; Zubiaur, P.; Román, M.; Ochoa, D.; Wojnicz, A.; Martín, S.; Romero-Palacián, D.; et al. Safety and Cardiovascular Effects of Multiple-dose Administration of Aripiprazole and Olanzapine in a Randomised Clinical Trial. Hum. Psychopharmacol. Clin. Exp. 2020, 36, e2761. [Google Scholar] [CrossRef]
- Zubiaur, P.; Benedicto, M.D.; Villapalos-García, G.; Navares-Gómez, M.; Mejía-Abril, G.; Román, M.; Martín-Vílchez, S.; Ochoa, D.; Abad-Santos, F. SLCO1B1 Phenotype and CYP3A5 Polymorphism Significantly Affect Atorvastatin Bioavailability. J. Pers. Med. 2021, 11, 204. [Google Scholar] [CrossRef]
- Zubiaur, P.; Saiz-Rodríguez, M.; Ochoa, D.; Navares-Gómez, M.; Mejía, G.; Román, M.; Koller, D.; Soria-Chacartegui, P.; Almenara, S.; Abad-Santos, F. Effect of Sex, Use of Pantoprazole and Polymorphisms in SLC22A1, ABCB1, CES1, CYP3A5 and CYP2D6 on the Pharmacokinetics and Safety of Dabigatran. Adv. Ther. 2020, 37, 3537–3550. [Google Scholar] [CrossRef] [PubMed]
- Saiz-Rodríguez, M.; Belmonte, C.; Román, M.; Ochoa, D.; Koller, D.; Talegón, M.; Ovejero-Benito, M.C.; López-Rodríguez, R.; Cabaleiro, T.; Abad-Santos, F. Effect of Polymorphisms on the Pharmacokinetics, Pharmacodynamics and Safety of Sertraline in Healthy Volunteers. Basic Clin. Pharmacol. Toxicol. 2017, 122, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Koller, D.; Belmonte, C.; Lubomirov, R.; Saiz-Rodríguez, M.; Zubiaur, P.; Román, M.; Ochoa, D.; Carcas, A.; Wojnicz, A.; Abad-Santos, F. Effects of Aripiprazole on Pupillometric Parameters Related to Pharmacokinetics and Pharmacogenetics after Single Oral Administration to Healthy Subjects. J. Psychopharmacol. 2018, 32, 1212–1222. [Google Scholar] [CrossRef] [PubMed]
- Koller, D.; Almenara, S.; Mejía, G.; Saiz-Rodríguez, M.; Zubiaur, P.; Román, M.; Ochoa, D.; Navares-Gómez, M.; Santos-Molina, E.; Pintos-Sánchez, E.; et al. Metabolic Effects of Aripiprazole and Olanzapine Multiple-Dose Treatment in a Randomised Crossover Clinical Trial in Healthy Volunteers: Association with Pharmacogenetics. Adv. Ther. 2020, 38, 1035–1054. [Google Scholar] [CrossRef]
- Zubiaur, P.; Saiz-Rodríguez, M.; Ochoa, D.; Belmonte, C.; Román, M.; Mejía, G.; Martín-Vilchez, S.; Abad-Santos, F. Influence of CYP2B6 Activity Score on the Pharmacokinetics and Safety of Single Dose Efavirenz in Healthy Volunteers. Pharm. J. 2019, 20, 235–245. [Google Scholar] [CrossRef]
- Cabaleiro, T.; Ochoa, D.; Román, M.; Moreno, I.; López-Rodríguez, R.; Novalbos, J.; Abad-Santos, F. Polymorphisms in CYP2D6 Have a Greater Effect on Variability of Risperidone Pharmacokinetics than Gender. Basic Clin. Pharmacol. Toxicol. 2015, 116, 124–128. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Gene | Allele | SNP (rs) | Ancestral | Mutant | Defines Actionable #1 Allele? |
|---|---|---|---|---|---|
| CYP4F2 | Not defined | rs2108622 | C | T | YES |
| CYP2B6 | Multiple | rs3745274 | G | T | YES |
| Multiple | rs3211371 | C | T | YES | |
| Not defined | rs4803419 | C | T | NO | |
| Multiple | rs2279343 | A | G | YES | |
| *22 | rs34223104 | C | T | YES | |
| *18, *16 | rs28399499 | T | C | YES | |
| CYP2C9 | *2 | rs1799853 | C | T | YES |
| *3 | rs1057910 | A | C | YES | |
| *5 | rs28371686 | C | G | YES | |
| *8 | rs9332094 | T | C | YES | |
| *8 | rs7900194 | T | G | YES | |
| *11 | rs28371685 | C | T | YES | |
| CYP2C19 | *2 | rs4244285 | G | A | YES |
| *3 | rs4986893 | G | A | YES | |
| *4 | rs28399504 | A | G | YES | |
| *6 | rs72552267 | G | A | YES | |
| *5 | rs56337013 | C | T | YES | |
| *7 | rs72558186 | T | C | YES | |
| *8 | rs41291556 | T | C | YES | |
| *9 | rs17884712 | G | A | YES | |
| *17 | rs12248560 | C | T | YES | |
| *2, *35 | rs12769205 | A | G | YES | |
| CYP2D6 | *3 | rs35742686 | T | - | YES |
| *4 | rs3892097 | C | T | YES | |
| *6 | rs5030655 | A | - | YES | |
| *7 | rs5030867 | T | G | YES | |
| *8 | rs5030865 | C | A | YES | |
| *9 | rs5030656 | CTT | - | YES | |
| *10, *4 | rs1065852 | C | T | YES | |
| *10 | rs1135840 | C | G | YES | |
| *12 | rs5030862 | C | T | YES | |
| *14 | rs5030865 | C | T | YES | |
| *15 | rs774671100 | A | - | YES | |
| *17 | rs28371706 | G | A | YES | |
| *19 | rs72549353 | AGTT | - | YES | |
| *29 | rs59421388 | G | A | YES | |
| *41 | rs28371725 | C | T | YES | |
| *56B | rs72549347 | G | A | YES | |
| *59 | rs79292917 | C | T | YES | |
| CYP3A5 | *3 | rs776746 | T | C | YES |
| *6 | rs10264272 | C | T | YES | |
| *7 | rs41303343 | A | - | YES | |
| DPYD | *2A | rs3918290 | C | G/T | YES |
| *12 | rs1057519962 | G | A | YES | |
| *12 | rs1057519962 | G | T | YES | |
| *10 | rs1801268 | C | A | YES | |
| *7 | rs72549309 | ATGAATGA | ATGA | YES | |
| *8 | rs1801266 | G | A | YES | |
| *13 | rs55886062 | A | C/T | YES | |
| HapB3 | rs75017182 | G | C | YES | |
| HapB3 | rs75017182 | G | T | YES | |
| c.2846A > T | rs67376798 | T | A | YES | |
| c.557A > G | rs115232898 | T | C | YES | |
| HapB3 (tag) | rs56038477 | C | T | YES | |
| c.680 + 139G > A | rs6668296 | T | C | NO | |
| HCP5 | HLA-B*57:01 | rs2395029 | T | G | YES #2 |
| HCP5 | HLA-B*57:01 | rs2395029 | T | G | YES |
| IL28B | rs12979860 | T | C | YES | |
| TPMT | *2 | rs1800462 | C | G | YES |
| *3B, *3A | rs1800460 | G | A | YES | |
| *3C, *3A | rs1142345 | A | G | YES | |
| *4 | rs1800584 | C | T | YES | |
| *11 | rs72552738 | C | T | YES | |
| REP TPMT | *2 | rs1800462 | C | G | YES |
| *3B, *3A | rs1800460 | G | A | YES | |
| NUDT15 | *3 | rs116855232 | C | T | YES |
| VKORC1 | (−1639G > A) | rs9923231 | C | T | YES |
| rs9934438 | G | A | NO | ||
| rs7294 | C | T | NO | ||
| UGT1A1 | *6 | rs4148323 | G | A | YES |
| *80 | rs887829 | C | T | YES #3 | |
| HLA-A3101 | rs1061235 | A | T | YES #4 | |
| SLCO1B1 | *5 | rs4149056 | T | C | YES |
| *1b | rs2306283 | G | A | YES | |
| c.−910G > A | rs4149015 | G | A | YES | |
| *2 | rs56101265 | T | C | YES | |
| *3 | rs56061388 | T | C | YES | |
| *6 | rs55901008 | T | C | YES | |
| *9 | rs59502379 | G | C | YES | |
| *10 | rs56199088 | A | G | YES | |
| rs11045879 | T | C | NO | ||
| CYP1A2 | *1C | rs2069514 | G | A | NO |
| *1F | rs762551 | A | C | NO | |
| *1B | rs2470890 | T | C | NO | |
| CYP2A6 | *9 | rs28399433 | A | C | NO |
| CYP2C8 | *2 | rs11572103 | T | A | NO |
| *3 | rs10509681 | T | C | NO | |
| rs11572080 | C | T | NO | ||
| *4 | rs1058930 | G | C | NO | |
| CYP3A4 | *3 | rs4986910 | A | G | NO |
| *2 | rs55785340 | A | G | NO | |
| *6 | rs4646438 | T | TT | NO | |
| *18 | rs28371759 | NO | |||
| *22 | rs35599367 | C | T | NO | |
| ABCB1 | C3435T | rs1045642 | C | T | NO |
| G2677 T/A | rs2032582 | C | A | NO | |
| G2677 T/A | rs2032582 | C | T | NO | |
| C1236T | rs1128503 | G | A | NO | |
| TBL1Y (SEX) | rs768983 | NO | |||
| ABCG2 | rs2231142 | G | T | NO | |
| ABCC2 | rs2273697 | G | A | NO | |
| COMT | rs4680 | G | A | NO | |
| rs13306278 | C | T | NO | ||
| OPRM1 | rs1799971 | A | G | NO | |
| SLC22A1 | *2 | rs72552763 | GAT | - | NO |
| *3 | rs12208357 | C | T | NO | |
| *5 | rs34059508 | G | A | NO | |
| UGT2B15 | rs1902023 | A | C | NO | |
| RARG | rs2229774 | G | A | NO | |
| SCL28A3 | rs7853758 | G | A | NO | |
| UGT1A4 | rs2011425 | T | A | NO | |
| UGT1A4 | rs2011425 | T | G | NO | |
| EPHX1 | rs2234922 | A | G | NO | |
| rs1051740 | T | C | NO | ||
| MTHFR | rs1801133 | G | A | NO | |
| XPC | rs2228001 | T | G | NO | |
| ERCC1 | rs11615 | A | G | NO | |
| ERCC1 | rs3212986 | A | C | NO | |
| XRCC1 | rs25487 | C | T | NO |
| Genotype | Count | % | Phenotype |
|---|---|---|---|
| *1/*1 | 618 | 92.4 | NM |
| *1/*3A | 33 | 4.9 | IM |
| *1/*2 | 9 | 1.3 | IM |
| *1/*3C | 5 | 0.8 | IM |
| *2/*2 | 1 | 0.2 | PM |
| *3A/*3C | 1 | 0.2 | PM |
| *1/*8 | 1 | 0.2 | Ind |
| *1/*19 | 1 | 0.2 | Ind |
| Total | 669 | 100 |
| HLA-B Allele | Count | % | HLA-B Allele | Count | % |
|---|---|---|---|---|---|
| *44 | 327 | 13.3 | *13 | 42 | 1.7 |
| *35 | 274 | 11.1 | *41 | 30 | 1.2 |
| *7 | 187 | 7.6 | *45 | 29 | 1.2 |
| *51 | 187 | 7.6 | *55 | 27 | 1.1 |
| *18 | 173 | 7.0 | *37 | 24 | 1.0 |
| *15 | 162 | 6.6 | *48 | 16 | 0.7 |
| *14 | 136 | 5.5 | *42 | 12 | 0.5 |
| *40 | 128 | 5.2 | *47 | 10 | 0.4 |
| *8 | 105 | 4.3 | *81 | 8 | 0.3 |
| *49 | 81 | 3.3 | *78 | 5 | 0.2 |
| *39 | 78 | 3.2 | *56 | 4 | 0.2 |
| *27 | 69 | 2.8 | *73 | 2 | 0.1 |
| *57 | 63 | 2.6 | *95 | 2 | 0.1 |
| *53 | 62 | 2.5 | *4 | 1 | 0.0 |
| *58 | 57 | 2.3 | *46 | 1 | 0.0 |
| *38 | 55 | 2.2 | *54 | 1 | 0.0 |
| *50 | 52 | 2.1 | *67 | 1 | 0.0 |
| *52 | 47 | 1.9 | Total * | 2458 | 100% |
| Genotype | Count | % | Phenotype |
|---|---|---|---|
| *1/*1 | 80 | 42.6 | NM |
| *1/*17 | 47 | 25.0 | RM |
| *1/*2 | 39 | 20.7 | IM |
| *2/*17 | 9 | 4.8 | IM |
| *17/17 | 9 | 4.8 | UM |
| *2/*2 | 4 | 2.1 | PM |
| Total | 188 | 100 |
| Genotype | CNV | Count | % | Phenotype |
|---|---|---|---|---|
| *1/*5 | 1 copy (6.3%) | 9 | 5.1 | IM |
| *4/*5 | 2 | 1.1 | PM | |
| *1/*10 | 2 copies (85.7%) | 82 | 46.9 | NM |
| *1/*4 | 26 | 14.9 | IM | |
| *1/*9 | 10 | 5.7 | NM | |
| *1/*41 | 6 | 3.4 | NM | |
| *1/*6 | 6 | 3.4 | IM | |
| *4/*4 | 5 | 2.9 | PM | |
| *1/*17 | 3 | 1.7 | NM | |
| *4/*9 | 3 | 1.7 | IM | |
| *10/*10 | 1 | <1% | IM | |
| *3/*3 | 1 | <1% | PM | |
| *3/*4 | 1 | <1% | PM | |
| *4/*10 | 1 | <1% | IM | |
| *4/*41 | 1 | <1% | IM | |
| *4/*6 | 1 | <1% | PM | |
| *9/*9 | 1 | <1% | IM | |
| *4/*17 | 1 | <1% | IM | |
| *41/*41 | 1 | <1% | IM | |
| (*1/*1) xN | 3 copies (8.0%) | 8 | 4.6 | UM |
| (*1/*4) xN | 3 | 1.7 | NM or IM | |
| (*1/*9) xN | 1 | <1% | NM or UM | |
| (*1/*10) xN | 1 | <1% | NM | |
| (*1/*41) xN | 1 | <1% | NM or UM | |
| Total | 175 | 100% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zubiaur, P.; Mejía-Abril, G.; Navares-Gómez, M.; Villapalos-García, G.; Soria-Chacartegui, P.; Saiz-Rodríguez, M.; Ochoa, D.; Abad-Santos, F. PriME-PGx: La Princesa University Hospital Multidisciplinary Initiative for the Implementation of Pharmacogenetics. J. Clin. Med. 2021, 10, 3772. https://doi.org/10.3390/jcm10173772
Zubiaur P, Mejía-Abril G, Navares-Gómez M, Villapalos-García G, Soria-Chacartegui P, Saiz-Rodríguez M, Ochoa D, Abad-Santos F. PriME-PGx: La Princesa University Hospital Multidisciplinary Initiative for the Implementation of Pharmacogenetics. Journal of Clinical Medicine. 2021; 10(17):3772. https://doi.org/10.3390/jcm10173772
Chicago/Turabian StyleZubiaur, Pablo, Gina Mejía-Abril, Marcos Navares-Gómez, Gonzalo Villapalos-García, Paula Soria-Chacartegui, Miriam Saiz-Rodríguez, Dolores Ochoa, and Francisco Abad-Santos. 2021. "PriME-PGx: La Princesa University Hospital Multidisciplinary Initiative for the Implementation of Pharmacogenetics" Journal of Clinical Medicine 10, no. 17: 3772. https://doi.org/10.3390/jcm10173772