
Factors Associated with Occurrence of Atelectasis during Sedation for Imaging in Pediatric Patients: A Retrospective Single Center Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
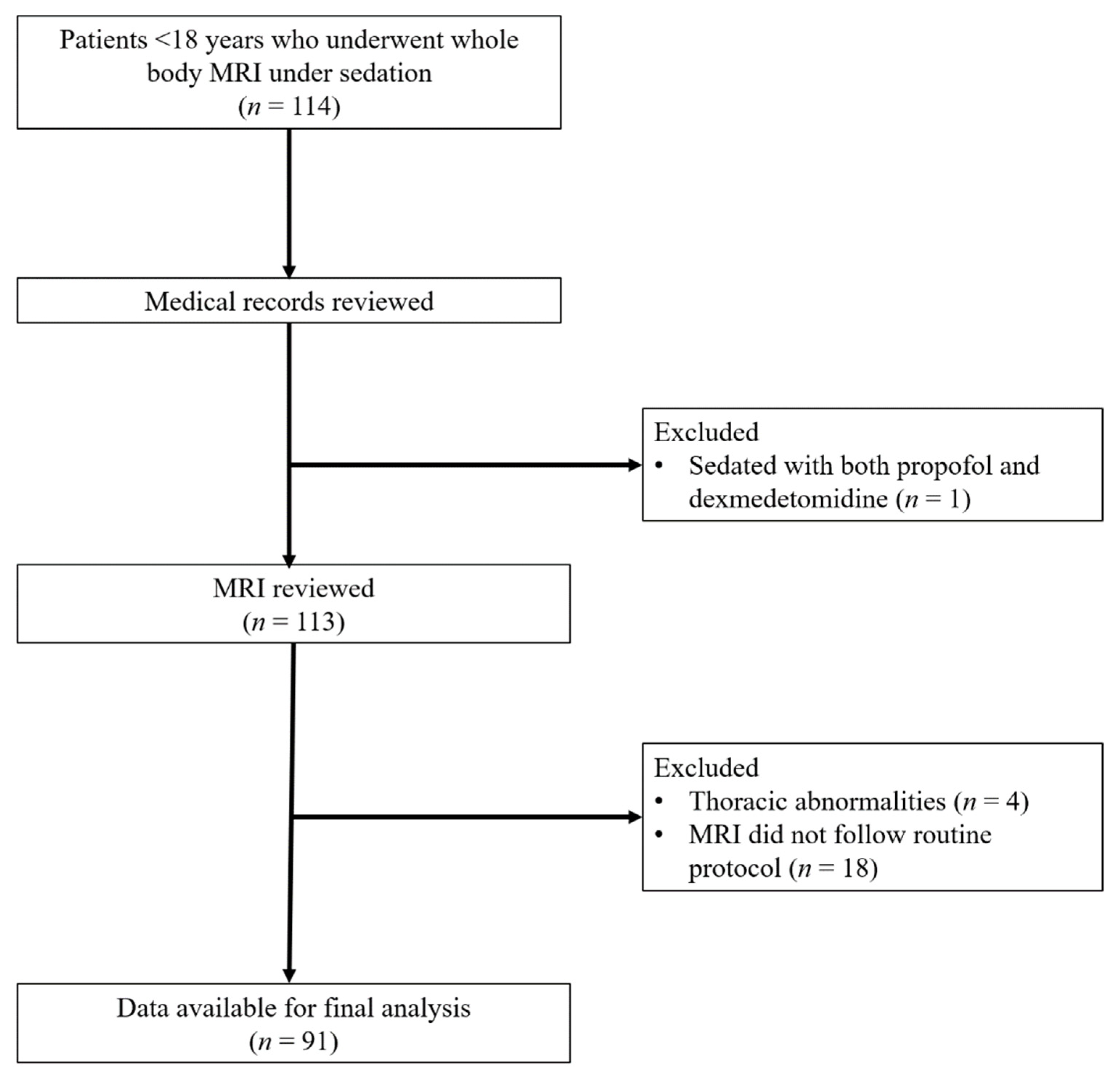
2.1. Study Population
2.2. Sedation Protocol
2.3. Image Acquisition
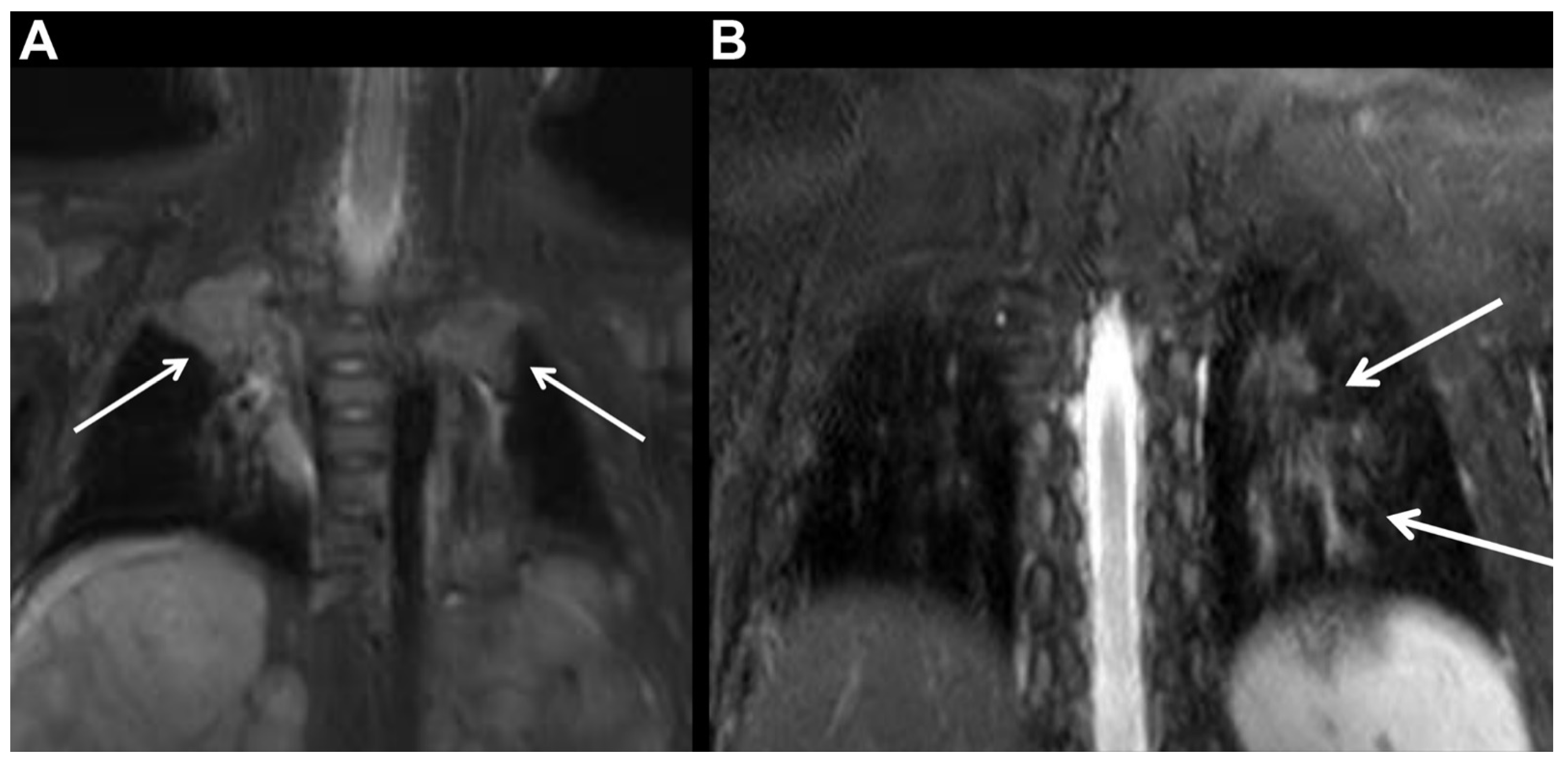
2.4. Evaluation of Atelectasis
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Supplemental Oxygen Administration and Rate of Atelectasis Occurrence
3.3. Factors Associated with Development of Atelectasis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arlachov, Y.; Ganatra, R.H. Sedation/anaesthesia in paediatric radiology. Br. J. Radiol. 2012, 85, e1018–e1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arthurs, O.J.; Sury, M. Anaesthesia or sedation for paediatric MRI: Advantages and disadvantages. Curr. Opin. Anaesthesiol. 2013, 26, 489–494. [Google Scholar] [CrossRef]
- Malviya, S.; Voepel-Lewis, T.; Eldevik, O.P.; Rockwell, D.T.; Wong, J.H.; Tait, A.R. Sedation and general anaesthesia in children undergoing MRI and CT: Adverse events and outcomes. Br. J. Anaesth. 2000, 84, 743–748. [Google Scholar] [CrossRef]
- Levati, A.; Paccagnella, F.; Pietrini, D.; Buscalferri, A.; Calamandrei, M.; Grossetti, R.; Lampugnani, E.; Stoffella, G.; Stoppa, F.; Tumolo, M.; et al. SIAARTI-SARNePI Guidelines for sedation in pediatric neuroradiology. Minerva Anestesiol. 2004, 70, 675–715. [Google Scholar] [PubMed]
- Sargent, M.A.; McEachern, A.M.; Jamieson, D.H.; Kahwaji, R. Atelectasis on pediatric chest CT: Comparison of sedation techniques. Pediatr. Radiol. 1999, 29, 509–513. [Google Scholar] [CrossRef]
- Lutterbey, G.; Wattjes, M.P.; Doerr, D.; Fischer, N.J.; Gieseke, J., Jr.; Schild, H.H. Atelectasis in children undergoing either propofol infusion or positive pressure ventilation anesthesia for magnetic resonance imaging. Paediatr. Anaesth. 2007, 17, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Hedenstierna, G.; Tokics, L.; Strandberg, A.; Lundquist, H.; Brismar, B. Correlation of gas exchange impairment to development of atelectasis during anaesthesia and muscle paralysis. Acta Anaesthesiol. Scand. 1986, 30, 183–191. [Google Scholar] [CrossRef]
- Dripps, R.D.; Van, N.D.M. Postoperative atelectasis and pneumonia: Diagnosis, etiology and management based upon 1240 cases of upper abdominal surgery. Ann. Surg. 1946, 124, 94–110. [Google Scholar] [CrossRef]
- Choe, J.W.; Jung, S.W.; Song, J.K.; Shim, E.; Choo, J.Y.; Kim, S.Y.; Hyun, J.J.; Koo, J.S.; Yim, H.J.; Lee, S.W. Predictive factors of atelectasis following endoscopic resection. Dig. Dis. Sci. 2016, 61, 181–188. [Google Scholar] [CrossRef]
- Malherbe, S.; Whyte, S.; Singh, P.; Amari, E.; King, A.; Ansermino, J.M. Total intravenous anesthesia and spontaneous respiration for airway endoscopy in children: A prospective evaluation. Paediatr. Anaesth. 2010, 20, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, D.S.; Vaux, K.K.; Ponaman, M.L.; Poss, B.W. The safe and effective use of propofol sedation in children undergoing diagnostic and therapeutic procedures: Experience in a pediatric ICU and a review of the literature. Pediatr. Emerg. Care 2003, 19, 385–392. [Google Scholar] [CrossRef]
- Koroglu, A.; Teksan, H.; Sagir, O.; Yucel, A.; Toprak, H.I.; Ersoy, O.M. A comparison of the sedative, hemodynamic, and respiratory effects of dexmedetomidine and propofol in children undergoing magnetic resonance imaging. Anesth. Analg. 2006, 103, 63–67. [Google Scholar] [CrossRef]
- Jensen, A.G.; Kalman, S.H.; Eintrei, C.; Fransson, S.G.; Morales, O. Atelectasis and oxygenation in major surgery with either propofol with or without nitrous oxide or isoflurane anaesthesia. Anaesthesia 1993, 48, 1094–1096. [Google Scholar] [CrossRef]
- Ostberg, E.; Auner, U.; Enlund, M.; Zetterstrom, H.; Edmark, L. Minimizing atelectasis formation during general anaesthesia-oxygen washout is a non-essential supplement to PEEP. Upsala J. Med. Sci. 2017, 122, 92–98. [Google Scholar] [CrossRef]
- Edmark, L.; Auner, U.; Enlund, M.; Ostberg, E.; Hedenstierna, G. Oxygen concentration and characteristics of progressive atelectasis formation during anaesthesia. Acta Anaesthesiol. Scand. 2011, 55, 75–81. [Google Scholar] [CrossRef]
- Mason, K.P. Sedation trends in the 21st century: The transition to dexmedetomidine for radiological imaging studies. Paediatr. Anaesth. 2010, 20, 265–272. [Google Scholar] [CrossRef]
- Hedenstierna, G.; Edmark, L. Mechanisms of atelectasis in the perioperative period. Best Pract. Res. Clin. Anaesthesiol. 2010, 24, 157–169. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, L.; Spahn, D.R. New concepts of atelectasis during general anaesthesia. Br. J. Anaesth. 2003, 91, 61–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joyce, C.J.; Baker, A.B.; Kennedy, R.R. Gas uptake from an unventilated area of lung: Computer model of absorption atelectasis. J. Appl. Physiol. 1993, 74, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Tokics, L.; Hedenstierna, G.; Strandberg, A.; Brismar, B.; Lundquist, H. Lung collapse and gas exchange during general anesthesia: Effects of spontaneous breathing, muscle paralysis, and positive end-expiratory pressure. Anesthesiology 1987, 66, 157–167. [Google Scholar] [CrossRef]
- Froese, A.B.; Bryan, A.C. Effects of anesthesia and paralysis on diaphragmatic mechanics in man. Anesthesiology 1974, 41, 242–255. [Google Scholar] [CrossRef] [PubMed]
- Hedenstierna, G.; Tokics, L.; Lundquist, H.; Andersson, T.; Strandberg, A.; Brismar, B. Phrenic nerve stimulation during halothane anesthesia: Effects of atelectasis. Anesthesiology 1994, 80, 751–760. [Google Scholar] [CrossRef]
- Carpagnano, G.E.; Kharitonov, S.A.; Foschino-Barbaro, M.P.; Resta, O.; Gramiccioni, E.; Barnes, P.J. Supplementary oxygen in healthy subjects and those with COPD increases oxidative stress and airway inflammation. Thorax 2004, 59, 1016–1019. [Google Scholar] [CrossRef] [Green Version]
- Kilgannon, J.H.; Jones, A.E.; Shapiro, N.I.; Angelos, M.G.; Milcarek, B.; Hunter, K.; Parrillo, J.E.; Trzeciak, S. Association between arterial hyperoxia following resuscitation from cardiac arrest and in-hospital mortality. JAMA 2010, 303, 2165–2171. [Google Scholar] [CrossRef] [Green Version]
- Balan, I.S.; Fiskum, G.; Hazelton, J.; Cotto-Cumba, C.; Rosenthal, R.E. Oximetry-guided reoxygenation improves neurological outcome after experimental cardiac arrest. Stroke 2006, 37, 3008–3013. [Google Scholar] [CrossRef] [Green Version]
- Reber, A.; Engberg, G.; Wegenius, G.; Hedenstierna, G. Lung aeration: The effect of pre-oxygenation and hyperoxygenation during total intravenous anaesthesia. Anaesthesia 1996, 51, 733–737. [Google Scholar] [CrossRef] [PubMed]
- Edmark, L.; Kostova-Aherdan, K.; Enlund, M.; Hedenstierna, G. Optimal oxygen concentration during induction of general anesthesia. Anesthesiology 2003, 98, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Young, T.P.; Lim, J.J.; Kim, T.Y.; Thorp, A.W.; Brown, L. Pediatric procedural sedation with propofol using a higher initial bolus dose. Pediatr. Emerg. Care 2014, 30, 689–693. [Google Scholar] [CrossRef]
- Rajasekaran, S.; Hackbarth, R.M.; Davis, A.T.; Kopec, J.S.; Cloney, D.L.; Fitzgerald, R.K.; Hassan, N.E.; Ndika, A.N.; Cornelius, K.; McCullough, A.; et al. The safety of propofol sedation for elective nonintubated esophagogastroduodenoscopy in pediatric patients. Pediatr. Crit. Care Med. 2014, 15, e261–e269. [Google Scholar] [CrossRef]
- Kiriyama, S.; Naitoh, H.; Kuwano, H. Propofol sedation during endoscopic treatment for early gastric cancer compared to midazolam. World J. Gastroenterol. 2014, 20, 11985–11990. [Google Scholar] [CrossRef]
- Picard, P.; Tramer, M.R. Prevention of pain on injection with propofol: A quantitative systematic review. Anesth. Analg. 2000, 90, 963–969. [Google Scholar] [CrossRef] [Green Version]
- Jager, M.D.; Aldag, J.C.; Deshpande, G.G. A presedation fluid bolus does not decrease the incidence of propofol-induced hypotension in pediatric patients. Hosp. Pediatr. 2015, 5, 85–91. [Google Scholar] [CrossRef] [Green Version]
- Mirrakhimov, A.E.; Voore, P.; Halytskyy, O.; Khan, M.; Ali, A.M. Propofol infusion syndrome in adults: A clinical update. Crit. Care Res. Pract. 2015, 2015, 260385. [Google Scholar] [CrossRef]
- Trachsel, D.; Svendsen, J.; Erb, T.O.; von Ungern-Sternberg, B.S. Effects of anaesthesia on paediatric lung function. Br. J. Anaesth. 2016, 117, 151–163. [Google Scholar] [CrossRef] [Green Version]
- von Ungern-Sternberg, B.S.; Frei, F.J.; Hammer, J.; Schibler, A.; Doerig, R.; Erb, T.O. Impact of depth of propofol anaesthesia on functional residual capacity and ventilation distribution in healthy preschool children. Br. J. Anaesth. 2007, 98, 503–508. [Google Scholar] [CrossRef] [Green Version]
- Eastwood, P.R.; Platt, P.R.; Shepherd, K.; Maddison, K.; Hillman, D.R. Collapsibility of the upper airway at different concentrations of propofol anesthesia. Anesthesiology 2005, 103, 470–477. [Google Scholar] [CrossRef] [Green Version]
- Hall, J.E.; Uhrich, T.D.; Barney, J.A.; Arain, S.R.; Ebert, T.J. Sedative, amnestic, and analgesic properties of small-dose dexmedetomidine infusions. Anesth. Analg. 2000, 90, 699–705. [Google Scholar] [CrossRef]
- Hsu, Y.W.; Cortinez, L.I.; Robertson, K.M.; Keifer, J.C.; Sum-Ping, S.T.; Moretti, E.W.; Young, C.C.; Wright, D.R.; Macleod, D.B.; Somma, J. Dexmedetomidine pharmacodynamics: Part I: Crossover comparison of the respiratory effects of dexmedetomidine and remifentanil in healthy volunteers. Anesthesiology 2004, 101, 1066–1076. [Google Scholar] [CrossRef]
- Restrepo, R.D.; Braverman, J. Current challenges in the recognition, prevention and treatment of perioperative pulmonary atelectasis. Expert Rev. Respir. Med. 2015, 9, 97–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, B.; Krane, E.J.; Gawande, R.; Holmes, T.H.; Robinson, T.E. Chest CT in children: Anesthesia and atelectasis. Pediatr. Radiol. 2014, 44, 164–172. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Propofol | Dexmedetomidine | p-Value | |
|---|---|---|---|
| No. of patients | 57 | 34 | |
| Age (months) * | 66.9 ± 43.5 | 56.2 ± 33.6 | 0.219 |
| Male:female | 27:30 | 19:15 | 0.432 |
| Height (cm) * | 107.6 ± 23.6 | 103.2 ± 19.9 | 0.362 |
| Weight (kg) * | 20.5 ± 11.8 | 18.8 ± 8.3 | 0.818 |
| Time interval between induction of sedation and initial image scanning (min) * | 17.1 ± 5.7 | 23.0 ± 5.3 | <0.001 |
| Time interval between initial and final image scanning (min) * | 37.8 ± 12.8 | 36.5 ± 8.6 | 0.568 |
| Overall image quality score on initial images * | 4.6 ± 0.6 | 4.4 ± 0.6 | 0.284 |
| Overall image quality score on final images * | 4.6 ± 0.6 | 4.34 ± 0.5 | 0.263 |
| Use of O2 | 37 (64.9%) | 1 (2.9%) | <0.001 |
| Use of adjuvant agents | 9 (15.3%) | 15 (44.1%) | 0.003 |
| Underlying disease | <0.001 | ||
| Neuroblastoma | 17 (29.8%) | 4 (11.8%) | |
| Neurofibromatosis Type I | 12 (21.1%) | 23 (67.6%) | |
| Leukemia/lymphoma | 10 (17.5%) | 0 | |
| Langerhans cell histiocytosis | 8 (14.0%) | 7 (20.6%) | |
| Other † | 10 (17.5%) | 0 |
| Supplemental Oxygen Administered | Atelectasis on Initial Images | Atelectasis on Final Images | Atelectasis on Either Initial or Final Images | |
|---|---|---|---|---|
| Propofol | 37/57 (66.7%) | 21/57 (36.8%) | 25/57 (43.9%) | 26/57 (45.6%) |
| Dexmedetomidine | 1/34 (2.9%) | 6/34 (17.6%) | 5/34 (14.7%) | 6/34 (17.6%) |
| p-value | <0.001 | 0.053 | 0.004 | 0.007 |
| Group | n | Atelectasis Grade | p-Value † | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | Any Atelectasis | I | II | III | |||
| I | Propofol + O2 (+) | 37 | 19 (51.4%) | 14 (37.8%) | 1 (2.7%) | 3 (8.1%) | 0 | 18 (48.6%) | NA | 0.015 | 0.016 |
| II | Propofol + O2 (−) | 20 | 17 (85.0%) | 3 (15.0%) | 0 | 0 | 0 | 3 (15.0%) | 0.015 | NA | 0.534 |
| III | Dexmedetomidine | 34 | 28 (82.4%) | 4 (11.8%) | 2 (5.9%) * | 0 | 0 | 6 (17.6%) | 0.016 | 0.534 | NA |
| Group | n | Atelectasis Grade | p-Value † | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | Any Atelectasis | I | II | III | |||
| I | Propofol + O2 (+) | 37 | 17 (45.9%) | 12 (32.4%) | 6 (16.2%) | 2 (5.4%) | 0 | 20 (54.1%) | NA | 0.013 | <0.001 |
| II | Propofol + O2 (−) | 20 | 15 (75.0%) | 5 (25.0%) | 0 | 0 | 0 | 5 (25.0%) | 0.013 | NA | 0.556 |
| III | Dexmedetomidine | 34 | 29 (85.3%) | 4 (11.8%) * | 1 (2.9%) | 0 | 0 | 5 (14.7%) | <0.001 | 0.556 | NA |
| Parameters | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| Unadjusted OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | |
| Age (months) | 1.008 | 0.997–1.019 | 0.157 | |||
| Sex | ||||||
| Female | Reference category | Reference category | ||||
| Male | 0.797 | 0.334–1.888 | 0.606 | |||
| Sedative type | ||||||
| Propofol | Reference category | Reference category | ||||
| Dexmedetomidine | 0.255 | 0.085–0.677 | 0.009 | 0.828 | 0.204–3.350 | 0.791 |
| Supplemental oxygen administration | 5.912 | 2.304–15.173 | <0.001 | 4.838 | 1.478–15.831 | 0.009 |
| Induction time (min) | 0.931 | 0.856–1.006 | 0.072 | 0.970 | 0.891–1.055 | 0.473 |
| Scan time (min) | 1.018 | 0.980–1.058 | 0.361 | |||
| Use of adjuvant agents | 0.692 | 0.252–1.899 | 0.474 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, P.H.; Park, Y.-S.; Yoon, H.-M.; Jung, A.Y.; Joo, E.-Y.; Choi, I.-C.; Song, M.-H. Factors Associated with Occurrence of Atelectasis during Sedation for Imaging in Pediatric Patients: A Retrospective Single Center Cohort Study. J. Clin. Med. 2021, 10, 3598. https://doi.org/10.3390/jcm10163598
Kim PH, Park Y-S, Yoon H-M, Jung AY, Joo E-Y, Choi I-C, Song M-H. Factors Associated with Occurrence of Atelectasis during Sedation for Imaging in Pediatric Patients: A Retrospective Single Center Cohort Study. Journal of Clinical Medicine. 2021; 10(16):3598. https://doi.org/10.3390/jcm10163598
Chicago/Turabian StyleKim, Pyeong Hwa, Yong-Seok Park, Hee-Mang Yoon, Ah Young Jung, Eun-Young Joo, In-Cheol Choi, and Myung-Hee Song. 2021. "Factors Associated with Occurrence of Atelectasis during Sedation for Imaging in Pediatric Patients: A Retrospective Single Center Cohort Study" Journal of Clinical Medicine 10, no. 16: 3598. https://doi.org/10.3390/jcm10163598