
Global Variations in the Mineral Content of Bottled Still and Sparkling Water and a Description of the Possible Impact on Nephrological and Urological Diseases

 , , , , , , , , add
Show full author list
, , , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rukin, N.J.; Siddiqui, Z.A.; Chedgy, E.C.P.; Somani, B.K. Trends in Upper Tract Stone Disease in England: Evidence from the Hospital Episodes Statistics Database. Urol. Int. 2017, 98, 391–396. [Google Scholar] [CrossRef]
- Wong, Y.; Cook, P.; Roderick, P.; Somani, B.K. Metabolic Syndrome and Kidney Stone Disease: A Systematic Review of Literature. J. Endourol. 2016, 30, 246–253. [Google Scholar] [CrossRef]
- Sorokin, I.; Mamoulakis, C.; Miyazawa, K.; Rodgers, A.; Talati, J.; Lotan, Y. Epidemiology of stone disease across the world. World J. Urol. 2017, 35, 1301–1320. [Google Scholar] [CrossRef]
- Ferraro, P.M.; Curhan, G.C.; D’Addessi, A.; Gambaro, G. Risk of recurrence of idiopathic calcium kidney stones: Analysis of data from the literature. J. Nephrol. 2017, 30, 227–233. [Google Scholar] [CrossRef]
- Ferraro, P.M.; Taylor, E.N.; Eisner, B.H.; Gambaro, G.; Rimm, E.B.; Mukamal, K.J.; Curhan, G.C. History of kidney stones and the risk of coronary heart disease. JAMA 2013, 310, 408–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cupisti, A.; D’Alessandro, C.; Samoni, S.; Meola, M.; Egidi, M.F. Nephrolithiasis and hypertension: Possible links and clinical implications. J. Nephrol. 2014, 27, 477–482. [Google Scholar] [CrossRef]
- Kim, S.Y.; Bang, W.J.; Min, C.; Choi, H.G. Association of nephrolithiasis with the risk of cardiovascular diseases: A longitudinal follow-up study using a national health screening cohort. BMJ Open 2020, 10, e040034. [Google Scholar] [CrossRef]
- Sakhaee, K. Nephrolithiasis as a systemic disorder. Curr. Opin. Nephrol. Hypertens. 2008, 17, 304–309. [Google Scholar] [CrossRef]
- Borghi, L.; Meschi, T.; Amato, F.; Briganti, A.; Novarini, A.; Giannini, A. Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: A 5-year randomized prospective study. J. Urol. 1996, 155, 839–843. [Google Scholar] [CrossRef]
- Skolarikos, A.; Straub, M.; Knoll, T.; Sarica, K.; Seitz, C.; Petřík, A.; Türk, C. Metabolic evaluation and recurrence prevention for urinary stone patients: Eau guidelines. Eur. Urol. 2015, 67, 750–763. [Google Scholar] [CrossRef]
- Pak, C.Y.C.; Sakhaee, K.; Crowther, C.; Brinkley, L. Evidence justifying a high fluid intake in treatment of nephrolithiasis. Ann. Intern. Med. 1980, 93, 36–39. [Google Scholar] [CrossRef]
- Gamage, K.N.; Jamnadass, E.; Sulaiman, S.K.; Pietropaolo, A.; Aboumarzouk, O.; Somani, B.K. The role of fluid intake in the prevention of kidney stone disease: A systematic review over the last two decades. Türk Üroloji Dergisi/Turkish J. Urol. 2020, 46, S92–S103. [Google Scholar] [CrossRef]
- Clark, W.F.; Moist, L.; Sontrop, J.M.; Huang, S.-H.; Bouby, N.; Bankir, L. Hydration and Chronic Kidney Disease Progression: A Critical Review of the Evidence. Am. J. Nephrol. 2016, 43, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Vannucci, L.; Fossi, C.; Quattrini, S.; Guasti, L.; Pampaloni, B.; Gronchi, G.; Giusti, F.; Romagnoli, C.; Cianferotti, L.; Marcucci, G.; et al. Calcium Intake in Bone Health: A Focus on Calcium-Rich Mineral Waters. Nutrients 2018, 10, 1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wynn, E.; Krieg, M.-A.; Aeschlimann, J.-M.; Burckhardt, P. Alkaline mineral water lowers bone resorption even in calcium sufficiency. Bone 2009, 44, 120–124. [Google Scholar] [CrossRef]
- Jiang, L.; He, P.; Chen, J.; Liu, Y.; Liu, D.; Qin, G.; Tan, N. Magnesium Levels in Drinking Water and Coronary Heart Disease Mortality Risk: A Meta-Analysis. Nutrients 2016, 8, 5. [Google Scholar] [CrossRef] [Green Version]
- Coe, F.L.; Worcester, F.L.C.E.M.; Evan, A.P. Idiopathic hypercalciuria and formation of calcium renal stones. Nat. Rev. Nephrol. 2016, 12, 519–533. [Google Scholar] [CrossRef] [Green Version]
- Ferraro, P.M.; Bargagli, M.; Trinchieri, A.; Gambaro, G. Risk of Kidney Stones: Influence of Dietary Factors, Dietary Patterns, and Vegetarian–Vegan Diets. Nutrients 2020, 12, 779. [Google Scholar] [CrossRef] [Green Version]
- Prezioso, D.; Strazzullo, P.; Lotti, T.; Bianchi, G.; Borghi, L.; Caione, P.; Carini, M.; Caudarella, R.; Gambaro, G.; Gelosa, M.; et al. Dietary treatment of urinary risk factors for renal stone formation. A review of CLU Working Group. Arch. Ital. Urol. Androl. 2015, 87, 105–120. [Google Scholar] [CrossRef]
- Goldfarb, D.S. Empiric therapy for kidney stones. Urolithiasis 2019, 47, 107–113. [Google Scholar] [CrossRef]
- Ferraro, P.M.; Taylor, E.N.; Gambaro, G.; Curhan, G.C. Soda and Other Beverages and the Risk of Kidney Stones. Clin. J. Am. Soc. Nephrol. CJASN 2013, 8, 1389–1395. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, F.M.; Garcia, S.G.; Corro, R.J.; Liesa, M.S.; Barón, F.R.; Martín, F.S.; Feu, O.A.; Rodríguez, R.M.; Mavrich, H.V. Análisis de las aguas embotelladas y de grifo españolas y de las implicaciones de su consumo en la litiasis urinaria. Actas Urol. Esp. 2009, 33, 778–793. [Google Scholar] [CrossRef] [Green Version]
- Hubert, J. Drinking water: Which type should be chosen? Prog. Urol. 2010, 20, 806–809. [Google Scholar] [CrossRef]
- Azoulay, A.; Garzon, P.; Eisenberg, M.J. Comparison of the mineral content of tap water and bottled waters. J. Gen. Intern. Med. 2001, 16, 168–175. [Google Scholar] [CrossRef]
- Stoots, S.J.; Geraghty, R.; Kamphuis, G.M.; Jamnadass, E.; Henderickx, M.M.; Ventimiglia, E.; Traxer, O.; Keller, E.X.; De Coninck, V.; Talso, M.; et al. Variations in the Mineral Content of Bottled “Still” Water Across Europe: Comparison of 182 Brands Across 10 Countries. J. Endourol. 2021, 35, 206–214. [Google Scholar] [CrossRef]
- Stoots, S.J.; Geraghty, R.; Kamphuis, G.M.; Jamnadass, E.; Henderickx, M.M.; Ventimiglia, E.; Traxer, O.; Keller, E.X.; De Coninck, V.; Talso, M.; et al. Variations in the mineral content of bottled ‘carbonated or sparkling’ water across Europe: A comparison of 126 brands across 10 countries. Cent. Eur. J. Urol. 2021, 74, 71–75. [Google Scholar] [CrossRef]
- Costi, D.; Calcaterra, P.G.; Iori, N.; Vourna, S.; Nappi, G.; Passeri, M. Importance of bioavailable calcium drinking water for the maintenance of bone mass in post-menopausal women. J. Endocrinol. Investig. 1999, 22, 852–856. [Google Scholar] [CrossRef]
- Bushinsky, D.A.; Frick, K.K. The effects of acid on bone. Curr. Opin. Nephrol. Hypertens. 2000, 9, 369–379. [Google Scholar] [CrossRef]
- Xiao, Q.; Murphy, R.A.; Houston, D.; Harris, T.B.; Chow, W.-H.; Park, Y. Dietary and supplemental calcium intake and cardiovascular disease mortality. JAMA Intern. Med. 2013, 173, 639–646. [Google Scholar] [CrossRef]
- Michaëlsson, K.; Melhus, H.; Lemming, E.W.; Wolk, A.; Byberg, L. Long term calcium intake and rates of all cause and cardiovascular mortality: Community based prospective longitudinal cohort study. BMJ 2013, 346, f228. [Google Scholar] [CrossRef] [Green Version]
- Chung, M.; Tang, A.M.; Fu, Z.; Wang, D.D.; Newberry, S.J. Calcium Intake and Cardiovascular Disease Risk. Ann. Intern. Med. 2016, 165, 856–866. [Google Scholar] [CrossRef] [Green Version]
- Myung, S.-K.; Kim, H.-B.; Lee, Y.-J.; Choi, Y.-J.; Oh, S.-W. Calcium Supplements and Risk of Cardiovascular Disease: A Meta-Analysis of Clinical Trials. Nutrients 2021, 13, 368. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Shi, X.; Xia, H.; Yang, X.; Liu, H.; Pan, D.; Sun, G. The Evidence and Controversy Between Dietary Calcium Intake and Calcium Supplementation and the Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Cohort Studies and Randomized Controlled Trials. J. Am. Coll. Nutr. 2019, 39, 352–370. [Google Scholar] [CrossRef]
- Ferraro, P.M.; Ticinesi, A.; Meschi, T.; Rodgers, A.; Di Maio, F.; Fulignati, P.; Borghi, L.; Gambaro, G. Short-Term Changes in Urinary Relative Supersaturation Predict Recurrence of Kidney Stones: A Tool to Guide Preventive Measures in Urolithiasis. J. Urol. 2018, 200, 1082–1087. [Google Scholar] [CrossRef]
- Borghi, L.; Schianchi, T.; Meschi, T.; Guerra, A.; Allegri, F.; Maggiore, U.; Novarini, A. Comparison of Two Diets for the Prevention of Recurrent Stones in Idiopathic Hypercalciuria. N. Engl. J. Med. 2002, 346, 77–84. [Google Scholar] [CrossRef]
- Curhan, G.C.; Willett, W.C.; Rimm, E.B.; Stampfer, M.J. A Prospective Study of Dietary Calcium and Other Nutrients and the Risk of Symptomatic Kidney Stones. N. Engl. J. Med. 1993, 328, 833–838. [Google Scholar] [CrossRef]
- Ticinesi, A.; Nouvenne, A.; Maalouf, N.M.; Borghi, L.; Meschi, T. Salt and nephrolithiasis. Nephrol. Dial. Transplant. 2016, 31, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Nouvenne, A.; Meschi, T.; Prati, B.; Guerra, A.; Allegri, F.; Vezzoli, G.; Soldati, L.; Gambaro, G.; Maggiore, U.; Borghi, L. Effects of a low-salt diet on idiopathic hypercalciuria in calcium-oxalate stone formers: A 3-mo randomized controlled trial. Am. J. Clin. Nutr. 2009, 91, 565–570. [Google Scholar] [CrossRef] [Green Version]
- Bonny, O.; Edwards, A. Calcium reabsorption in the distal tubule: Regulation by sodium, pH, and flow. Am. J. Physiol. Physiol. 2013, 304, F585–F600. [Google Scholar] [CrossRef]
- Mente, A.; O’Donnell, M.; Rangarajan, S.; McQueen, M.; Dagenais, G.; Wielgosz, A.; Lear, S.; Ah, S.T.L.; Wei, L.; Diaz, R.; et al. Urinary sodium excretion, blood pressure, cardiovascular disease, and mortality: A community-level prospective epidemiological cohort study. Lancet 2018, 392, 496–506. [Google Scholar] [CrossRef]
- Keßler, T.; Hesse, A. Cross-over study of the influence of bicarbonate-rich mineral water on urinary composition in comparison with sodium potassium citrate in healthy male subjects. Br. J. Nutr. 2000, 84, 865–871. [Google Scholar] [CrossRef] [Green Version]
- Karagülle, O.; Smorag, U.; Candir, F.; Gundermann, G.; Jonas, U.; Becker, A.J.; Gehrke, A.; Gutenbrunner, C. Clinical study on the effect of mineral waters containing bicarbonate on the risk of urinary stone formation in patients with multiple episodes of CaOx-urolithiasis. World J. Urol. 2007, 25, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Tavasoli, S.; Taheri, M.; Taheri, F.; Basiri, A.; Amiri, F.B. Evaluating the associations between urinary excretion of magnesium and that of other components in calcium stone-forming patients. Int. Urol. Nephrol. 2018, 51, 279–284. [Google Scholar] [CrossRef]
- Glasdam, S.-M.; Glasdam, S.; Peters, G.H. The Importance of Magnesium in the Human Body. Adv. Virus Res. 2016, 73, 169–193. [Google Scholar] [CrossRef] [Green Version]
- Del Gobbo, L.C.; Imamura, F.; Wu, J.H.Y.; Otto, M.C.D.O.; E Chiuve, S.; Mozaffarian, D. Circulating and dietary magnesium and risk of cardiovascular disease: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2013, 98, 160–173. [Google Scholar] [CrossRef] [Green Version]
- Pickering, R.; Bradlee, M.; Singer, M.; Moore, L. Higher Intakes of Potassium and Magnesium, but Not Lower Sodium, Reduce Cardiovascular Risk in the Framingham Offspring Study. Nutrients 2021, 13, 269. [Google Scholar] [CrossRef] [PubMed]
- Leenders, N.H.; Vermeulen, E.A.; van Ballegooijen, A.J.; Hoekstra, T.; de Vries, R.; Beulens, J.W.; Vervloet, M.G. The association between circulating magnesium and clinically relevant outcomes in patients with chronic kidney disease: A systematic review and meta-analysis. Clin. Nutr. 2021, 40, 3133–3147. [Google Scholar] [CrossRef]
- Gianfredi, V.; Bragazzi, N.L.; Nucci, D.; Villarini, M.; Moretti, M. Cardiovascular diseases and hard drinking waters: Implications from a systematic review with meta-analysis of case-control studies. J. Water Health 2016, 15, 31–40. [Google Scholar] [CrossRef]
- Ferraro, P.M.; Mandel, E.I.; Curhan, G.C.; Gambaro, G.; Taylor, E.N. Dietary Protein and Potassium, Diet–Dependent Net Acid Load, and Risk of Incident Kidney Stones. Clin. J. Am. Soc. Nephrol. 2016, 11, 1834–1844. [Google Scholar] [CrossRef]
- Pearle, M.S.; Goldfarb, D.; Assimos, D.G.; Curhan, G.; Denu-Ciocca, C.J.; Matlaga, B.R.; Monga, M.; Penniston, K.L.; Preminger, G.M.; Turk, T.M.; et al. Medical Management of Kidney Stones: AUA Guideline. J. Urol. 2014, 192, 316–324. [Google Scholar] [CrossRef]
- Türk, C.; Neisius, A.; Petřík, A.; Seitz, C.; Thomas, K.; Skolarikos, A. EAU Guidelines on Urolithiasis 2020. In European Association of Urology Guidelines, 2020th ed.; vol presented at the EAU Annual Congress Amsterdam 2020; The European Association of Urology Guidelines Office: Arnhem, The Netherlands, 2020. [Google Scholar]
- Qian, N. Bottled Water or Tap Water? A Comparative Study of Drinking Water Choices on University Campuses. Water 2018, 10, 59. [Google Scholar] [CrossRef] [Green Version]
- Brei, V.A. How is a bottled water market created? WIREs Water 2018, 5, e1220. [Google Scholar] [CrossRef]
- Arnold, E.; Larsen, J. Bottled Water: Pouring Resources down the Drain. 2006. Available online: http://www.earth-policy.org/plan_b_updates/2006/update51/a/p (accessed on 20 May 2021).
- Frassetto, L.; Morris, R.C., Jr.; Sellmeyer, D.E.; Todd, K.; Sebastian, A. Diet, evolution and aging–the pathophysiologic effects of the post-agricultural inversion of the potassium-to-sodium and base-to-chloride ratios in the human diet. Eur. J. Nutr. 2001, 40, 200–213. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
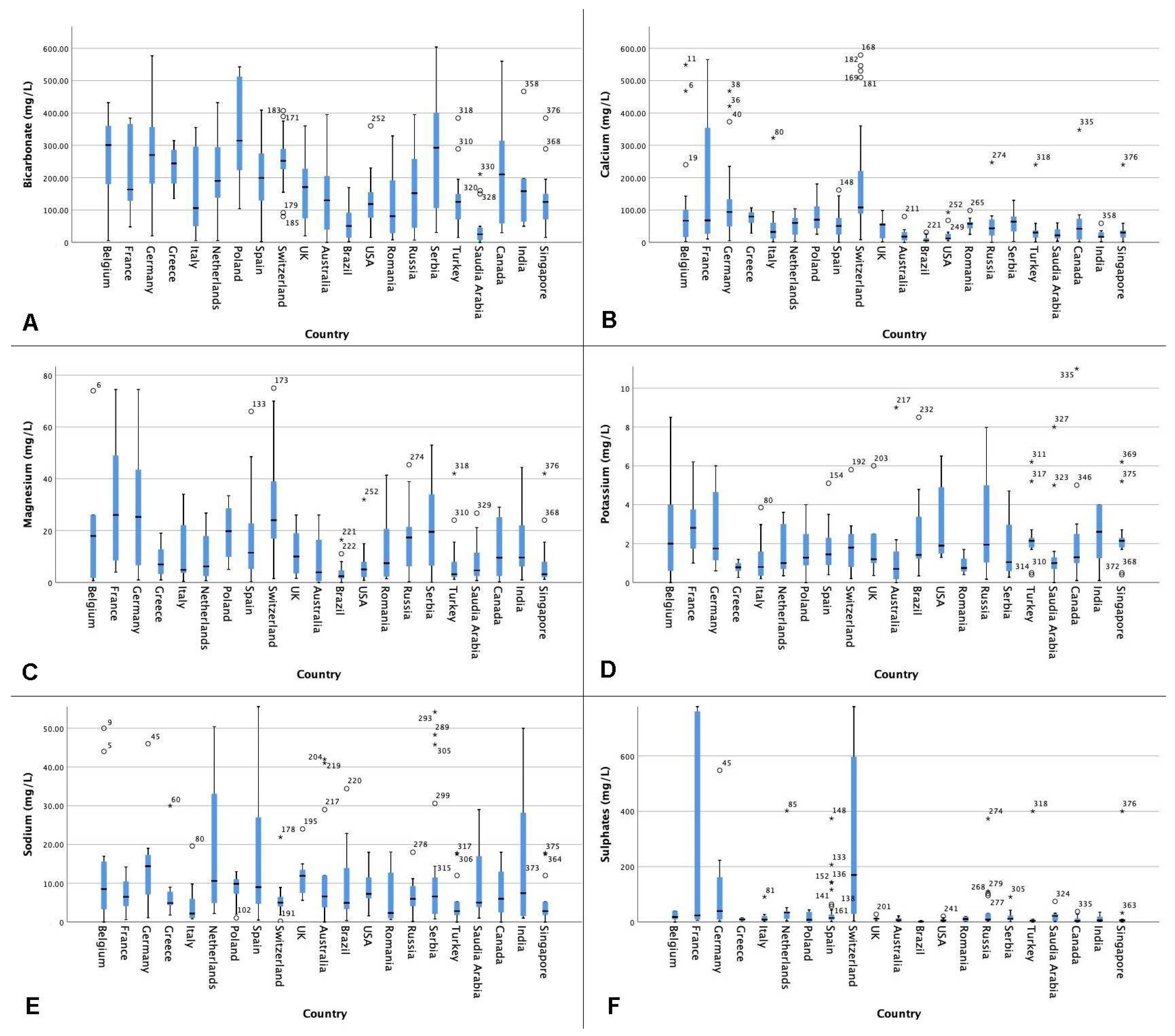
| Country | Mineral Composition (mg/L) | |||||
|---|---|---|---|---|---|---|
| Bicarbonate | Calcium | Magnesium | Potassium | Sodium | Sulphates | |
| Australia | 130.00 (34.00–258.00) | 18.00 (6.40–31.95) | 3.95 (0.525–16.50) | 0.70 (0.17–1.60) | 6.60 (3.79–12.00) | 6.55 (3.40–14.00) |
| Belgium | 301.00 (180.00–360.00) | 66.80 (16.50–101.00) | 18.00 (1.80–26.00) | 2.00 (0.60–4.00) | 8.50 (3.25–15.60) | 18.00 (10.00–40.00) |
| Brazil | 50.71 (13.20–95.49) | 5.78 (3.43–13.30) | 2.42 (1.55–4.71) | 1.42 (1.22–4.00) | 4.95 (3.34–13.93) | 1.56 (0.93–2.95) |
| Canada | 210.00 (35.00–330.00) | 42.00 (7.00–73.00) | 9.60 (2.50–25.15) | 1.30 (1.00–3.00) | 6.00 (2.48–13.00) | 4.10 (1.50–12.55) |
| France | 163.50 (127.00–372.00) | 68.00 (19.00–468.00) | 26.00 (8.00–56.00) | 2.80 (1.60–4.00) | 6.50 (3.00–11.60) | 24.00 (8.10–1121) |
| Germany | 270.00 (182.00–356.50) | 94.00 (47.00–142.00) | 25.25 (6.65–43.50) | 1.75 (1.15–4.65) | 14.40 (7.10–17.30) | 39.55 (9.00–162.00) |
| Greece | 244.00 (182.00–286.00) | 79.65 (60.00–93.10) | 7.00 (3.30–12.80) | 0.79 (0.60–1.00) | 4.90 (4.35–7.80) | 9.15 (5.00–14.00) |
| India | 158.50 (64.00–196.80) | 17.00 (13.60–33.60) | 9.65 (6.20–22.00) | 2.60 (0.50–4.00) | 7.45 (1.55–28.2) | 6.00 (3.20–19.30) |
| Italy | 106.00 (50.00–296.00) | 32.20 (11.80–60.36) | 4.90 (3.70–22.10) | 0.80 (0.35–1.60) | 2.20 (1.00–6.00) | 8.60 (6.00–22.00) |
| The Netherlands | 190.00 (106.00–305.00) | 60.00 (15.00–80.00) | 6.25 (2.46–18.00) | 1.00 (0.60–3.30) | 10.60 (4.80–36.20) | 34.00 (10.00–40.00) |
| Poland | 314.45 (223.40–512.45) | 70.13 (43.85–111.20) | 19.75 (9.92–28.55) | 1.28 (0.89–2.50) | 9.85 (7.28–11.05) | 7.94 (0.00–36.25) |
| Romania | 81.11 (28.00–192.03) | 57.85 (43.50–62.77) | 7.50 (2.21–20.60) | 0.75 (0.40–1.70) | 2.33 (0.93–12.74) | 10.70 (2.10–19.29) |
| Russia | 152.00 (45.00–258.00) | 43.30 (21.20–70.60) | 17.40 (6.22–21.40) | 1.95 (1.03–5.00) | 5.96 (4.10–9.29) | 8.50 (6.12–31.00) |
| Saudi Arabia | 25.00 (6.10–50.00) | 21.50 (12.00–40.50) | 4.70 (2.00–13.00) | 1.00 (0.70–1.40) | 5.00 (3.80–17.00) | 21.80 (4.00–30.00) |
| Serbia | 292.5 (106.00–400.80) | 64.01 (33.82–79.90) | 19.50 (6.50–34.00) | 1.05 (0.59–2.96) | 6.60 (2.10–11.50) | 11.55 (7.15–23.00) |
| Singapore | 125.00 (71.00–150.00) | 30.50 (15.00–37.10) | 3.20 (2.10–8.00) | 2.15 (1.80–2.30) | 2.80 (1.80–5.20) | 6.00 (3.00–9.10) |
| Spain | 199.30 (129.20–275.00) | 50.79 (24.25–75.25) | 11.50 (5.00–23.40) | 1.45 (0.90–2.30) | 9.00 (4.70–27.00) | 14.40 (8.10–26.75) |
| Switzerland | 252.00 (226.30–289.00) | 108.00 (89.00–221.00) | 24.00 (17.00–39.00) | 1.80 (0.80–2.50) | 5.00 (4.00–6.50) | 170.00 (29.50–597.00) |
| Turkey | 125.00 (71.00–150.00) | 30.50 (15.00–37.10) | 3.20 (2.10–8.00) | 2.15 (1.80–2.30) | 2.80 (1.80–5.20) | 4.50 (2.90–8.60) |
| The United Kingdom | 171.00 (74.00–240.00) | 55.00 (12.00–59.00) | 10.05 (3.50–19.00) | 1.20 (1.00–2.50) | 11.90 (7.03–15.00) | 12.00 (9.00–14.00) |
| The United States | 118.50 (76.00–155.00) | 12.00 (8.70–26.20) | 5.05 (2.10–8.05) | 1.90 (1.50–4.90) | 7.25 (6.15–11.55) | 5.65 (3.80–10.00) |
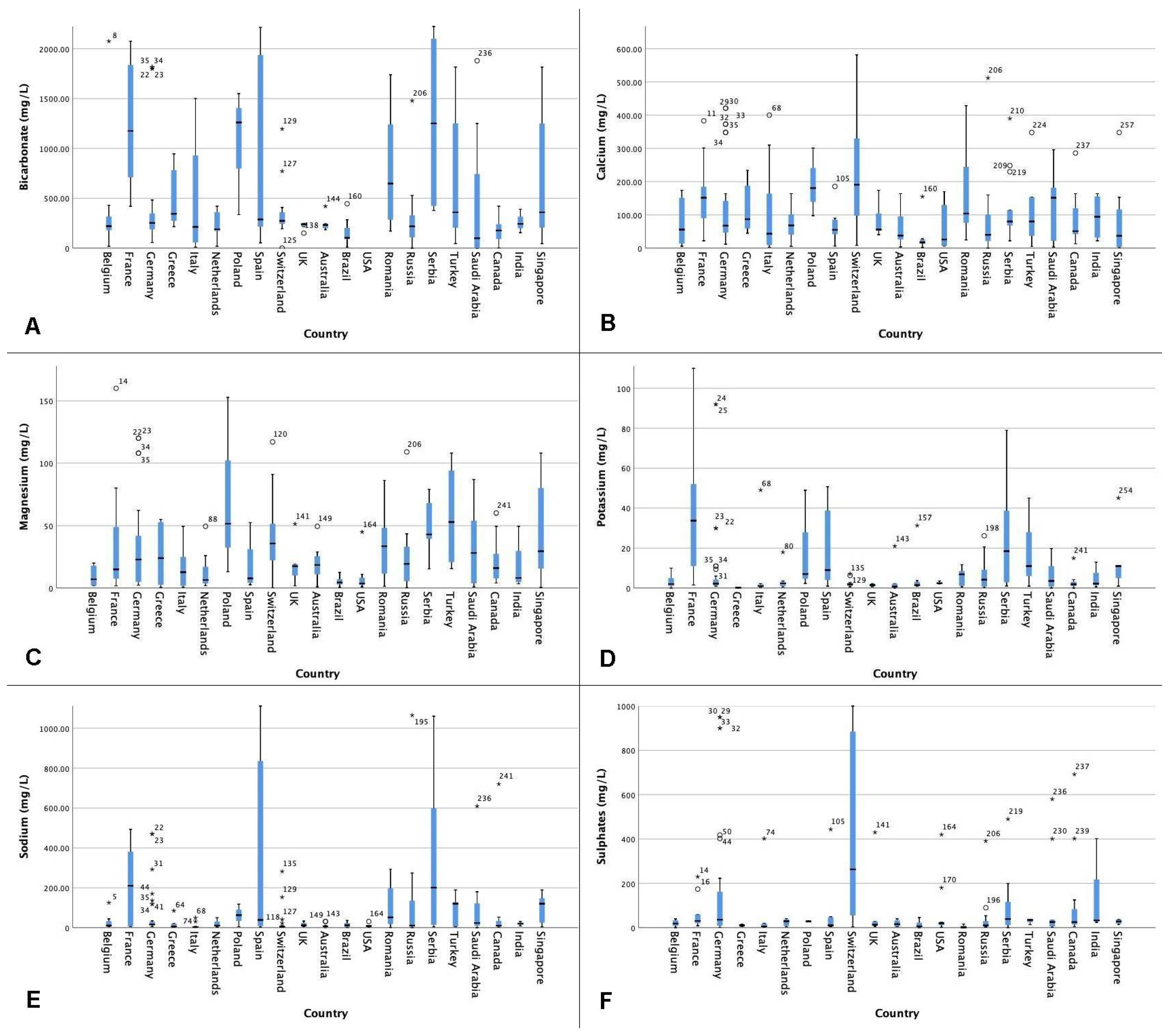
| Country | Mineral Composition (mg/L) | |||||
|---|---|---|---|---|---|---|
| Bicarbonate | Calcium | Magnesium | Potassium | Sodium | Sulphates | |
| Australia | 233.00 (200.00–243.00) | 37.75 (25.98–95.60) | 19.00 (4.00–29.00) | 1.00 (0.00–2.00) | 7.00 (1.90–10.00) | 16.00 (6.00–33.00) |
| Belgium | 22.00 (180.00–317.00) | 56.00 (13.50–151.50) | 7.00 (2.00–18.00) | 2.00 (1.00–5.00) | 10.60 (9.00–33.30) | 19.00 (8.00–33.00) |
| Brazil | 102.84 (91.41–203.28) | 17.14 (13.90–26.05) | 4.00 (3.00–7.00) | 1.00 (1.00–3.00) | 11.80 (3.98–23.02) | 6.00 (2.00–38.00) |
| Canada | 176.60 (77.00–243.00) | 51.00 (42.00–150.00) | 16.00 (6.00–29.00) | 2.00 (1.00–4.00) | 10.00 (6.00–36.10) | 25.00 (11.00–125.00) |
| France | 1175.00 (710.00–1837.00) | 151.50 (90.00–185.00) | 15.00 (8.00–49.00) | 34.00 (11.00–52.00) | 210.00 (7.47–381.00) | 30.00 (20.00–59.00) |
| Germany | 253.00 (189.00–349.00) | 67.50 (47.00–142.00) | 23.00 (5.00–42.00) | 2.00 (1.00–4.00) | 15.80 (13.30–29.90) | 36.00 (9.00–162.00) |
| Greece | 344.15 (274.00–781.00) | 87.20 (59.30–188.00) | 24.00 (3.00–53.00) | 0.00 (0.00–0.00) | 6.02 (4.43–20.00) | 11.00 (5.00–12.00) |
| India | 243.00 (155.00–390.00) | 94.30 (3.65–155.65) | 8.00 (5.00–30.00) | 2.00 (1.00–13.00) | 20.00 (9.00–31.20) | 33.00 (24.00–402.00) |
| Italy | 212.55 (57.40–930.00) | 43.50 (9.10–164.00) | 13.00 (2.00–25.00) | 1.00 (1.00–2.00) | 3.07 (1.50–6.00) | 6.00 (4.00–18.00) |
| The Netherlands | 190.00 (170.00–360.00) | 68.50 (40.90–101.50) | 7.00 (3.00–18.00) | 2.00 (1.00–3.00) | 10.30 (6.00–30.60) | 29.00 (9.00–37.00) |
| Poland | 1260.00 (335.60–1550.00) | 180.90 (97.80–301.00) | 52.00 (13.00–153.00) | 7.00 (2.00–49.00) | 63.00 (4.59–118.00) | 29.00 (27.00–32.00) |
| Romania | 648.00 (244.00–1364.50) | 104.00 (74.85–252.60) | 34.00 (11.00–49.00) | 7.00 (1.00–9.00) | 51.40 (15.41–205.00) | 1.00 (1.00–16.00) |
| Russia | 218.50 (107.00–330.00) | 40.20 (21.60–101.00) | 19.00 (6.00–33.00) | 4.00 (1.00–9.00) | 10.41 (4.90–135.00) | 10.00 (5.00–30.00) |
| Saudi Arabia | 100.00 (0.00–744.00) | 151.50 (22.00–182.00) | 28.00 (4.00–54.00) | 4.00 (1.00–11.00) | 23.50 (9.60–122.00) | 25.00 (5.00–35.00) |
| Serbia | 1251.00 (423.00–2100.00) | 80.00 (67.84–114.00) | 43.00 (40.00–68.00) | 19.00 (3.00–39.00) | 200.70 (14.10–598.00) | 39.00 (11.00–116.00) |
| Singapore | 360.00 (205.00–1250.00) | 37.10 (1.00–153.00) | 30.00 (16.00–80.00) | 11.00 (5.00–11.00) | 120.50 (24.75–148.00) | 28.00 (18.00–37.00) |
| Spain | 287.00 (215.50–1935.50) | 55.00 (32.00–86.80) | 8.00 (4.00–31.00) | 9.00 (3.00–49.00) | 38.80 (7.55–835.50) | 11.00 (7.00–48.00) |
| Switzerland | 273.50 (243.50–360.50) | 191.00 (97.70–330.00) | 36.00 (22.00–52.00) | 2.00 (1.00–3.00) | 5.20 (4.00–7.00) | 263.00 (55.00–885.00) |
| Turkey | 360.00 (205.00–1250.00) | 80.00 (37.10–153.00) | 53.00 (21.00–94.00) | 11.00 (6.00–28.00) | 120.50 (6.50–128.00) | 35.00 (14.00–38.00) |
| The United Kingdom | 240.00 (215.00–245.00) | 56.00 (55.00–104.00) | 18.00 (10.00–19.00) | 2.00 (1.00–2.00) | 11.50 (7.47–24.00) | 13.00 (9.00–28.00) |
| The United States | n.a. | 25.95 (6.65–130.00) | 4.00 (2.00–8.00) | 2.00 (2.00–4.00) | 8.30 (3.30–11.00) | 20.00 (11.00–26.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoots, S.J.M.; Kamphuis, G.M.; Geraghty, R.; Vogt, L.; Henderickx, M.M.E.L.; Hameed, B.M.Z.; Ibrahim, S.; Pietropaolo, A.; Jamnadass, E.; Aljumaiah, S.M.; et al. Global Variations in the Mineral Content of Bottled Still and Sparkling Water and a Description of the Possible Impact on Nephrological and Urological Diseases. J. Clin. Med. 2021, 10, 2807. https://doi.org/10.3390/jcm10132807
Stoots SJM, Kamphuis GM, Geraghty R, Vogt L, Henderickx MMEL, Hameed BMZ, Ibrahim S, Pietropaolo A, Jamnadass E, Aljumaiah SM, et al. Global Variations in the Mineral Content of Bottled Still and Sparkling Water and a Description of the Possible Impact on Nephrological and Urological Diseases. Journal of Clinical Medicine. 2021; 10(13):2807. https://doi.org/10.3390/jcm10132807
Chicago/Turabian StyleStoots, Simone J. M., Guido M. Kamphuis, Rob Geraghty, Liffert Vogt, Michaël M. E. L. Henderickx, B. M. Zeeshan Hameed, Sufyan Ibrahim, Amelia Pietropaolo, Enakshee Jamnadass, Sahar M. Aljumaiah, and et al. 2021. "Global Variations in the Mineral Content of Bottled Still and Sparkling Water and a Description of the Possible Impact on Nephrological and Urological Diseases" Journal of Clinical Medicine 10, no. 13: 2807. https://doi.org/10.3390/jcm10132807