
Preoperative Routine Laboratory Markers for Predicting Postoperative Recurrence and Death in Patients with Breast Cancer

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
3. Results
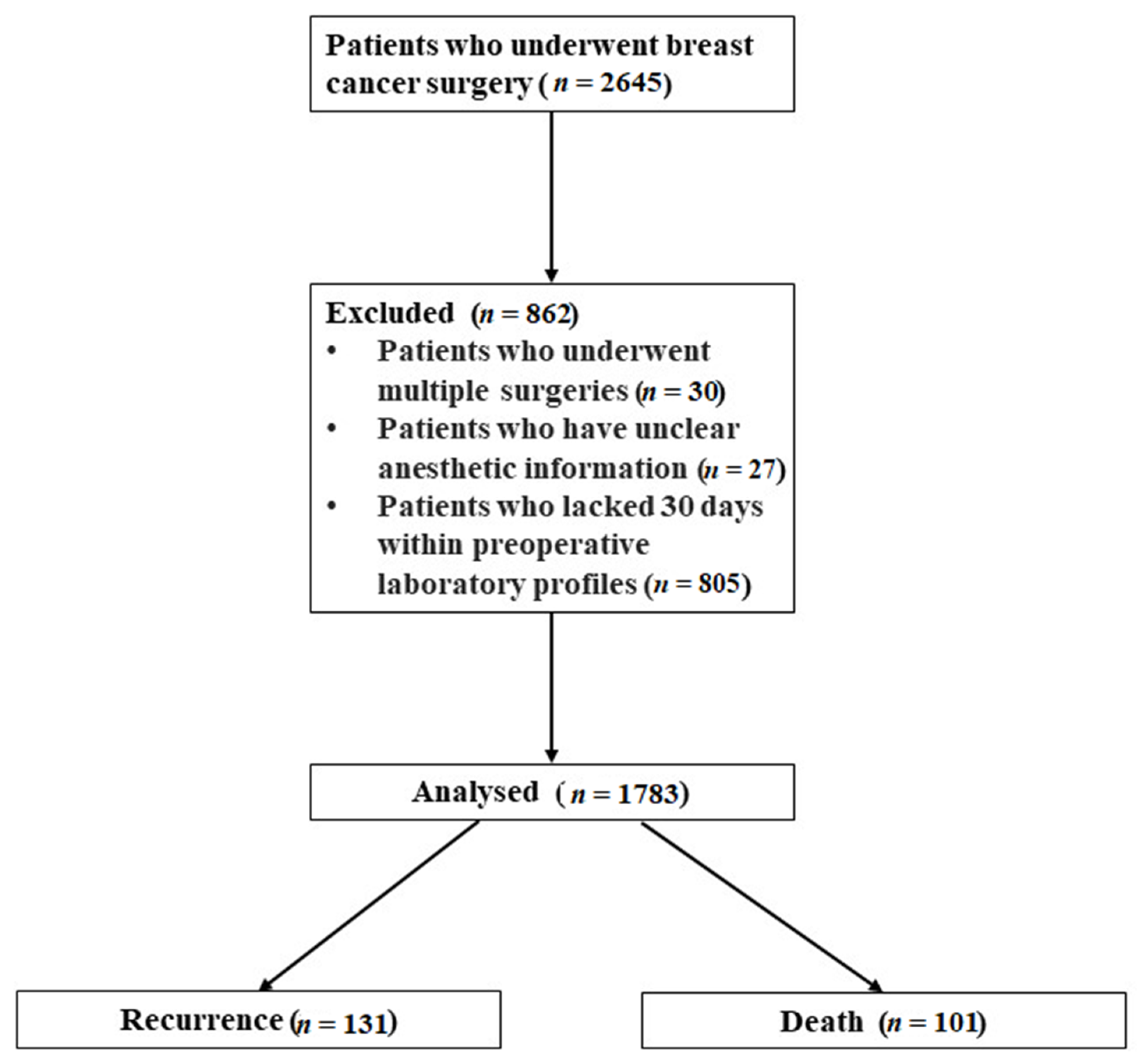
3.1. Subjects
3.2. Comparison of Patients’ Characteristics
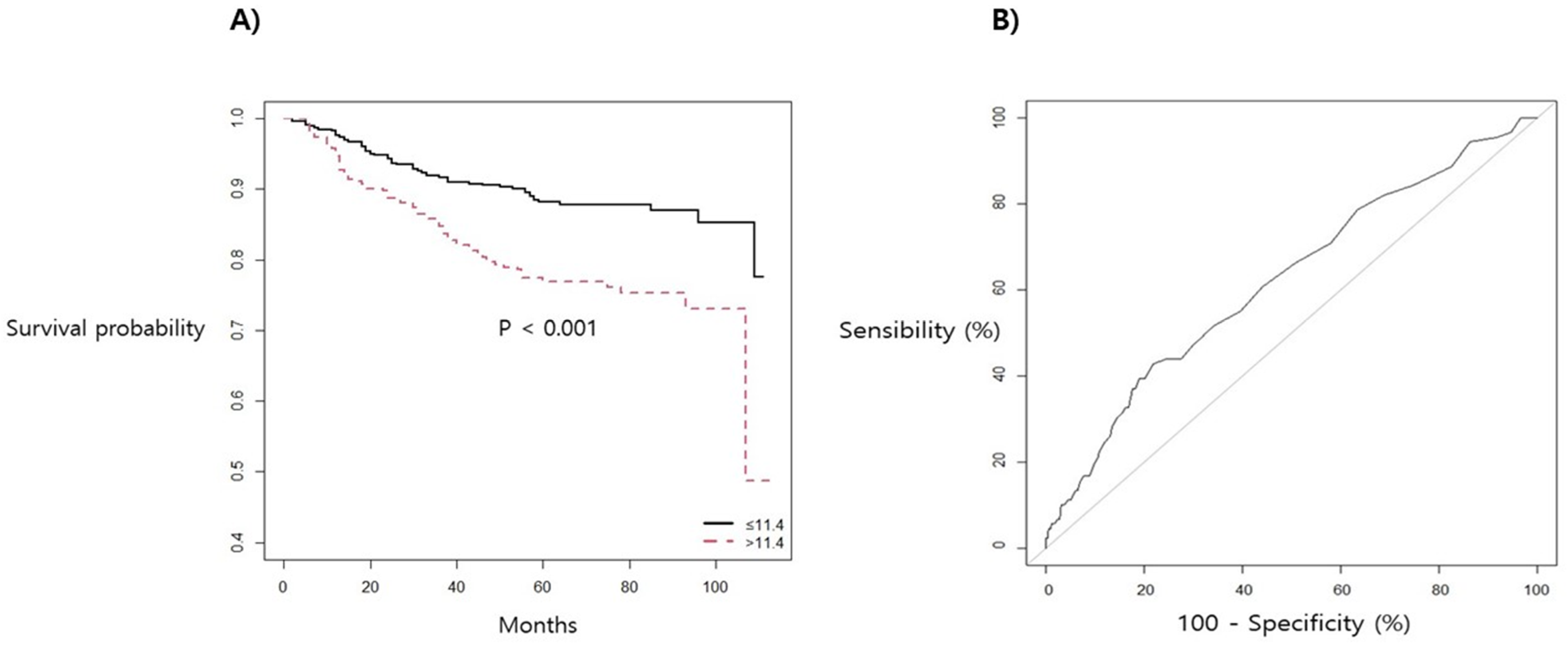
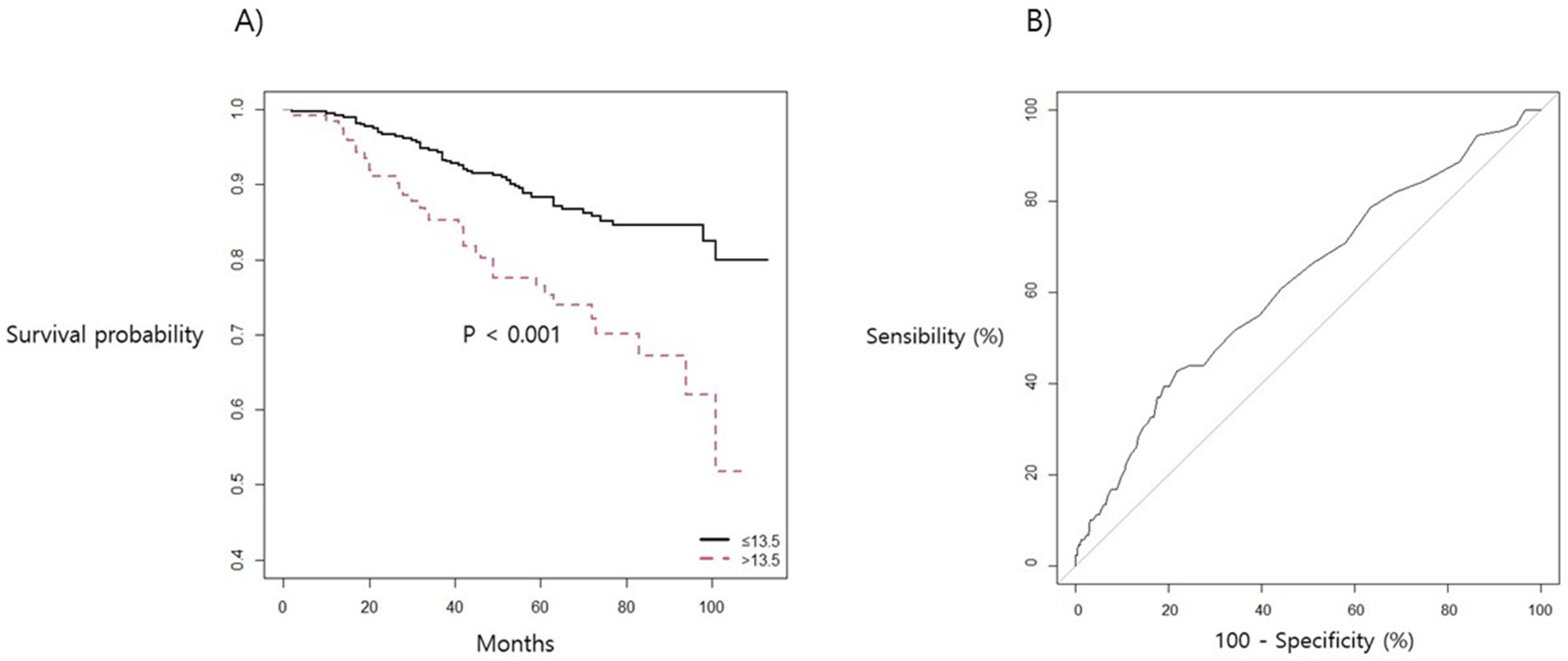
3.3. Predictors for Postoperative Recurrence and Mortality after Breast Cancer Surgery
3.4. Independent Risk Factors for Postoperative Recurrence and Mortality in Breast Cancer Surgery
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RBC | red blood cell |
| WBC | white blood cell |
| RDW | red blood cell distribution width |
| PDW | platelet distribution width |
| NLR | neutrophil-to-lymphocyte ratio |
| MPV | mean platelet volume |
| PT | prothrombin time |
| ALP | alkaline phosphatase |
| CEA | carcinoembryonic antigen |
| CA | cancer antigen |
| TIVA | total intravenous anesthesia |
| NSAIDs | non-steroidal anti-inflammatory drugs |
| BCS | breast-conserving surgery |
| TNM | tumor-node-metastasis |
| HER2 | human epidermal growth factor receptor 2 |
| CI | confidence interval |
| HR | hazard ratio |
| ROC | receiver operating characteristic |
References
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; Coggeshall, M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- DeSantis, C.; Ma, J.; Bryan, L.; Jemal, A. Breast cancer statistics, 2013. CA A Cancer J. Clin. 2013, 64, 52–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Satpathy, M. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar]
- Amoroso, V.; Generali, D.; Buchholz, T.; Cristofanilli, M.; Pedersini, R.; Curigliano, G.; Daidone, M.G.; Di Cosimo, S.; Dowsett, M.; Fox, S.; et al. International Expert Consensus on Primary Systemic Therapy in the Management of Early Breast Cancer: Highlights of the Fifth Symposium on Primary Systemic Therapy in the Management of Operable Breast Cancer, Cremona, Italy (2013). J. Natl. Cancer Inst. Monogr. 2015, 2015, 90–96. [Google Scholar] [CrossRef]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.-J.; Albain, K.S.; Andre, F.; Bergh, J.; et al. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef] [PubMed]
- Peto, R.; Davies, C.; Godwin, J.; Gray, R.; Pan, H.C.; Clarke, M.; Pritchard, K. Comparisons between different polychemotherapy regimens for early breast cancer: Meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet 2012, 379, 432–444. [Google Scholar]
- Wapnir, I.L.; Anderson, S.J.; Mamounas, E.P.; Jeong, J.; Tan-Chiu, E.; Fisher, B.; Wolmark, N. Prognosis After Ipsilateral Breast Tumor Recurrence and Locoregional Recurrences in Five National Surgical Adjuvant Breast and Bowel Project Node-Positive Adjuvant Breast Cancer Trials. J. Clin. Oncol. 2006, 24, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.; Anderson, S.; Bryant, J.; Margolese, R.G.; Deutsch, M.; Fisher, E.R.; Jeong, J.; Wolmark, N. Twenty-Year Follow-up of a Randomized Trial Comparing Total Mastectomy, Lumpectomy, and Lumpectomy plus Irradiation for the Treatment of Invasive Breast Cancer. N. Engl. J. Med. 2002, 347, 1233–1241. [Google Scholar] [CrossRef] [Green Version]
- Schnitt, S.J. Classification and prognosis of invasive breast cancer: From morphology to molecular taxonomy. Mod. Pathol. 2010, 23, S60–S64. [Google Scholar] [CrossRef] [Green Version]
- Ito, M.; Shien, T.; Omori, M.; Mizoo, T.; Iwamoto, T.; Nogami, T.; Motoki, T.; Taira, N.; Doihara, H.; Miyoshi, S. Evaluation of aldehyde dehydrogenase 1 and transcription factors in both primary breast cancer and axillary lymph node metastases as a prognostic factor. Breast Cancer 2015, 23, 437–444. [Google Scholar] [CrossRef]
- Watanabe, G.; Ishida, T.; Furuta, A.; Takahashi, S.; Watanabe, M.; Nakata, H.; Kato, S.; Ishioka, C.; Ohuchi, N. Combined Immunohistochemistry of PLK1, p21, and p53 for Predicting TP53 Status. Am. J. Surg. Pathol. 2015, 39, 1026–1034. [Google Scholar] [CrossRef]
- Chen, B.; Tang, H.; Liu, X.; Liu, P.; Yang, L.; Xie, X.; Ye, F.; Song, C.; Xie, X.; Wei, W. miR-22 as a prognostic factor targets glucose transporter protein type 1 in breast cancer. Cancer Lett. 2015, 356, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Wall, T.; Sherwin, A.; Ma, D.; Buggy, D. Influence of perioperative anaesthetic and analgesic interventions on oncological outcomes: A narrative review. Br. J. Anaesth. 2019, 123, 135–150. [Google Scholar] [CrossRef] [PubMed]
- Bajwa, S.J.S.; Anand, S.; Kaur, G. Anesthesia and cancer recurrences: The current knowledge and evidence. J. Cancer Res. Ther. 2015, 11, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Rivenbark, A.G.; O’Connor, S.M.; Coleman, W.B. Molecular and cellular heterogeneity in breast cancer: Challenges for personalized medicine. Am. J. Pathol. 2013, 183, 1113–1124. [Google Scholar] [CrossRef] [Green Version]
- Stegner, D.; Dütting, S.; Nieswandt, B. Mechanistic explanation for platelet contribution to cancer metastasis. Thromb. Res. 2014, 133, S149–S157. [Google Scholar] [CrossRef]
- Koh, C.-H.; Bhoopathy, N.; Ng, K.-L.; Jabir, R.S.; Tan, G.-H.; See, M.H.; Jamaris, S.; Taib, N. Utility of pre-treatment neutrophil–lymphocyte ratio and platelet–lymphocyte ratio as prognostic factors in breast cancer. Br. J. Cancer 2015, 113, 150–158. [Google Scholar] [CrossRef]
- Hammond, M.E.H.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Fitzgibbons, P.L.; Francis, G.; Goldstein, N.S.; Hayes, M.; et al. American Society of Clinical Oncology/College of American Pathologists Guideline Recommendations for Immunohistochemical Testing of Estrogen and Progesterone Receptors in Breast Cancer. J. Clin. Oncol. 2010, 28, 2784–2795. [Google Scholar] [CrossRef] [Green Version]
- Zwart, W.; Flach, K.D.; Rudraraju, B.; Abdel-Fatah, T.M.; Gojis, O.; Canisius, S.; Moore, D.; Nevedomskaya, E.; Opdam, M.; Droog, M.; et al. SRC3 Phosphorylation at Serine 543 Is a Positive Independent Prognostic Factor in ER-Positive Breast Cancer. Clin. Cancer Res. 2016, 22, 479–491. [Google Scholar] [CrossRef] [Green Version]
- Rui, X.; Li, Y.; Jin, F.; Li, F. TMPRSS3 is a novel poor prognostic factor for breast cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 5435–5442. [Google Scholar] [PubMed]
- Dong, L.-L.; Chen, L.-M.; Wang, W.-M.; Zhang, L.-M. Decreased expression of microRNA-124 is an independent unfavorable prognostic factor for patients with breast cancer. Diagn. Pathol. 2015, 10, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Seong, M.-K.; Lee, J.-Y.; Byeon, J.; Sohn, Y.-J.; Seol, H.; Lee, J.-K.; Kim, E.-K.; Kim, H.-A.; Noh, W.C. Bcl-2 is a highly significant prognostic marker of hormone-receptor-positive, human epidermal growth factor receptor-2-negative breast cancer. Breast Cancer Res. Treat. 2015, 150, 141–148. [Google Scholar] [CrossRef]
- Feely, M.; Collins, C.S.; Daniels, P.R.; Kebede, E.B.; Jatoi, A.; Mauck, K.F. Preoperative testing before noncardiac surgery: Guidelines and recommendations. Am. Fam. Physician 2013, 87, 414–418. [Google Scholar] [PubMed]
- Burns, C.D.; Brown, J.P.; Corwin, H.L.; Gross, I.; Ozawa, S.J.; Shander, A. Special Report From the Society for the Advancement of Blood Management: The Choosing Wisely Campaign. Anesth. Analg. 2019, 129, 1381–1386. [Google Scholar] [CrossRef]
- Lippi, G.; Targher, G.; Montagnana, M.; Salvagno, G.L.; Zoppini, G.; Guidi, G.C. Relation between red blood cell distribution width and inflammatory biomarkers in a large cohort of unselected outpatients. Arch. Pathol. Lab. Med. 2009, 133, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Maurya, P.K.; Kumar, P.; Chandra, P. Biomarkers of oxidative stress in erythrocytes as a function of human age. World J. Methodol. 2015, 5, 216–222. [Google Scholar] [CrossRef] [Green Version]
- Mohanty, J.G.; Nagababu, E.; Rifkind, J.M. Red blood cell oxidative stress impairs oxygen delivery and induces red blood cell aging. Front. Physiol. 2014, 5, 84. [Google Scholar] [CrossRef] [Green Version]
- Kordbacheh, F.; O’Meara, C.H.; Coupland, L.A.; Lelliott, P.M.; Parish, C. Extracellular histones induce erythrocyte fragility and anemia. Blood 2017, 130, 2884–2888. [Google Scholar] [CrossRef] [PubMed]
- Abrahan, I.L.L.; Ramos, J.D.A.; Cunanan, E.L.; Tiongson, M.D.A.; Punzalan, F.E.R. Red Cell Distribution Width and Mortality in Patients With Acute Coronary Syndrome: A Meta-Analysis on Prognosis. Cardiol. Res. 2018, 9, 144–152. [Google Scholar] [CrossRef]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F.R. Cancer-related inflammation. Nat. Cell Biol. 2008, 454, 436–444. [Google Scholar] [CrossRef]
- Balkwill, F.R.; Mantovani, A. Cancer-related inflammation: Common themes and therapeutic opportunities. Semin. Cancer Biol. 2012, 22, 33–40. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The Next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, M.D.; Jones, L.J. The role of inflammation in progression of breast cancer: Friend or foe? Int. J. Oncol. 2015, 47, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.-P.; Ma, R.-M.; Xiang, Y.-Q. Utility of Red Cell Distribution Width as a Prognostic Factor in Young Breast Cancer Patients. Medicine 2016, 95, e3430. [Google Scholar] [CrossRef] [PubMed]
- Yao, D.; Wang, Z.; Cai, H.; Li, Y.; Li, B. Relationship between red cell distribution width and prognosis in patients with breast cancer after operation: A retrospective cohort study. Biosci. Rep. 2019, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olafsson, H.B.; Sigurdarson, G.A.; Christopher, K.B.; Karason, S.; Sigurdsson, G.H.; Sigurdsson, M.I. A retrospective cohort study on the association between elevated preoperative red cell distribution width and all-cause mortality after noncardiac surgery. Br. J. Anaesth. 2020, 124, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Buamah, P.K.; Bent, D.J.; Bodger, W.A.H.; Skillen, A.W. A profile of serum CA 15-3, carcinoembryonic antigen, alkaline phosphatase, and γ-glutamyl transferase levels in patients with breast cancer. J. Surg. Oncol. 1993, 53, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Basuyau, J.P.; Brunelle, P.; Charrot, P.; Chevallier, B.; Delapierre, F.; Graic, Y.; Julien, J.P.; Veyret, C. CA 15.3 and early diagnosis of recurrence in breast cancer. Bull Cancer 1993, 80, 213–218. [Google Scholar] [PubMed]
- Lauro, S.; Trasatti, L.; Bordin, F.; Lanzetta, G.; Bria, E.; Gelibter, A.; Reale, M.G.; Vecchione, A. Comparison of CEA, MCA, CA 15-3 and CA 27-29 in follow-up and monitoring therapeutic response in breast cancer patients. Anticancer Res. 1999, 19, 3511–3515. [Google Scholar]
- NCCN Clinical Practice Guidelines in Oncology; Breast Cancer Version 5; NCCN Guidelines®: Plymouth Meeting, PA, USA, 2020.
- Hayes, D.F.; Zurawski, V.R.; Kufe, D.W. Comparison of circulating CA15-3 and carcinoembryonic antigen levels in patients with breast cancer. J. Clin. Oncol. 1986, 4, 1542–1550. [Google Scholar] [CrossRef]
- Molina, R.; Jo, J.; Filella, X.; Zanón, G.; Farrus, B.; Muñoz, M.; Latre, M.L.; Pahisa, J.; Velasco, M.; Fernandez, P.; et al. C-erbB-2, CEA and CA 15.3 serum levels in the early diagnosis of recurrence of breast cancer patients. Anticancer Res. 1999, 19, 2551–2555. [Google Scholar]
- Wu, S.-G.; He, Z.-Y.; Zhou, J.; Sun, J.-Y.; Li, F.-Y.; Lin, Q.; Guo, L.; Lin, H.-X. Serum levels of CEA and CA15-3 in different molecular subtypes and prognostic value in Chinese breast cancer. Breast 2014, 23, 88–93. [Google Scholar] [CrossRef]
- Uehara, M.; Kinoshita, T.; Hojo, T.; Akashi-Tanaka, S.; Iwamoto, E.; Fukutomi, T. Long-term prognostic study of carcinoembryonic antigen (CEA) and carbohydrate antigen 15-3 (CA 15-3) in breast cancer. Int. J. Clin. Oncol. 2008, 13, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Dai, D.; Chen, B.; Tang, H.; Xie, X.; Wei, W. Clinicopathological and Prognostic Significance of Cancer Antigen 15-3 and Carcinoembryonic Antigen in Breast Cancer: A Meta-Analysis including 12,993 Patients. Dis. Markers 2018, 2018, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina, R.; Barak, V.; Van Dalen, A.; Duffy, M.J.; Einarsson, R.; Gion, M.; Goike, H.; Lamerz, R.; Nap, M.; Sölétormos, G.; et al. Tumor Markers in Breast Cancer—European Group on Tumor Markers Recommendations. Tumor Biol. 2005, 26, 281–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, L.; Fritsche, H.; Mennel, R.; Norton, L.; Ravdin, P.; Taube, S.; Somerfield, M.R.; Hayes, D.F.; Bast, R.C., Jr. American society of clinical oncology 2007 update of recommendations for the use of tumor markers in breast cancer. J. Clin. Oncol. 2007, 25, 5287–5312. [Google Scholar] [CrossRef] [Green Version]
- Park, B.-W.; Oh, J.-W.; Kim, J.-H.; Park, S.H.; Kim, K.-S.; Lee, K.S. Preoperative CA 15-3 and CEA serum levels as predictor for breast cancer outcomes. Ann. Oncol. 2007, 19, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Park, S.; Park, J.M.; Cho, J.H.; Kim, S.I.; Park, B.-W. Elevated levels of preoperative CA 15-3 and CEA serum levels have independently poor prognostic significance in breast cancer. Ann. Oncol. 2012, 24, 1225–1231. [Google Scholar] [CrossRef]
- Nam, S.E.; Lim, W.; Jeong, J.; Lee, S.; Choi, J.; Park, H.; Jung, Y.; Jung, S.P.; Bae, S.Y. The prognostic significance of preoperative tumor marker (CEA, CA15-3) elevation in breast cancer patients: Data from the Korean Breast Cancer Society Registry. Breast Cancer Res. Treat. 2019, 177, 669–678. [Google Scholar] [CrossRef]
- Senkus, E.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rutgers, E.; Zackrisson, S.; Cardoso, F. Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26, v8–v30. [Google Scholar] [CrossRef]
- Malmström, P.; Bendahl, P.-O.; Boiesen, P.; Brünner, N.; Idvall, I.; Fernö, M. S-Phase Fraction and Urokinase Plasminogen Activator Are Better Markers for Distant Recurrences Than Nottingham Prognostic Index and Histologic Grade in a Prospective Study of Premenopausal Lymph Node–Negative Breast Cancer. J. Clin. Oncol. 2001, 19, 2010–2019. [Google Scholar] [CrossRef] [PubMed]
- Blamey, R.; Ellis, I.; Pinder, S.; Lee, A.; Macmillan, R.; Morgan, D.; Robertson, J.; Mitchell, M.; Ball, G.; Haybittle, J.; et al. Survival of invasive breast cancer according to the Nottingham Prognostic Index in cases diagnosed in 1990–1999. Eur. J. Cancer 2007, 43, 1548–1555. [Google Scholar] [CrossRef]
- Galea, M.H.; Blamey, R.W.; Elston, C.E.; Ellis, I.O. The Nottingham prognostic index in primary breast cancer. Breast Cancer Res. Treat. 1992, 22, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.; Luo, W.; Jia, W.; Liang, G.; Xie, X.; Zheng, W.; Song, E.; Su, F.; Gong, C. A combination of Nottingham prognostic index and IHC4 score predicts pathological complete response of neoadjuvant chemotherapy in estrogen receptor positive breast cancer. Oncotarget 2016, 7, 87312–87322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Ye, Y.; Barcenas, C.H.; Chow, W.-H.; Meng, Q.H.; Chavez-MacGregor, M.; Hildebrandt, M.A.T.; Zhao, H.; Gu, X.; Deng, Y.; et al. Personalized Prognostic Prediction Models for Breast Cancer Recurrence and Survival Incorporating Multidimensional Data. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drukker, C.A.; Nijenhuis, M.V.; Bueno-De-Mesquita, J.M.; Retèl, V.; Van Harten, W.H.; Van Tinteren, H.; Wesseling, J.; Schmidt, M.K.; Veer, L.J.V.; Sonke, G.S.; et al. Optimized outcome prediction in breast cancer by combining the 70-gene signature with clinical risk prediction algorithms. Breast Cancer Res. Treat. 2014, 145, 697–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, W.; Kim, K.S.; Lee, J.E.; Noh, D.-Y.; Kim, S.-W.; Jung, Y.S.; Park, M.Y.; Park, R.W. Development of Novel Breast Cancer Recurrence Prediction Model Using Support Vector Machine. J. Breast Cancer 2012, 15, 230–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Before 1 to 5 Propensity Score Matching | After 1 to 5 Propensity Score Matching | |||||
|---|---|---|---|---|---|---|
| Parameters | Non-Recurrence (n = 1649) | Recurrence (n = 134) | p-Value | Non-Recurrence (n = 645) | Recurrence (n = 129) | p-Value |
| Demographic data | ||||||
| Age (yr) | 50.1 ± 9.9 | 49.7 ± 11.2 | 0.683 | 48.7 ± 9.49 | 49.69 ± 10.88 | 0.333 |
| Body mass index (kg/m2) | 23.3 ± 3.2 | 23.0 ± 3.0 | 0.244 | 23.0 ± 3.1 | 23.1 ± 3.0 | 0.851 |
| Comorbidities | ||||||
| Hypertension | 321 (19.5) | 30 (22.4) | 0.413 | 114 (17.7) | 27 (20.9) | 0.382 |
| Diabetes mellitus | 110 (6.7) | 13 (9.7) | 0.183 | 37 (5.7) | 12 (9.3) | 0.129 |
| Cardiac | 43 (2.6) | 4 (3.0) | 0.777 | 18 (2.8) | 4 (3.1) | 0.775 |
| Pulmonary | 27 (1.6) | 4 (3.0) | 0.287 | 10 (1.5) | 0 (0.0) | 0.384 |
| Endocrine | 79 (4.8) | 7 (5.2) | 0.822 | 26 (4.0) | 7 (5.4) | 0.474 |
| Renal | 10 (0.6) | 0 (0.0) | >0.999 | 0 (0.0) | 0 (0.0) | >0.999 |
| Liver | 8 (0.5) | 1 (0.8) | 0.506 | 3 (0.5) | 1 (0.8) | 0.519 |
| Neurological | 24 (1.5) | 2 (1.5) | >0.999 | 9 (1.4) | 1 (0.8) | >0.999 |
| Others | 10 (0.6) | 1 (0.8) | 0.578 | 3 (0.5) | 1 (0.8) | 0.519 |
| Hematologic markers | ||||||
| Hemoglobin (g/dl) | 12.9 ± 1.2 | 12.6 ± 1.4 | 0.032 | 12.8 ± 1.2 | 12.6 ± 1.5 | 0.098 |
| Hematocrit (%) | 39.0 ± 3.3 | 38.2 ± 4.2 | 0.023 | 38.9 ± 3.2 | 38.1 ± 4.2 | 0.070 |
| RBC count (106/µL) | 4.33 ± 0.38 | 4.23 ± 0.49 | 0.018 | 4.33 ± 0.37 | 4.23 ± 0.50 | 0.027 |
| RDW (%) | 13.16 ± 1.35 | 13.55 ± 1.80 | 0.014 | 13.20 ± 1.37 | 13.53 ± 1.80 | 0.051 |
| PDW (fL) | 11.12 ± 1.45 | 10.97 ± 1.50 | 0.265 | 11.09 ± 1.44 | 10.97 ± 1.49 | 0.358 |
| WBC count (103/µL) | 6.01 ± 1.74 | 6.00 ± 1.83 | 0.983 | 6.12 ± 1.88 | 6.01 ± 1.85 | 0.563 |
| Neutrophil (%) | 3.67 ± 1.48 | 3.75 ± 1.50 | 0.550 | 3.75 ± 1.57 | 3.76 ± 1.52 | 0.982 |
| Lymphocyte (%) | 1.86 ± 0.60 | 1.76 ± 0.65 | 0.067 | 1.88 ± 0.61 | 1.78 ± 0.66 | 0.082 |
| NLR | 2.16 ± 1.20 | 2.41 ± 1.49 | 0.065 | 2.18 ± 1.17 | 2.40 ± 1.51 | 0.109 |
| Platelet (103/µL) | 258.17 ± 60.17 | 252.90 ± 72.14 | 0.413 | 262.55 ± 63.35 | 252.12 ± 72.70 | 0.131 |
| MPV (fL) | 9.77 ± 0.86 | 9.57 ± 1.06 | 0.039 | 9.75 ± 0.86 | 9.57 ± 1.06 | 0.079 |
| PT (sec) | 11.00 ± 0.76 | 11.05 ± 0.74 | 0.540 | 11.04 ± 0.83 | 11.05 ± 0.74 | 0.853 |
| ALP (IU/L) | 59.97 ± 20.02 | 63.52 ± 20.29 | 0.049 | 59.14 ± 19.26 | 63.22 ± 19.89 | 0.030 |
| CEA (ng/mL) | 1.74 ± 3.04 | 1.91 ± 2.88 | 0.539 | 1.62 ± 1.77 | 1.92 ± 2.93 | 0.253 |
| CA 15-3 (U/mL) | 11.97 ± 6.55 | 13.78 ± 7.66 | 0.009 | 11.95 ± 7.07 | 13.75 ± 7.68 | 0.010 |
| Anesthetic information | ||||||
| Anesthetic agent | 0.554 | 0.480 | ||||
| Sevoflurane | 1017 (61.7) | 76 (56.7) | 399 (61.9) | 75 (58.1) | ||
| TIVA | 20 (1.2) | 3 (2.2) | 7 (1.1) | 2 (1.6) | ||
| Desflurane | 442 (26.8) | 38 (28.4) | 190 (29.5) | 36 (27.9) | ||
| Isoflurane | 151 (9.2) | 14 (10.5) | 40 (6.20) | 13 (10.08) | ||
| Enflurane | 19 (1.2) | 3 (2.2) | 9 (1.40) | 3 (2.33) | ||
| Analgesic agents | ||||||
| NSAIDs | 1486 (90.1) | 125(93.3) | 0.230 | 581 (90.1) | 120 (93.0) | 0.296 |
| Opioids | 1023 (62.0) | 87(64.9) | 0.508 | 387 (60.0) | 86 (66.7) | 0.157 |
| Tramadol | 625 (37.9) | 43(32.1) | 0.182 | 255 (39.5) | 43 (33.3) | 0.187 |
| Dexamethasone | 138 (8.4) | 14(10.5) | 0.407 | 51 (7.9) | 13 (10.1) | 0.414 |
| Surgical information | ||||||
| Procedure | <0.001 | <0.001 | ||||
| BCS | 851 (51.6) | 33 (24.6) | 329 (51.0) | 32 (24.8) | ||
| Mastectomy | 798 (48.4) | 101 (75.4) | 316 (49.0) | 97 (75.2) | ||
| Surgical time | 207.8 ± 134.5 | 221.3 ± 121.9 | 0.263 | 204.6 ± 125.3 | 223.3 ± 123.4 | 0.120 |
| TNM stage | <0.001 | <0.001 | ||||
| 1 | 849 (51.5) | 31 (23.1) | 310 (48.1) | 29 (22.5) | ||
| 2 | 617 (37.4) | 49 (36.6) | 258 (40.0) | 47 (36.4) | ||
| 3 | 183 (11.1) | 54 (40.3) | 77 (11.9) | 53 (41.1) | ||
| Receptor status | ||||||
| Estrogen | 1185 (71.86) | 78 (58.2) | <0.001 | 469 (72.7) | 75 (58.1) | <0.001 |
| Progesterone | 1081 (65.55) | 72 (53.7) | 0.006 | 429 (66.5) | 71 (55.0) | 0.013 |
| HER2 | 455 (27.59) | 31 (23.1) | 0.265 | 156 (24.2) | 31 (24.0) | 0.970 |
| Histological grade | <0.001 | <0.001 | ||||
| Well | 369 (22.4) | 14 (10.5) | 152 (23.6) | 14 (10.9) | ||
| Moderate | 740 (44.9) | 59 (44.0) | 289 (44.8) | 55 (42.6) | ||
| Poorly | 369 (22.4) | 57 (42.5) | 142 (22.0) | 56 (43.4) | ||
| Other | 171 (10.4) | 4 (3.0) | 62 (9.6) | 4 (3.1) | ||
| Neoadjuvant chemotherapy | 64 (3.9) | 19 (14.2) | <0.001 | 25 (3.9) | 18 (14.0) | <0.001 |
| Adjuvant chemotherapy | 937 (56.8) | 98 (73.1) | <0.001 | 392 (60.8) | 96 (74.4) | 0.004 |
| Radiotherapy | 1062 (64.4) | 83 (61.9) | 0.568 | 429 (66.5) | 80 (62.0) | 0.326 |
| Before 1 to 5 Propensity Score Matching | After 1 to 5 Propensity Score Matching | |||||
|---|---|---|---|---|---|---|
| Parameters | Non-Death (n = 1682) | Death (n = 101) | p-Value | Non-Death (n = 445) | Death (n = 89) | p-Value |
| Demographic data | ||||||
| Age (yr) | 49.9 ± 9.8 | 52.4 ± 12.7 | 0.054 | 50.8 ± 9.8 | 50.9 ± 11.8 | 0.333 |
| Body mass index (kg/m2) | 23.3 ± 3.1 | 22.8 ± 3.1 | 0.102 | 22.9 ± 2.9 | 22.9 ± 3.1 | 0.851 |
| Comorbidities | ||||||
| Hypertension | 323 (19.2) | 28 (27.7) | 0.037 | 110 (24.7) | 21 (23.6) | 0.382 |
| Diabetes mellitus | 110 (6.5) | 13 (12.9) | 0.015 | 44 (9.9) | 8 (9.0) | 0.129 |
| Cardiac | 41 (2.4) | 6 (5.9) | 0.046 | 4 (0.9) | 3 (3.4) | 0.775 |
| Pulmonary | 25 (1.5) | 6 (5.9) | 0.007 | 1 (0.2) | 0 (0.0) | 0.384 |
| Endocrine | 81 (4.8) | 5 (5.0) | 0.814 | 17 (3.8) | 4 (4.5) | 0.765 |
| Renal | 9 (0.54) | 1 (1.0) | 0.443 | 3 (0.7) | 1 (1.1) | 0.519 |
| Liver | 7 (0.4) | 2 (2.0) | 0.088 | 0 (0.0) | 0 (0.0) | >0.999 |
| Neurological | 24 (1.4) | 2 (2.0) | 0.656 | 8 (1.8) | 2 (2.3) | 0.676 |
| Others | 11 (0.7) | 0 (0.0) | >0.999 | 0 (0.0) | 0 (0.0) | >0.999 |
| Hematologic markers | ||||||
| Hemoglobin (g/dl) | 12.9 ± 1.2 | 12.6 ± 1.5 | 0.069 | 12.9 ± 1.2 | 12.5 ± 1.6 | 0.033 |
| Hematocrit (%) | 39.0 ± 3.3 | 38.1 ± 4.5 | 0.043 | 39.0 ± 3.2 | 37.8 ± 4.6 | 0.018 |
| RBC count (106/µL) | 4.33 ± 0.38 | 4.19 ± 0.52 | 0.007 | 4.34 ± 0.36 | 4.16 ± 0.53 | 0.004 |
| RDW (%) | 13.15 ± 1.33 | 13.84 ± 2.05 | 0.002 | 13.11 ± 1.22 | 13.87 ± 2.17 | 0.002 |
| PDW (fL) | 11.12 ± 1.45 | 10.91 ± 1.53 | 0.161 | 11.04 ± 1.44 | 10.85 ± 1.48 | 0.283 |
| WBC count (103/µL) | 5.98 ± 1.73 | 6.38 ± 2.01 | 0.053 | 6.01 ± 1.57 | 6.38 ± 2.09 | 0.122 |
| Neutrophil (%) | 3.66 ± 1.47 | 3.95 ± 1.67 | 0.060 | 3.67 ± 1.35 | 3.98 ± 1.72 | 0.116 |
| Lymphocyte (%) | 1.85 ± 0.59 | 1.90 ± 0.75 | 0.559 | 1.88 ± 0.57 | 1.88 ± 0.77 | 0.916 |
| NLR | 2.17 ± 1.19 | 2.44 ± 1.66 | 0.104 | 2.14 ± 1.17 | 2.50 ± 1.73 | 0.057 |
| Platelet (103/µL) | 257.92 ± 59.95 | 255.32 ± 78.72 | 0.745 | 264.28 ± 59.61 | 257.71 ± 80.41 | 0.467 |
| MPV (fL) | 9.77 ± 0.87 | 9.42 ± 1.03 | 0.001 | 9.73 ± 0.89 | 9.41 ± 1.03 | 0.003 |
| PT (sec) | 11.01 ± 0.75 | 11.04 ± 0.78 | 0.627 | 10.94 ± 0.78 | 11.01 ± 0.74 | 0.407 |
| ALP (IU/L) | 59.80 ± 19.81 | 67.53 ± 22.74 | 0.002 | 60.48 ± 18.55 | 65.62 ± 21.67 | 0.039 |
| CEA (ng/mL) | 1.74 ± 3.09 | 1.93 ± 1.58 | 0.284 | 1.83 ± 4.09 | 1.78 ± 1.41 | 0.811 |
| CA 15-3 (U/mL) | 11.98 ± 6.53 | 14.25 ± 8.12 | 0.007 | 12.21 ± 6.10 | 13.98 ± 7.56 | 0.040 |
| Anesthetic information | ||||||
| Anesthetic agent | 0.107 | 0.174 | ||||
| Sevoflurane | 1037 (61.7) | 56 (55.5) | 268 (60.2) | 50 (56.2) | ||
| TIVA | 21 (1.3) | 2 (2.0) | 4 (0.9) | 1 (1.1) | ||
| Desflurane | 451 (26.8) | 29 (28.7) | 128 (28.8) | 26 (29.2) | ||
| Isoflurane | 155 (9.2) | 10 (9.9) | 41 (9.2) | 8 (9.0) | ||
| Enflurane | 18 (1.1) | 4 (4.0) | 4 (0.9) | 4 (4.5) | ||
| Analgesic agents | ||||||
| NSAIDs | 1520 (90.4) | 91 (90.1) | 0.929 | 404 (90.8) | 83 (93.3) | 0.453 |
| Opioids | 1044 (62.1) | 66 (65.4) | 0.510 | 265 (59.6) | 59 (66.3) | 0.235 |
| Tramadol | 643 (38.2) | 25 (24.8) | 0.007 | 179 (40.2) | 25 (28.1) | 0.032 |
| Dexamethasone | 144 (8.6) | 8 (7.9) | 0.823 | 34 (7.6) | 6 (6.7) | 0.769 |
| Surgical information | ||||||
| Procedure | <0.001 | <0.001 | ||||
| BCS | 865 (51.4) | 19 (18.8) | 218 (49.0) | 18 (20.2) | ||
| Mastectomy | 817 (48.6) | 82 (81.2) | 227 (51.0) | 71 (79.8) | ||
| Surgical time | 209.5 ± 135.7 | 197.7 ± 91.5 | 0.224 | 204.6 ± 125.3 | 223.3 ± 123.4 | 0.120 |
| TNM stage | <0.001 | <0.001 | ||||
| 1 | 862 (51.3) | 18 (17.8) | 226 (50.8) | 14 (15.7) | ||
| 2 | 625 (37.2) | 41 (40.6) | 166 (37.3) | 37 (41.6) | ||
| 3 | 195 (11.6) | 42 (41.6) | 53 (11.9) | 38 (42.7) | ||
| Receptor status | ||||||
| Estrogen | 1215 (72.2) | 48 (47.5) | <0.001 | 336 (75.5) | 40 (44.9) | <0.001 |
| Progesterone | 1110 (66.0) | 43 (42.6) | <0.001 | 292 (65.6) | 38 (42.7) | <0.001 |
| HER2 | 458 (27.2) | 28 (27.7) | 0.914 | 123 (27.6) | 25 (28.1) | 0.932 |
| Histological grade | <0.001 | <0.001 | ||||
| Well | 373 (22.2) | 10 (9.9) | 116 (26.1) | 7 (7.8) | ||
| Moderate | 760 (45.2) | 39 (38.6) | 190 (42.7) | 33 (37.1) | ||
| Poorly | 380 (22.6) | 46 (45.5) | 92 (20.7) | 43 (48.3) | ||
| Other | 169 (10.1) | 6 (5.9) | 47 (10.6) | 6 (6.7) | ||
| Neoadjuvantchemotherapy | 63 (3.8) | 20 (19.8) | <0.001 | 16 (3.6) | 19 (21.4) | <0.001 |
| Adjuvantchemotherapy | 965 (57.4) | 70 (69.3) | 0.019 | 268 (60.2) | 65 (73.0) | 0.023 |
| Radiotherapy | 1085 (64.5) | 60 (59.4) | 0.299 | 273 (61.4) | 55 (61.8) | 0.937 |
| Parameter | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Hematologic markers | |||||
| RDW (%) | >13.4 | 1.713 (1.196–2.453) | 0.004 | 1.238 (0.849–1.806) | 0.267 |
| ALP (IU/L) | >63 | 1.475 (1.040–2.093) | 0.030 | – | |
| CEA (ng/mL) | >2.73 | 1.653 (1.060–2.577) | 0.027 | 1.543 (0.988–2.411) | 0.056 |
| CA 15-3 (U/mL) | >11.4 | 2.145 (1.513–3.040) | <0.001 | 1.655 (1.154–2.374) | 0.007 |
| Surgical procedure | BCS | 1 (ref) | 1 (ref) | ||
| Mastectomy | 2.741 (1.837–4.088) | <0.001 | 2.169 (1.419–3.314) | <0.001 | |
| TNM stage | 1 | 1 (ref) | 1 (ref) | ||
| 2 | 1.781 (1.121–2.831) | 0.015 | 1.173 (0.728–1.891) | 0.512 | |
| 3 | 5.863 (3.725–9.226) | <0.001 | 3.481 (2.136–5.672) | <0.001 | |
| Estrogen receptor | Negative | 1 (ref) | 1 (ref) | ||
| Positive | 0.512 (0.360–0.727) | <0.001 | 0.671 (0.455–0.990) | 0.045 | |
| Progesterone receptor | Negative | 1 (ref) | 1 (ref) | ||
| Positive | 0.598 (0.422–0.846) | 0.004 | – | ||
| Neoadjuvant chemotherapy | 3.090 (1.876–5.089) | <0.001 | 1.957 (1.127–3.397) | 0.018 | |
| Adjuvant chemotherapy | 1.659 (1.116–2.465) | 0.013 | – | ||
| Histological grade | Good | 1 (ref) | 1 (ref) | ||
| Moderate | 2.152 (1.194–3.876) | 0.011 | 2.071 (1.139–3.766) | 0.017 | |
| Poor | 4.165 (2.312–7.503) | <0.001 | 3.878 (2.044–7.357) | <0.001 | |
| Other | 0.734 (0.242–2.231) | 0.586 | 0.598 (0.194–1.840) | 0.370 | |
| Parameter | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Age | <40 | 1 (ref) | 1 (ref) | ||
| 40–50 | 0.528 (0.284–0.980) | 0.043 | – | ||
| 50–60 | 0.622 (0.330–1.170) | 0.141 | – | ||
| 60–70 | 0.701 (0.354–1.389) | 0.309 | – | ||
| ≥70 | 1.343 (0.491–3.669) | 0.566 | – | ||
| Hematologic markers | |||||
| Hemoglobin (g/dl) | 0.809 (0.697–0.940) | 0.006 | – | ||
| RDW (%) | >13.5 | 2.368 (1.546–3.625) | <0.001 | 1.723 (1.098–2.704) | 0.019 |
| WBC count (103/µL) | 1.137 (1.009–1.281) | 0.035 | – | ||
| NLR | >2.82 | 1.936 (1.238–3.029) | 0.004 | 1.771 (1.108–2.832) | 0.017 |
| MPV (fL) | >8.6 | 0.358 (0.213–0.601) | <0.001 | 0.469 (0.271–0.811) | 0.007 |
| ALP (IU/L) | >76 | 1.729 (1.104–2.708) | 0.017 | 2.257 (1.412–3.607) | <0.001 |
| CEA (ng/mL) | >1.57 | 1.590 (1.046–2.417) | 0.031 | 1.553 (1.007–2.395) | 0.047 |
| CA 15-3 (U/mL) | >11.5 | 2.126 (1.396–3.236) | <0.001 | 1.423 (0.919–2.206) | 0.115 |
| Surgical procedure | BCS | 1 (ref) | 1 (ref) | ||
| Mastectomy | 3.287 (1.959–5.516) | <0.001 | 2.993 (1.750–5.118) | <0.001 | |
| TNM stage | 1 | 1 (ref) | 1 (ref) | ||
| 2 | 3.172 (1.714–5.869) | <0.001 | 2.310 (1.239–4.306) | 0.009 | |
| 3 | 8.676 (4.699–16.019) | <0.001 | 6.563 (3.482–12.370) | <0.001 | |
| Estrogen receptor | Negative | 1 (ref) | 1 (ref) | ||
| Positive | 0.279 (0.184–0.425) | <0.001 | 0.350 (0.219–0.561) | <0.001 | |
| Progesterone receptor | Negative | 1 (ref) | 1 (ref) | ||
| Positive | 0.387 (0.254–0.589) | <0.001 | – | ||
| Radiotherapy | 1.027 (0.669–1.576) | 0.904 | – | ||
| Neoadjuvant chemotherapy | 4.403 (2.649–7.319) | <0.001 | 1.890 (1.048–3.409) | 0.035 | |
| Adjuvant chemotherapy | 1.533(0.959–2.450) | 0.074 | – | ||
| Histological grade | Good | 1 (ref) | 1 (ref) | ||
| Moderate | 2.991 (1.320–6.776) | 0.009 | 3.253 (1.412–7.491) | 0.006 | |
| Poor | 7.661 (3.430–17.111) | <0.001 | 6.455 (2.757–15.113) | <0.001 | |
| Other | 2.012 (0.676–5.991) | 0.209 | 1.452 (0.480–4.393) | 0.509 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, Y.-C.; Park, S.; Kim, H.-J.; Jung, H.-E.; Kim, J.-Y.; Kim, M.-H. Preoperative Routine Laboratory Markers for Predicting Postoperative Recurrence and Death in Patients with Breast Cancer. J. Clin. Med. 2021, 10, 2610. https://doi.org/10.3390/jcm10122610
Yoo Y-C, Park S, Kim H-J, Jung H-E, Kim J-Y, Kim M-H. Preoperative Routine Laboratory Markers for Predicting Postoperative Recurrence and Death in Patients with Breast Cancer. Journal of Clinical Medicine. 2021; 10(12):2610. https://doi.org/10.3390/jcm10122610
Chicago/Turabian StyleYoo, Young-Chul, Seho Park, Hyun-Joo Kim, Hyun-Eom Jung, Ji-Young Kim, and Myoung-Hwa Kim. 2021. "Preoperative Routine Laboratory Markers for Predicting Postoperative Recurrence and Death in Patients with Breast Cancer" Journal of Clinical Medicine 10, no. 12: 2610. https://doi.org/10.3390/jcm10122610