
A Meta-Analysis of the Influence of Antipsychotics on Cytokines Levels in First Episode Psychosis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
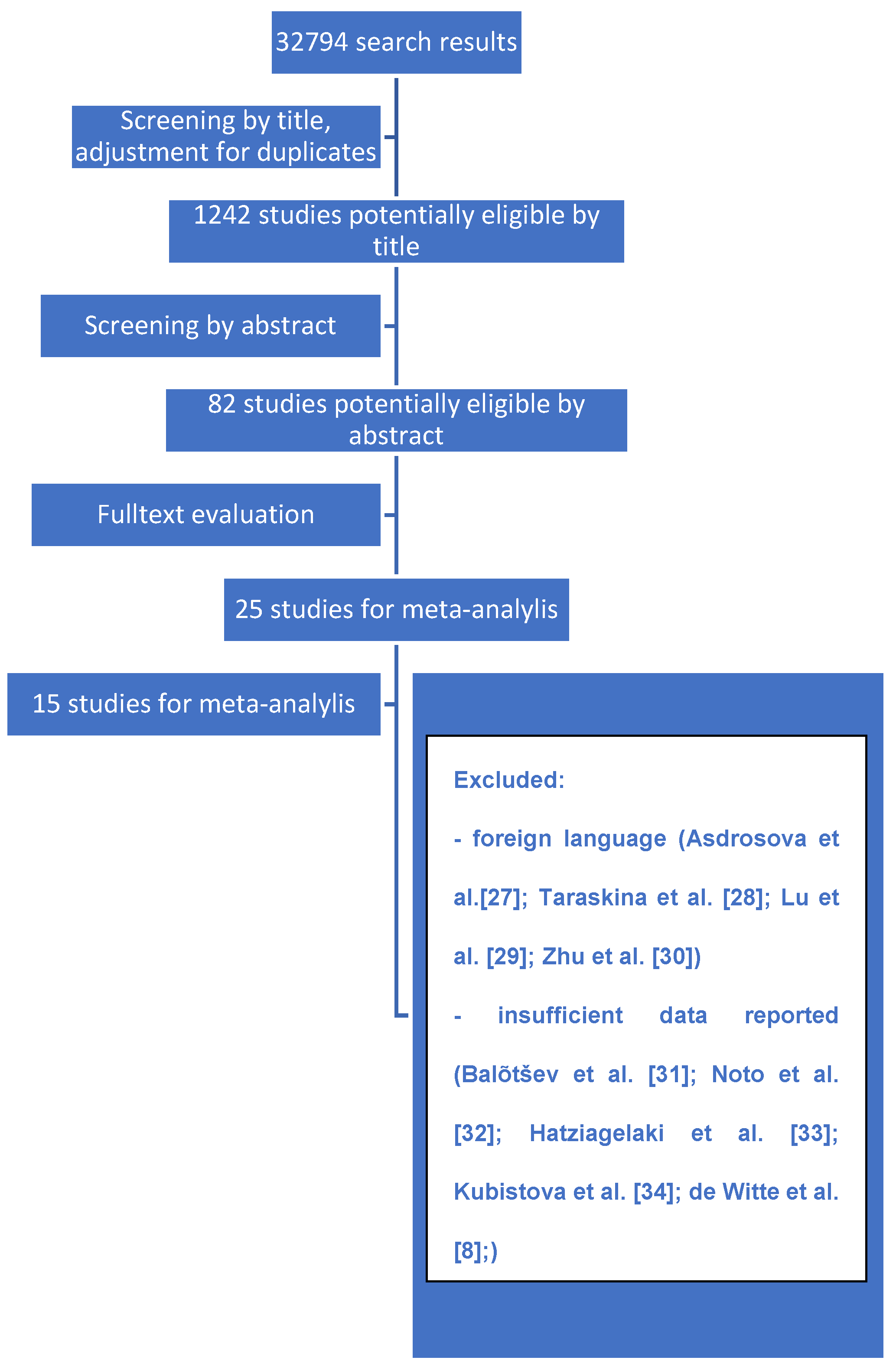
2.1. Systematic Search and Criteria
2.2. Statistical Methods
- Low data quality. This criterion mainly includes missing data and results not published in English. It was assumed that they would not be considered or substituted by statistically computed values on the basis of other studies.
- Several sensitivity analyses were performed after excluding each individual study (only one study each time). Studies shown to influence the overall result were excluded. This method was applied in the case of 3 or more analyzed studies.
- The study was excluded if its rejection abolished the publication bias. We created funnel plots to check for the existence of publication bias. This method was applied in case of 5 or more analyzed studies.
3. Results
3.1. Characteristics of Included Studies
3.1.1. IL-10
3.1.2. IL-17
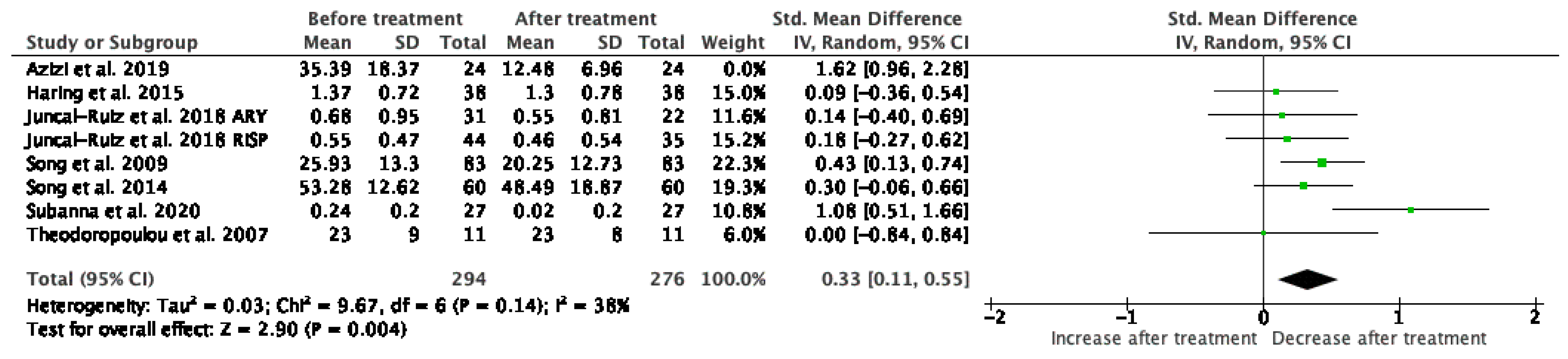
3.1.3. IL-1β
3.1.4. IL-2
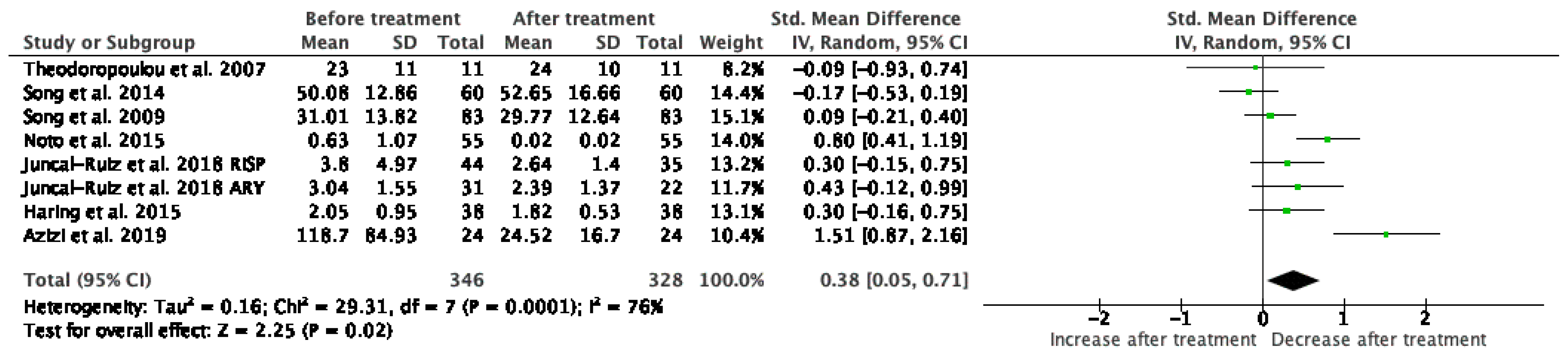
3.1.5. TNF-α
3.1.6. IFN-γ
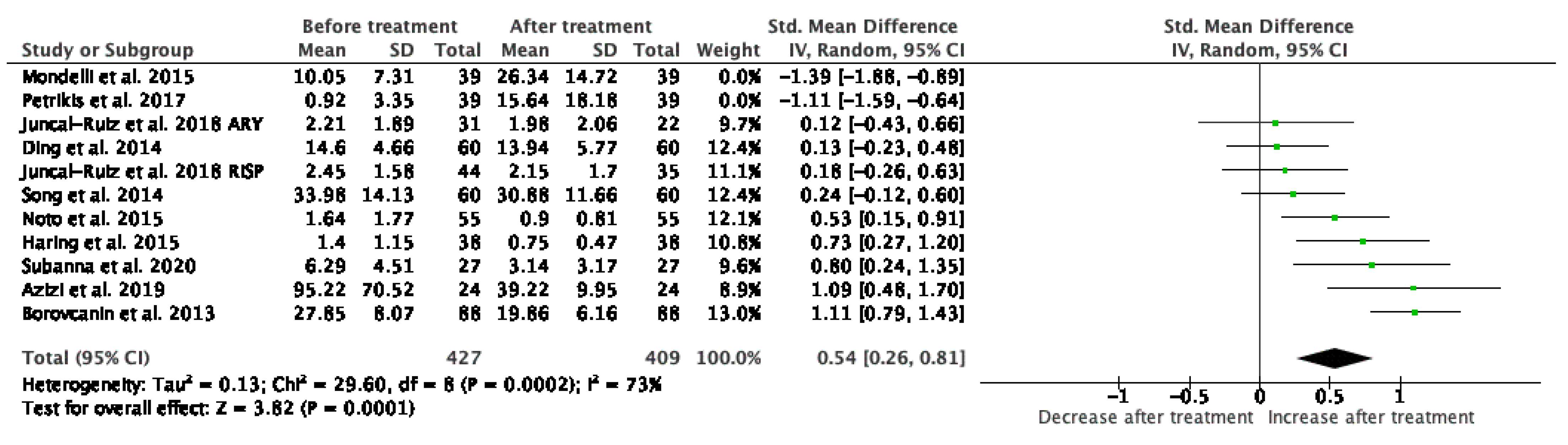
3.1.7. IL-6
3.1.8. IL-4
3.2. Risk of Bias
4. Discussion
5. Limitations
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brown, A.S.; Begg, M.D.; Gravenstein, S.; Schaefer, C.A.; Wyatt, R.J.; Bresnahan, M.; Babulas, V.P.; Susser, E.S. Serologic Evidence of Prenatal Influenza in the Etiology of Schizophrenia. Arch. Gen. Psychiatry 2004, 61, 774–780. [Google Scholar] [CrossRef] [Green Version]
- Buka, S.L. Maternal Infections and Subsequent Psychosis Among Offspring. Arch. Gen. Psychiatry 2001, 58, 1032–1037. [Google Scholar] [CrossRef] [Green Version]
- Buka, S.L.; Cannon, T.D.; Torrey, E.F.; Yolken, R.H. Maternal Exposure to Herpes Simplex Virus and Risk of Psychosis Among Adult Offspring. Biol. Psychiatry 2008, 63, 809–815. [Google Scholar] [CrossRef]
- De Miranda, A.S.; Zhang, C.-J.; Katsumoto, A.; Teixeira, A.L. Hippocampal adult neurogenesis: Does the immune system matter? J. Neurol. Sci. 2017, 372, 482–495. [Google Scholar] [CrossRef]
- Kipnis, J.; Cohen, H.; Cardon, M.; Ziv, Y.; Schwartz, M. T cell deficiency leads to cognitive dysfunction: Implications for therapeutic vaccination for schizophrenia and other psychiatric conditions. Proc. Natl. Acad. Sci. USA 2004, 101, 8180–8185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, Y.Y. Multi-tasking of helper T cells. Immunology 2010, 130, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Noto, M.N.; Maes, M.; Nunes, S.O.V.; Ota, V.K.; Rossaneis, A.C.; Verri, W.A.; Cordeiro, Q.; Belangero, S.I.; Gadelha, A.; Bressan, R.A.; et al. Activation of the immune-inflammatory response system and the compensatory immune-regulatory system in antipsychotic naive first episode psychosis. Eur. Neuropsychopharmacol. 2019, 29, 416–431. [Google Scholar] [CrossRef] [PubMed]
- De Witte, L.; Tomasik, J.; Schwarz, E.; Guest, P.; Rahmoune, H.; Kahn, R.S.; Bahn, S. Cytokine alterations in first-episode schizophrenia patients before and after antipsychotic treatment. Schizophr. Res. 2014, 154, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Bueno, B.; Bioque, M.; Mac-Dowell, K.S.; Barcones, M.F.; Martinez-Cengotitabengoa, M.; Pina-Camacho, L.; Rodríguez-Jiménez, R.; Sáiz, P.A.; Castro, C.; Lafuente, A.; et al. Pro-/anti-inflammatory dysregulation in patients with first episode of psychosis: Toward an integrative inflammatory hypothesis of schizophrenia. Schizophr. Bull. 2013, 40, 376–387. [Google Scholar] [CrossRef] [Green Version]
- Kato, T.; Mizoguchi, Y.; Monji, A.; Horikawa, H.; Suzuki, S.O.; Seki, Y.; Iwaki, T.; Hashioka, S.; Kanba, S. Inhibitory effects of aripiprazole on interferon--induced microglial activation via intracellular Ca2+regulationin vitro. J. Neurochem. 2008, 106, 815–825. [Google Scholar] [CrossRef]
- Jarskog, L.; Xiao, H.; Wilkie, M.B.; Lauder, J.M.; Gilmore, J.H. Cytokine regulation of embryonic rat dopamine and serotonin neuronal survival in vitro. Int. J. Dev. Neurosci. 1997, 15, 711–716. [Google Scholar] [CrossRef]
- Potter, E.D.; Ling, Z.D.; Carvey, P.M. Cytokine-induced conversion of mesencephalic-derived progenitor cells into dopamine neurons. Cell Tissue Res. 1999, 296, 235–246. [Google Scholar] [CrossRef] [PubMed]
- Felger, J.C.; Mun, J.; Kimmel, H.L.; Nye, J.A.; Drake, D.F.; Hernandez, C.R.; Freeman, A.A.; Rye, D.B.; Goodman, M.M.; Howell, L.L.; et al. Chronic Interferon-α Decreases Dopamine 2 Receptor Binding and Striatal Dopamine Release in Association with Anhedonia-Like Behavior in Nonhuman Primates. Neuropsychopharmacology 2013, 38, 2179–2187. [Google Scholar] [CrossRef]
- Schwarcz, R.; Stone, T. The kynurenine pathway and the brain: Challenges, controversies and promises. Neuropharmacology 2017, 112, 237–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Gras, I.; García-Sánchez, F.; Guaza, C.; Rodríguez-Jiménez, R.; Andrés-Esteban, E.; Palomo, T.; Rubio, G.; Borrell, J. Altered immune function in unaffected first-degree biological relatives of schizophrenia patients. Psychiatry Res. 2012, 200, 1022–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, B.J.; Buckley, P.; Seabolt, W.; Mellor, A.; Kirkpatrick, B. Meta-Analysis of Cytokine Alterations in Schizophrenia: Clinical Status and Antipsychotic Effects. Biol. Psychiatry 2011, 70, 663–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breitborde, N.J.K.; Srihari, V.H.; Woods, S.W. Review of the operational definition for first-episode psychosis. Early Interv. Psychiatry 2009, 3, 259–265. [Google Scholar] [CrossRef]
- Goldsmith, D.R.; Rapaport, M.H.; Miller, B.J. A meta-analysis of blood cytokine network alterations in psychiatric patients: Comparisons between schizophrenia, bipolar disorder and depression. Mol. Psychiatry 2016, 21, 1696–1709. [Google Scholar] [CrossRef]
- Fraguas, D.; Díaz-Caneja, C.M.; Rodríguez-Quiroga, A.; Arango, C. Oxidative Stress and Inflammation in Early Onset First Episode Psychosis: A Systematic Review and Meta-Analysis. Int. J. Neuropsychopharmacol. 2017, 20, 435–444. [Google Scholar] [CrossRef]
- Feigenson, K.A.; Kusnecov, A.W.; Silverstein, S.M. Inflammation and the two-hit hypothesis of schizophrenia. Neurosci. Biobehav. Rev. 2014, 38, 72–93. [Google Scholar] [CrossRef] [Green Version]
- Martinuzzi, E.; Barbosa, S.; Daoudlarian, D.; Ali, W.B.H.; Gilet, C.; Fillatre, L.; Khalfallah, O.; Troudet, R.; Jamain, S.; the OPTiMiSE Study Group; et al. Stratification and prediction of remission in first-episode psychosis patients: The OPTiMiSE cohort study. Transl. Psychiatry 2019, 9, 1–13. [Google Scholar] [CrossRef]
- Romeo, B.; Brunet-Lecomte, M.; Martelli, C.; Benyamina, A. Kinetics of Cytokine Levels during Antipsychotic Treatment in Schizophrenia: A Meta-Analysis. Int. J. Neuropsychopharmacol. 2018, 21, 828–836. [Google Scholar] [CrossRef]
- Tourjman, V.; Kouassi, É.; Koué, M.-È.; Rocchetti, M.; Fortin-Fournier, S.; Fusar-Poli, P.; Potvin, S. Antipsychotics’ effects on blood levels of cytokines in schizophrenia: A meta-analysis. Schizophr. Res. 2013, 151, 43–47. [Google Scholar] [CrossRef]
- Capuzzi, E.; Bartoli, F.; Crocamo, C.; Clerici, M.; Carrà, G. Acute variations of cytokine levels after antipsychotic treatment in drug-naïve subjects with a first-episode psychosis: A meta-analysis. Neurosci. Biobehav. Rev. 2017, 77, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Cochrane Collaboration. Review Manager (RevMan), version 5.3; The Nordic Cochrane Centre: Copenhagen, Denmark, 2014. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Borovcanin, M.; Jovanovic, I.; Radosavljevic, G.; Dejanovic, S.D.; Stefanovic, V.; Arsenijevic, N.; Lukic, M.L. Antipsychotics can modulate the cytokine profile in schizophrenia: Attenuation of the type-2 inflammatory response. Schizophr. Res. 2013, 147, 103–109. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021). Cochrane. 2021. Available online: www.training.cochrane.org/handbook (accessed on 3 March 2021).
- Juncal-Ruiz, M.; Riesco-Dávila, L.; de la Foz, V.O.-G.; Martínez-Garcia, O.; Ramírez-Bonilla, M.; Ocejo-Viñals, J.G.; Leza, J.C.; López-Hoyos, M.; Crespo-Facorro, B. Comparison of the anti-inflammatory effect of aripiprazole and risperidone in 75 drug-naïve first episode psychosis individuals: A 3 months randomized study. Schizophr. Res. 2018, 202, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Haring, L.; Koido, K.; Vasar, V.; Leping, V.; Zilmer, K.; Zilmer, M.; Vasar, E. Antipsychotic treatment reduces psychotic symptoms and markers of low-grade inflammation in first episode psychosis patients, but increases their body mass index. Schizophr. Res. 2015, 169, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Fan, X.; Li, X.; Zhang, W.; Gao, J.; Zhao, J.; Harrington, A.; Ziedonis, D.M.; Lv, L. Changes in pro-inflammatory cytokines and body weight during 6-month risperidone treatment in drug naïve, first-episode schizophrenia. Psychopharmacology 2014, 231, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Subbanna, M.; Shivakumar, V.; Venugopal, D.; Narayanaswamy, J.C.; Berk, M.; Varambally, S.; Venkatasubramanian, G.; Debnath, M. Impact of antipsychotic medication on IL-6/ STAT3 signaling axis in peripheral blood mononuclear cells of drug-naive schizophrenia patients. Psychiatry Clin. Neurosci. 2019, 74, 64–69. [Google Scholar] [CrossRef]
- Theodoropoulou, S.; Spanakos, G.; Baxevanis, C.; Economou, M.; Gritzapis, A.; Papamichail, M.; Stefanis, C. Cytokine serum levels, autologous mixed lymphocyte reaction and surface marker analysis in never medicated and chronically medicated schizophrenic patients. Schizophr. Res. 2001, 47, 13–25. [Google Scholar] [CrossRef]
- Song, X.; Lv, L.-X.; Li, W.-Q.; Hao, Y.-H.; Zhao, J.-P. The Interaction of Nuclear Factor-Kappa B and Cytokines Is Associated with Schizophrenia. Biol. Psychiatry 2009, 65, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Azizi, E.; Hosseini, A.Z.; Soudi, S.; Noorbala, A.A. Alteration of Serum Levels of Cytokines in Schizophrenic Patients before and after Treatment with Risperidone. Iran. J. Allergy Asthma Immunol. 2019, 18, 262–268. [Google Scholar] [CrossRef]
- Petrikis, P.; Voulgari, P.V.; Tzallas, A.T.; Boumba, V.A.; Archimandriti, D.T.; Zambetas, D.; Papadopoulos, I.; Tsoulos, I.; Skapinakis, P.; Mavreas, V. Changes in the cytokine profile in first-episode, drug-naïve patients with psychosis after short-term antipsychotic treatment. Psychiatry Res. 2017, 256, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Noto, C.; Ota, V.K.; Gouvea, E.S.; Rizzo, L.B.; Spindola, L.M.N.; Honda, P.H.S.; Cordeiro, Q.; Belangero, S.I.; Bressan, R.A.; Gadelha, A.; et al. Effects of Risperidone on Cytokine Profile in Drug-Naive First-Episode Psychosis. Int. J. Neuropsychopharmacol. 2014, 18, pyu042. [Google Scholar] [CrossRef]
- Ding, M.; Song, X.; Zhao, J.; Gao, J.; Li, X.; Yang, G.; Wang, X.; Harrington, A.; Fan, X.; Lv, L. Activation of Th17 cells in drug naïve, first episode schizophrenia. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2014, 51, 78–82. [Google Scholar] [CrossRef]
- Mondelli, V.; Ciufolini, S.; Murri, M.B.; Bonaccorso, S.; Di Forti, M.; Giordano, A.; Marques, T.R.; Zunszain, P.A.; Morgan, C.; Murray, R.M.; et al. Cortisol and Inflammatory Biomarkers Predict Poor Treatment Response in First Episode Psychosis. Schizophr. Bull. 2015, 41, 1162–1170. [Google Scholar] [CrossRef] [Green Version]
- Van Os, J.; Kapur, S. Schizophrenia. Lancet 2009, 374, 635–645. [Google Scholar] [CrossRef]
- Tek, C.; Kucukgoncu, S.; Guloksuz, S.; Woods, S.W.; Srihari, V.H.; Annamalai, A. Antipsychotic-induced weight gain in first-episode psychosis patients: A meta-analysis of differential effects of antipsychotic medications. Early Interv. Psychiatry 2016, 10, 193–202. [Google Scholar] [CrossRef] [Green Version]
- Srikanthan, K.; Feyh, A.; Visweshwar, H.; Shapiro, J.I.; Sodhi, K. Systematic Review of Metabolic Syndrome Biomarkers: A Panel for Early Detection, Management, and Risk Stratification in the West Virginian Population. Int. J. Med. Sci. 2016, 13, 25–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques, P.; Collado, A.; Martinez-Hervás, S.; Domingo, E.; Benito, E.; Piqueras, L.; Real, J.T.; Ascaso, J.F.; Sanz, M.-J. Systemic Inflammation in Metabolic Syndrome: Increased Platelet and Leukocyte Activation, and Key Role of CX3CL1/CX3CR1 and CCL2/CCR2 Axes in Arterial Platelet-Proinflammatory Monocyte Adhesion. J. Clin. Med. 2019, 8, 708. [Google Scholar] [CrossRef] [Green Version]
- Russell, A.; Ciufolini, S.; Gardner-Sood, P.; Bonaccorso, S.; Gaughran, F.; Dazzan, P.; Pariante, C.M.; Mondelli, V. Inflammation and metabolic changes in first episode psychosis: Preliminary results from a longitudinal study. Brain Behav. Immun. 2015, 49, 25–29. [Google Scholar] [CrossRef]
- Dinesh, A.A.; Islam, J.; Khan, J.; Turkheimer, F.; Vernon, A.C. Effects of Antipsychotic Drugs: Cross Talk Between the Nervous and Innate Immune System. CNS Drugs 2020, 34, 1229–1251. [Google Scholar] [CrossRef]
- Kato, T.A.; Monji, A.; Mizoguchi, Y.; Hashioka, S.; Horikawa, H.; Seki, Y.; Kasai, M.; Utsumi, H.; Kanba, S. Anti-Inflammatory Properties of Antipsychotics Via Microglia Modulations: Are Antipsychotics a Fire Extinguisher in the Brain of Schizophrenia? Mini Rev. Med. Chem. 2011, 11, 565–574. [Google Scholar] [CrossRef]
- Karanikas, E.; Griveas, I.; Ntouros, E.; Floros, G.; Garyfallos, G. Evidence for increased immune mobilization in First Episode Psychosis compared with the prodromal stage in males. Psychiatry Res. 2016, 244, 333–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Şimşek, Ş.; Yıldırım, V.; Çim, A.; Kaya, S. Serum IL-4 and IL-10 Levels Correlate with the Symptoms of the Drug-Naive Adolescents with First Episode, Early Onset Schizophrenia. J. Child. Adolesc. Psychopharmacol. 2016, 26, 721–726. [Google Scholar] [CrossRef]
- Färber, K.; Pannasch, U.; Kettenmann, H. Dopamine and noradrenaline control distinct functions in rodent microglial cells. Mol. Cell. Neurosci. 2005, 29, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Monji, A.; Hashioka, S.; Kanba, S. Risperidone significantly inhibits interferon-γ-induced microglial activation in vitro. Schizophr. Res. 2007, 92, 108–115. [Google Scholar] [CrossRef]
- MacDowell, K.S.; García-Bueno, B.; Madrigal, J.L.M.; Parellada, M.; Arango, C.; Micó, J.A.; Leza, J.C. Risperidone normalizes increased inflammatory parameters and restores anti-inflammatory pathways in a model of neuroinflammation. Int. J. Neuropsychopharmacol. 2013, 16, 121–135. [Google Scholar] [CrossRef] [Green Version]
- Arimoto, T.; Choi, D.-Y.; Lu, X.; Liu, M.; Nguyen, X.V.; Zheng, N.; Stewart, C.A.; Kim, H.-C.; Bing, G. Interleukin-10 protects against inflammation-mediated degeneration of dopaminergic neurons in substantia nigra. Neurobiol. Aging 2007, 28, 894–906. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, J.M.; Wang, Y.; Ambinder, E.B.; Ward, R.E.; Minn, I.; Vranesic, M.; Kim, P.K.; Ford, C.N.; Higgs, C.; Hayes, L.N.; et al. In vivo markers of inflammatory response in recent-onset schizophrenia: A combined study using [11C]DPA-713 PET and analysis of CSF and plasma. Transl. Psychiatry 2016, 6, e777. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, D.R.; Haroon, E.; Miller, A.H.; Addington, J.; Bearden, C.; Cadenhead, K.; Cannon, T.; Cornblatt, B.; Mathalon, D.; McGlashan, T.; et al. Association of baseline inflammatory markers and the development of negative symptoms in individuals at clinical high risk for psychosis. Brain Behav. Immun. 2019, 76, 268–274. [Google Scholar] [CrossRef]
- Bulzacka, E.; Boyer, L.; Schürhoff, F.; Godin, O.; Berna, F.; Brunel, L.; Andrianarisoa, M.; Aouizerate, B.; Capdevielle, D.; Chéreau-Boudet, I.; et al. Chronic Peripheral Inflammation is Associated With Cognitive Impairment in Schizophrenia: Results From the Multicentric FACE-SZ Dataset. Schizophr. Bull. 2016, 42, 1290–1302. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.Y.; Cao, L.Y.; Song, C.; Wu, G.Y.; Chen, D.C.; Qi, L.Y.; Wang, F.; Xiu, M.H.; Chen, S.; Zhang, Y.; et al. Lower serum cytokine levels in smokers than nonsmokers with chronic schizophrenia on long-term treatment with antipsychotics. Psychopharmacology 2008, 201, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.J.; Goldsmith, D.R. Towards an Immunophenotype of Schizophrenia: Progress, Potential Mechanisms, and Future Directions. Neuropsychopharmacology 2017, 42, 299–317. [Google Scholar] [CrossRef] [Green Version]
- Nitta, M.; Kishimoto, T.; Müller, N.; Weiser, M.; Davidson, M.; Kane, J.M.; Correll, C.U. Adjunctive Use of Nonsteroidal Anti-inflammatory Drugs for Schizophrenia: A Meta-analytic Investigation of Randomized Controlled Trials. Schizophr. Bull. 2013, 39, 1230–1241. [Google Scholar] [CrossRef] [Green Version]
- Grüber, L.; Bunse, T.; Weidinger, E.; Reichard, H.; Müller, N. Adjunctive Recombinant Human Interferon Gamma-1b for Treatment-Resistant Schizophrenia in 2 Patients. J. Clin. Psychiatry 2014, 75, 1266–1267. [Google Scholar] [CrossRef] [Green Version]
- Miller, B.J.; Dias, J.K.; Lemos, H.P.; Buckley, P.F. An Open-Label, Pilot Trial of Adjunctive Tocilizumab in Schizophrenia. J. Clin. Psychiatry 2016, 77, 275–276. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cytokine | Number of Studies | N before/after Treatment | SMD | 95% CI | p | I2 | Studies |
|---|---|---|---|---|---|---|---|
| IL-1β | 7 | 294/276 | 0.43 | 0.13, 0.74 | 0.006 | 74% | Juncal-Ruiz 2018 [32], Haring 2015 [33], Song 2014 [34] Subanna 2020 [35], Theodoropoulou 2007 [36], Song 2009 [37], Azizi 2019 [38] |
| IL-2 | 4 | 163/145 | −0.1 | −1.12, 0.93 | 0.85 | 96% | Petrikis 2017 [39], Juncal-Ruiz 2018 [32], Haring 2015 [33], Theodoropoulou 2001 [36] |
| IL-4 | 4 | 168/150 | 0.38 | 0.09, 0.68 | 0.01 | 42% | Noto 2015 [40], Juncal-Ruiz 2018 [32], Haring 2015 [33], Borovcanin 2013 [30] |
| IL-6 | 10 | 427/409 | 0.54 | 0.26, 0.81 | 0.0001 | 73% | Noto 2015 [40], Petrikis 2017 [39], Juncal-Ruiz 2018 [32], Haring 2015 [33], Song 2014 [34], Subanna 2020 [35], Ding 2014 [41], Mondelli 2015 [42], Borovcanin 2013 [30], Azizi 2019 [38] |
| IL-10 | 3 | 168/150 | 0.5 | 0.09, 0.90 | 0.02 | 68% | Noto 2015 [40], Juncal-Ruiz 2018 [32], Haring 2015 [33] |
| IL-17 | 3 | 203 | 0.29 | −0.49, 0.99 | 0.51 | 93% | Noto 2015 [40], Ding 2014 [41], Borovcanin 2013 [30] |
| IFN-γ | 5 | 261/243 | 0.38 | 0.13, 0.64 | 0.003 | 49% | Juncal-Ruiz 2018 [32], Haring 2015 [33], Ding 2014 [41], Mondelli 2015 [42], Borovcanin 2013 [30] |
| TNF-α | 7 | 346/328 | 0.35 | 0.03, 0.67 | 0.03 | 78% | Juncal-Ruiz 2018 [32], Haring 2015 [33], Song 2014 [34], Noto 2015 [40], Theodoropoulou 2001 [36], Song 2009 [37], Azizi 2019 [38] |
| Study | Duration | Cytokines | Medication | Sample | N |
|---|---|---|---|---|---|
| Noto, 2015 [40] | 10 weeks | IL-1b, Il-6, IL-4, IL-10 | Risperidone | serum | 55 |
| Petrikis, 2017 [39] | 6 weeks | IL-2, IL-6, TGF-β2 | Olanzapine, Risperidone, Aripiprazole, Quetiapine, Haloperidol | serum | 39 |
| Juncal-Ruiz, 2018 [32] | 12 weeks | IL-6 IL-1β TNF-α IFN-γ IL10 IL-17α IL-13 IL-12 IL-2 IL-21 IL-4 IL-23 IL-5 IL-7 IL-8 MIP-1α MIP-1β MIP-3α ITAC GMCSF Fractalkine | Aripiprazole, Risperidone | serum | 75 |
| Haring, 2015 [33] | 28 weeks | IL-2, IL-4, IL-6, IL-8, IL-10, VEGF, IFN-γ, TNF-α, IL-1α, IL-1β, MCP-1, EGF, | No data | serum | 38 |
| Song, 2014 [34] | 2, 4, 8, 12, 24 weeks | IL-1β, TNF-α, IL-6 | Risperidone | serum | 62 |
| Azizi, 2019 [38] | 12 weeks | TNF-α, IL-1β, IL6 | Risperidone | serum | 24 |
| Song, 2009 [37] | 4 weeks | TNF-α, IL-1β | Risperidone | serum | 83 |
| Subbanna, 2020 [35] | 12 weeks | IL-1β, IL-6, IL-17A, IL-23, IL-33 | No data | plasma | 27 |
| Ding 2014 [41] | 4 weeks | IL-17, IFN-γ, IL-6 | Risperidone | plasma | 69 |
| Mondelli 2015 [42] | 12 weeks | IFN-γ, IL-6 | Olanzapine, Risperidone, Quetiapine, Aripiprazole. | serum | 39 |
| Theodoropoulou 2001 [36] | 4 weeks | TNF-α, IL-2, IL-1β | No data | serum | 53 |
| Borovcanin 2013 [30] | 4 weeks | IFN-γ, IL-17, IL-4, IL-6, IL-27, TGF-β | No data | serum | 78 |
| Study | Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of the Outcome | Bias in Selection of the Reported Result |
|---|---|---|---|---|---|---|---|
| Noto, 2015 [40] | 2 | 1 | 1 | 0 | 1 | 1 | 2 |
| Petrikis, 2017 [39] | 2 | 3 | 1 | 0 | 1 | 1 | 1 |
| Juncal-Ruiz, 2018 [32] | 2 | 1 | 1 | 0 | 1 | 1 | 1 |
| Haring, 2015 [33] | 2 | 2 | 1 | 0 | 1 | 1 | 1 |
| Song, 2014 [34] | 1 | 1 | 1 | 0 | 1 | 1 | 1 |
| Azizi, 2019 [38] | 2 | 2 | 1 | 0 | 1 | 1 | 2 |
| Song, 2009 [37] | 1 | 1 | 1 | 0 | 1 | 1 | 1 |
| Subbanna, 2020 [35] | 1 | 2 | 1 | 0 | 1 | 1 | 2 |
| Ding 2014 [41] | 1 | 1 | 1 | 2 | 1 | 1 | 1 |
| Mondelli 2015 [42] | 2 | 1 | 1 | 0 | 1 | 1 | 1 |
| Theodoropoulou 2001 [36] | 3 | 1 | 1 | 1 | 1 | 1 | 1 |
| Borovcanin 2013 [30] | 3 | 2 | 1 | 1 | 1 | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcinowicz, P.; Więdłocha, M.; Zborowska, N.; Dębowska, W.; Podwalski, P.; Misiak, B.; Tyburski, E.; Szulc, A. A Meta-Analysis of the Influence of Antipsychotics on Cytokines Levels in First Episode Psychosis. J. Clin. Med. 2021, 10, 2488. https://doi.org/10.3390/jcm10112488
Marcinowicz P, Więdłocha M, Zborowska N, Dębowska W, Podwalski P, Misiak B, Tyburski E, Szulc A. A Meta-Analysis of the Influence of Antipsychotics on Cytokines Levels in First Episode Psychosis. Journal of Clinical Medicine. 2021; 10(11):2488. https://doi.org/10.3390/jcm10112488
Chicago/Turabian StyleMarcinowicz, Piotr, Magdalena Więdłocha, Natalia Zborowska, Weronika Dębowska, Piotr Podwalski, Błażej Misiak, Ernest Tyburski, and Agata Szulc. 2021. "A Meta-Analysis of the Influence of Antipsychotics on Cytokines Levels in First Episode Psychosis" Journal of Clinical Medicine 10, no. 11: 2488. https://doi.org/10.3390/jcm10112488