Comparison of Jaw Elevation Device vs. Conventional Airway Assist during Sedation in Chronic Kidney Diseases Undergoing Arteriovenous Fistula Surgery: A Randomized Controlled Trial

 ,
,
Abstract
:1. Introduction
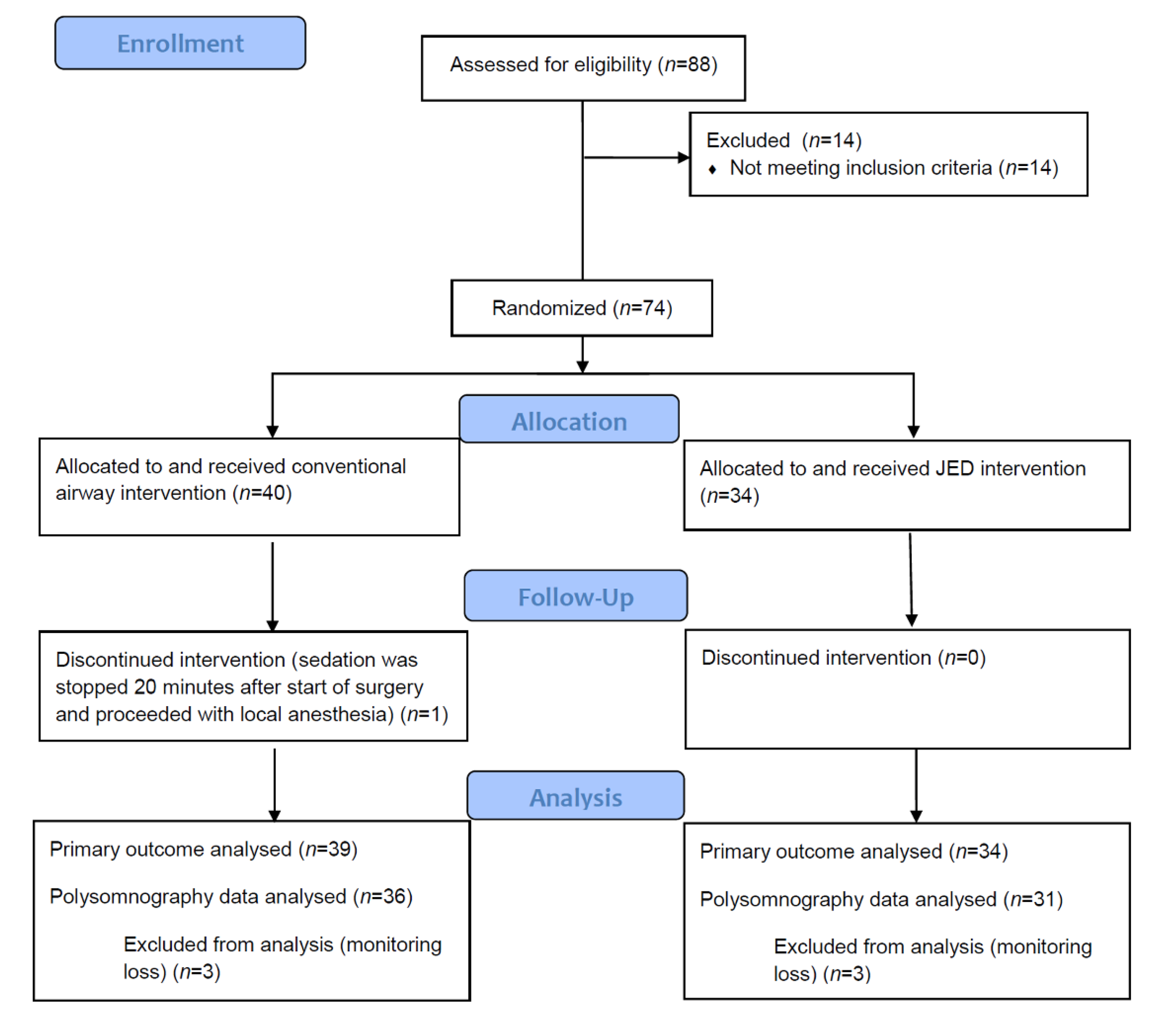
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lam, T.; Singh, M.; Yadollahi, A.; Chung, F. Is Perioperative Fluid and Salt Balance a Contributing Factor in Postoperative Worsening of Obstructive Sleep Apnea? Anesth. Analg. 2016, 122, 1335–1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrone, O.; Battaglia, S.; Steiropoulos, P.; Basoglu, O.K.; Kvamme, J.A.; Ryan, S.; Pepin, J.L.; Verbraecken, J.; Grote, L.; Hedner, J.; et al. Chronic kidney disease in European patients with obstructive sleep apnea: The ESADA cohort study. J. Sleep Res. 2016, 25, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Voulgaris, A.; Marrone, O.; Bonsignore, M.R.; Steiropoulos, P. Chronic kidney disease in patients with obstructive sleep apnea. A narrative review. Sleep Med. Rev. 2019, 47, 74–89. [Google Scholar] [CrossRef]
- Umbro, I.; Fabiani, V.; Fabiani, M.; Angelico, F.; Del Ben, M. A systematic review on the association between obstructive sleep apnea and chronic kidney disease. Sleep Med. Rev. 2020, 53, 101337. [Google Scholar] [CrossRef] [PubMed]
- Sekercioglu, N.; Curtis, B.; Murphy, S.; Barrett, B. Sleep apnea in patients with chronic kidney disease: A single center experience. Ren. Fail. 2015, 37, 83–87. [Google Scholar] [CrossRef]
- Shanmugam, G.V.; Abraham, G.; Mathew, M.; Ilangovan, V.; Mohapatra, M.; Singh, T. Obstructive sleep apnea in non-dialysis chronic kidney disease patients. Ren. Fail. 2015, 37, 214–218. [Google Scholar] [CrossRef] [Green Version]
- Mirrakhimov, A.E. Obstructive sleep apnea and kidney disease: Is there any direct link? Sleep Breath. 2012, 16, 1009–1016. [Google Scholar] [CrossRef]
- Lin, C.H.; Perger, E.; Lyons, O.D. Obstructive sleep apnea and chronic kidney disease. Curr. Opin. Pulm. Med. 2018, 24, 549–554. [Google Scholar] [CrossRef]
- Lee, Y.C.; Hung, S.Y.; Wang, H.K.; Lin, C.W.; Wang, H.H.; Chen, S.W.; Chang, M.Y.; Ho, L.C.; Chen, Y.T.; Liou, H.H.; et al. Sleep apnea and the risk of chronic kidney disease: A nationwide population-based cohort study. Sleep 2015, 38, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Hanly, P.J.; Ahmed, S.B. Sleep apnea and the kidney: Is sleep apnea a risk factor for chronic kidney disease? Chest 2014, 146, 1114–1122. [Google Scholar] [CrossRef]
- Abuyassin, B.; Sharma, K.; Ayas, N.T.; Laher, I. Obstructive Sleep Apnea and Kidney Disease: A Potential Bidirectional Relationship? J. Clin. Sleep Med. 2015, 11, 915–924. [Google Scholar] [CrossRef]
- Lin, C.H.; Lurie, R.C.; Lyons, O.D. Sleep Apnea and Chronic Kidney Disease: A State-of-the-Art Review. Chest 2020, 157, 673–685. [Google Scholar] [CrossRef]
- Cole, N.M.; Vlassakov, K.; Brovman, E.Y.; Heydarpour, M.; Urman, R.D. Regional Anesthesia for Arteriovenous Fistula Surgery May Reduce Hospital Length of Stay and Reoperation Rates. Vasc. Endovasc. Surg. 2018, 52, 418–426. [Google Scholar] [CrossRef]
- Kobayashi, M.; Ayuse, T.; Hoshino, Y.; Kurata, S.; Moromugi, S.; Schneider, H.; Kirkness, J.P.; Schwartz, A.R.; Oi, K. Effect of head elevation on passive upper airway collapsibility in normal subjects during propofol anesthesia. Anesthesiology 2011, 115, 273–281. [Google Scholar] [CrossRef] [Green Version]
- Ehsan, Z.; Mahmoud, M.; Shott, S.R.; Amin, R.S.; Ishman, S.L. The effects of anesthesia and opioids on the upper airway: A systematic review. Laryngoscope 2016, 126, 270–284. [Google Scholar] [CrossRef]
- Eastwood, P.R.; Platt, P.R.; Shepherd, K.; Maddison, K.; Hillman, D.R. Collapsibility of the upper airway at different concentrations of propofol anesthesia. Anesthesiology 2005, 103, 470–477. [Google Scholar] [CrossRef] [Green Version]
- Devaraj, U.; Rajagopala, S.; Kumar, A.; Ramachandran, P.; Devereaux, P.J.; D’Souza, G.A. Undiagnosed Obstructive Sleep Apnea and Postoperative Outcomes: A Prospective Observational Study. Respiration 2017, 94, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, G.V.; Horst, A.; Eberhardt, J.M.; Kumar, S.; Sarker, S. Obstructive sleep apnea in general surgery patients: Is it more common than we think? Am. J. Surg. 2014, 207, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Koh, K.F. Clinical update on managing the obstructed airway. Ann. Acad. Med. Singap. 2002, 31, 253–256. [Google Scholar] [PubMed]
- Ikeda, H.; Ayuse, T.; Oi, K. The effects of head and body positioning on upper airway collapsibility in normal subjects who received midazolam sedation. J. Clin. Anesth. 2006, 18, 185–193. [Google Scholar] [CrossRef]
- McKay, W.P.; Krysak, T.; Tyan, C.C. Investigation of a novel oral airway for awake flexible bronchoscopy. Can. J. Anaesth. 2020, 67, 1305–1306. [Google Scholar] [CrossRef] [PubMed]
- McKay, W.P. Description of a novel oral airway: The McKay airway. Can. J. Anaesth. 2020, 67, 1112–1113. [Google Scholar] [CrossRef] [PubMed]
- Altschul, D.J.; Vats, T.; Unda, S.R.; Osborn, I.; McHenry, J.; Zampolin, R. Jaw Elevation Device: Tool for Neck Immobilization to Facilitate Recovery in Endovascular Thrombectomy via Transcervical Access. World Neurosurg. 2020, 140, 109–113. [Google Scholar] [CrossRef]
- Chung, F.; Abdullah, H.R.; Liao, P. STOP-Bang Questionnaire: A Practical Approach to Screen for Obstructive Sleep Apnea. Chest 2016, 149, 631–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, F.; Subramanyam, R.; Liao, P.; Sasaki, E.; Shapiro, C.; Sun, Y. High STOP-Bang score indicates a high probability of obstructive sleep apnoea. Br. J. Anaesth. 2012, 108, 768–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, F.; Yang, Y.; Liao, P. Predictive performance of the STOP-Bang score for identifying obstructive sleep apnea in obese patients. Obes. Surg. 2013, 23, 2050–2057. [Google Scholar] [CrossRef]
- Tan, A.; Yin, J.D.; Tan, L.W.; van Dam, R.M.; Cheung, Y.Y.; Lee, C.H. Predicting obstructive sleep apnea using the STOP-Bang questionnaire in the general population. Sleep Med. 2016, 27–28, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Chung, F.; Elsaid, H. Screening for obstructive sleep apnea before surgery: Why is it important? Curr. Opin. Anaesthesiol. 2009, 22, 405–411. [Google Scholar] [CrossRef]
- Aarab, G.; Lobbezoo, F.; Hamburger, H.L.; Naeije, M. Variability in the apnea-hypopnea index and its consequences for diagnosis and therapy evaluation. Respiration 2009, 77, 32–37. [Google Scholar] [CrossRef]
- Cundrle, I., Jr.; Belehrad, M.; Jelinek, M.; Olson, L.J.; Ludka, O.; Sramek, V. The utility of perioperative polygraphy in the diagnosis of obstructive sleep apnea. Sleep Med. 2016, 25, 151–155. [Google Scholar] [CrossRef]
- Chen, H.; Lowe, A.A.; Bai, Y.; Hamilton, P.; Fleetham, J.A.; Almeida, F.R. Evaluation of a portable recording device (ApneaLink) for case selection of obstructive sleep apnea. Sleep Breath. 2009, 13, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.; Oh, M.; Chung, Y.H.; Ki, H.; Lee, J.J. Effects of continuous positive airway pressure in patients at high risk of obstructive sleep apnea during propofol sedation after spinal anesthesia. J. Clin. Monit. Comput. 2019, 33, 657–663. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Conventional Group n = 39 | JED Group n = 34 | p Value | |||
|---|---|---|---|---|---|
| Median (IQR) | 95% CI | Median (IQR) | 95% CI | ||
| Age (year) | 64.0 (55.8–71.5) | 61.9–69.0 | 61.5 (54.0–67.0) | 55.0–65.0 | 0.234 |
| Weight (kg) | 64.7 (58.5–70.7) | 60.5–69.3 | 66.2 (55.5–71.7) | 58.9–69.2 | 0.867 |
| Height (cm) | 165.7 (159.1–168.8) | 160.0–168.0 | 167.5 (160.0–171.0) | 164.5–170.0 | 0.279 |
| Male | 25 (64.1%) | 23 (67.6%) | 0.808 | ||
| Diabetes Mellitus (%) | 22 (56.4%) | 17 (51.5%) | 0.813 | ||
| Hypertension (%) | 33 (84.6%) | 27 (79.4%) | 0.760 | ||
| History of obstructive sleep apnea (%) | 4 (10.3%) | 6 (17.6%) | 0.499 | ||
| STOP-BANG score 1 | 4.0 (2.5–5.0) | 3.0–4.1 | 3.5 (3.0–5.0) | 3.0–4.2 | 0.860 |
| Conventional Group n = 39 | JED Group n = 34 | p Value | |||
|---|---|---|---|---|---|
| Median (IQR) | 95% CI | Median (IQR) | 95% CI | ||
| Surgery duration (min) | 83.0 (73.8–100.0) | 77.9–91.1 | 88.0 (77.0–97.0) | 81.7–92.5 | 0.756 |
| Intravenous crystalloid fluid (mL) | 170.0 (150.0–250.0) | 150–250 | 200.0 (150.0–300.0) | 150.0–300.0 | 0.528 |
| Midazolam (mg) | 1.0 (1.0–1.0) | 0.0–1.0 | 1.0 (1.0–1.0) | 0.0–1.0 | 0.507 |
| Hourly infused propofol (mg) | 2.49 (2.08–3.12) | 2.21–2.82 | 2.66 (2.02–3.12) | 2.14–3.01 | 0.748 |
| Hourly infused remifentanil (mcg) | 1.92 (1.54–2.38) | 1.66–2.10 | 2.07 (1.61–2.54) | 1.74–2.31 | 0.494 |
| Bispectral index (BIS) (n) | |||||
| Value ranges 60–80 | 29 (74.4%) | 23 (67.6%) | |||
| Value ranges/40–60 | 9 (23.0%) | 11 (32.4%) | |||
| BIS fail | 1 (2.6%) | 0 (0%) | 0.436 | ||
| Conventional Group n = 39 | JED Group n = 34 | p Value | |||
|---|---|---|---|---|---|
| Median (IQR) | 95% CI | Median (IQR) | 95% CI | ||
| Number of additional airway interventions in each patient, n | 1 (0.0–2.0) | 0–1.0 | 0 (0.0–0.0) | 0.0–0.0 | 0.002 |
| Number (%) of patients in each group with no requirement for additional airway interventions, n (%) | 17 (43.6%) | 26 (76.5%) | 0.004 | ||
| Number (%) of patients in each group with additional airway interventions applied during sedation | |||||
| (1) head lateral rotation | 18 (46.2%) | 1 (2.9%) | <0.001 | ||
| (2) neck extension | 8 (20.5%) | 1 (2.9%) | 0.032 | ||
| (3) oral airway insertion | 12 (30.8%) | 5 (14.7%) | 0.165 | ||
| (4) nasal airway insertion | 0 (0%) | 1 (2.9%) | 0.466 | ||
| (5) jaw thrust maneuver | 3 (7.7%) | 5 (14.7%) | 0.460 | ||
| Conventional Group n = 36 | JED Group n = 31 | ||||
|---|---|---|---|---|---|
| Median (IQR) | 95% CI | Median (IQR) | 95% CI | p value | |
| Polysomnography analysis time (min) | 77 (70.5–88.0) | 72.0–81.7 | 82 (74.5–91.8) | 77.6–90.4 | 0.280 |
| AHI | 9.3 (3.8–21.9) | 6.1–17.9 | 4.5 (1.5–11.9) | 1.7–7.6 | 0.015 |
| Snoring time (min) | 45.7 (29.7–56.0) | 37.3–54.8 | 39.2 (23.2–57.3) | 30.6–53.9 | 0.440 |
| Relative snoring time per analysis (%) | 63.8 (43.5–77.3) | 53.5–69.8 | 46.3 (27.9–76.5) | 39.8–70.9 | 0.228 |
| Average SpO2 | 98.9 (98.3–99.4) | 98.5–99.2 | 99.2 (98.4–99.9) | 98.9–99.4 | 0.206 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.H.; Jeong, J.S.; Jang, J.; Shin, Y.H.; Gil, N.-S.; Choi, J.-w.; Hahm, T.S. Comparison of Jaw Elevation Device vs. Conventional Airway Assist during Sedation in Chronic Kidney Diseases Undergoing Arteriovenous Fistula Surgery: A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 2280. https://doi.org/10.3390/jcm10112280
Lee SH, Jeong JS, Jang J, Shin YH, Gil N-S, Choi J-w, Hahm TS. Comparison of Jaw Elevation Device vs. Conventional Airway Assist during Sedation in Chronic Kidney Diseases Undergoing Arteriovenous Fistula Surgery: A Randomized Controlled Trial. Journal of Clinical Medicine. 2021; 10(11):2280. https://doi.org/10.3390/jcm10112280
Chicago/Turabian StyleLee, Sang Hyun, Ji Seon Jeong, Jaeni Jang, Young Hee Shin, Nam-Su Gil, Ji-won Choi, and Tae Soo Hahm. 2021. "Comparison of Jaw Elevation Device vs. Conventional Airway Assist during Sedation in Chronic Kidney Diseases Undergoing Arteriovenous Fistula Surgery: A Randomized Controlled Trial" Journal of Clinical Medicine 10, no. 11: 2280. https://doi.org/10.3390/jcm10112280