
Speckle-Tracking Echocardiography with Novel Imaging Technique of Higher Frame Rate

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Populations
2.2. Imaging Acquisition
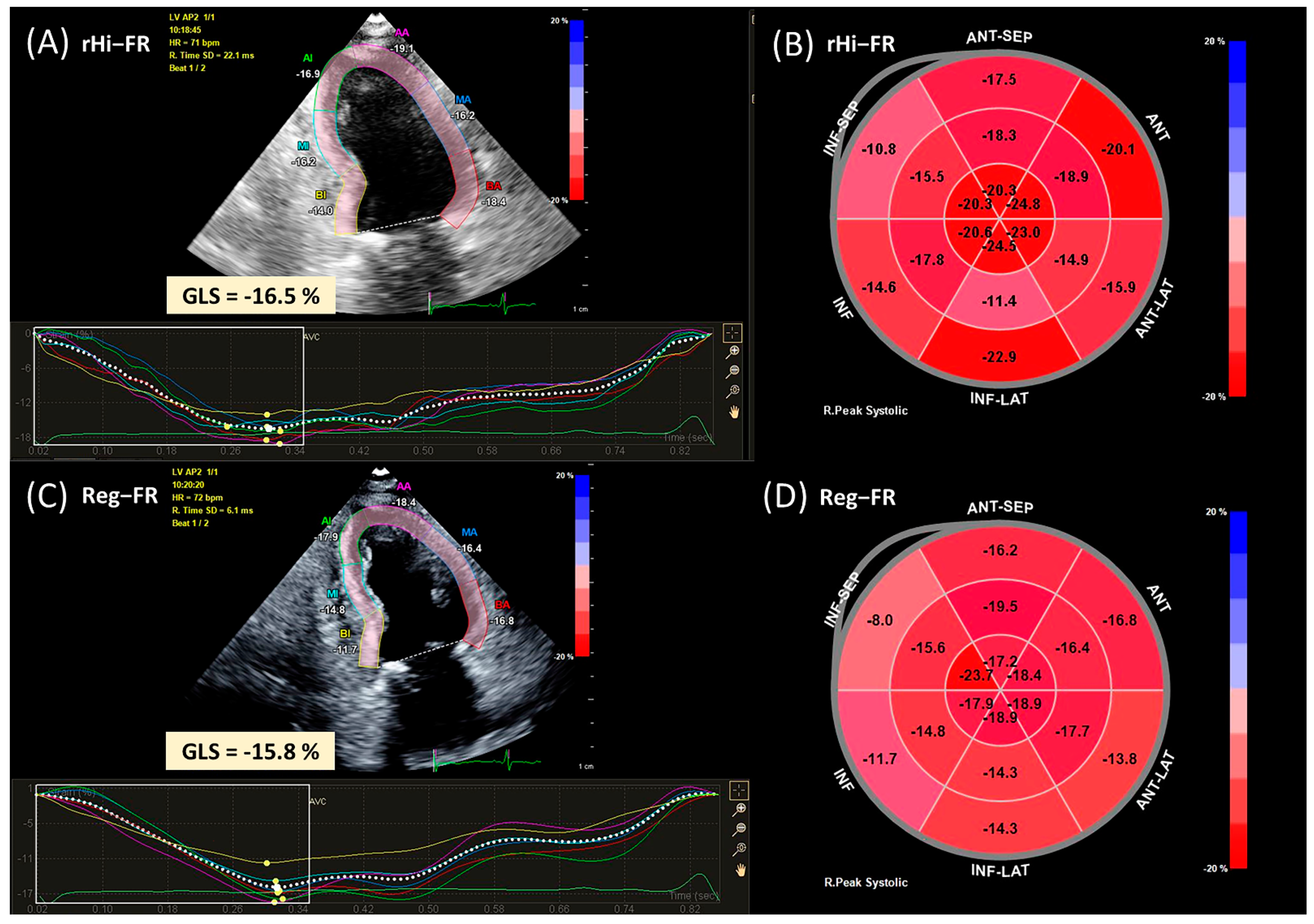
2.3. Speckle-Tracking Echocardiography—Strain Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Population and Characteristics
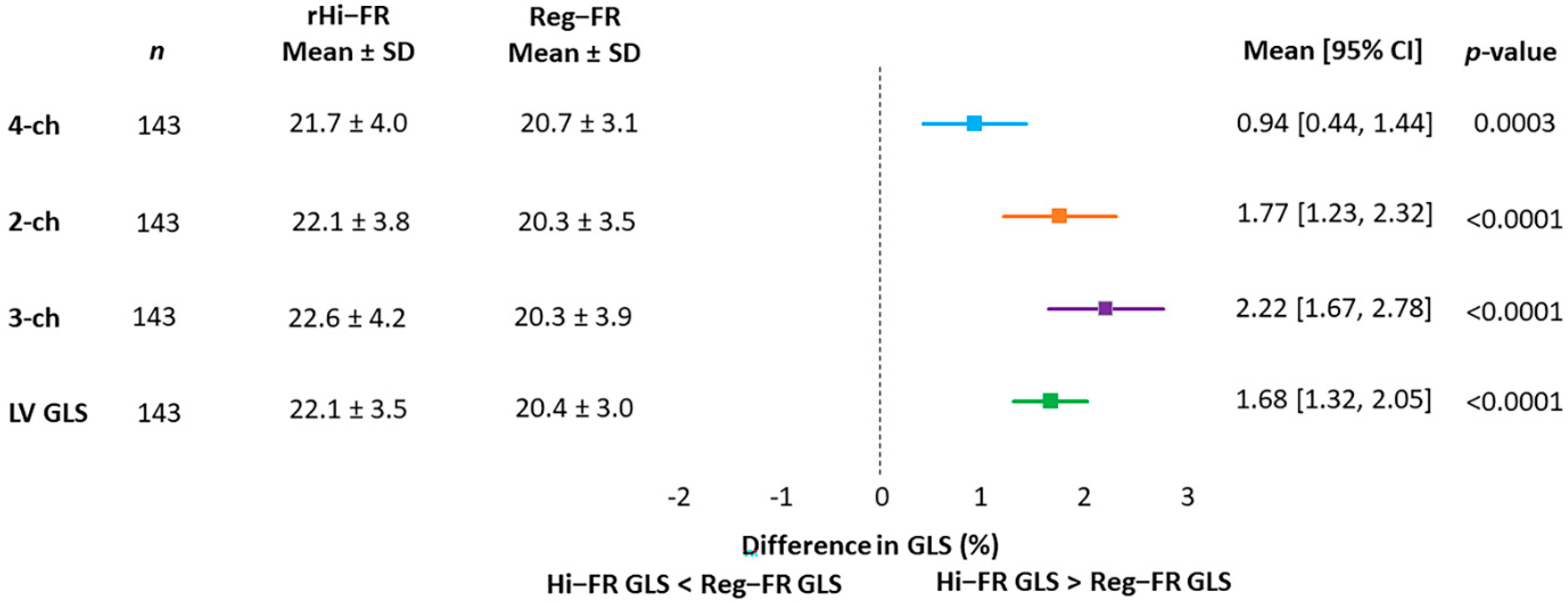
3.2. GLS in rHI-FR vs. REG-FR
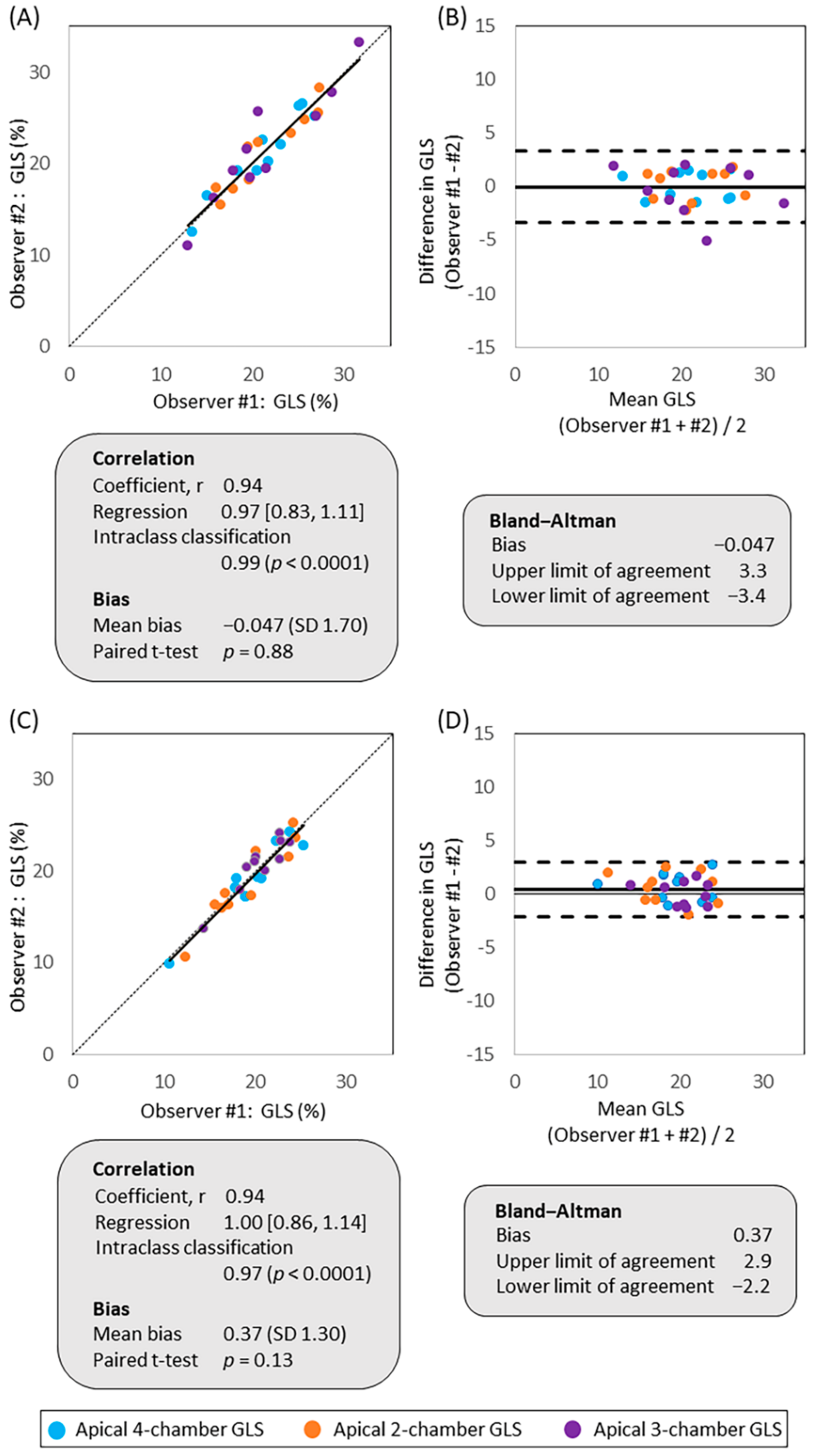
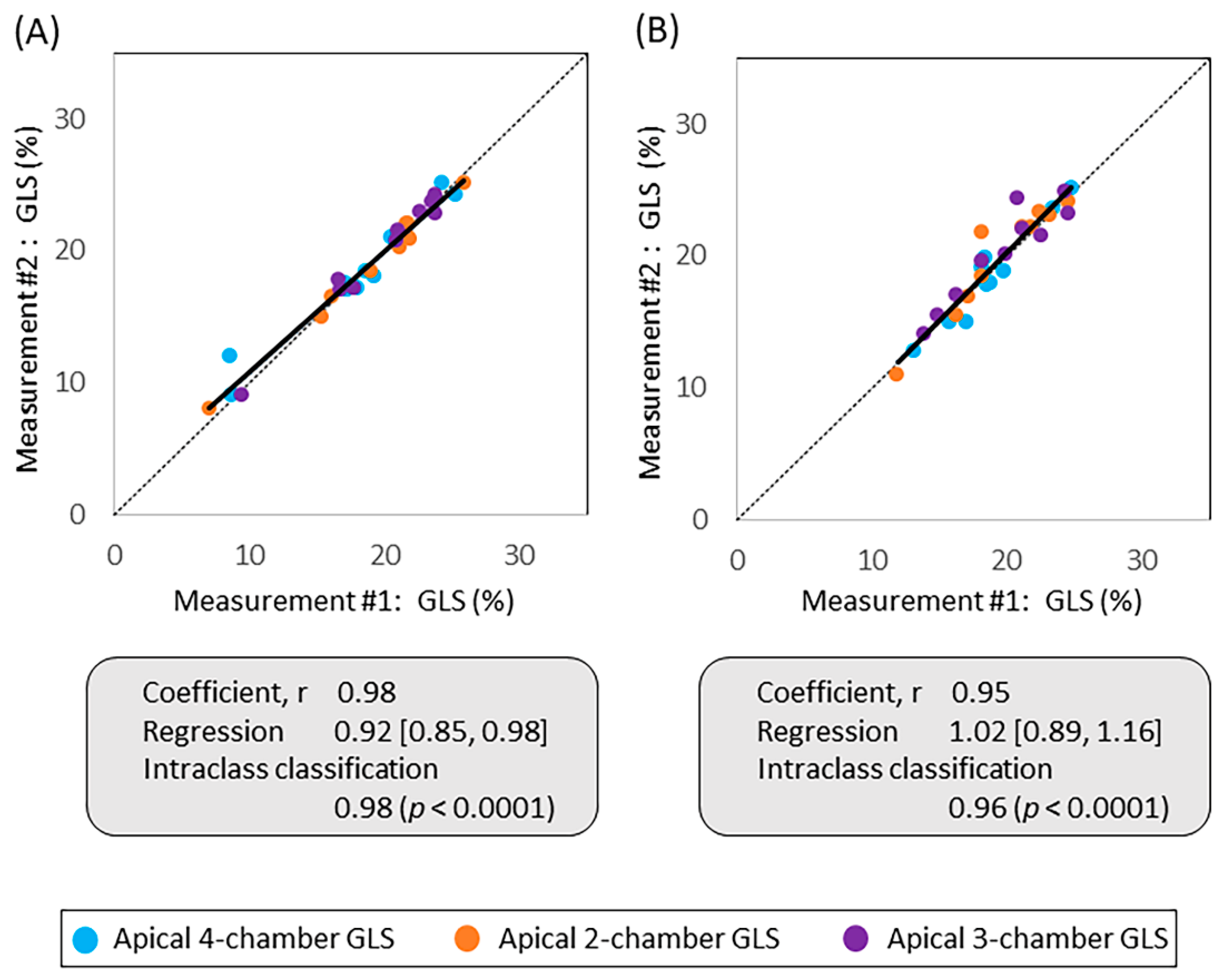
3.3. Inter-Observer and Intra-Observer Variabilities
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 2D | 2-dimensional |
| CAD | coronary artery disease |
| CI | confidence interval |
| FOV | field of view |
| GLS | global longitudinal strain |
| ICC | intraclass correlation coefficient |
| LV | left ventricle |
| LVEF | left ventricular ejection fraction |
| Reg-FR | regular (conventional) frame rate |
| rHi-FR | relatively high frame rate |
| STE | speckle-tracking echocardiography |
References
- Spencer, K.T.; Kimura, B.J.; Korcarz, C.E.; Pellikka, P.A.; Rahko, P.S.; Siegel, R.J. Focused Cardiac Ultrasound: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2013, 26, 567–581. [Google Scholar] [CrossRef] [PubMed]
- Collier, P.; Phelan, D.; Klein, A. A Test in Context: Myocardial Strain Measured by Speckle-Tracking Echocardiography. J. Am. Coll. Cardiol. 2017, 69, 1043–1056. [Google Scholar] [CrossRef] [PubMed]
- Rösner, A.; Barbosa, D.; Aarsæther, E.; Kjønås, D.; Schirmer, H.; D’Hooge, J. The influence of frame rate on two-dimensional speckle-tracking strain measurements: A study on silico-simulated models and images recorded in patients. Eur. Hear J.-Cardiovasc. Imaging 2015, 16, 1137–1147. [Google Scholar] [CrossRef] [PubMed]
- Voigt, J.-U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Hear J.-Cardiovasc. Imaging 2014, 16, 1–11. [Google Scholar] [CrossRef]
- Papadacci, C.; Pernot, M.; Couade, M.; Fink, M. High contrast ultrafast imaging of the human heart. IEEE Tran. Ultras. Ferroelect. Fre. Control 2016, 61, 288–301. [Google Scholar] [CrossRef] [PubMed]
- Poree, J.; Posada, D.; Hodzic, A.; Tournoux, F.; Cloutier, G.; Garcia, D. High-Frame-Rate Echocardiography Using Coherent Compounding with Doppler-Based Motion-Compensation. IEEE Trans. Med. Imaging 2016, 35, 1647–1657. [Google Scholar] [CrossRef] [PubMed]
- Joos, P.; Poree, J.; Liebgott, H.; Vray, D.; Baudet, M.; Faurie, J.; Tournoux, F.; Cloutier, G.; Nicolas, B.; Garcia, D. High-Frame-Rate Speckle-Tracking Echocardiography. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2018, 65, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.-N.; Provost, J.; Fujikura, K.; Konofagou, E.E. In vivo study of myocardial elastography under graded ischemia conditions. Phys. Med. Biol. 2011, 56, 1155–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.P.; et al. Expert Consensus for Multimodality Imaging Evaluation of Adult Patients during and after Cancer Therapy: A Report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2014, 27, 911–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunting, K.V.; Steeds, R.P.; Slater, L.T.; Rogers, J.K.; Gkoutos, G.V.; Kotecha, D. A Practical Guide to Assess the Reproducibility of Echocardiographic Measurements. J. Am. Soc. Echocardiogr. 2019, 32, 1505–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellerin, D.; Sharma, R.; Elliott, P.; Veyrat, C. Tissue Doppler, strain, and strain rate echocardiography for the assessment of left and right systolic ventricular function. Heart 2003, 89, 9–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, J.; Fujikura, K.; Homma, S.; Konofagou, E.E. Myocardial Elastography at Both High Temporal and Spatial Resolution for the Detection of Infarcts. Ultrasound Med. Biol. 2007, 33, 1206–1223. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Varghese, T.; Rahko, P.S.; Zagzebski, J. Ultrasound frame rate requirements for cardiac elastography: Experimental and in vivo results. Ultrasonics 2009, 49, 98–111. [Google Scholar] [CrossRef] [PubMed]
- Amzulescu, M.S.; De Craene, M.; Langet, H.; Pasquet, A.; Vancraeynest, D.; Pouleur, A.C.; Vanoverschelde, J.L.; Gerber, B.L. Myocardial strain imaging: Review of general principles, validation, and sources of discrepancies. Eur. Hear J.-Cardiovasc. Imaging 2019, 20, 605–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, S.; Larson, M.G.; McCabe, E.L.; Osypiuk, E.; Lehman, B.T.; Stanchev, P.; Aragam, J.; Benjamin, E.J.; Solomon, S.D.; Vasan, R.S. Reproducibility of Speckle-Tracking-Based Strain Measures of Left Ventricular Function in a Community-Based Study. J. Am. Soc. Echocardiogr. 2013, 26, 1258–1266.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellikka, P.A.; Arruda-Olson, A.; Chaudhry, F.A.; Chen, M.H.; Marshall, J.E.; Porter, T.R.; Sawada, S.G. Guidelines for Performance, Interpretation, and Application of Stress Echocardiography in Ischemic Heart Disease: From the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2020, 33, 1–41.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joyce, E.; Hoogslag, G.E.; Al Amri, I.; Debonnaire, P.; Katsanos, S.; Bax, J.J.; Delgado, V.; Marsan, N.A. Quantitative Dobutamine Stress Echocardiography Using Speckle-Tracking Analysis versus Conventional Visual Analysis for Detection of Significant Coronary Artery Disease after ST-Segment Elevation Myocardial Infarction. J. Am. Soc. Echocardiogr. 2015, 28, 1379–1389.e1. [Google Scholar] [CrossRef] [PubMed]
- Yü, Y.; Villarraga, H.R.; Saleh, H.K.; Cha, S.S.; Pellikka, P.A. Can ischemia and dyssynchrony be detected during early stages of dobutamine stress echocardiography by 2-dimensional speckle tracking echocardiography? Int. J. Cardiovasc. Imaging 2012, 29, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, A.A.; Levy, P.T.; Sekarski, T.J.; Hamvas, A.; Holland, M.R.; Singh, G.K. Effects of Frame Rate on Two-Dimensional Speckle Tracking-Derived Measurements of Myocardial Deformation in Premature Infants. Echocardiography 2015, 32, 839–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farsalinos, K.E.; Daraban, A.M.; Ünlü, S.; Thomas, J.D.; Badano, L.P.; Voigt, J.-U. Head-to-head comparison of global longitudinal strain measurements among nine different vendors: The EACVI/ASE inter-vendor comparison study. J. Am. Soc. Echocardiogr. 2015, 28, 1171–1181.e2. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 143 | |
|---|---|
| Male, n (%) | 47 (32.9) |
| Age, mean ± SD (y) | 60.1 ± 15.1 |
| Ethnicity | |
| African American, n (%) | 42 (29.4) |
| Hispanic, n (%) | 61 (42.7) |
| Caucasian, n (%) | 10 (7.0) |
| Asian, n (%) | 2 (1.4) |
| Others, n (%) | 28 (19.6) |
| Hypertension, n (%) | 96 (67.1) |
| Diabetes, n (%) | 42 (29.4) |
| Coronary artery disease, n (%) | 25 (17.5) |
| Hyperlipidemia, n (%) | 74 (51.8) |
| Body surface area, mean ± SD (m2) | 1.84 ± 0.23 |
| Systolic blood pressure, mean ± SD (mmHg) | 133.3 ± 23.2 |
| Diastolic blood pressure, mean ± SD (mmHg) | 77.2 ± 11.8 |
| Heart rate, mean ± SD (beat per minute) | 70.6 ± 12.7 |
| LVEF, mean ± SD (%) | 63.0 ± 5.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujikura, K.; Makkiya, M.; Farooq, M.; Xing, Y.; Humphrey, W.; Mustehsan, M.H.; Garcia, M.J.; Taub, C.C. Speckle-Tracking Echocardiography with Novel Imaging Technique of Higher Frame Rate. J. Clin. Med. 2021, 10, 2095. https://doi.org/10.3390/jcm10102095
Fujikura K, Makkiya M, Farooq M, Xing Y, Humphrey W, Mustehsan MH, Garcia MJ, Taub CC. Speckle-Tracking Echocardiography with Novel Imaging Technique of Higher Frame Rate. Journal of Clinical Medicine. 2021; 10(10):2095. https://doi.org/10.3390/jcm10102095
Chicago/Turabian StyleFujikura, Kana, Mohammed Makkiya, Muhammad Farooq, Yun Xing, Wayne Humphrey, Mohammad Hashim Mustehsan, Mario J. Garcia, and Cynthia C. Taub. 2021. "Speckle-Tracking Echocardiography with Novel Imaging Technique of Higher Frame Rate" Journal of Clinical Medicine 10, no. 10: 2095. https://doi.org/10.3390/jcm10102095