
The Use of Propofol versus Dexmedetomidine for Patients Receiving Drug-Induced Sleep Endoscopy: A Meta-Analysis of Randomized Controlled Trials

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection Criteria and Data Extraction
2.3. Primary Outcome, Secondary Outcomes, and Definitions
2.4. Assessment of Risk of Bias for Included Studies
2.5. Statistical Analysis
3. Results
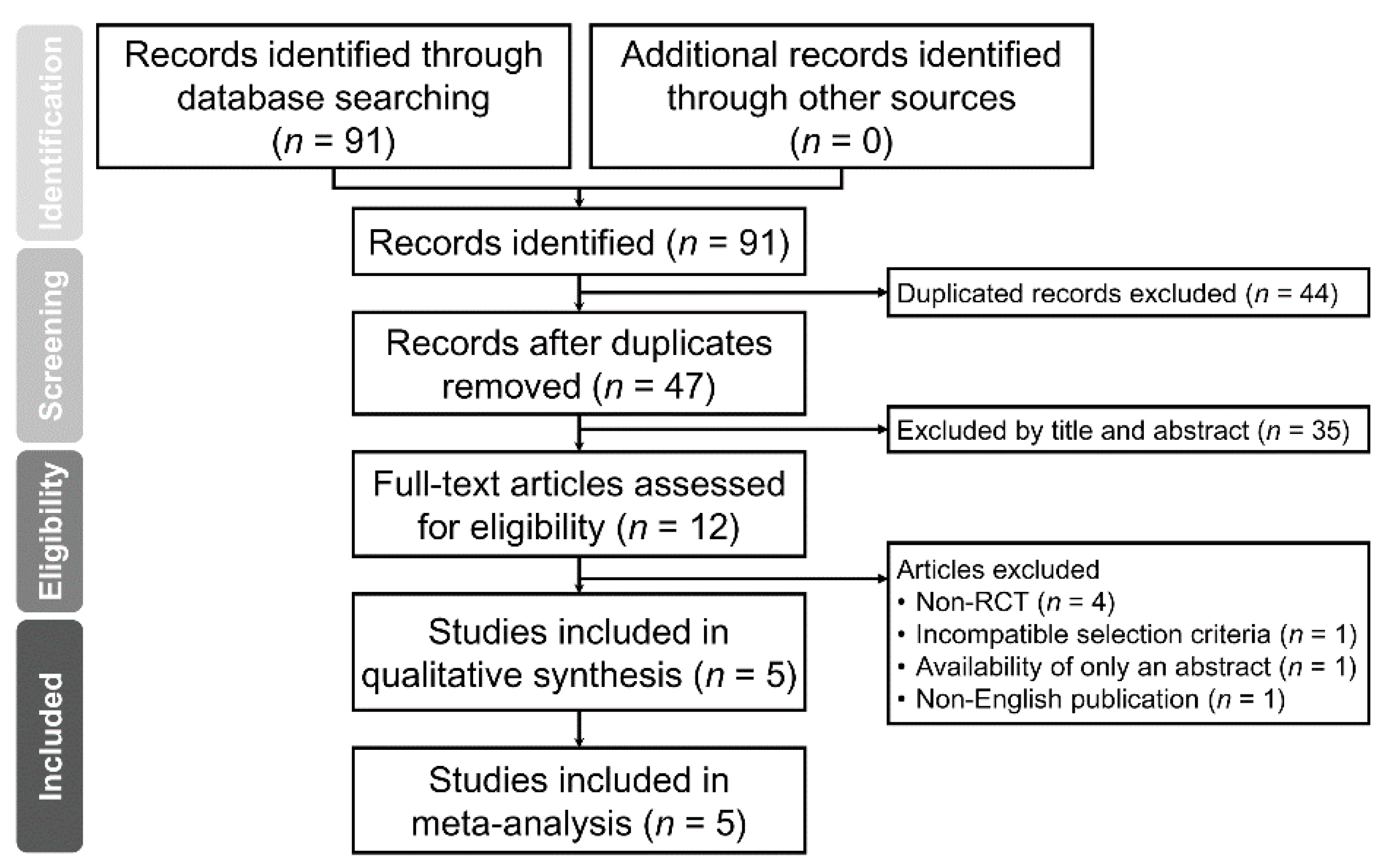
3.1. Study Selection
3.2. Characteristics of Included Studies
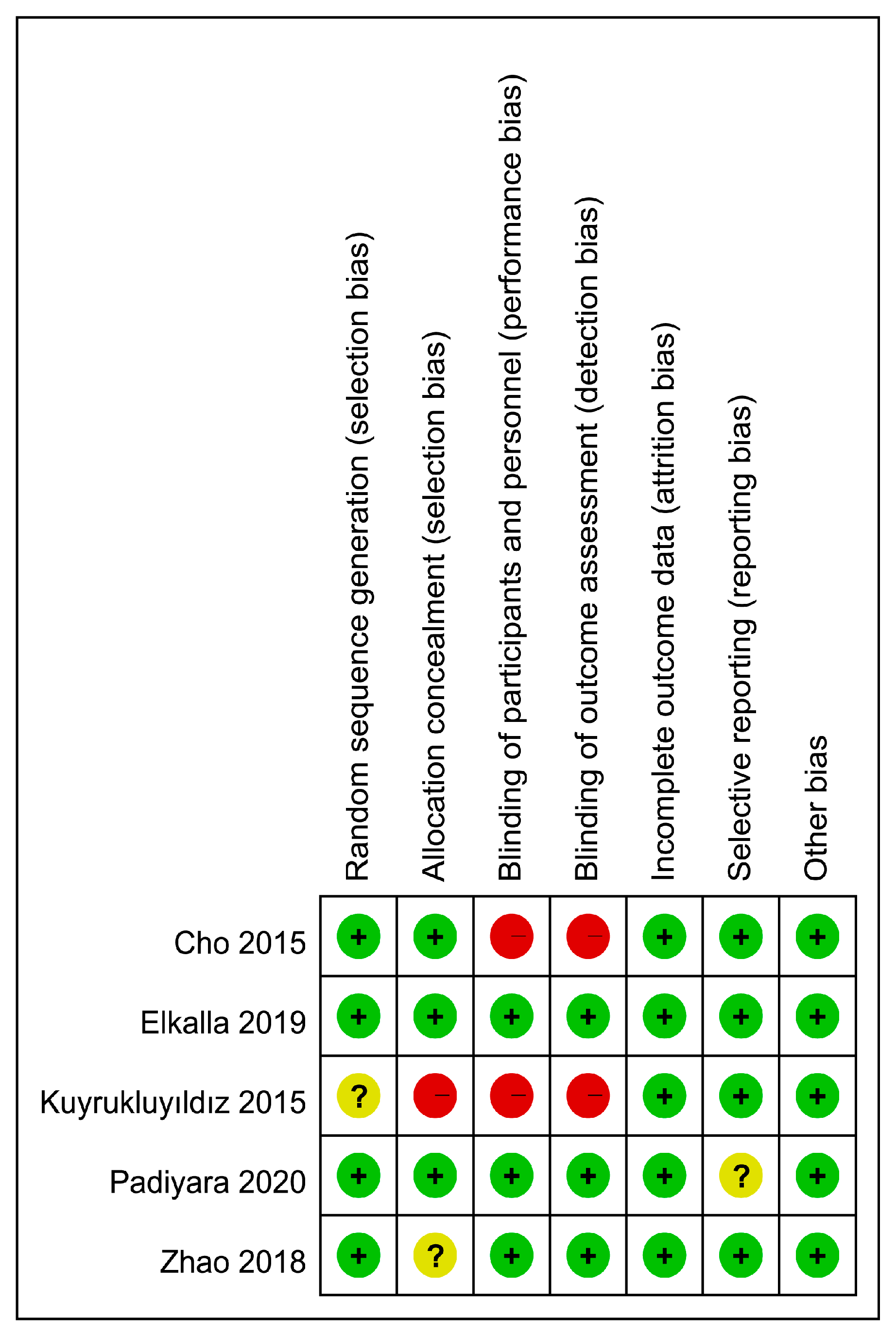
3.3. Risk of Bias Assessment
3.4. Sedative Outcomes
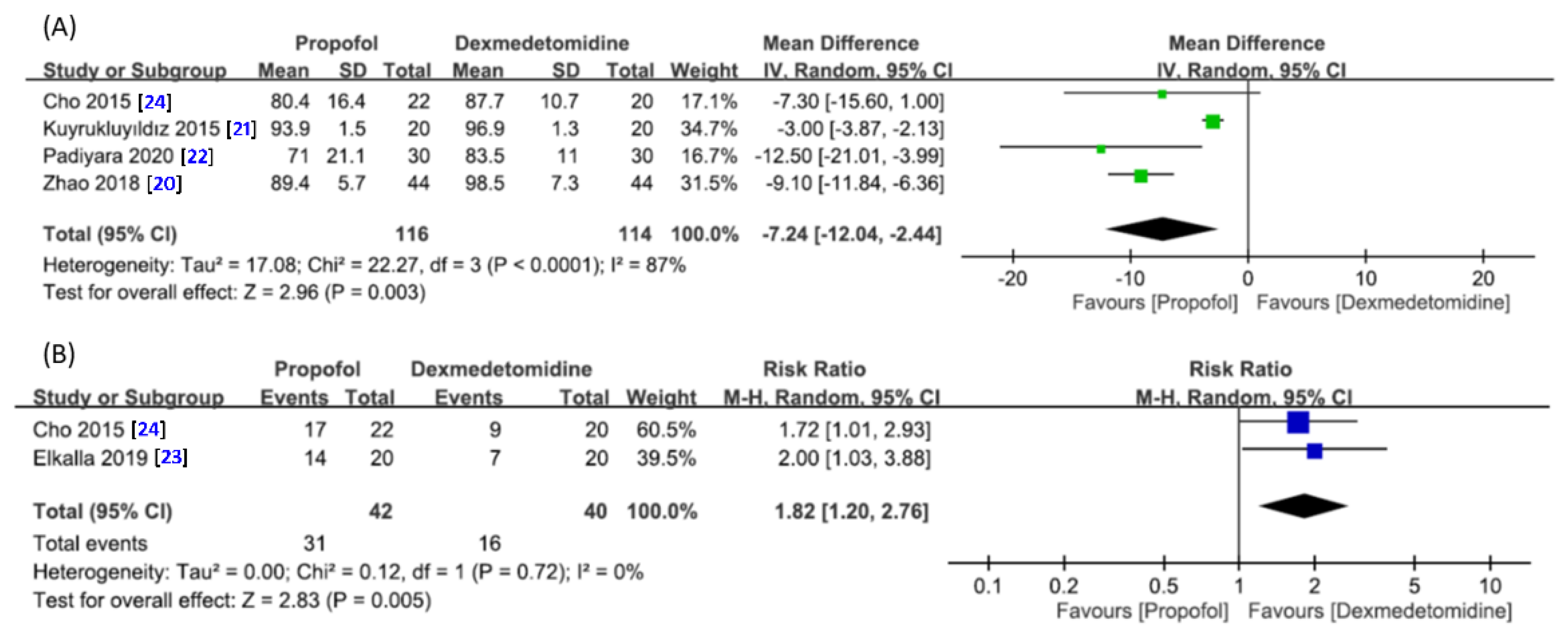
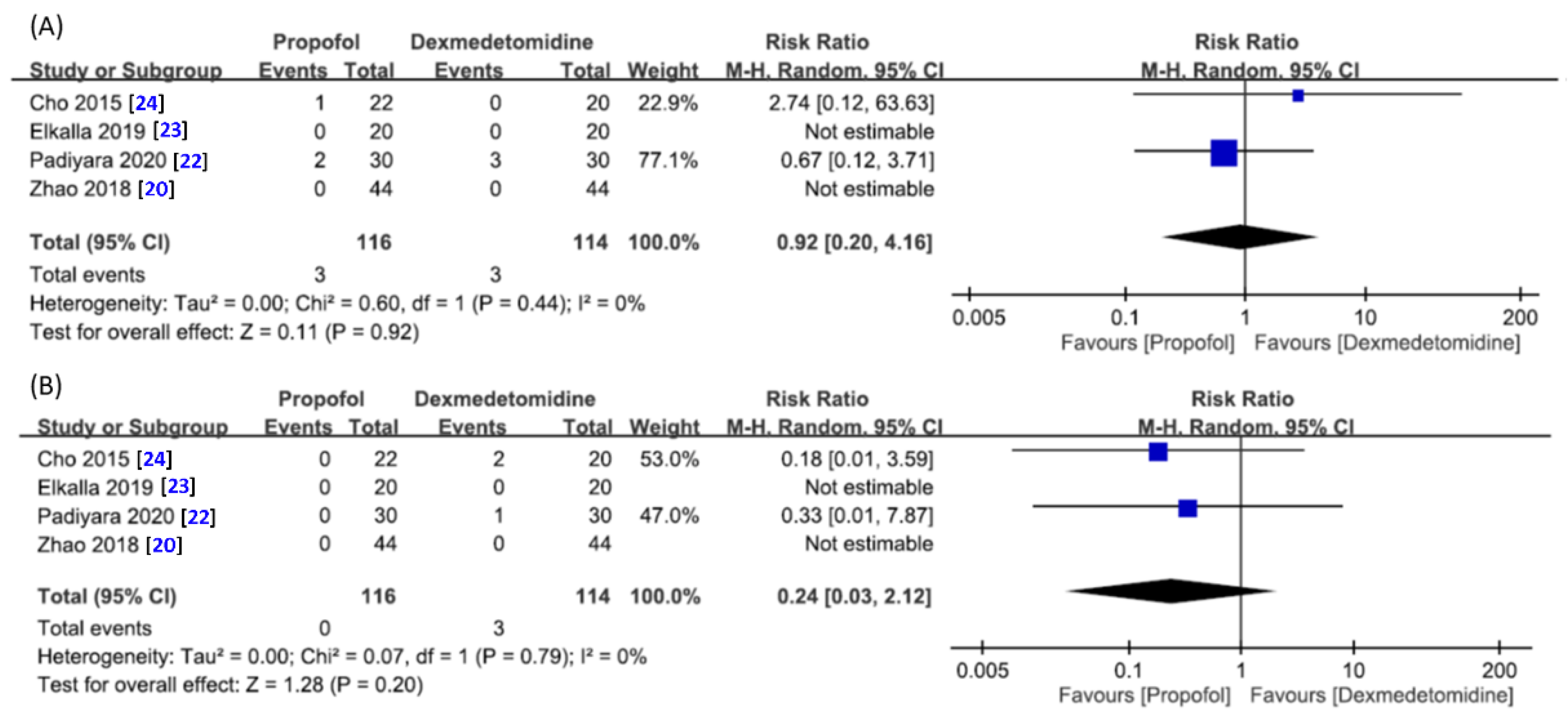
3.4.1. Difference in Minimum Oxygen Saturation and Risk of Desaturation
3.4.2. Risk of Failed Sedation Procedure for Drug-Induced Sleep Endoscopy
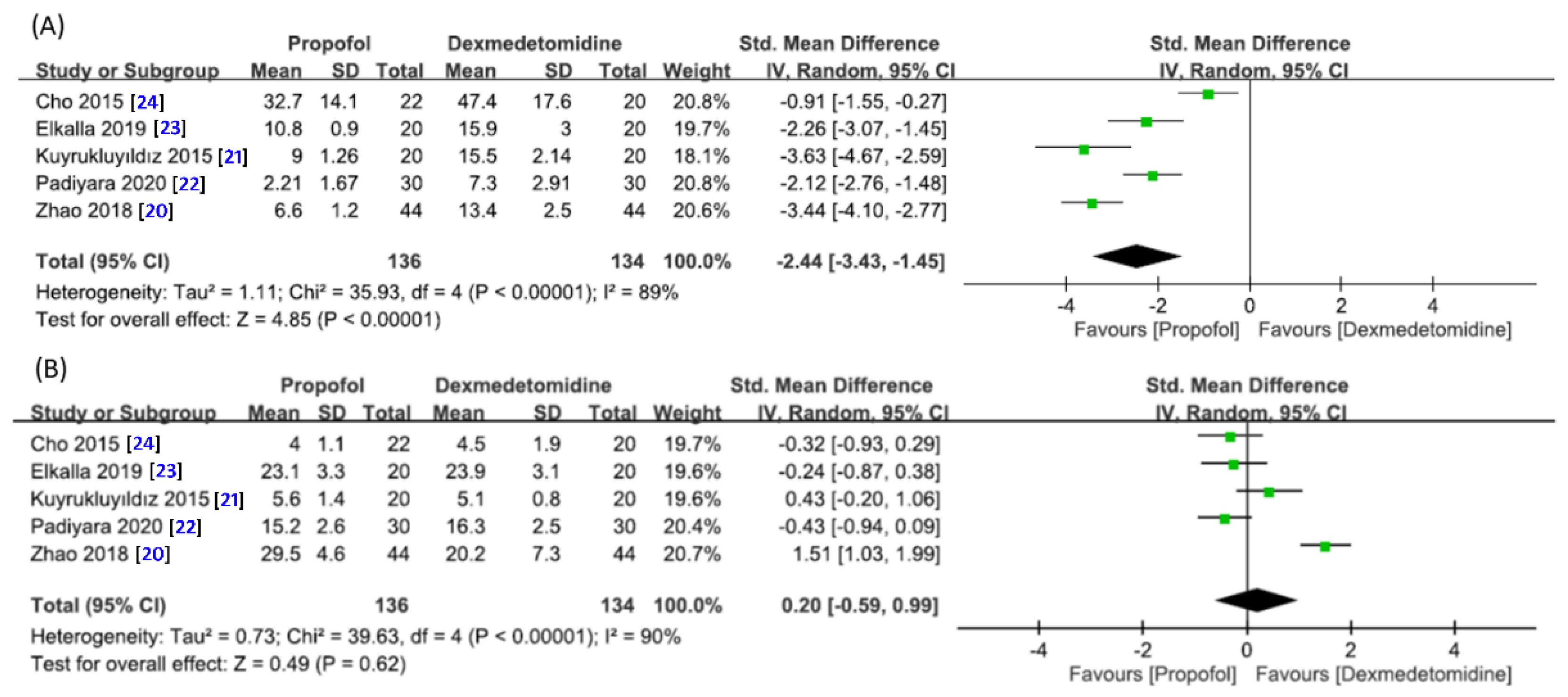
3.4.3. Time to Fall Asleep and Duration of Endoscopic Examination
3.4.4. Risk of Hypotension or Bradycardia
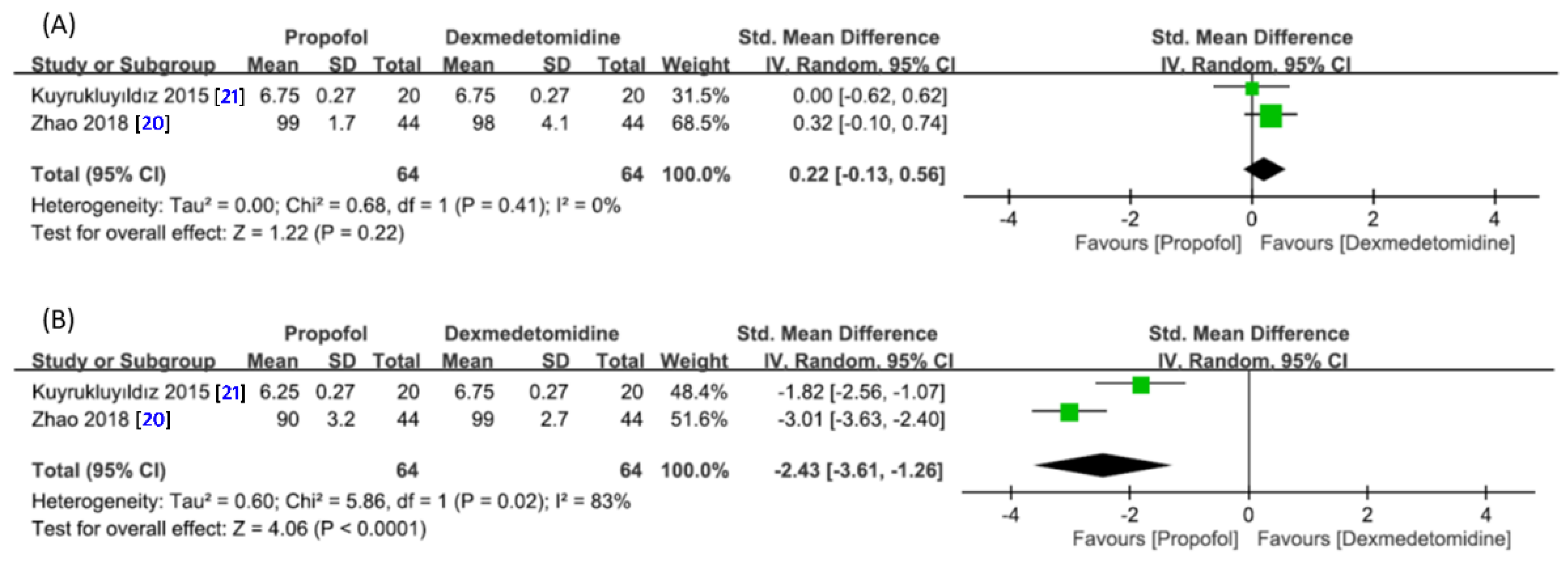
3.4.5. Satisfaction of Endoscopic Performers or Patients with the Sedation Technique
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Barrera, J.E.; Pau, C.Y.; Forest, V.I.; Holbrook, A.B.; Popelka, G.R. Anatomic measures of upper airway structures in obstructive sleep apnea. World J. Otorhinolaryngol. Head Neck Surg. 2017, 3, 85–91. [Google Scholar] [CrossRef]
- Osman, A.M.; Carberry, J.C.; Burke, P.G.; Toson, B.; Grunstein, R.R.; Eckert, D.J. Upper airway collapsibility measured using a simple wakefulness test closely relates to the pharyngeal critical closing pressure during sleep in obstructive sleep apnea. Sleep 2019, 42, zsz080. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, C.; Berthon-Jones, M.; Issa, F.; Eves, L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet 1981, 1, 862–865. [Google Scholar] [CrossRef]
- Zaghi, S.; Holty, J.-E.C.; Certal, V.; Abdullatif, J.; Guilleminault, C.; Powell, N.B.; Riley, R.W.; Camacho, M. Maxillomandibular Advancement for Treatment of Obstructive Sleep Apnea: A Meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Jo, S.Y.; Lee, S.M.; Lee, K.H.; Kim, D.K. Effect of long-term oral appliance therapy on obstruction pattern in patients with obstructive sleep apnea. Eur. Arch. Otorhinolaryngol. 2018, 275, 1327–1333. [Google Scholar] [CrossRef] [PubMed]
- Camacho, M.; Dunn, B.; Torre, C.; Sasaki, J.; Gonzales, R.; Liu, S.Y.-C.; Chan, D.K.; Certal, V.; Cable, B.B. Supraglottoplasty for laryngomalacia with obstructive sleep apnea: A systematic review and meta-analysis. Laryngoscope 2016, 126, 1246–1255. [Google Scholar] [CrossRef] [Green Version]
- Camacho, M.; Li, D.; Kawai, M.; Zaghi, S.; Teixeira, J.; Senchak, A.J.; Brietzke, S.E.; Frasier, S.; Certal, V. Tonsillectomy for adult obstructive sleep apnea: A systematic review and meta-analysis. Laryngoscope 2016, 126, 2176–2186. [Google Scholar] [CrossRef]
- Tanna, N.; Smith, B.D.; Zapanta, P.E.; Karanetz, I.; Andrews, B.T.; Urata, M.M.; Bradley, J.P. Surgical Management of Obstructive Sleep Apnea. Plast. Reconstr. Surg. 2016, 137, 1263–1272. [Google Scholar] [CrossRef]
- Katsantonis, G.P.; Maas, C.S.; Walsh, J.K. The predictive efficacy of the Müller maneuver in uvulopalatopharyngoplasty. Laryngoscope 1989, 99, 677–680. [Google Scholar] [CrossRef]
- Croft, C.B.; Pringle, M. Sleep nasendoscopy: A technique of assessment in snoring and obstructive sleep apnoea. Clin. Otolaryngol. Allied Sci. 1991, 16, 504–509. [Google Scholar] [CrossRef]
- Razek, A.A.K.A. Diagnostic Role of Magnetic Resonance Imaging in Obstructive Sleep Apnea Syndrome. J. Comput. Assist. Tomogr. 2015, 39, 565–571. [Google Scholar] [CrossRef]
- Chong, K.B.; De Vito, A.; Vicini, C. Drug-Induced Sleep Endoscopy in Treatment Options Selection. Sleep Med. Clin. 2019, 14, 33–40. [Google Scholar] [CrossRef]
- Blumen, M.; Bequignon, E.; Chabolle, F. Drug-induced sleep endoscopy: A new gold standard for evaluating OSAS? Part II: Results. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2017, 134, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Heiser, C.; Fthenakis, P.; Hapfelmeier, A.; Berger, S.; Hofauer, B.; Hohenhorst, W.; Kochs, E.F.; Wagner, K.J.; Edenharter, G.M. Drug-induced sleep endoscopy with target-controlled infusion using propofol and monitored depth of sedation to determine treatment strategies in obstructive sleep apnea. Sleep Breath. 2017, 21, 737–744. [Google Scholar] [CrossRef]
- Kim, J.S.; Heo, S.J. Test-retest reliability of drug-induced sleep endoscopy using midazolam. J. Clin. Sleep Med. 2020, 16, 675–678. [Google Scholar] [CrossRef] [PubMed]
- Viana, A.; Zhao, C.; Rosa, T.; Couto, A.; Neves, D.D.; Araújo-Melo, M.H.; Capasso, R. The Effect of Sedating Agents on Drug-Induced Sleep Endoscopy Findings. Laryngoscope 2019, 129, 506–513. [Google Scholar] [CrossRef]
- Chang, E.T.; Certal, V.; Song, S.A.; Zaghi, S.; Carrasco-Llatas, M.; Torre, C.; Capasso, R.; Camacho, M. Dexmedetomidine versus propofol during drug-induced sleep endoscopy and sedation: A systematic review. Sleep Breath. 2017, 21, 727–735. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Chin. Integr. Med. 2009, 7, 889–896. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Zhao, L.L.; Liu, H.; Zhang, Y.Y.; Wei, J.Q.; Han, Y.; Han, L.; Yang, J.P. A Comparative Study on Efficacy and Safety of Propofol versus Dexmedetomidine in Sleep Apnea Patients undergoing Drug-Induced Sleep Endoscopy: A Consort-Prospective, Randomized, Controlled Clinical Trial. BioMed Res. Int. 2018, 2018, 8696510. [Google Scholar] [CrossRef]
- Kuyrukluyıldız, U.; Binici, O.; Onk, D.; Celik, S.A.; Torun, M.T.; Unver, E.; Ozcicek, A.; Alagol, A. Comparison of dexmedetomidine and propofol used for drug-induced sleep endoscopy in patients with obstructive sleep apnea syndrome. Int. J. Clin. Exp. Med. 2015, 8, 5691–5698. [Google Scholar]
- Padiyara, T.V.; Bansal, S.; Jain, D.; Arora, S.; Gandhi, K. Dexmedetomidine versus propofol at different sedation depths during drug-induced sleep endoscopy: A randomized trial. Laryngoscope 2020, 130, 257–262. [Google Scholar] [CrossRef]
- Elkalla, R.S.; El Mourad, M.B. Respiratory and hemodynamic effects of three different sedative regimens for drug induced sleep endoscopy in sleep apnea patients. A prospective randomized study. Minerva Anestesiol. 2020, 86, 132–140. [Google Scholar] [CrossRef]
- Cho, J.S.; Soh, S.; Kim, E.J.; Cho, H.J.; Shin, S.; Kim, H.J.; Koo, B.N. Comparison of three sedation regimens for drug-induced sleep endoscopy. Sleep Breath. 2015, 19, 711–717. [Google Scholar] [CrossRef]
- Barr, J.; Fraser, G.L.; Puntillo, K.; Ely, E.W.; Gélinas, C.; Dasta, J.F.; Davidson, J.E.; Devlin, J.W.; Kress, J.P.; Joffe, A.M.; et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit. Care Med. 2013, 41, 263–306. [Google Scholar] [CrossRef]
- Sundaram, S.; Lim, J.; Lasserson, T.J. Surgery for obstructive sleep apnoea. Cochrane Database Syst. Rev. 2005, 4, Cd001004. [Google Scholar]
- Blumen, M.; Bequignon, E.; Chabolle, F. Drug-induced sleep endoscopy: A new gold standard for evaluating OSAS? Part I: Technique. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2017, 134, 101–107. [Google Scholar] [CrossRef]
- Weerink, M.A.; Struys, M.M.; Hannivoort, L.N.; Barends, C.R.; Absalom, A.R.; Colin, P. Clinical Pharmacokinetics and Pharmacodynamics of Dexmedetomidine. Clin. Pharmacokinet. 2017, 56, 893–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lodenius, Å.; Ebberyd, A.; Hårdemark Cedborg, A.; Hagel, E.; Mkrtchian, S.; Christensson, E.; Ullman, J.; Scheinin, M.; Eriksson, L.I.; Jonsson Fagerlund, M. Sedation with Dexmedetomidine or Propofol Impairs Hypoxic Control of Breathing in Healthy Male Volunteers: A Nonblinded, Randomized Crossover Study. Anesthesiology 2016, 125, 700–715. [Google Scholar] [CrossRef]
- Belleville, J.P.; Ward, D.S.; Bloor, B.C.; Maze, M. Effects of intravenous dexmedetomidine in humans. I. Sedation, ventilation, and metabolic rate. Anesthesiology 1992, 77, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H.; Rosenberg, J. Late post-operative hypoxaemia and organ dysfunction. Eur. J. Anaesthesiol. Suppl. 1995, 10, 31–34. [Google Scholar] [PubMed]
- Holm, C.; Christensen, M.; Rasmussen, V.; Schulze, S.; Rosenberg, J. Hypoxaemia and myocardial ischaemia during colonoscopy. Scand. J. Gastroenterol. 1998, 33, 769–772. [Google Scholar]
- Johnston, S.D.; McKenna, A.; Tham, T.C.K. Silent myocardial ischaemia during endoscopic retrograde cholangiopancreatography. Endoscopy 2003, 35, 1039–1042. [Google Scholar] [CrossRef]
- Patel, N.; Donahue, C.; Shenoy, A.; Patel, A.; El-Sherif, N. Obstructive sleep apnea and arrhythmia: A systemic review. Int. J. Cardiol. 2017, 228, 967–970. [Google Scholar] [CrossRef]
- Ruokonen, E.; Parviainen, I.; Jakob, S.M.; Nunes, S.; Kaukonen, M.; Shepherd, S.T.; Sarapohja, T.; Bratty, J.R.; Takala, J. Dexmedetomidine versus propofol/midazolam for long-term sedation during mechanical ventilation. Intensive Care Med. 2009, 35, 282–290. [Google Scholar] [CrossRef]
- Holliday, S.F.; Kane-Gill, S.L.; Empey, P.E.; Buckley, M.S.; Smithburger, P.L. Interpatient variability in dexmedetomidine response: A survey of the literature. Sci. World J. 2014, 2014, 805013. [Google Scholar] [CrossRef] [Green Version]
- Cavaliere, M.; Russo, F.; Iemma, M. Awake versus drug-induced sleep endoscopy: Evaluation of airway obstruction in obstructive sleep apnea/hypopnoea syndrome. Laryngoscope 2013, 123, 2315–2318. [Google Scholar] [CrossRef]
- Salamanca, F.; Costantini, F.; Bianchi, A.; Amaina, T.; Colombo, E.; Zibordi, F. Identification of obstructive sites and patterns in obstructive sleep apnoea syndrome by sleep endoscopy in 614 patients. Acta Otorhinolaryngol. Ital. 2013, 33, 261–266. [Google Scholar]
- De Vito, A.; Agnoletti, V.; Berrettini, S.; Piraccini, E.; Criscuolo, A.; Corso, R.; Campanini, A.; Gambale, G.; Vicini, C. Drug-induced sleep endoscopy: Conventional versus target controlled infusion techniques--a randomized controlled study. Eur. Arch. Otorhinolaryngol. 2011, 268, 457–462. [Google Scholar] [CrossRef]
- Hong, S.D.; Dhong, H.J.; Kim, H.Y.; Sohn, J.H.; Jung, Y.G.; Chung, S.K.; Park, J.Y.; Kim, J.K. Change of obstruction level during drug-induced sleep endoscopy according to sedation depth in obstructive sleep apnea. Laryngoscope 2013, 123, 2896–2899. [Google Scholar] [CrossRef]
- Nishizawa, T.; Suzuki, H.; Hosoe, N.; Ogata, H.; Kanai, T.; Yahagi, N. Dexmedetomidine vs propofol for gastrointestinal endoscopy: A meta-analysis. United Eur. Gastroenterol. J. 2017, 5, 1037–1045. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, C.; Cui, X.; Guo, Y.; Wang, Q.; Liang, H. The role of drug-induced sleep endoscopy: Predicting and guiding upper airway surgery for adult OSA patients. Sleep Breath. 2018, 22, 925–931. [Google Scholar] [CrossRef]
- Certal, V.F.; Pratas, R.; Guimaraes, L.; Lugo, R.; Tsou, Y.; Camacho, M.; Capasso, R. Awake examination versus DISE for surgical decision making in patients with OSA: A systematic review. Laryngoscope 2016, 126, 768–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Age (year) | BMI (kg/m2) | AHI | Number | Goal of Sedation | Intervention | Comparison | Sedation Technique |
|---|---|---|---|---|---|---|---|---|
| Cho 2015 [24] | Pro = 41.7 ± 12.8 Dex = 40.8 ± 11.8 | Pro = 25.4 ± 3.7 Dex = 25.9 + 3.5 | Pro = 40.1 ± 26.0 Dex = 48.0 ± 20.1 | 42 | OAA/S score of 3–5 or BIS of 55–75 | Pro/Remi | Dex/Remi | Target-controlled infusion |
| Elkalla 2019 [23] | Pro = 38.6 ± 8.3 Dex = 39.4 ± 7.7 | Pro = 27.3 ± 2 Dex = 26.9 ± 2.1 | Pro = 32.2 ± 10.8 Dex = 30.7 ± 12 | 40 | RSS ≥ 3 | Pro | Dex | Infusion |
| Padiyara 2020 [22] | Pro = 40.7 ± 11.2 Dex = 40.6 ± 12.9 | Pro = 30.1 ± 4.0 Dex = 29.2 ± 3.3 | Pro = 55.9 ± 25.0 Dex = 48.6 ± 28.0 | 60 | Beginning of snoring and BIS = 70 | Pro | Dex | Infusion |
| Zhao 2018 [20] | Pro = 43.2 ± 6.6 Dex = 42.5 ± 6.0 | Pro = 28.9 ± 3.1 Dex = 28.0 ± 3.5 | Pro = 54.3 ± 20.4 Dex = 56.3 ± 21.5 | 88 | Disappearance of eyelash reflex | Pro | Dex | Bolus and infusion |
| Kuyrukluyıldız 2015 [21] | Pro = 43.3 ± 10.6 Dex = 47.4 ± 11.6 | Pro = 28.9 ± 3.9 Dex = 29.5 ± 4.1 | NA | 40 | BIS < 75 and RSS = 4 | Pro | Dex | Infusion |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-T.; Sun, C.-K.; Wu, K.-Y.; Chang, Y.-J.; Chiang, M.-H.; Chen, I.-W.; Liao, S.-W.; Hung, K.-C. The Use of Propofol versus Dexmedetomidine for Patients Receiving Drug-Induced Sleep Endoscopy: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 1585. https://doi.org/10.3390/jcm10081585
Chen Y-T, Sun C-K, Wu K-Y, Chang Y-J, Chiang M-H, Chen I-W, Liao S-W, Hung K-C. The Use of Propofol versus Dexmedetomidine for Patients Receiving Drug-Induced Sleep Endoscopy: A Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2021; 10(8):1585. https://doi.org/10.3390/jcm10081585
Chicago/Turabian StyleChen, Yi-Ting, Cheuk-Kwan Sun, Kuan-Yu Wu, Ying-Jen Chang, Min-Hsien Chiang, I-Wen Chen, Shu-Wei Liao, and Kuo-Chuan Hung. 2021. "The Use of Propofol versus Dexmedetomidine for Patients Receiving Drug-Induced Sleep Endoscopy: A Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 10, no. 8: 1585. https://doi.org/10.3390/jcm10081585