
Skin Manifestation of SARS-CoV-2: The Italian Experience

 ,
,  , , and
, , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
COVID-19 and Skin
2. Materials and Methods
3. Results
4. Discussion
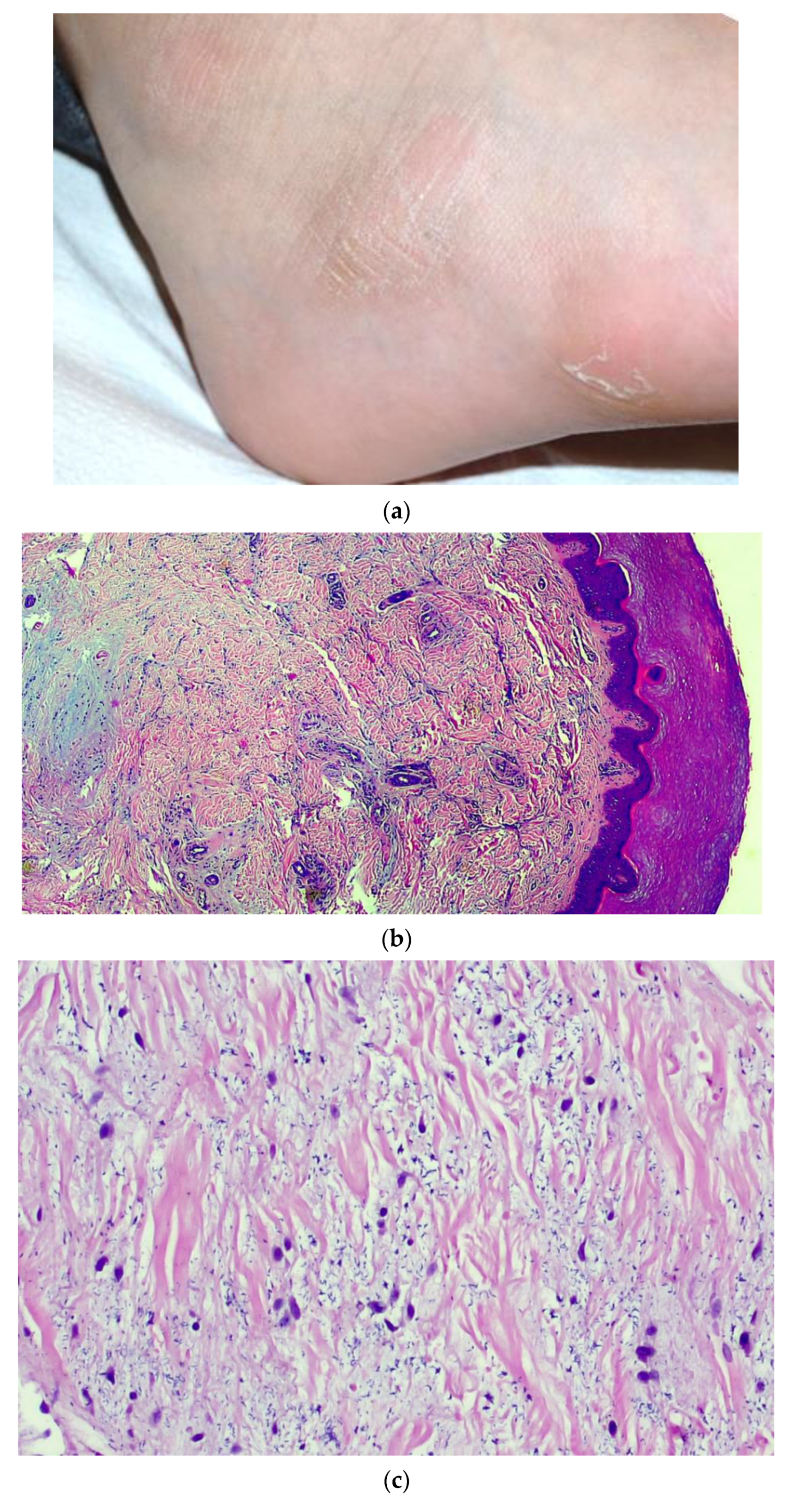
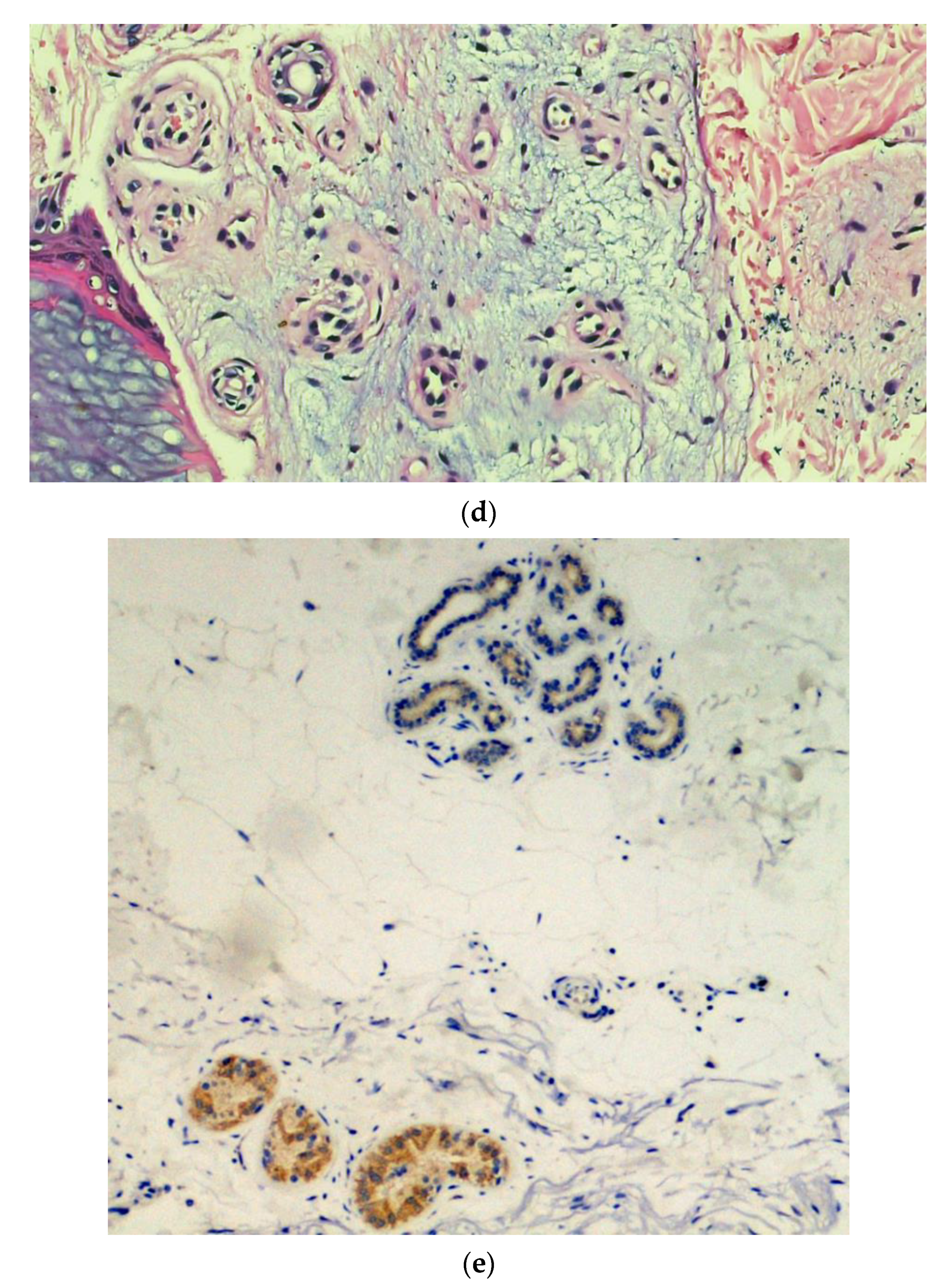
4.1. Chilblain-Like Lesions on Fingers and Toes
4.2. Acro-Ischemic Lesions
4.3. Rash with Petechiae and Purpuric Rash
4.4. Chickenpox-Like Rash
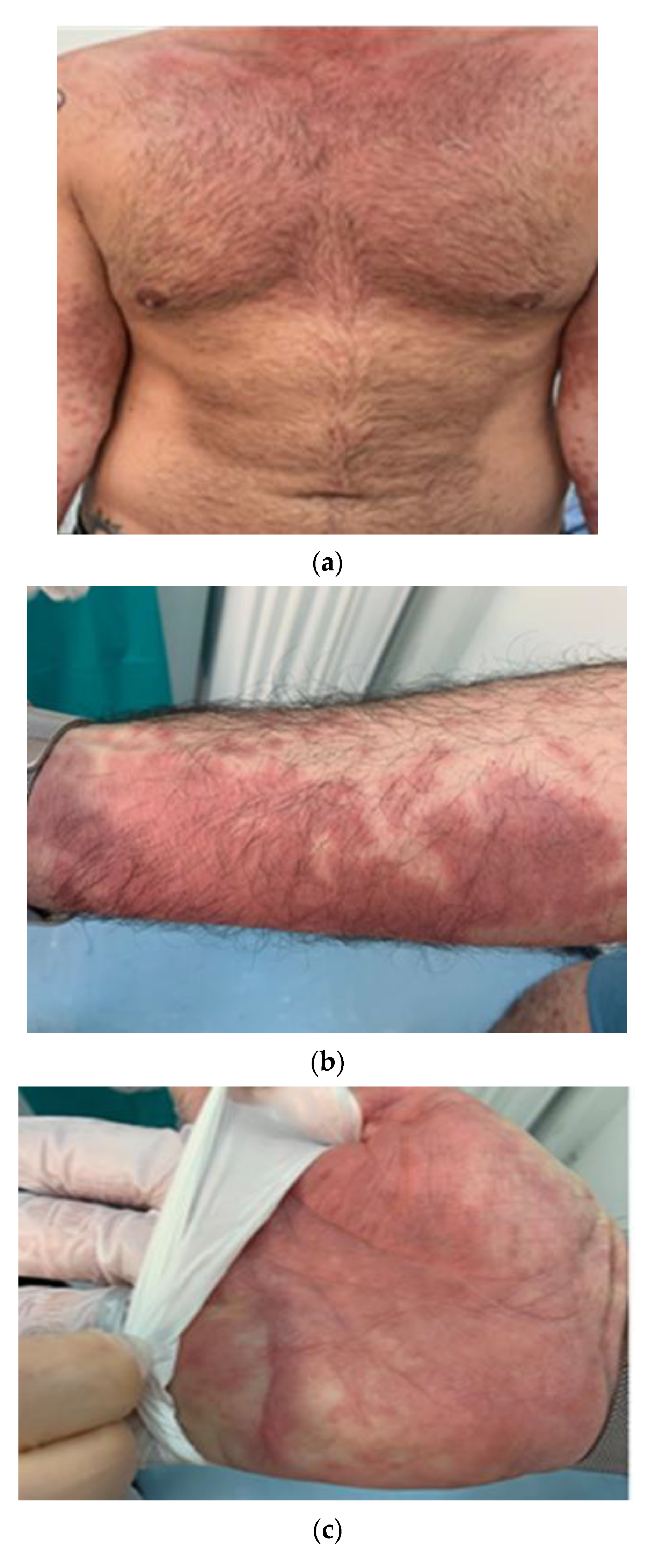
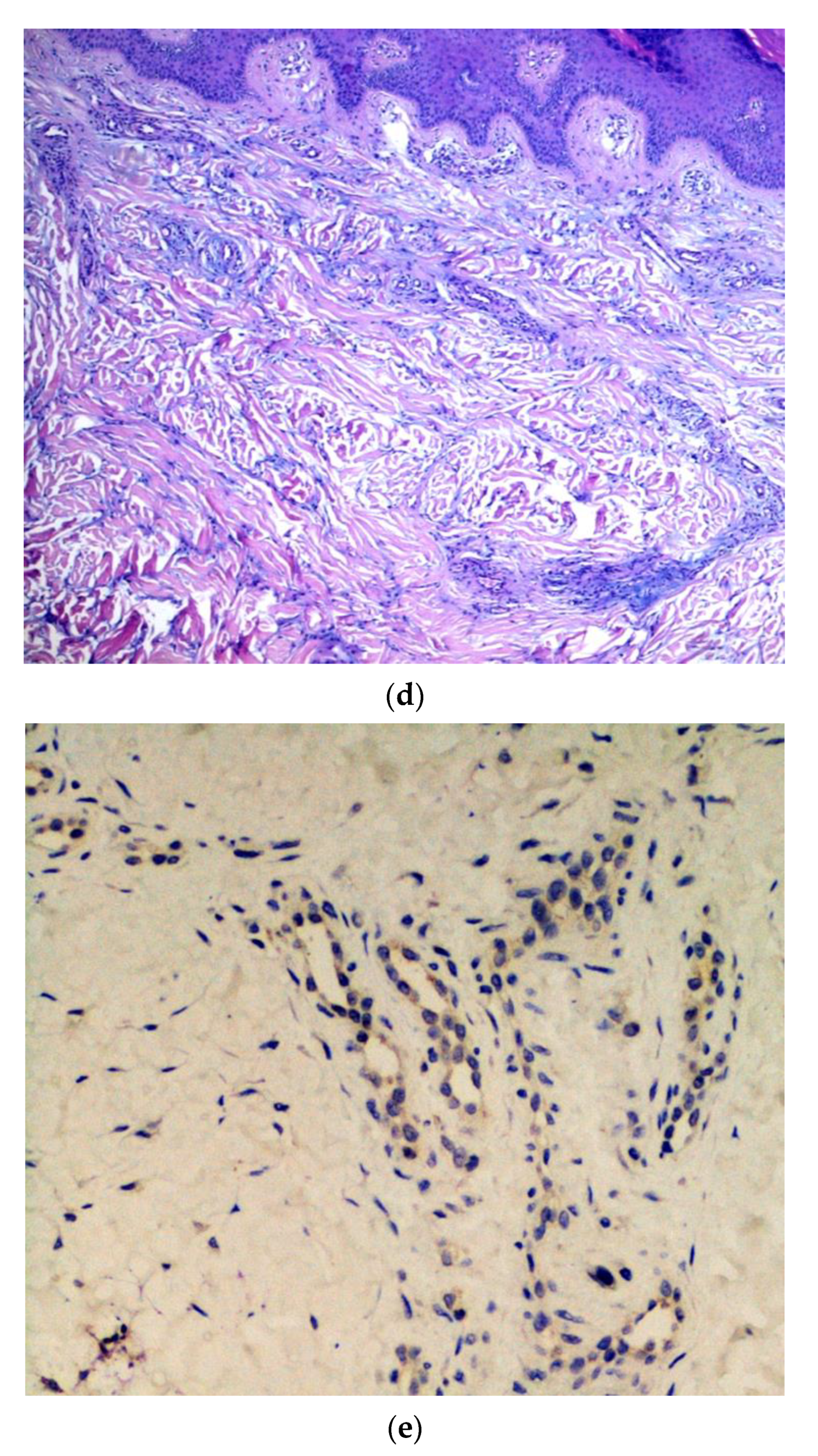
4.5. Urticarial and Erythema Multiforme-Like Rash
4.6. Maculopapular Rash
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| WHO | World Health Organization |
| COVID-19 | Coronavirus Disease-19 |
| PCR | Polymerase Chain Reaction |
| ACE2 | Angiotensin conversion enzyme 2 receptor |
| ARDS | Acute Respiratory Distress Syndrome |
| RT-PCR | Reverse transcription-polymerase chain reaction |
| H&E | Hematoxylin and eosin |
| IHC | Immunohistochemistry |
| AGEP | Acute generalized exanthematous pustolosis |
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Yang, H. The transmission and diagnosis of 2019 novel coronavirus infection disease (COVID-19): A Chinese perspective. J. Med. Virol. 2020, 92, 639–644. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Coronavirus Disease (COVID-19)—Events as They Happen. Rolling Updates on Coronavirus Disease (COVID-19). 2020. Available online: https://coronavirus.jhu.edu (accessed on 7 February 2021).
- Johns Hopkins Corona Resource Center. Available online: https://coronavirus.jhu.edu (accessed on 7 February 2021).
- WHO Coronavirus Diseases. Available online: https://covid19.who.int/region/euro/country/it (accessed on 7 February 2021).
- Zhai, P.; Ding, Y.; Wu, X.; Long, J.; Zhong, Y.; Li, Y. The epidemiology, diagnosis and treatment of COVID-19. Int. J. Antimicrob. Agents 2020, 55, 105955. [Google Scholar] [CrossRef]
- Klejtman, T. Skin and COVID-19. JMV J. Méd. Vasc. 2020, 45, 175–176. [Google Scholar] [CrossRef]
- Kaur, A.; Bhalla, V.; Salahuddin, M.; Rahman, S.O.; Pottoo, F.H. COVID-19 infection: Epidemiology, Virology, Clinical Features, Diagnosis and Pharmacological Treatment. Curr. Pharm. Des. 2021. [Google Scholar] [CrossRef]
- Ksiazek, T.G.; Erdman, D.; Goldsmith, C.S.; Zaki, S.R.; Peret, T.; Emery, S.; Tong, S.; Urbani, C.; Comer, J.A.; Lim, W.; et al. A novel coronavirus associated with severe acute respiratory syndrome. N. Engl. J. Med. 2003, 348, 1953–1966. [Google Scholar] [CrossRef] [PubMed]
- Su, S.; Wong, G.; Shi, W.; Liu, J.; Lai, A.C.; Zhou, J.; Liu, W.; Bi, Y.; Gao, G.F. Epidemiology, genetic recombination, and pathogenesis of coronaviruses. Trends Microbiol. 2016, 24, 490–502. [Google Scholar] [CrossRef] [Green Version]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Recalcati, S. Cutaneous manifestations in COVID-19: A first perspective. J. Eur. Acad. Dermatol. Venereol. 2020, 34. [Google Scholar] [CrossRef] [PubMed]
- Mazzotta, F.; Troccoli, T.; Bonifazi, E. A new vasculitis at the time of COVID-19. Eur. J. Pediat. Dermatol. 2020, 30, 75–78. [Google Scholar]
- Mungmungpuntipantip, R.; Wiwanitkit, V. COVID-19 and cutaneous manifestations. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e246. [Google Scholar]
- Lei, Y.; Huang, X.; Bamu, S.; Lan, Y.; Lu, J.; Zeng, F. Clinical features of imported cases of coronavirus disease 2019 in Tibetan patients in the plateau area. Infect. Dis. Poverty 2020. [Google Scholar] [CrossRef] [Green Version]
- Gianotti, R.; Veraldi, S.; Recalcati, S.; Cusini, M.; Ghislanzoni, M.; Boggio, F.; Fox, L. Cutaneous clinico-pathological findings in three COVID-19-positive patients observed in the Metropolitan area of Milan, Italy. Acta Derm. Venereol. 2020, 100, adv00124. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, M.; Gianotti, R.; Shah, M.; Bradanini, L.; Tosi, D.; Veraldi, S.; Ziv, M.; Leshem, E.; Dodiuk-Gad, R.P. Cutaneous manifestations of COVID-19: Report of three cases and a review of literature. J. Dermatol. Sci. 2020, 98, 75–81. [Google Scholar] [CrossRef]
- Gianotti, R.; Zerbi, P.; Dodiuk-Gad, R.P. Clinical and histopathological study of skin dermatoses in patients affected by COVID-19 infection in the Northern part of Italy. J. Dermatol. Sci. 2020, 98, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Gianotti, R.; Barberis, M.; Fellegara, G.; Galván-Casas, C.; Gianotti, E. COVID-19-related dermatosis in November 2019: Could this case be Italy’s patient zero? Br. J. Dermatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Tosti, G.; Barisani, A.; Queirolo, P.; Pennacchioli, E.; Villa, L.; Lodeserto, A.M.; Vaccari, S. Skin signs resembling vascular acrosyndromes during the COVID-19 outbreak in Italy. Clin. Exp. Dermatol. 2020, 45, 757–758. [Google Scholar] [CrossRef] [PubMed]
- Colonna, C.; Monzani, N.A.; Rocchi, A.; Gianotti, R.; Boggio, F.; Gelmetti, C. Chilblain-like lesions in children following suspected COVID-19 infection. Pediatr. Dermatol. 2020, 37, 437–440. [Google Scholar] [CrossRef] [PubMed]
- Genovese, G.; Colonna, C.; Marzano, A.V. Varicella-like exanthem associated with COVID-19 in an 8-year-old girl: A diagnostic clue? Pediatr. Dermatol. 2020, 37, 435–436. [Google Scholar] [CrossRef]
- El Hachem, M.; Diociaiuti, A.; Concato, C.; Carsetti, R.; Carnevale, C.; Ciofi Degli Atti, M.; Giovannelli, L.; Latella, E.; Porzio, O.; Rossi, S.; et al. A clinical, histopathological and laboratory study of 19 consecutive Italian paediatric patients with chilblain-like lesions: Lights and shadows on the relationship with COVID-19 infection. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2620–2629. [Google Scholar] [CrossRef]
- Marzano, A.V.; Genovese, G.; Fabbrocini, G.; Pigatto, P.; Monfrecola, G.; Piraccini, B.M.; Veraldi, S.; Rubegni, P.; Cusini, M.; Caputo, V.; et al. Varicella-like exanthem as a specific COVID-19–associated skin manifestation: Multicenter case series of 22 patients. J. Am. Acad. Dermatol. 2020, 83, 280–285. [Google Scholar] [CrossRef]
- Diotallevi, F.; Campanati, A.; Bianchelli, T.; Bobyr, I.; Luchetti, M.M.; Marconi, B.; Martina, E.; Radi, G.; Offidani, A. Skin involvement in SARS-CoV-2 infection: Case series. J. Med. Virol. 2020, 92, 2332–2334. [Google Scholar] [CrossRef] [PubMed]
- Tammaro, A.; Adebanjo, G.A.R.; Parisella, F.R.; Pezzuto, A.; Rello, J. Cutaneous manifestations in COVID-19: The expe-riences of Barcelona and Rome. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e306–e307. [Google Scholar] [CrossRef]
- Tammaro, A.; Chello, C.; Sernicola, A.; Magri, F.; Adebanjo, G.A.R.; Parisella, F.R.; Scarabello, A.; Pezzuto, A.; Ramirez-Estrada, S.; Rello, J. Necrotic acral lesions and lung failure in a fatal case of COVID-19. Australas. J. Dermatol. 2020, 61. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, V.; Neri, I.; Filippeschi, C.; Oranges, T.; Argenziano, G.; Battarra, V.C.; Berti, S.; Manunza, F.; Fortina, A.B.; Di Lernia, V.; et al. Chilblain-like lesions during COVID-19 epidemic: A preliminary study on 63 patients. J. Eur. Acad. Dermatol. Venereol. 2020, 34. [Google Scholar] [CrossRef] [PubMed]
- Gianotti, R.; Recalcati, S.; Fantini, F.; Riva, C.; Milani, M.; Dainese, E.; Boggio, F. Histopathological study of a broad spectrum of skin dermatoses in patients affected or highly suspected of infection by COVID-19 in the Northern part of Italy: Analysis of the many faces of the viral-induced skin diseases in previous and new reported cases. Am. J. Dermatopathol. 2020, 42, 564–570. [Google Scholar] [CrossRef]
- Recalcati, S.; Barbagallo, T.; Frasin, L.; Prestinari, F.; Cogliardi, A.; Provero, M.; Dainese, E.; Vanzati, A.; Fantini, F. Acral cutaneous lesions in the time of COVID-19. J. Eur. Acad. Dermatol. Venereol. 2020, 34. [Google Scholar] [CrossRef] [PubMed]
- De Giorgi, V.; Recalcati, S.; Jia, Z.; Chong, W.; Ding, R.; Deng, Y.; Scarfi, F.; Venturi, F.; Trane, L.; Gori, A.; et al. Cutaneous manifestations related to coronavirus disease 2019 (COVID-19): A prospective study from China and Italy. J. Am. Acad. Dermatol. 2020, 83, 674–675. [Google Scholar] [CrossRef]
- Castelnovo, L.; Capelli, F.; Tamburello, A.; Faggioli, P.M.; Mazzone, A. Symmetric cutaneous vasculitis in COVID-19 pneumonia. J. Eur. Acad. Dermatol. Venereol. 2020, 34. [Google Scholar] [CrossRef]
- Locatelli, A.G.; Robustelli, E.; Vezzoli, P.; Carugno, A.; Moggio, E.; Consonni, L.; Gianatti, A.; Sena, P. Histologic features of long-lasting chilblain-like lesions in a paediatric COVID-19 patient. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e365–e368. [Google Scholar] [CrossRef]
- Colonna, C.; Genovese, G.; Monzani, N.A.; Picca, M.; Boggio, F.; Gianotti, R.; Marzano, A.V. Outbreak of chilblain-like acral lesions in children in the metropolitan area of Milan, Italy, during the COVID-19 pandemic. J. Am. Acad. Dermatol. 2020, 83, 965–969. [Google Scholar] [CrossRef] [PubMed]
- Maniaci, A.; Iannella, G.; Vicini, C.; Pavone, P.; Nunnari, G.; Falsaperla, R.; Di Mauro, P.; Ferlito, S.; Cocuzza, S. A case of COVID-19 with late-onset rash and transient loss of taste and smell in a 15-year-old boy. Am. J. Case Rep. 2020, 21, e925813. [Google Scholar] [CrossRef] [PubMed]
- Freeman, E.E.; McMahon, D.E.; Lipoff, J.B.; Rosenbach, M.; Kovarik, C.; Desai, S.R.; Harp, J.; Takeshita, J.; French, L.E.; Lim, H.W.; et al. The spectrum of COVID-19-associated dermatologic manifestations: An international registry of 716 patients from 31 countries. J. Am. Acad. Dermatol. 2020, 83, 1118–1129. [Google Scholar] [CrossRef] [PubMed]
- Brazzelli, V.; Vassallo, C.; Barruscotti, S.; Giorgini, C.; Michelerio, A.; Pizzulli, M.; Veronesi, R.; Vecchia, M.; Bruno, R.; Tomasini, C.F. Late-onset cutaneous eruption in hospitalized COVID-19 patients. Eur. J. Dermatol. 2020, 30, 621–622. [Google Scholar] [CrossRef] [PubMed]
- Guarneri, C.; Rullo, E.V.; Gallizzi, R.; Ceccarelli, M.; Cannavò, S.; Nunnari, G. Diversity of clinical appearance of cutaneous manifestations in the course of COVID-19. J. Eur. Acad. Dermatol. Venereol. 2020, 34. [Google Scholar] [CrossRef] [PubMed]
- Gaspari, V.; Neri, I.; Misciali, C.; Patrizi, A. COVID-19: How it can look on the skin. Clinical and pathological features in 20 COVID-19 patients observed in Bologna, north-eastern Italy. J. Eur. Acad. Dermatol. Venereol. 2020, 34. [Google Scholar] [CrossRef] [PubMed]
- Di Nunno, D.; Laghi, A.; Troiani, G.; Marseglia, B.; Anelli, L.; Farina, E.; Tarricone, F.; Mammana, G.; Catalano, C.; Bonito, A.; et al. Cutaneous manifestations in an Italian military COVID hub. G. Ital. Dermatol. Venereol. 2020, 155, 632–635. [Google Scholar] [CrossRef] [PubMed]
- Caputo, V.; Schroeder, J.; Rongioletti, F. A generalized purpuric eruption with histopathologic features of leucocytoclastic vasculitis in a patient severely ill with COVID-19. J. Eur. Acad. Dermatol. Venereol. 2020, 34. [Google Scholar] [CrossRef]
- Balestri, R.; Termine, S.; Rech, G.; Girardelli, C.R. Late onset of acral necrosis after SARS-CoV-2 infection resolution. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e448–e449. [Google Scholar] [CrossRef] [PubMed]
- Rossi, E.; Lasagni, C.; Trakatelli, M.; Rowan, S.W.; Magnoni, C. Acute maculopapular eruption in Covid-19 patient: A case report. Dermatol. Ther. 2020, 33, e13812. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Guadagno, A.; Greco, M.; Parodi, A.; Burlando, M. An unusual case of bullous haemorrhagic vasculitis in a COVID-19 patient. J. Eur. Acad. Dermatol. Venereol. 2020, 34. [Google Scholar] [CrossRef] [PubMed]
- Carugno, A.; Gambini, D.M.; Raponi, F.; Vezzoli, P.; Test, E.R.; Arosio, M.E.; Callegaro, A.; Sena, P. Coronavirus disease 2019 (COVID-19) rash in a psoriatic patient treated with Secukinumab: Is there a role for Interleukin 17? Dermatol. Ther. 2020, 33, e14011. [Google Scholar] [CrossRef]
- Proietti, I.; Tolino, E.; Bernardini, N.; Mambrin, A.; Balduzzi, V.; Marchesiello, A.; Michelini, S.; Del Borgo, C.; Skroza, N.; Lichtner, M.; et al. Auricle perniosis as a manifestation of Covid-19 infection. Dermatol. Ther. 2020, 33. [Google Scholar] [CrossRef] [PubMed]
- Annunziata, M.C.; Patrì, A.; Ruggiero, A.; Di Guida, A.; Menicanti, C.; Greco, V.; Fabbrocini, G. Cutaneous involvement during COVID-19 pandemic: An emerging sign of infection. J. Eur. Acad. Dermatol. Venereol. 2020, 34. [Google Scholar] [CrossRef] [PubMed]
- Promenzio, L.; Arcangeli, F.; Cortis, E.; Sama, E.; Longhini, F. Erythema pernio-like in four adolescents in the era of the Coronavirus-2 infection. Rev. Recent Clin. Trials 2020, 15, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Quaglino, P.; Fava, P.; Cariti, C.; Ortoncelli, M.; Aimetti, M.; Milan, A.; Dapavo, P.; Tonella, L.; Ribero, S.; Fierro, M.T. Evolution of different clinical patterns of cutaneous lesions in a suspected COVID-19 patient. Eur. J. Dermatol. 2020, 30, 747–748. [Google Scholar] [CrossRef]
- Denina, M.; Pellegrino, F.; Morotti, F.; Coppo, P.; Bonsignori, I.M.; Garazzino, S.; Ravanini, P.; Avolio, M.; Cavallo, R.; Bertolotti, L.; et al. All that glisters is not COVID: Low prevalence of seroconversion against SARS-CoV-2 in a pediatric cohort of patients with chilblain-like lesions. J. Am. Acad. Dermatol. 2020, 83, 1751–1753. [Google Scholar] [CrossRef] [PubMed]
- Montinari, M.; Atzori, L.; Valdevit, S.; Rongioletti, F. Erythema annulare centrifugum with anosmia and ageusia in a SARS-CoV-2 exposed patient successfully treated with doxycycline. Int. J. Dermatol. 2021, 60, 384–386. [Google Scholar] [CrossRef]
- Pezzarossa, E.; Ungari, M.; Caresana, G.; Sagradi, F.; Cimardi, L.; Pan, A.; Testa, S.; Aguggini, S.; Varotti, E.; Tanzi, G.; et al. Acute Generalized Exanthematous Pustulosis (AGEP) in 12 patients treated for SARS-CoV-2 positive pneumonia. Am. J. Dermatopathol. 2021. [Google Scholar] [CrossRef]
- Patrì, A.; Vargas, M.; Buonanno, P.; Annunziata, M.C.; Russo, D.; Staibano, S.; Servillo, G.; Fabbrocini, G. From SARS-CoV-2 hematogenous spreading to endothelial dysfunction: Clinical-histopathological study of cutaneous signs of COVID-19. Diagn. Pathol. 2021, 16, 16. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Magri, F.; Michelini, S.; Sernicola, A.; Muscianese, M.; Caro, G.; Di Fraia, M.; Chello, C.; Fortuna, M.C.; Grieco, T. New onset of alopecia areata in a patient with SARS-COV-2 infection: Possible pathogenetic correlations? J. Cosmet. Dermatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Mastrolonardo, M.; Romita, P.; Bonifazi, E.; Giuffrida, R.; Lotti, T.; Foti, C.; Bonamonte, D. The management of the out-break of acral skin manifestations in asymptomatic children during COVID-19 era. Dermatol. Ther. 2020, 33, e13617. [Google Scholar] [CrossRef] [PubMed]
- Naldi, L. The skin as a target for SARS-CoV-2 infection: Exploiting the web for suitable data. Br. J. Dermatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Proietti, I.; Mambrin, A.; Bernardini, N.; Tolino, E.; Balduzzi, V.; Maddalena, P.; Marchesiello, A.; Michelini, S.; Volpe, S.; Skroza, N.; et al. Urticaria in an infant with SARS-CoV-2 positivity. Dermatol. Ther. 2020, 33, e14043. [Google Scholar] [CrossRef] [PubMed]
- Wollina, U.; Karadağ, A.S.; Rowland-Payne, C.; Chiriac, A.; Lotti, T. Cutaneous signs in COVID-19 patients: A review. Dermatol. Ther. 2020, 33. [Google Scholar] [CrossRef] [PubMed]
- Casas, C.G.; Català, A.; Hernández, G.C.; Rodríguez-Jiménez, P.; Fernández-Nieto, D.; Lario, A.R.; Fernández, I.N.; Ruiz-Villaverde, R.; Falkenhain-López, D.; Velasco, M.L.; et al. Classification of the cutaneous manifestations of COVID-19: A rapid prospective nationwide consensus study in Spain with 375 cases. Br. J. Dermatol. 2020, 183, 71–77. [Google Scholar] [CrossRef]
- Palma, G.; Pasqua, T.; Silvestri, G.; Rocca, C.; Gualtieri, P.; Barbieri, A.; De Bartolo, A.; De Lorenzo, A.; Angelone, T.; Avolio, E.; et al. PI3Kδ Inhibition as a Potential Therapeutic Target in COVID-19. Front. Immunol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cazzato, G.; Foti, C.; Colagrande, A.; Cimmino, A.; Scarcella, S.; Cicco, G.; Sablone, S.; Arezzo, F.; Romita, P.; Lettini, T.; et al. Skin Manifestation of SARS-CoV-2: The Italian Experience. J. Clin. Med. 2021, 10, 1566. https://doi.org/10.3390/jcm10081566
Cazzato G, Foti C, Colagrande A, Cimmino A, Scarcella S, Cicco G, Sablone S, Arezzo F, Romita P, Lettini T, et al. Skin Manifestation of SARS-CoV-2: The Italian Experience. Journal of Clinical Medicine. 2021; 10(8):1566. https://doi.org/10.3390/jcm10081566
Chicago/Turabian StyleCazzato, Gerardo, Caterina Foti, Anna Colagrande, Antonietta Cimmino, Sara Scarcella, Gerolamo Cicco, Sara Sablone, Francesca Arezzo, Paolo Romita, Teresa Lettini, and et al. 2021. "Skin Manifestation of SARS-CoV-2: The Italian Experience" Journal of Clinical Medicine 10, no. 8: 1566. https://doi.org/10.3390/jcm10081566