
MCP-1 Predicts Recurrent Cardiovascular Events in Patients with Persistent Inflammation

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Biomarkers and Primary Outcome
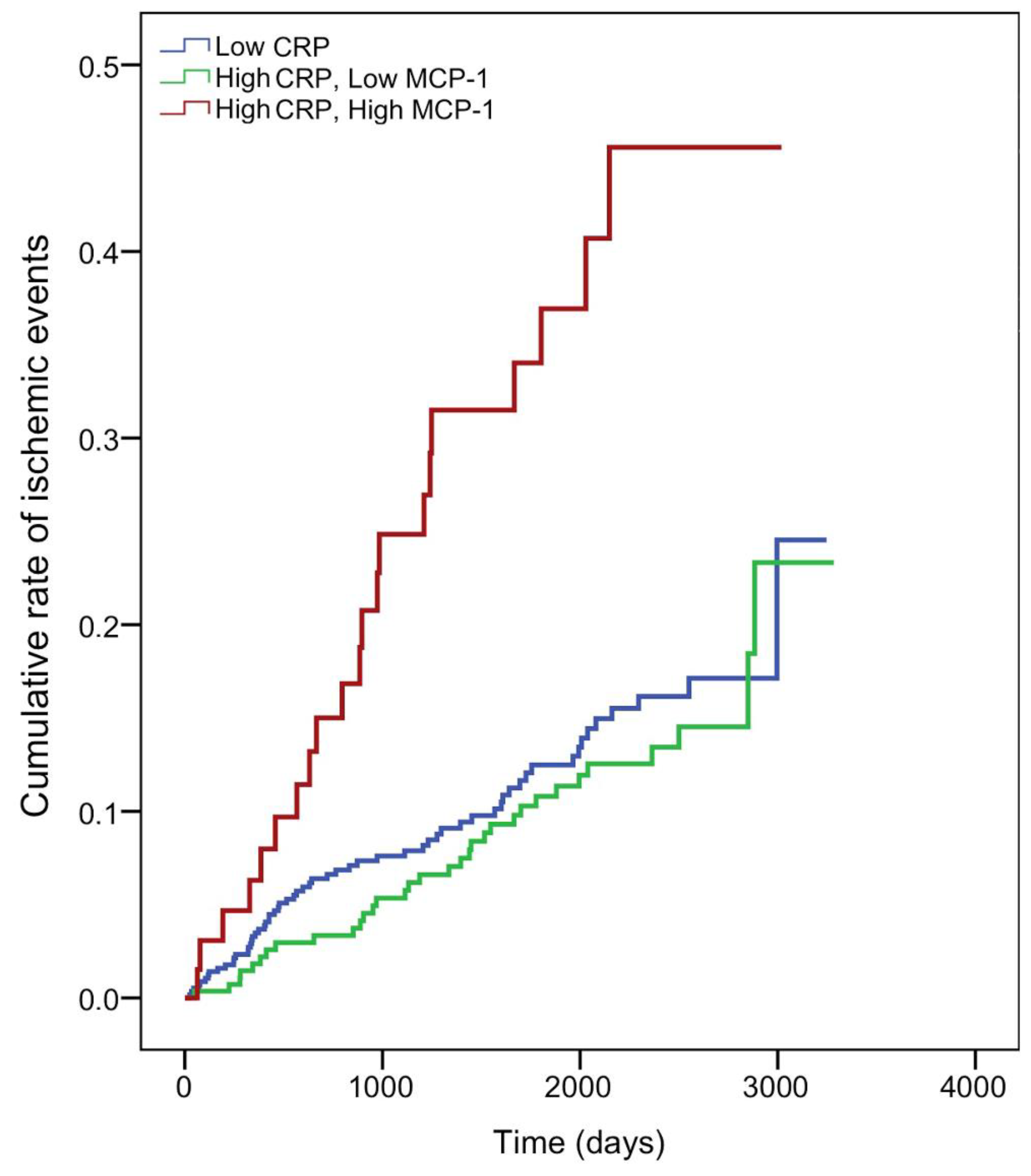
2.2. MCP-1 and Acute Ischemic Events
2.3. NT-proBNP and HF or Death
3. Discussion
4. Patients and Methods
4.1. Patients
4.2. Ethics Statement
4.3. Study Design
4.4. Biomarker and Analytical Studies
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hansson, G.K. Inflammation, atherosclerosis, and coronary artery disease. N. Engl. J. Med. 2005, 352, 1685–1695. [Google Scholar] [CrossRef] [Green Version]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Leducq transatlantic network on atherothrombosis inflammation in atheroscle-rosis: From pathophysiology to practice. J. Am. Coll. Cardiol. 2009, 54, 2129–2138. [Google Scholar] [CrossRef] [Green Version]
- Libby, P.; Hansson, G.K. Inflammation and immunity in diseases of the arterial tree: Players and layers. Circ. Res. 2015, 116, 307–311. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Koike, T.; Ichikawa, T.; Hatakeyama, K.; Shiomi, M.; Zhang, B.; Kitajima, S.; Morimoto, M.; Watanabe, T.; Asada, Y. C-reactive protein in atherosclerotic lesions: Its origin and pathophysiological significance. Am. J. Pathol. 2005, 167, 1139–1148. [Google Scholar] [CrossRef]
- Volanakis, J.E. Human C-reactive protein: Expression, structure, and function. Mol. Immunol. 2001, 38, 189–197. [Google Scholar] [CrossRef]
- Ridker, P.M.; Cushman, M.; Stampfer, M.J.; Tracy, R.P.; Hennekens, C.H. Inflammation, aspirin, and the risk of cardio-vascular disease in apparently healthy men. N. Engl. J. Med. 1997, 336, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Hennekens, C.H.; Buring, J.E.; Rifai, N. C-reactive protein and other markers of inflammation in the predic-tion of cardiovascular disease in women. N. Engl. J. Med. 2000, 342, 836–843. [Google Scholar] [CrossRef] [PubMed]
- Koenig, W.; Sund, M.; Fröhlich, M.; Fischer, H.G.; Löwel, H.; Döring, A.; Hutchinson, W.L.; Pepys, M.B. C-Reactive protein, a sensitive marker of inflammation, predicts future risk of coronary heart disease in initially healthy middle-aged men: Results from the MONICA (Monitoring Trends and Determinants in Cardiovascular Disease) Augsburg Cohort Study 1984 to 1992. Circulation 1999, 99, 237–242. [Google Scholar] [PubMed] [Green Version]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O.; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Centers for disease control and prevention, american heart association. markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar]
- McMurray, J.J.; Kjekshus, J.; Gullestad, L.; Dunselman, P.; Hjalmarson, A.; Wedel, H.; Lindberg, M.; Waagstein, F.; Grande, P.; Hradec, J.; et al. Effects of statin therapy according to plasma high-sensitivity C-reactive protein concentration in the Controlled Rosuvastatin Multinational Trial in Heart Failure (CORONA): A retrospective analysis. Circulation 2009, 120, 2188–2196. [Google Scholar] [CrossRef]
- Tuñón, J.; Blanco-Colio, L.M.; Cristóbal, C.; Tarín, N.; Higueras, J.; Huelmos, A.; Alonso, J.J.; Egido, J.; Asensio, D.; Lorenzo, Ó.; et al. Usefulness of a combination of monocyte chemoattractant protein-1, galectin-3, and N-terminal probrain natriuretic peptide to predict cardiovascular events in patients with coronary artery disease. Am. J. Cardiol. 2014, 113, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Bianconi, V.; Sahebkar, A.; Atkin, S.L.; Pirro, M. The regulation and importance of monocyte chemoattractant protein-1. Curr. Opin. Hematol. 2018, 25, 44–51. [Google Scholar] [CrossRef]
- Gao, Z.; Liu, Z.; Wang, R.; Zheng, Y.; Li, H.; Yang, L. Galectin-3 is a potential mediator for atherosclerosis. J. Immunol. Res. 2020, 2020, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelken, N.A.; Coughlin, S.R.; Gordon, D.; Wilcox, J.N. Monocyte chemoattractant protein-1 in human atheromatous plaques. J. Clin. Investig. 1991, 88, 1121–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikeda, U.; Matsui, K.; Murakami, Y.; Shimada, K. Monocyte chemoattractant protein-1 and coronary artery disease. Clin. Cardiol. 2002, 25, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Namiki, M.; Kawashima, S.; Yamashita, T.; Ozaki, M.; Hirase, T.; Ishida, T.; Inoue, N.; Hirata, K.-I.; Matsukawa, A.; Mor-ishita, R.; et al. Local overexpression of monocyte chemoattractant protein-1 at vessel wall induces infiltration of macrophages and formation of atherosclerotic lesion: Synergism with hypercholesterolemia. Arterioscler. Thromb. Vasc. Biol. 2020, 22, 115–120. [Google Scholar] [CrossRef] [Green Version]
- Yla-Herttuala, S.; Lipton, B.A.; Rosenfeld, M.E.; Sarkioja, T.; Yoshimura, T.; Leonard, E.J.; Witztum, J.L.; Steinberg, D. Expression of monocyte chemoattractant protein 1 in macrophage-rich areas of human and rabbit atherosclerotic lesions. Proc. Natl. Acad. Sci. USA 1991, 88, 5252–5256. [Google Scholar] [CrossRef] [Green Version]
- Zhong, L.; Chen, W.Q.; Ji, X.P.; Zhang, M.; Zhao, Y.X.; Yao, G.H.; Zhang, P.F.; Zhang, C.; Zhang, Y. Dominant-negative mutation of monocyte chemoattractant protein-1 prevents vulnerable plaques from rupture in rabbits independent of serum lipid levels. J. Cell. Mol. Med. 2008, 12, 2362–2371. [Google Scholar] [CrossRef] [Green Version]
- Gosling, J.; Slaymaker, S.; Gu, L.; Tseng, S.; Zlot, C.H.; Young, S.G.; Rollins, B.J.; Charo, I.F. MCP-1 deficiency reduces susceptibility to atherosclerosis in mice that overexpress human apolipoprotein B. J. Clin. Investig. 1999, 103, 773–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, L.; Okada, Y.; Clinton, S.K.; Gerard, C.; Sukhova, G.K.; Libby, P.; Rollins, B.J. Absence of monocyte chemoattractant protein-1 reduces atherosclerosis in low density lipoprotein receptor–deficient mice. Mol. Cell 1998, 2, 275–281. [Google Scholar] [CrossRef]
- Boring, L.; Gosling, J.; Cleary, M.; Charo, I.F. Decreased lesion formation in CCR2−/− mice reveals a role for chemokines in the initiation of atherosclerosis. Nature 1998, 394, 894–897. [Google Scholar] [CrossRef] [PubMed]
- Deo, R.; Khera, A.; McGuire, D.K.; Murphy, S.A.; Neto, J.D.P.M.; Morrow, D.A.; De Lemos, J.A. Association among plasma levels of monocyte chemoattractant protein-1, traditional cardiovascular risk factors, and subclinical atherosclerosis. J. Am. Coll. Cardiol. 2004, 44, 1812–1818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herder, C.; Baumert, J.; Thorand, B.; Martin, S.; Löwel, H.; Kolb, H.; Koenig, W. Chemokines and incident coronary heart disease: Results from the MONICA/KORA Augsburg case-cohort study, 1984–2002. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2147–2152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoogeveen, R.C.; Morrison, A.; Boerwinkle, E.; Miles, J.S.; Rhodes, C.E.; Sharrett, A.R.; Ballantyne, C.M. Plasma MCP-1 level and risk for peripheral arterial disease and incident coronary heart disease: Atherosclerosis Risk in Communities study. Atherosclerosis 2005, 183, 301–307. [Google Scholar] [CrossRef] [PubMed]
- De Lemos, J.A.; Morrow, D.A.; Sabatine, M.S.; Murphy, S.A.; Gibson, C.M.; Antman, E.M.; McCabe, C.H.; Cannon, C.P.; Braunwald, E. Association between plasma levels of monocyte chemoattractant protein-1 and long-term clinical outcomes in patients with acute coronary syndromes. Circulation 2003, 107, 690–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Lemos, J.A.; Morrow, D.A.; Blazing, M.A.; Jarolim, P.; Wiviott, S.D.; Sabatine, M.S.; Califf, R.M.; Braunwald, E. Serial measurement of monocyte chemoattractant protein-1 after acute coronary syndromes: Results from the A to Z trial. J. Am. Coll. Cardiol 2007, 50, 2117–2124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]
- Nidorf, S.M.; Eikelboom, J.W.; Budgeon, C.A.; Thompson, P.L. Low-dose colchicine for secondary prevention of cardio-vascular disease. J. Am. Coll. Cardiol. 2013, 61, 404–410. [Google Scholar] [CrossRef] [Green Version]
- Nidorf, S.M.; Fiolet, A.T.L.; Mosterd, A.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.J.; The, S.H.K.; Xu, X.-F.; Ireland, M.A.; Lenderink, T.; et al. Colchicine in patients with chronic coronary disease. N. Engl. J. Med. 2020, 383, 1838–1847. [Google Scholar] [CrossRef]
- Yamashita, T.; Kawashima, S.; Ozaki, M.; Namiki, M.; Inoue, N.; Hirata, K.-I.; Yokoyama, M. Propagermanium reduces atherosclerosis in apolipoprotein E knockout mice via inhibition of macrophage infiltration. Arter. Thromb. Vasc. Biol. 2002, 22, 969–974. [Google Scholar] [CrossRef]
- Masuda, T.; Noda, M.; Kogawa, T.; Kitagawa, D.; Hayashi, N.; Jomori, T.; Nakanishi, Y.; Nakayama, K.I.; Ohno, S.; Mimori, K.; et al. Phase I dose-escalation trial to repurpose propagermanium, an oral CCL2 inhibitor, in patients with breast cancer. Cancer Sci. 2020, 111, 924–931. [Google Scholar] [CrossRef] [Green Version]
- Raghu, G.; Martinez, F.J.; Brown, K.K.; Costabel, U.; Cottin, V.; Wells, A.U.; Lancaster, L.; Gibson, K.F.; Haddad, T.; Agarwal, P.; et al. CC-chemokine ligand 2 inhibition in idi-opathic pulmonary fibrosis: A phase 2 trial of carlumab. Eur. Respir. J. 2015, 46, 1740–1750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, J.; Lekstrom-Himes, J.; Donaldson, D.; Lee, Y.; Hu, M.; Xu, J.; Wyant, T.; Davidson, M. Effect of CC chemokine receptor 2 CCR2 blockade on serum C-reactive protein in individuals at atherosclerotic risk and with a single nucleotide polymorphism of the monocyte chemoattractant protein-1 promoter region. Am. J. Cardiol. 2011, 107, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Goetze, J.P.; Bruneau, B.G.; Ramos, H.R.; Ogawa, T.; De Bold, M.K.; De Bold, A.J. Cardiac natriuretic peptides. Nat. Rev. Cardiol. 2020, 17, 698–717. [Google Scholar] [CrossRef]
- Lorenzo-Almorós, A.; Pello, A.; Aceña, Á.; Martínez-Milla, J.; González-Lorenzo, Ó.; Tarín, N.; Cristóbal, C.; Blanco-Colio, L.M.; Martín-Ventura, J.L.; Huelmos, A.; et al. Galectin-3 is associated with cardiovascular events in post-acute coronary syndrome patients with type-2 diabetes. J. Clin. Med. 2020, 9, 1105. [Google Scholar] [CrossRef] [Green Version]
- Andersson, T.; Alfredsson, L.; Källberg, H.; Zdravkovic, S.; Ahlbom, A. Calculating measures of biological interaction. Eur. J. Epidemiol. 2005, 20, 575–579. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Patients with CRP < 2 mg/L (n = 574) | Patients with CRP ≥ 2 mg/L (n = 343) | p-Value |
| Age (year) | 60 (52–71) | 61 (51–72) | 0.686 |
| Male sex (%) | 76.3 | 74.9 | 0.637 |
| Body mass index (kg/m2) | 27.7 (25.1–30.2) | 28.7 (26.6–32.0) | <0.001 |
| Smoker (%) | 73.0 | 79.3 | 0.032 |
| Hypertension (%) | 61.0 | 68.2 | 0.027 |
| Diabetes (%) | 20.9 | 28.3 | 0.011 |
| Previous heart failure (%) | 9.6 | 15.2 | 0.011 |
| Cerebrovascular event (%) | 1.9 | 4.1 | 0.051 |
| Present or past atrial fibrillation (%) | 5.7 | 6.7 | 0.558 |
| Total Cholesterol (mg/dL) | 140 (121–158) | 154 (134–172) | <0.001 |
| LDL Cholesterol (mg/dL) | 75 (63–89) | 83 (68–99) | <0.001 |
| HDL Cholesterol (mg/dL) | 41 (35–48) | 41 (36–47) | 0.686 |
| Triglycerides (mg/dL) | 93 (72–125) | 120 (89–167) | <0.001 |
| Glucose (mg/dL) | 101 (91–112) | 100 (92–118) | 0.243 |
| GFR (CKD-EPI) (mL/min/1.73 m2) | 81 (68–94) | 77 (60–90) | <0.001 |
| High-sensitivity C-reactive protein (mg/L) | 0.5 (0.1–1.0) | 4.1 (2.8–7.3) | <0.001 |
| High-sensitivity troponin I (ng/L) | 3.0 (0.0–9.0) | 3.5 (0.0–12.0) | 0.152 |
| NT-ProBNP (ng/L) | 165 (87–350) | 188 (96–481) | 0.034 |
| MCP-1 (ng/L) | 129 (103–171) | 142 (111–180) | 0.006 |
| Galectin-3 (µg/L) | 7.8 (6.0–9.7) | 7.8 (5.8–10.0) | 0.942 |
| Medical Therapy | |||
| Acetylsalicylic acid (%) | 94.6 | 91.2 | 0.049 |
| AntiP2Y12 (%) | 78.9 | 67.6 | <0.001 |
| Acenocumarol (%) | 4.2 | 7.9 | 0.018 |
| Statins (%) | 95.5 | 93.0 | 0.111 |
| Oral antidiabetic drugs (%) | 13.6 | 21.3 | 0.002 |
| Insulin (%) | 5.4 | 7.9 | 0.137 |
| ACE inhibitors (%) | 64.0 | 55.7 | 0.013 |
| Angiotensin receptor blockers (%) | 14.8 | 18.1 | 0.192 |
| Aldosterone receptor blockers (%) | 7.3 | 4.4 | 0.074 |
| Betablockers (%) | 79.6 | 77.2 | 0.399 |
| Diuretics (%) | 15.8 | 23.3 | 0.005 |
| Nitrates (%) | 11.5 | 17.2 | 0.015 |
| Data at Last Acute Coronary Event | |||
| STEMI/Non-STEACS (%) | 53.0 | 42.0 | <0.001 |
| Number of vessels diseased | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 0.001 |
| Coronary artery bypass graft (%) | 5.6 | 11.1 | 0.002 |
| Complete revascularization (%) | 72.1 | 64.7 | 0.019 |
| CRP < 2 mg/L | ||
| Parameter | HR (95% CI) | p-Value |
| Age, years | 1.03 (1.00–1.05) | 0.028 |
| Diabetes, yes | 1.32 (0.65–2.66) | 0.445 |
| Hypertension, yes | 1.64 (0.91–2.96) | 0.098 |
| History of CVE, yes | 2.51 (0.97–6.45) | 0.057 |
| Ejection fraction < 40%, yes | 1.00 (0.49–2.06) | 0.997 |
| CKD-EPI < 60 mL/min/1.73 m2 | 1.04 (0.59–1.82) | 0.906 |
| Statins, yes | 0.43 (0.20–0.89) | 0.023 |
| ACE inhibitors, yes | 0.77 (0.45–1.34) | 0.364 |
| ARB, yes | 1.75 (0.93–3.29) | 0.238 |
| Antialdosterone, yes | 1.58 (0.74–3.39) | 0.238 |
| β-Blockers, yes | 0.54 (0.34–0.84) | 0.007 |
| Nitrates, yes | 1.39 (0.83–2.31) | 0.207 |
| Diuretics, yes | 0.81 (0.46–1.41) | 0.456 |
| Insulin, yes | 1.40 (0.64–3.08) | 0.401 |
| Oral antidiabetic drugs, yes | 1.34 (0.62–2.92) | 0.458 |
| NT-proBNP, 1-SD | 1.14 (0.96–1.35) | 0.144 |
| MCP-1, 1-SD | 1.07 (0.88–1.28) | 0.493 |
| Tn-I, 1-SD | 1.05 (0.70–1.58) | 0.815 |
| CRP ≥ 2 mg/L | ||
| Parameter | HR (95% CI) | p-Value |
| Age, years | 1.02 (1.00–1.04) | 0.073 |
| Sex, male | 0.80 (0.48–1.32) | 0.381 |
| Hypertension, yes | 0.93 (0.52–1.65) | 0.803 |
| Ejection fraction < 40%, yes | 1.60 (0.88–2.92) | 0.126 |
| Atrial Fibrillation, yes | 2.36 (1.04–5.33) | 0.039 |
| Acute myocardial infarction, yes | 0.58 (0.34–0.99) | 0.046 |
| Complete Revascularization | 0.59 (0.36–0.95) | 0.029 |
| LDL-c, mg/dL | 1.01 (1.00–1.01) | 0.091 |
| HDL-c, mg/dL | 1.02 (1.00–1.04) | 0.081 |
| Anticoagulants, yes | 0.77 (0.34–1.74) | 0.531 |
| Statins, yes | 0.44 (0.23–0.86) | 0.016 |
| Nitrates, yes | 1.64 (0.93–2.90) | 0.085 |
| Diuretics, yes | 1.04 (0.62–1.77) | 0.874 |
| Insulin, yes | 2.14 (1.07–4.28) | 0.031 |
| NT-proBNP, 1-SD | 1.22 (1.06–1.41) | 0.007 |
| MCP-1, 1-SD | 1.26 (1.02–1.56) | 0.032 |
| Gal-3, 1-SD | 1.16 (0.93–1.46) | 0.192 |
| Tn-I, 1-SD | 1.18 (0.95–1.32) | 0.136 |
| Parameter | HR (95% CI) | p-Value |
|---|---|---|
| Complete Revascularization | 0.62 (0.43–0.91) | 0.014 |
| LDL-c, mg/dL | 1.01 (1.00–1.01) | 0.022 |
| Statins, yes | 0.45 (0.25–0.79) | 0.006 |
| Insulin, yes | 2.32 (1.35–3.99) | 0.002 |
| CRP < 2 mg/L | 1.00 | |
| CRP ≥ 2 mg/L, MCP-1 ≤ 188 ng/L | 0.79 (0.52–1.21) | 0.280 |
| CRP ≥ 2 mg/L, MCP-1 > 188 ng/L | 2.08 (1.25–3.47) | 0.005 |
| CRP < 2 mg/L | ||
| Parameter | HR (95% CI) | p-Value |
| Age, years | 1.08 (1.04–1.12) | <0.001 |
| Body mass index, kg/m2 | 0.97 (0.89–1.06) | 0.498 |
| Diabetes, yes | 2.89 (1.01–8.28) | 0.048 |
| Hypertension, yes | 1.61 (0.53–4.93) | 0.402 |
| History of CVE, yes | 0.97 (0.19–4.95) | 0.969 |
| Ejection fraction < 40%, yes | 1.06 (0.41–2.74) | 0.906 |
| LDL-c, mg/dL | 0.98 (0.97–1.00) | 0.034 |
| CKD-EPI < 60 mL/min/1.73 m2 | 0.99 (0.44–2.25) | 0.906 |
| Anticoagulants, yes | 1.60 (0.44–5.87) | 0.475 |
| Statins, yes | 0.46 (0.14–1.50) | 0.200 |
| Antialdosterone, yes | 3.01 (1.12–8.08) | 0.029 |
| β-Blockers, yes | 0.40 (0.20–0.80) | 0.009 |
| Nitrates, yes | 1.08 (0.50–2.36) | 0.837 |
| Diuretics, yes | 1.27 (0.56–2.86) | 0.563 |
| Insulin, yes | 1.33 (0.42–4.20) | 0.630 |
| Oral antidiabetic drugs, yes | 1.00 (0.32–3.11) | 0.997 |
| NT-proBNP, 1-SD | 1.27 (1.03–1.57) | 0.024 |
| MCP-1, 1-SD | 1.13 (0.85–1.49) | 0.140 |
| Tn-I, 1-SD | 1.33 (0.91–1.95) | 0.140 |
| CRP ≥ 2 mg/L | ||
| Parameter | HR (95% CI) | p-Value |
| Age, years | 1.07 (1.03–1.10) | <0.001 |
| Sex, male | 0.99 (0.49–2.02) | 0.980 |
| Hypertension, yes | 0.82 (0.36–1.88) | 0.644 |
| History of CVE, yes | 2.11 (0.43–10.3) | 0.358 |
| Ejection fraction < 40%, yes | 2.60 (1.22–5.51) | 0.012 |
| Atrial Fibrillation, yes | 3.61 (1.28–10.1) | 0.015 |
| Complete Revascularization | 0.76 (0.39–1.47) | 0.413 |
| HDL-c, mg/dL | 1.05 (1.02–1.08) | 0.001 |
| CKD-EPI < 60 mL/min/1.73 m2 | 0.70 (0.35–1.41) | 0.319 |
| Anticoagulants, yes | 0.56 (0.20–1.59) | 0.279 |
| Statins, yes | 0.44 (0.17–1.16) | 0.096 |
| Antialdosterone, yes | 0.55 (0.13–2.32) | 0.414 |
| Nitrates, yes | 1.98 (0.89–4.43) | 0.094 |
| Diuretics, yes | 1.11 (0.55–2.28) | 0.765 |
| Insulin, yes | 3.22 (1.28–8.13) | 0.013 |
| NT-proBNP, 1-SD | 1.39 (1.16–1.66) | <0.001 |
| MCP-1, 1-SD | 1.01 (0.74–1.38) | 0.931 |
| Gal-3, 1-SD | 1.50 (0.93–3.08) | 0.094 |
| Tn-I, 1-SD | 1.26 (0.90–1.43) | 0.234 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanco-Colio, L.M.; Méndez-Barbero, N.; Pello Lázaro, A.M.; Aceña, Á.; Tarín, N.; Cristóbal, C.; Martínez-Milla, J.; González-Lorenzo, Ó.; Martín-Ventura, J.L.; Huelmos, A.; et al. MCP-1 Predicts Recurrent Cardiovascular Events in Patients with Persistent Inflammation. J. Clin. Med. 2021, 10, 1137. https://doi.org/10.3390/jcm10051137
Blanco-Colio LM, Méndez-Barbero N, Pello Lázaro AM, Aceña Á, Tarín N, Cristóbal C, Martínez-Milla J, González-Lorenzo Ó, Martín-Ventura JL, Huelmos A, et al. MCP-1 Predicts Recurrent Cardiovascular Events in Patients with Persistent Inflammation. Journal of Clinical Medicine. 2021; 10(5):1137. https://doi.org/10.3390/jcm10051137
Chicago/Turabian StyleBlanco-Colio, Luis M., Nerea Méndez-Barbero, Ana María Pello Lázaro, Álvaro Aceña, Nieves Tarín, Carmen Cristóbal, Juan Martínez-Milla, Óscar González-Lorenzo, José Luis Martín-Ventura, Ana Huelmos, and et al. 2021. "MCP-1 Predicts Recurrent Cardiovascular Events in Patients with Persistent Inflammation" Journal of Clinical Medicine 10, no. 5: 1137. https://doi.org/10.3390/jcm10051137