
Speckle Tracking Analysis Reveals Altered Left Atrial and Ventricular Myocardial Deformation in Patients with End-Stage Liver Disease

 , and
, and
Abstract
:1. Introduction
1.1. Cirrhotic Cardiomyopathy
1.2. Speckle Tracking Echocardiography
1.3. Aim
2. Methodology
2.1. Patients and Control Group
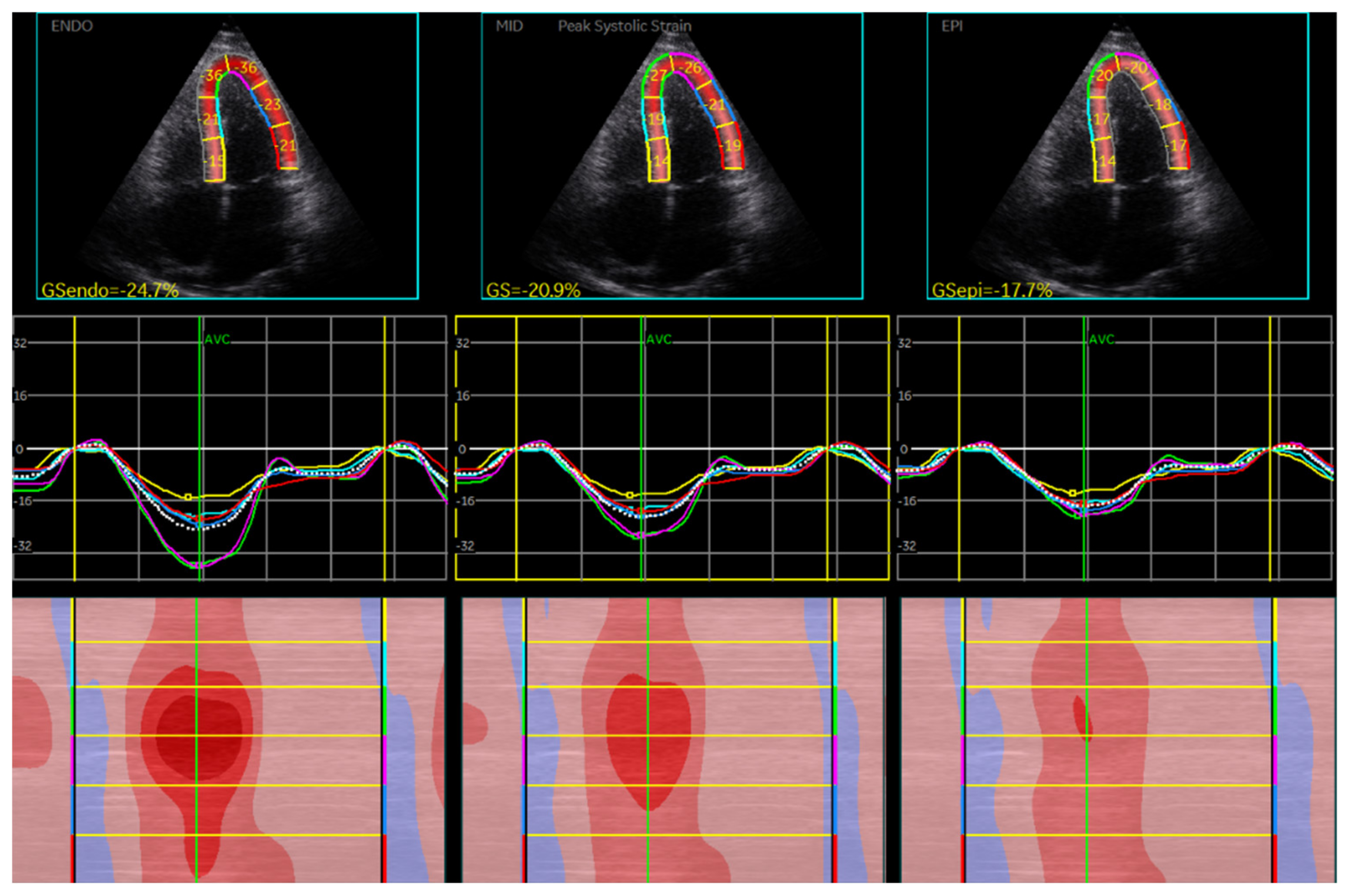
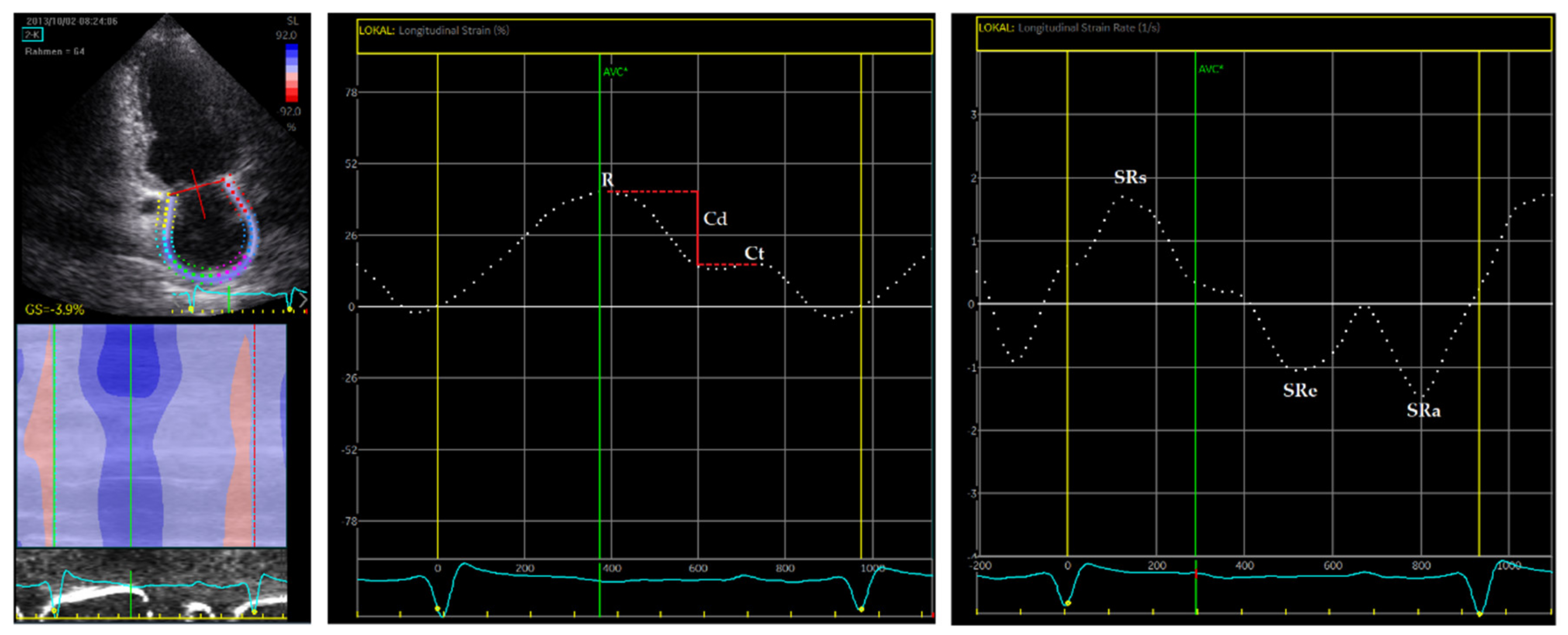
2.2. Echocardiography and STE
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
3.2. Echocardiography and Strain Measurements of the Left Ventricle
3.3. Echocardiography and Strain Measurements of the Left Atrium
3.4. Prevalence of CCM in Study Cohort
3.5. Correlation Analysis in ESLD Patients
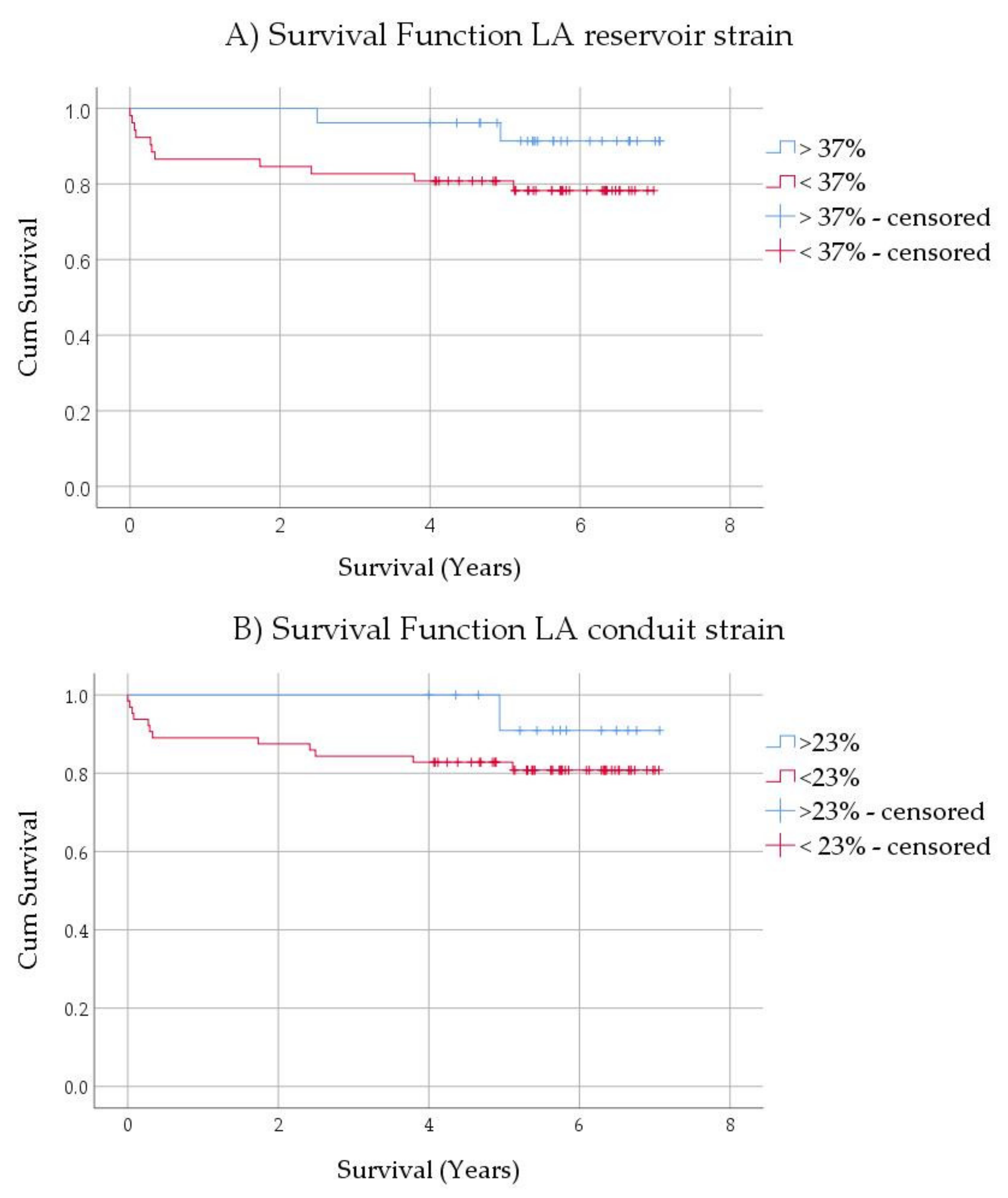
3.6. Mortality Analysis in ESLD Patients
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Izzy, M.; VanWagner, L.B.; Lin, G.; Altieri, M.; Findlay, J.Y.; Oh, J.K.; Watt, K.D.; Lee, S.S.; Cirrhotic Cardiomyopathy Consortium. Redefining Cirrhotic Cardiomyopathy for the Modern Era. Hepatology 2020, 71, 334–345. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, M.V.H.; Kroll, P.C.; Kroll, R.T.M.; Carvalho, V.N. Cirrhotic cardiomyopathy: The liver affects the heart. Braz. J. Med. Biol. Res. 2019, 52, e7809. [Google Scholar] [CrossRef]
- Farr, M.; Schulze, P.C. Recent advances in the diagnosis and management of cirrhosis-associated cardiomyopathy in liver transplant candidates: Advanced echo imaging, cardiac biomarkers, and advanced heart failure therapies. Clin. Med. Insights Cardiol. 2014, 8, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Jayakumar, S.; Traboulsi, M.; Lee, S.S. Cirrhotic cardiomyopathy: Implications for liver transplantation. Liver Transpl. 2017, 23, 826–835. [Google Scholar] [CrossRef] [Green Version]
- Dimitroglou, Y.; Aggeli, C.; Alexopoulou, A.; Mavrogeni, S.; Tousoulis, D. Cardiac Imaging in Liver Transplantation Candidates: Current Knowledge and Future Perspectives. J. Clin. Med. 2019, 8, 2132. [Google Scholar] [CrossRef] [Green Version]
- Karki, N.; Kc, S.; Sharma, D.; Jaisi, B.; Khadka, S. Cardiac Dysfunction in Patients with Liver Cirrhosis. J. Nepal Health Res. Counc. 2019, 17, 357–361. [Google Scholar] [CrossRef]
- Naqvi, I.H.; Mahmood, K.; Naeem, M.; Vashwani, A.S.; Ziaullah, S. The heart matters when the liver shatters! Cirrhotic cardiomyopathy: Frequency, comparison, and correlation with severity of disease. Prz. Gastroenterol. 2016, 11, 247–256. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-del-Arbol, L.; Serradilla, R. Cirrhotic cardiomyopathy. World J. Gastroenterol. 2015, 21, 11502–11521. [Google Scholar] [CrossRef]
- Bansal, M.; Kasliwal, R.R. How do I do it? Speckle-tracking echocardiography. Indian Heart J. 2013, 65, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correction. Hepatology 2020, 72, 1161. [CrossRef]
- Gan, G.C.H.; Ferkh, A.; Boyd, A.; Thomas, L. Left atrial function: Evaluation by strain analysis. Cardiovasc. Diagn. Ther. 2018, 8, 29–46. [Google Scholar] [CrossRef] [Green Version]
- Pathan, F.; D’Elia, N.; Nolan, M.T.; Marwick, T.H.; Negishi, K. Normal Ranges of Left Atrial Strain by Speckle-Tracking Echocardiography: A Systematic Review and Meta-Analysis. J. Am. Soc. Echocardiogr. 2017, 30, 59–70.e58. [Google Scholar] [CrossRef]
- Morris, D.A.; Belyavskiy, E.; Aravind-Kumar, R.; Kropf, M.; Frydas, A.; Braunauer, K.; Marquez, E.; Krisper, M.; Lindhorst, R.; Osmanoglou, E.; et al. Potential Usefulness and Clinical Relevance of Adding Left Atrial Strain to Left Atrial Volume Index in the Detection of Left Ventricular Diastolic Dysfunction. JACC Cardiovasc. Imaging 2018, 11, 1405–1415. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.A.; Gailani, M.; Vaz Perez, A.; Blaschke, F.; Dietz, R.; Haverkamp, W.; Ozcelik, C. Left atrial systolic and diastolic dysfunction in heart failure with normal left ventricular ejection fraction. J. Am. Soc. Echocardiogr. 2011, 24, 651–662. [Google Scholar] [CrossRef]
- To, A.C.; Flamm, S.D.; Marwick, T.H.; Klein, A.L. Clinical utility of multimodality LA imaging: Assessment of size, function, and structure. JACC Cardiovasc. Imaging 2011, 4, 788–798. [Google Scholar] [CrossRef] [Green Version]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Chan, A.C.; Chan, S.C.; Chok, S.H.; Sharr, W.; Fung, J.; Liu, J.H.; Zhen, Z.; Sin, W.C.; Lo, C.M.; et al. A detailed evaluation of cardiac function in cirrhotic patients and its alteration with or without liver transplantation. J. Cardiol. 2016, 67, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Jansen, C.; Cox, A.; Schueler, R.; Schneider, M.; Lehmann, J.; Praktiknjo, M.; Pohlmann, A.; Chang, J.; Manekeller, S.; Nickenig, G.; et al. Increased myocardial contractility identifies patients with decompensated cirrhosis requiring liver transplantation. Liver Transpl. 2018, 24, 15–25. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.M.; Kim, H.K.; Lee, J.H.; Lee, Y.B.; Park, E.A.; Park, J.B.; Lee, S.P.; Kim, Y.J.; Kim, Y.J.; Yoon, J.H.; et al. Myocardial structural and functional changes in patients with liver cirrhosis awaiting liver transplantation: A comprehensive cardiovascular magnetic resonance and echocardiographic study. J. Cardiovasc. Magn. Reson. 2020, 22, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mechelinck, M.; Hartmann, B.; Hamada, S.; Becker, M.; Andert, A.; Ulmer, T.F.; Neumann, U.P.; Wirtz, T.H.; Koch, A.; Trautwein, C.; et al. Global Longitudinal Strain at Rest as an Independent Predictor of Mortality in Liver Transplant Candidates: A Retrospective Clinical Study. J. Clin. Med. 2020, 9, 2616. [Google Scholar] [CrossRef]
- Bolognesi, M.; Di Pascoli, M.; Verardo, A.; Gatta, A. Splanchnic vasodilation and hyperdynamic circulatory syndrome in cirrhosis. World J. Gastroenterol. 2014, 20, 2555–2563. [Google Scholar] [CrossRef] [PubMed]
- Zardi, E.M.; Abbate, A.; Zardi, D.M.; Dobrina, A.; Margiotta, D.; Van Tassell, B.W.; Afeltra, A.; Sanyal, A.J. Cirrhotic cardiomyopathy. J. Am. Coll. Cardiol. 2010, 56, 539–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagourelias, E.D.; Sotiriou, P.; Papadopoulos, C.E.; Cholongitas, E.; Giouleme, O.; Vassilikos, V. Left Ventricular Myocardial Mechanics in Cirrhosis: A Speckle Tracking Echocardiographic Study. Echocardiography 2016, 33, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Nasr, F.M.; Metwaly, A.; Khalik, A.A.; Darwish, H. Cardiac dysfunction in liver cirrhosis: A tissue Doppler imaging study from Egypt. Electron. Physician 2015, 7, 1135–1143. [Google Scholar] [CrossRef]
- Cesari, M.; Fasolato, S.; Rosi, S.; Angeli, P. Cardiac dysfunction in patients with cirrhosis: Is the systolic component its main feature? Eur. J. Gastroenterol. Hepatol. 2015, 27, 660–666. [Google Scholar] [CrossRef]
- Larsen, C.M.; Vanden Bussche, C.L.; Mankad, S. Principles of Measuring Chamber Size, Volume and Hemodynamic Assessment of the Heart. In Echocardiography; Nihoyannopoulos, P., Kisslo, J., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 111–128. [Google Scholar] [CrossRef]
- Bansal, M.; Sengupta, P.P.; Khandheria, B.K. Echocardiography in Heart Failure. In Echocardiography; Nihoyannopoulos, P., Kisslo, J., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 619–642. [Google Scholar] [CrossRef]
- Cameli, M.; Mandoli, G.E.; Loiacono, F.; Dini, F.L.; Henein, M.; Mondillo, S. Left atrial strain: A new parameter for assessment of left ventricular filling pressure. Heart Fail. Rev. 2016, 21, 65–76. [Google Scholar] [CrossRef]
- Vieira, M.J.; Teixeira, R.; Goncalves, L.; Gersh, B.J. Left atrial mechanics: Echocardiographic assessment and clinical implications. J. Am. Soc. Echocardiogr. 2014, 27, 463–478. [Google Scholar] [CrossRef]
- Mondillo, S.; Cameli, M.; Caputo, M.L.; Lisi, M.; Palmerini, E.; Padeletti, M.; Ballo, P. Early detection of left atrial strain abnormalities by speckle-tracking in hypertensive and diabetic patients with normal left atrial size. J. Am. Soc. Echocardiogr. 2011, 24, 898–908. [Google Scholar] [CrossRef]
- Morris, D.A.; Takeuchi, M.; Krisper, M.; Kohncke, C.; Bekfani, T.; Carstensen, T.; Hassfeld, S.; Dorenkamp, M.; Otani, K.; Takigiku, K.; et al. Normal values and clinical relevance of left atrial myocardial function analysed by speckle-tracking echocardiography: Multicentre study. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 364–372. [Google Scholar] [CrossRef] [Green Version]
- Hiebert, J.B.; Vacek, J.; Shah, Z.; Rahman, F.; Pierce, J.D. Use of speckle tracking to assess heart failure with preserved ejection fraction. J. Cardiol. 2019, 74, 397–402. [Google Scholar] [CrossRef] [Green Version]
- Sampaio, F.; Pimenta, J.; Bettencourt, N.; Fontes-Carvalho, R.; Silva, A.P.; Valente, J.; Bettencourt, P.; Fraga, J.; Gama, V. Left atrial function is impaired in cirrhosis: A speckle tracking echocardiographic study. Hepatol. Int. 2014, 8, 146–153. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | n | Controls | n | ESLD Patients | Statistics p | ||||
|---|---|---|---|---|---|---|---|---|---|
| Gender (Male %) | 30 | 46.70 | 80 | 58.80 | 0.258 | ||||
| Age (years) | 30 | 48.57 | ± | 12.93 | 80 | 52.47 | ± | 10.24 | 0.145 |
| BMI (kg/m2) | 30 | 24.43 | ± | 3.40 | 79 | 26.30 | ± | 5.11 | 0.067 |
| ALAT (U/L) | 30 | 23.63 | ± | 10.19 | 80 | 58.39 | ± | 48.49 | <0.001 |
| ASAT (U/L) | 30 | 27.73 | ± | 21.51 | 80 | 81.48 | ± | 73.86 | <0.001 |
| AP (U/L) | 29 | 66.34 | ± | 18.01 | 80 | 235.91 | ± | 376.25 | <0.001 |
| γGT (U/L) | 30 | 21.40 | ± | 11.80 | 80 | 159.75 | ± | 212.32 | <0.001 |
| Creatinine (mg/dL) | 30 | 1.02 | ± | 0.06 | 80 | 1.16 | ± | 0.33 | 0.028 |
| Bilirubin (mg/dL) | 29 | 1.02 | ± | 0.06 | 80 | 7.01 | ± | 8.64 | <0.001 |
| INR | 29 | 1.02 | ± | 0.04 | 80 | 1.55 | ± | 0.52 | <0.001 |
| MELD Score | 29 | 7 | ± | 0.70 | 80 | 17 | ± | 6.65 | <0.001 |
| Variables | n | Controls | n | ESLD Patients | Statistics p | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Aorta sinus (mm) | 30 | 29.53 | ± | 3.60 | 78 | 30.56 | ± | 3.49 | 0.176 | |
| LVEDD (mm) | 30 | 44.80 | ± | 5.74 | 80 | 47.59 | ± | 6.63 | 0.045 | |
| LVESD (mm) | 30 | 34.20 | ± | 4.47 | 80 | 35.75 | ± | 9.22 | 0.416 | |
| IVS (mm) | 30 | 9.50 | ± | 1.59 | 80 | 11.12 | ± | 1.84 | <0.001 | |
| PW (mm) | 30 | 9.77 | ± | 1.52 | 80 | 11.05 | ± | 1.89 | 0.001 | |
| RWT | 30 | 0.44 | ± | 0.07 | 80 | 0.47 | ± | 0.10 | 0.121 | |
| LVM (g) | 30 | 149.27 | ± | 51.96 | 80 | 199.11 | ± | 62.34 | <0.001 | |
| LVMI (g/m2) | 30 | 79.87 | ± | 21.99 | 79 | 102.49 | ± | 28.50 | <0.001 | |
| LV Volumemax | 30 | 107.43 | ± | 31.03 | 80 | 118.50 | ± | 38.52 | 0.161 | |
| LV Volumemin | 30 | 59.20 | ± | 22.73 | 80 | 57.11 | ± | 20.24 | 0.642 | |
| E (m/sec) | 29 | 0.71 | ± | 0.16 | 75 | 0.80 | ± | 0.22 | 0.058 | |
| A (m/sec) | 29 | 0.59 | ± | 0.17 | 75 | 0.70 | ± | 0.23 | 0.035 | |
| E/A ratio | 29 | 1.25 | ± | 0.36 | 75 | 1.23 | ± | 0.41 | 0.828 | |
| DT (ms) | 29 | 214.10 | ± | 50.59 | 75 | 236.43 | ± | 56.92 | 0.068 | |
| e’ sept (m/sec) | 28 | 0.13 | ± | 0.20 | 75 | 0.08 | ± | 0.02 | 0.188 | |
| e’ lat (m/sec) | 28 | 0.10 | ± | 0.03 | 69 | 0.10 | ± | 0.02 | 0.984 | |
| E/e’ ratio | 28 | 7.57 | ± | 2.88 | 69 | 9.42 | ± | 2.88 | 0.005 | |
| TR (m/sec) | 16 | 2.41 | ± | 0.33 | 65 | 2.53 | ± | 0.38 | 0.232 | |
| LVEF (%) | 30 | 60.90 | ± | 4.70 | 79 | 60.00 | ± | 5.17 | 0.274 | |
| Strain Analysis (%) | ||||||||||
| GLS average | 30 | −18.73 | ± | 2.95 | 80 | −21.39 | ± | 4.06 | <0.001 | |
| GLS mid-myocardial | 30 | −18.56 | ± | 2.63 | 80 | −21.26 | ± | 4.05 | <0.001 | |
| GLS endocardial | 30 | −21.34 | ± | 3.00 | 80 | −24.16 | ± | 4.58 | <0.001 | |
| GLS epicardial | 30 | −16.28 | ± | 2.39 | 80 | −18.75 | ± | 3.62 | <0.001 | |
| GCS | 22 | −17.16 | ± | 5.06 | 55 | −19.85 | ± | 6.69 | 0.093 | |
| GRS | 22 | 30.77 | ± | 21.22 | 55 | 35.92 | ± | 18.79 | 0.298 | |
| Etiology | Average GLS | LA Reservoir Strain | ||||
|---|---|---|---|---|---|---|
| Idiopathic (n = 7) | −22.06 | ± | 4.16 | 40.91 | ± | 15.53 |
| Alcoholic (n = 25) | −20.91 | ± | 4.12 | 30.28 | ± | 10.03 |
| HCV (n = 10) | −22.44 | ± | 4.01 | 33.70 | ± | 9.15 |
| NASH (n = 8) | −20.05 | ± | 4.76 | 33.32 | ± | 12.82 |
| PSC (n = 7) | −20.85 | ± | 3.19 | 34.00 | ± | 11.10 |
| Autoimmune (n = 8) | −24.73 | ± | 4.66 | 33.95 | ± | 10.46 |
| Others (n = 15) | −20.35 | ± | 3.11 | 31.50 | ± | 8.49 |
| p | 0.143 | 0.748 | ||||
| Variables | n | Controls | n | ESLD Patients | Statistics p | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| LA Volumemax (mL) | 30 | 28.85 | ± | 17.21 | 80 | 75.13 | ± | 49.52 | <0.001 | |
| LA Volumepre-A (mL) | 22 | 16.65 | ± | 8.64 | 60 | 40.68 | ± | 28,90 | <0.001 | |
| LA Volumemin (mL) | 30 | 9.00 | ± | 6.11 | 80 | 21.27 | ± | 14.95 | <0.001 | |
| LAVImax (mL/m2) | 30 | 15.37 | ± | 8.65 | 79 | 38.73 | ± | 24.04 | <0.001 | |
| LAVIpre-A(mL/m2) | 22 | 8.90 | ± | 4.23 | 59 | 21.24 | ± | 15.04 | <0.001 | |
| LAVImin (mL/m2) | 30 | 4.83 | ± | 3.27 | 79 | 10.90 | ± | 7.11 | <0.001 | |
| LA TotEV (mL) | 30 | 19.85 | ± | 13.15 | 80 | 53.86 | ± | 38.48 | <0.001 | |
| LA PassEV (mL) | 22 | 9.96 | ± | 6.14 | 60 | 35.71 | ± | 32.13 | <0.001 | |
| LA ActEV (mL) | 22 | 8.45 | ± | 5.45 | 60 | 19.81 | ± | 18.61 | 0.001 | |
| LA TotEF (%) | 30 | 68 | ± | 17 | 80 | 71 | ± | 11 | 0.872 | |
| LA PassEF (%) | 22 | 39 | ± | 13 | 60 | 45 | ± | 16 | 0.052 | |
| LA ActEF (%) | 22 | 51 | ± | 18 | 60 | 48 | ± | 16 | 0.213 | |
| Strain Analysis (%) | ||||||||||
| Reservoir strain | 30 | 39.97 | ± | 9.74 | 80 | 32.86 | ± | 10.65 | 0.002 | |
| Conduit strain | 30 | 21.12 | ± | 7.40 | 80 | 15.38 | ± | 6.94 | <0.001 | |
| Contractile strain | 30 | 18.85 | ± | 5.08 | 80 | 17.48 | ± | 7.37 | 0.352 | |
| Strain Rate Analysis (1/s) | ||||||||||
| Reservoir SR | 30 | 1.66 | ± | 0.44 | 80 | 1.39 | ± | 0.40 | 0.003 | |
| Conduit SR | 30 | −1.92 | ± | 0.72 | 80 | −1.23 | ± | 0.47 | <0.001 | |
| Contractile SR | 30 | −2.43 | ± | 0.68 | 80 | −1.87 | ± | 0.64 | <0.001 | |
| Variables | r | |||||||
|---|---|---|---|---|---|---|---|---|
| ALAT (U/L) | ASAT (U/L) | AP (U/L) | γGT (U/L) | Creatinine (mg/dL) | Bilirubin | INR | MELD Score | |
| Left ventricle | ||||||||
| GLS average | −0.306 ** | −0.297 ** | 0.065 | 0.192 | −0.084 | −0.328 ** | −0.324 ** | −0.361 ** |
| GLS mid-myocardial | −0.304 ** | −0.294 ** | 0.071 | 0.190 | −0.090 | −0.325 ** | −0.325 ** | −0.360 ** |
| GLS endocardial | −0.302 ** | −0.300 ** | 0.080 | 0.198 | −0.063 | −0.313 ** | −0.338 ** | −0.346 ** |
| GLS epicardial | −0.306 ** | −0.296 ** | 0.037 | 0.173 | −0.114 | −0.349 ** | −0.293 ** | −0.379 ** |
| Left atrium | ||||||||
| R strain | 0.275 * | 0.301 ** | 0.079 | 0.018 | −0.271 * | 0.228 * | 0.162 | 0.111 |
| Ct strain | 0.223 * | 0.316 ** | 0.205 | 0.025 | −0.239 * | 0.228 * | 0.119 | 0.127 |
| Cd strain | 0.186 | 0.191 | −0.032 | −0.001 | −0.155 | 0.160 | 0.107 | 0.058 |
| SRs | 0.249 * | 0.234 * | 0.004 | −0.030 | −0.246 * | 0.198 | 0.179 | 0.144 |
| SRe | −0.273 * | −0.217 | −0.141 | −0.130 | 0.250 * | −0.272 * | −0.014 | −0.102 |
| SRa | −0.315 ** | −0.274 * | −0.024 | −0.121 | 0.288 ** | −0.105 | 0.055 | 0.068 |
| TotEV | 0.010 | −0.022 | −0.078 | −0.174 | 0.296 ** | 0.076 | 0.324 ** | 0.273 * |
| PassEV | −0.040 | −0.076 | −0.003 | −0.113 | 0.323 * | 0.085 | 0.227 | 0.227 |
| ActEV | −0.087 | −0.147 | −0.330 ** | −0.158 | 0.155 | −0.126 | 0.345 ** | 0.058 |
| TotEF | 0.282 * | 0.158 | 0.072 | −0.067 | −0.145 | 0.102 | −0.041 | 0.012 |
| PassEF | 0.209 | 0.195 | 0.317 * | 0.070 | 0.090 | 0.281 * | −0.038 | 0.226 |
| ActEF | 0.317 * | 0.156 | −0.094 | −0.088 | −0.233 | −0.029 | 0.111 | −0.046 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
von Köckritz, F.; Braun, A.; Schmuck, R.B.; Dobrindt, E.M.; Eurich, D.; Heinzel, F.R.; Pieske, B.; Escher, F.; Zhang, K. Speckle Tracking Analysis Reveals Altered Left Atrial and Ventricular Myocardial Deformation in Patients with End-Stage Liver Disease. J. Clin. Med. 2021, 10, 897. https://doi.org/10.3390/jcm10050897
von Köckritz F, Braun A, Schmuck RB, Dobrindt EM, Eurich D, Heinzel FR, Pieske B, Escher F, Zhang K. Speckle Tracking Analysis Reveals Altered Left Atrial and Ventricular Myocardial Deformation in Patients with End-Stage Liver Disease. Journal of Clinical Medicine. 2021; 10(5):897. https://doi.org/10.3390/jcm10050897
Chicago/Turabian Stylevon Köckritz, Franzisca, Alexander Braun, Rosa B. Schmuck, Eva M. Dobrindt, Dennis Eurich, Frank R. Heinzel, Burkert Pieske, Felicitas Escher, and Kun Zhang. 2021. "Speckle Tracking Analysis Reveals Altered Left Atrial and Ventricular Myocardial Deformation in Patients with End-Stage Liver Disease" Journal of Clinical Medicine 10, no. 5: 897. https://doi.org/10.3390/jcm10050897