
The Prevalence of Sarcopenia and Its Impact on Clinical Outcomes in Lumbar Degenerative Spine Disease—A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Study Quality Assessment
2.5. Statistical Analysis
3. Results
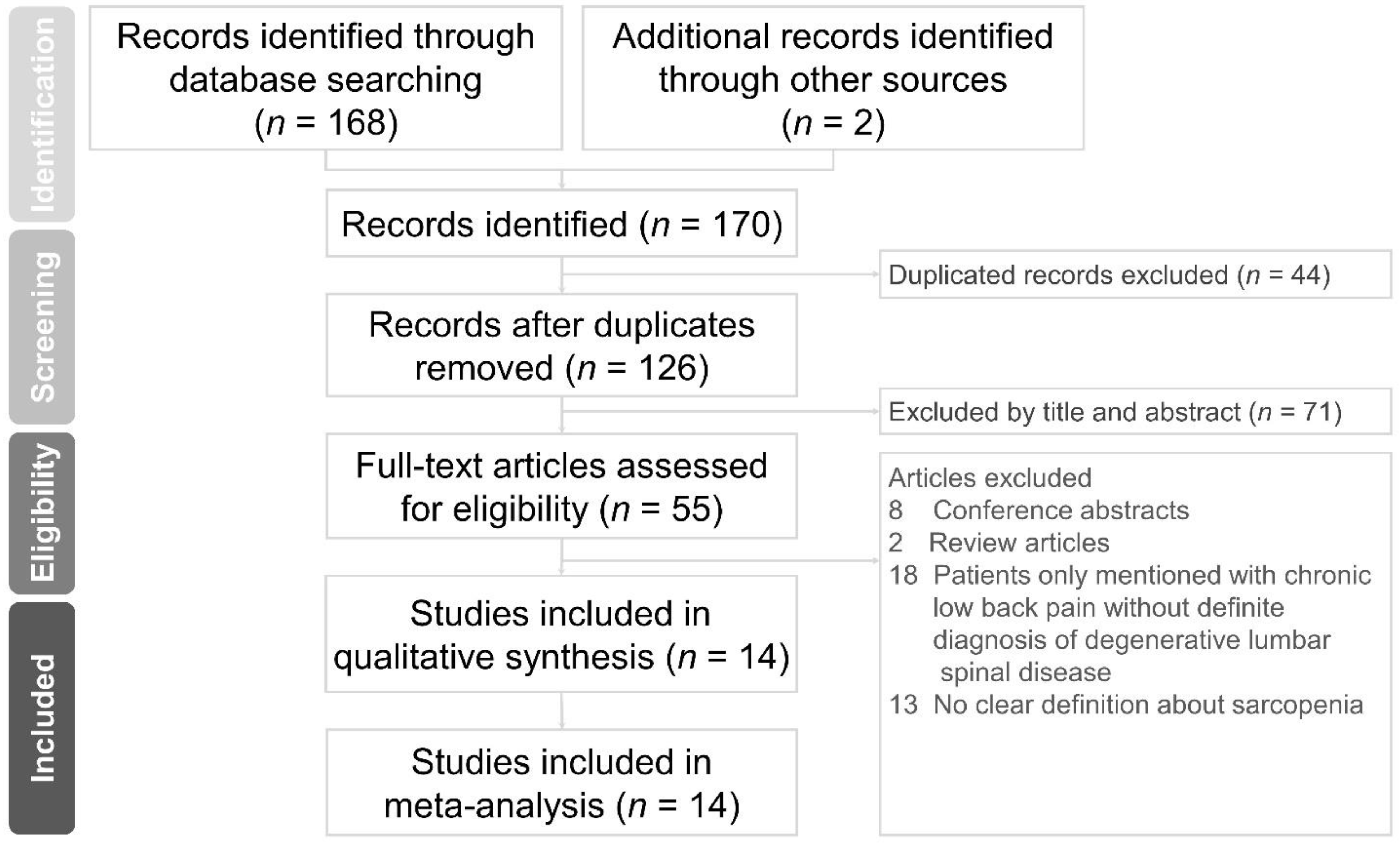
3.1. Literature Search
3.2. Study Characteristics
3.2.1. Quality Assessment of the Included Studies
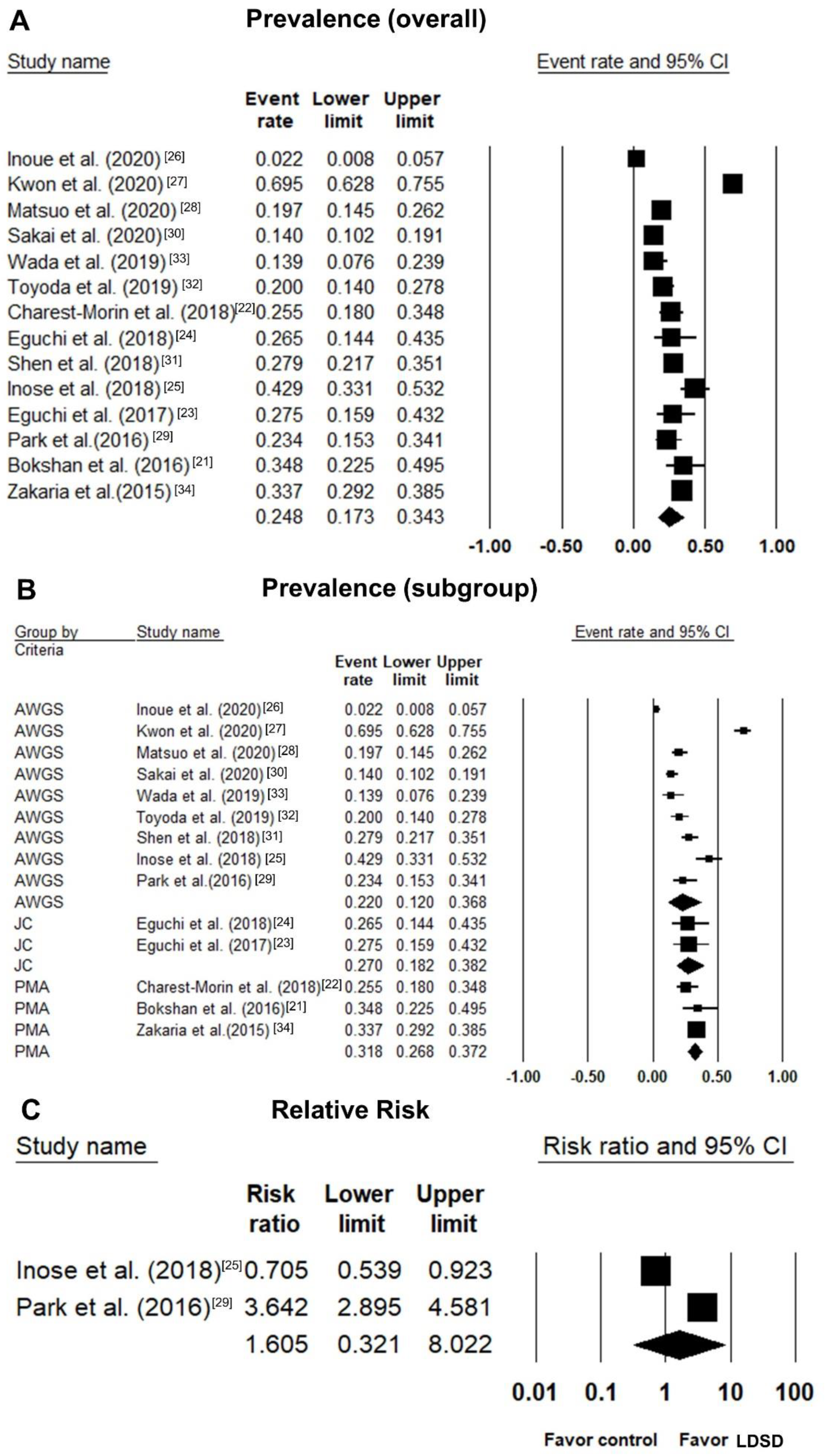
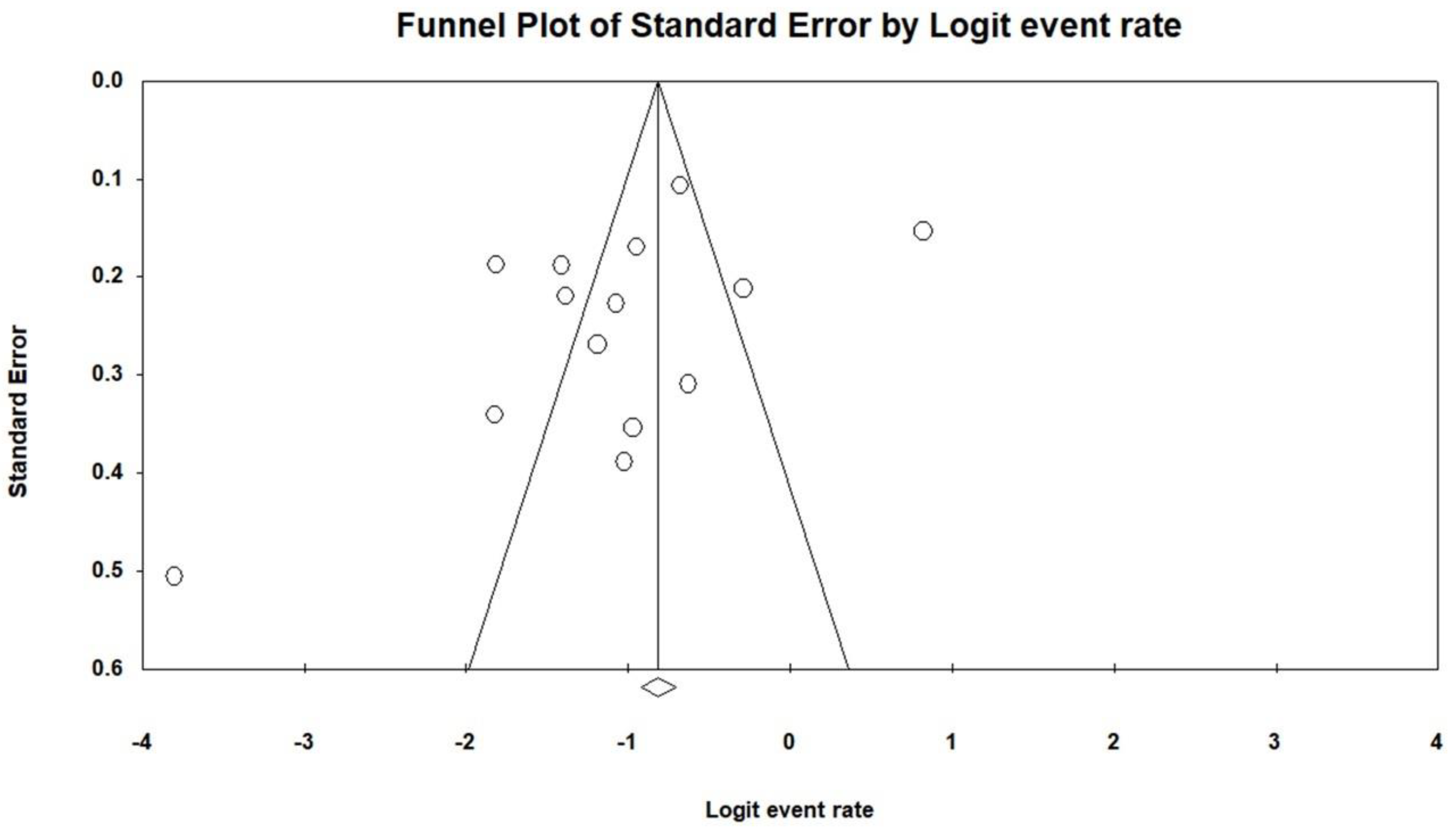
3.2.2. Prevalence of Sarcopenia in LDSD
3.2.3. Relative Risk of Sarcopenia in LDSD vs. Controls
3.3. Clinical Outcomes
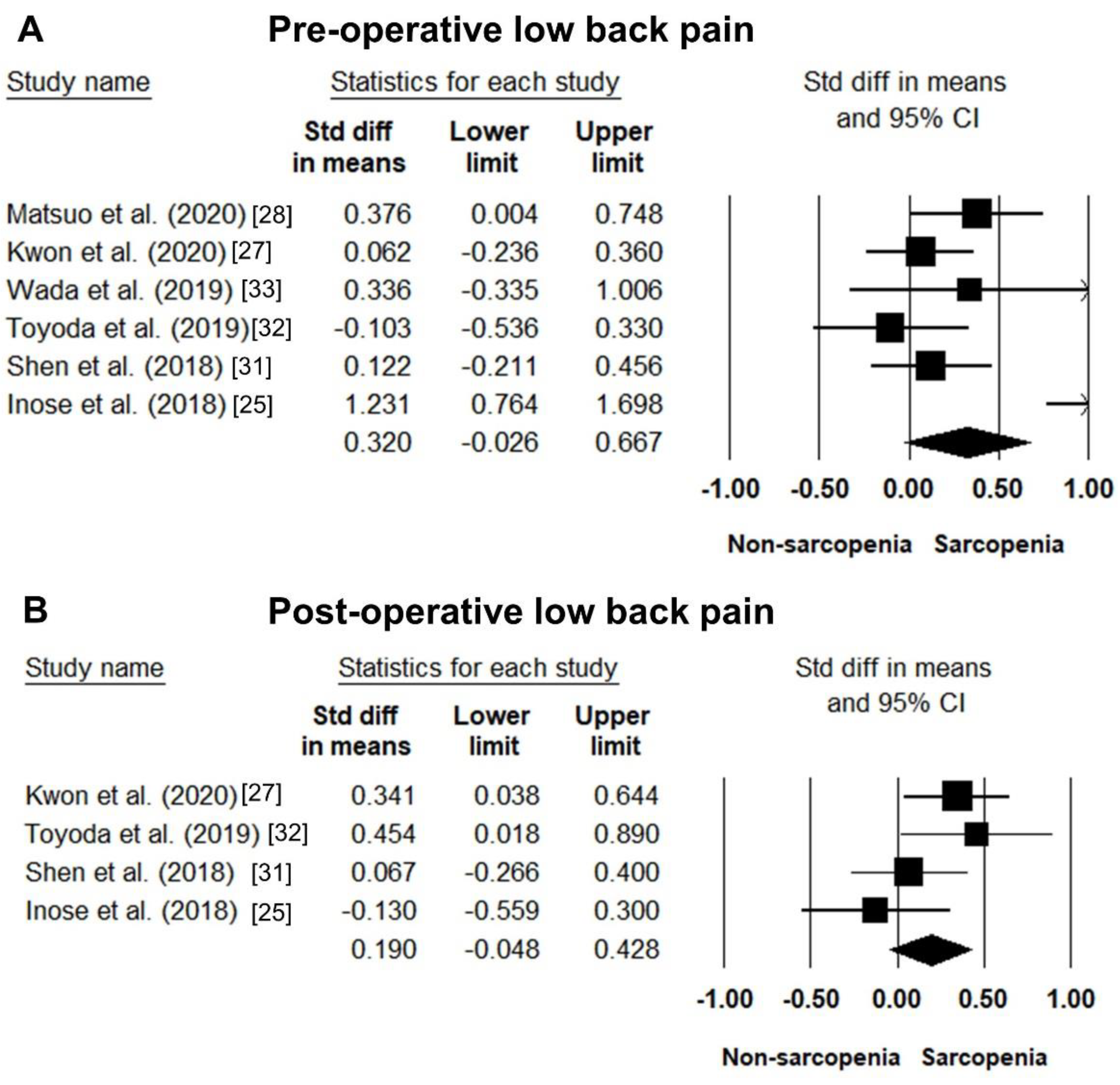
3.3.1. Low Back Pain
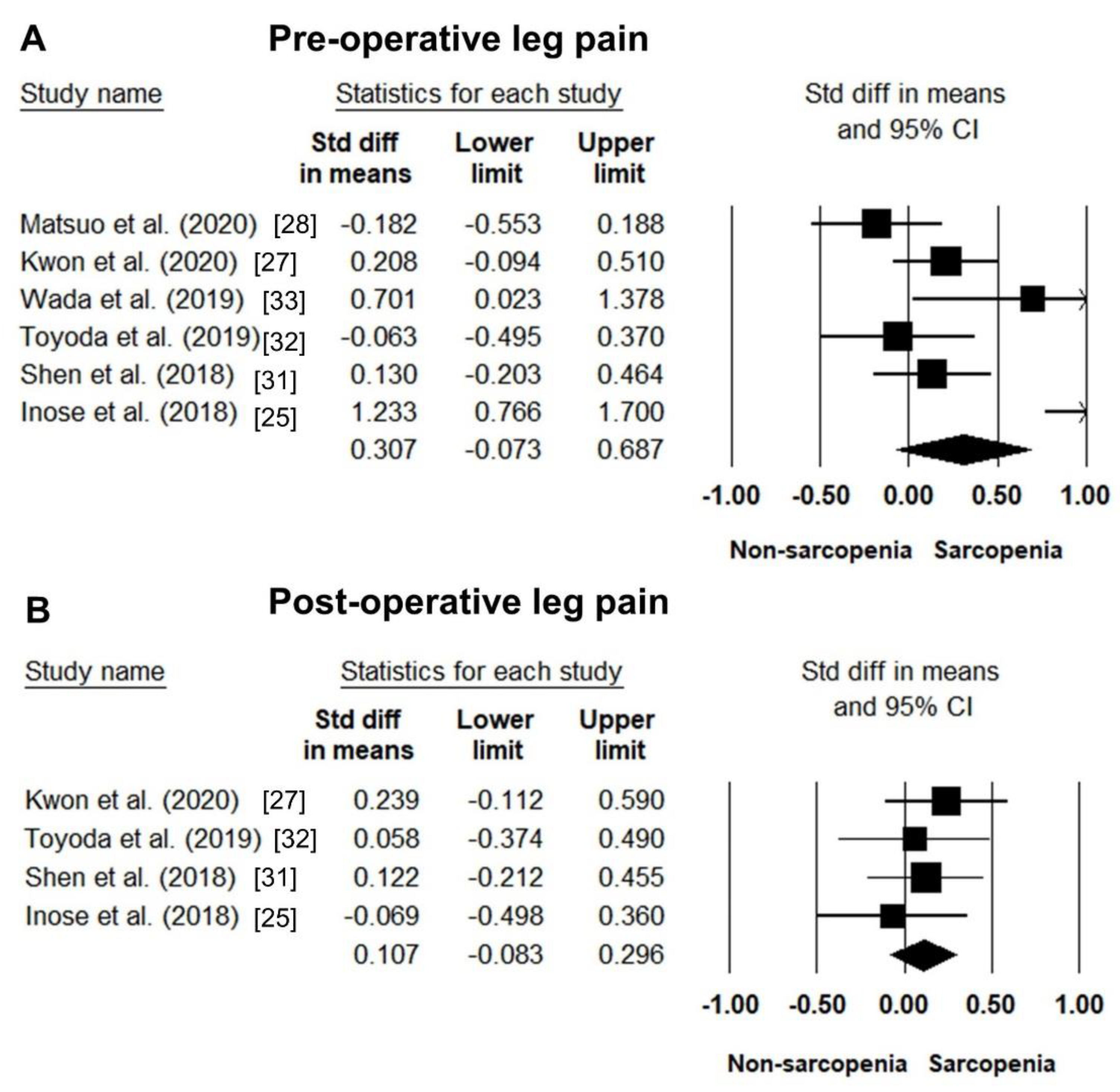
3.3.2. Leg Pain
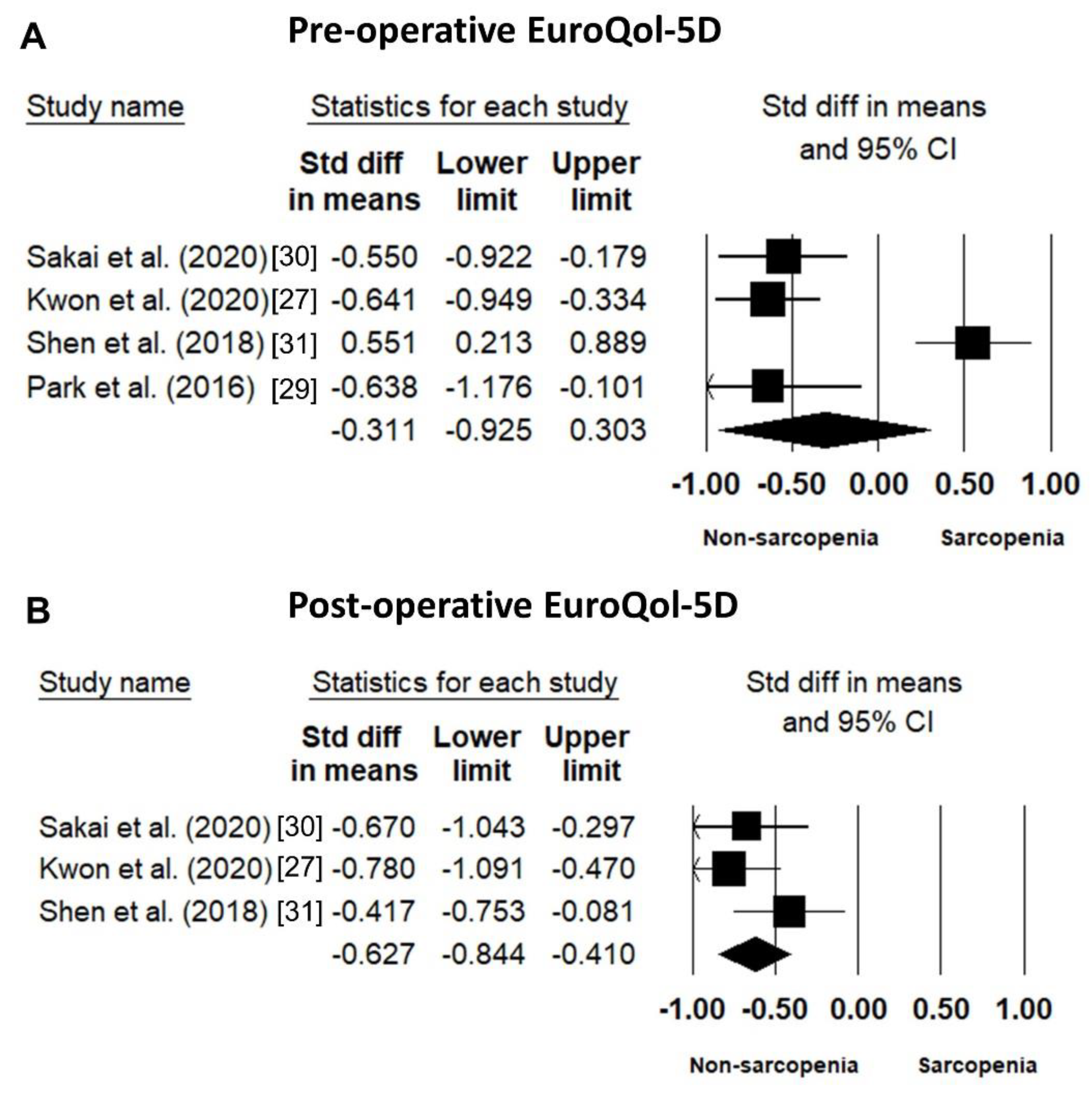
3.3.3. EuroQol-5D (EQ-5D)
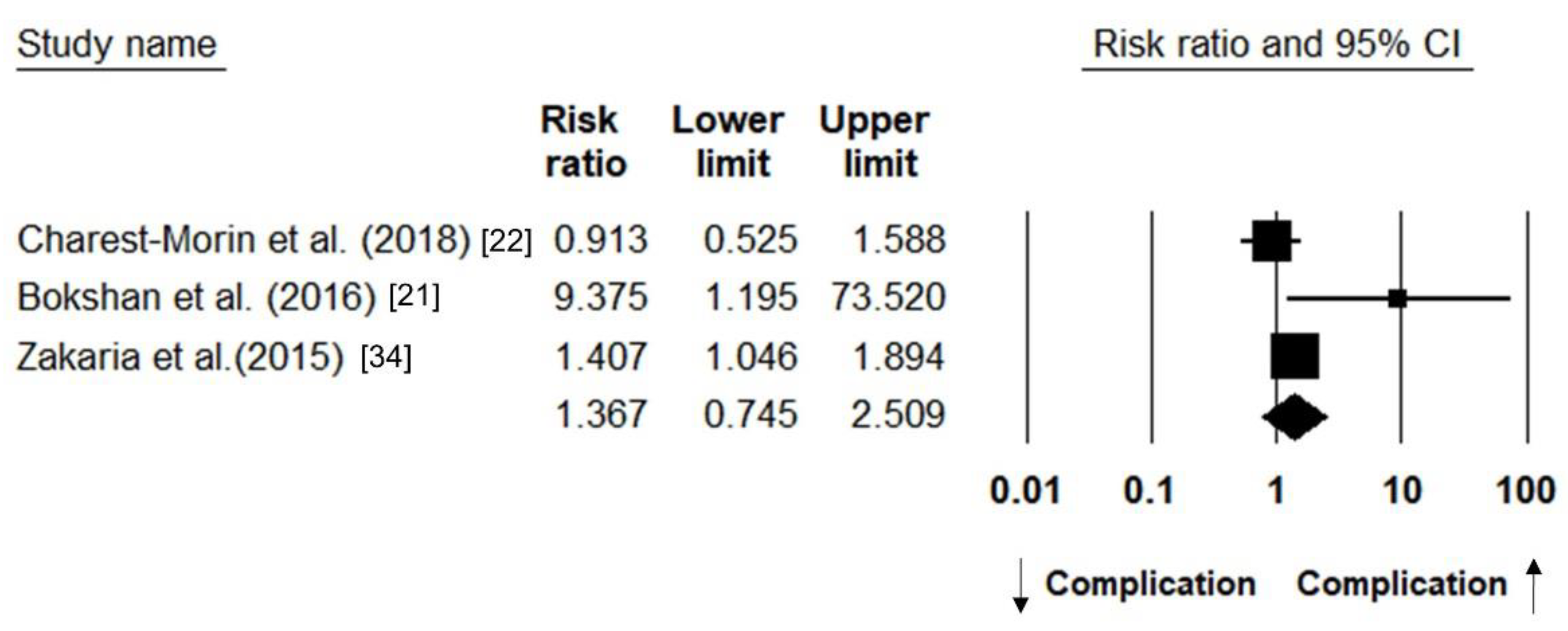
3.3.4. Post-Operative Complication
4. Discussion
5. Conclusions
Protocol Registration
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| LDSD | Lumbar degenerative spine diseases |
| RR | Risk ratio |
| SMD | Standardized mean difference |
| AWGS | Asian Working Group for Sarcopenia |
| EQ-5D | EuroQol-5D |
Appendix A. Strategy of Literature Search
References
- Fatoye, F.; Gebrye, T.; Odeyemi, I. Real-world incidence and prevalence of low back pain using routinely collected data. Rheumatol. Int. 2019, 39, 619–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, A.Y.; Karppinen, J.; Samartzis, D. Low back pain in older adults: Risk factors, management options and future directions. Scoliosis Spinal Disord. 2017, 12, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Muraki, S.; Oka, H.; Akune, T.; Mabuchi, A.; En-Yo, Y.; Yoshida, M.; Saika, A.; Suzuki, T.; Yoshida, H.; Ishibashi, H.; et al. Prevalence of radiographic lumbar spondylosis and its association with low back pain in elderly subjects of population-based cohorts: The ROAD study. Ann. Rheum. Dis. 2008, 68, 1401–1406. [Google Scholar] [CrossRef]
- Parker, S.L.; Wong, C.C.; Gates, M.J.; Godil, S.S.; Devin, C.J.; McGirt, M.J. The relative impact of lumbar spondylosis on quality of life in the United States: A population health perspective. Spine J. 2012, 12, S85. [Google Scholar] [CrossRef]
- Middleton, K.; Fish, D.E. Lumbar spondylosis: Clinical presentation and treatment approaches. Curr. Rev. Musculoskelet. Med. 2009, 2, 94–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, D.B.; Luca, K.; Jensen, R.K.; Eyles, J.P.; Van Gelder, J.M.; Friedly, J.L.; Maher, C.G.; Ferreira, M.L. A critical appraisal of clinical practice guidelines for the treatment of lumbar spinal stenosis. Spine J. 2021, 25, 455–464. [Google Scholar]
- Grotle, M.; Småstuen, M.C.; Fjeld, O.; Grøvle, L.; Helgeland, J.; Storheim, K.; Solberg, T.K.; Zwart, J.-A. Lumbar spine surgery across 15 years: Trends, complications and reoperations in a longitudinal observational study from Norway. BMJ Open 2019, 9, e028743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amado Diago, C.A.; Abascal Bolado, B.; Agüero Calvo, J.; Durantes, B.; Ruiz De Infante, M.; Guerra, A.R.; García-Unzueta, M.T.; Alio Lavín, B.; Arnaiz-García, E. Sarcopenia index correlates with COPD clinical outcomes. European Respiratory Journal. 2018, 52 (Suppl. 62), PA722. [Google Scholar]
- Zhang, N.; Zhu, W.-L.; Liu, X.-H.; Chen, W.; Zhu, M.-L.; Kang, L.; Tian, R. Prevalence and prognostic implications of sarcopenia in older patients with coronary heart disease. J. Geriatr. Cardiol. 2019, 16, 756–763. [Google Scholar] [PubMed]
- Moon, S.J.; Kim, T.H.; Yoon, S.Y.; Chung, J.H.; Hwang, H.-J. Relationship between stage of chronic kidney disease and sarcopenia in korean aged 40 years and older using the Korea National Health and Nutrition Examination Surveys (Knhanes IV-2, 3, and V-1, 2), 2008–2011. PLoS ONE 2015, 10, e0130740. [Google Scholar] [CrossRef] [Green Version]
- Borggreve, A.S.; den Boer, R.B.; van Boxel, G.I.; de Jong, P.A.; Veldhuis, W.B.; Steenhagen, E.; van Hillegersberg, R.; Ruurda, J.P. The predictive value of low muscle mass as measured on CT scans for postoperative complications and mortality in gastric cancer patients: A systematic review and meta-analysis. J. Clin. Med. 2020, 9, 199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, K.-V.; Chen, J.-D.; Wu, W.-T.; Huang, K.-C.; Hsu, C.-T.; Han, D.-S. Association between loss of skeletal muscle mass and mortality and tumor recurrence in hepatocellular carcinoma: A systematic review and meta-analysis. Liver Cancer 2018, 7, 90–103. [Google Scholar] [CrossRef] [PubMed]
- Wiedmer, P.; Jung, T.; Castro, J.P.; Pomatto, L.C.; Sun, P.Y.; Davies, K.J.; Grune, T. Sarcopenia–Molecular mechanisms and open questions. Ageing Res. Rev. 2021, 65, 101200. [Google Scholar] [CrossRef] [PubMed]
- Moskven, E.; Bourassa-Moreau, É.; Charest-Morin, R.; Flexman, A.; Street, J. The impact of frailty and sarcopenia on postoperative outcomes in adult spine surgery. A systematic review of the literature. Spine J. 2018, 18, 2354–2369. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, D.; Ahern, D.P.; Curley, A.E.; Kepler, C.K.; Butler, J.S. Impact of sarcopenia on degenerative lumbar spondylosis. Clin. Spine Surg. 2020. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in me-ta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for me-ta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Chu, H. Quantifying publication bias in meta-analysis. Biometrics 2018, 74, 785–794. [Google Scholar] [CrossRef]
- Bokshan, S.L.; Han, A.L.; DePasse, J.M.; Eltorai, A.E.M.; Marcaccio, S.E.; Palumbo, M.A.; Daniels, A.H. Effect of sarcopenia on postoperative morbidity and mortality after thoracolumbar spine surgery. Orthopedics 2016, 39, e1159–e1164. [Google Scholar] [CrossRef] [Green Version]
- Charest-Morin, R.; Street, J.; Zhang, H.; Roughead, T.; Ailon, T.; Boyd, M.; Dvorak, M.; Kwon, B.; Paquette, S.; Dea, N.; et al. Frailty and sarcopenia do not predict adverse events in an elderly population undergoing non-complex primary elective surgery for de-generative conditions of the lumbar spine. Spine J. 2018, 18, 245–254. [Google Scholar] [CrossRef]
- Eguchi, Y.; Suzuki, M.; Yamanaka, H.; Tamai, H.; Kobayashi, T.; Orita, S.; Yamauchi, K.; Suzuki, M.; Inage, K.; Fujimoto, K.; et al. Associ-ations between sarcopenia and degenerative lumbar scoliosis in older women. Scoliosis Spinal Disord. 2017, 12, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eguchi, Y.; Suzuki, M.; Kanamoto, H.; Abe, K.; Norimoto, M.; Umimura, T.; Aoki, Y.; Koda, M.; Furuya, T.; Toyone, T.; et al. Influence of skeletal muscle mass and spinal alignment on surgical outcomes for lumbar spinal stenosis. Asian Spine J. 2018, 12, 556–562. [Google Scholar] [CrossRef]
- Inose, H.; Yamada, T.; Hirai, T.; Yoshii, T.; Abe, Y.; Okawa, A. The impact of sarcopenia on the results of lumbar spinal surgery. Osteoporos. Sarcopenia 2018, 4, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Inoue, H.; Watanabe, H.; Okami, H.; Shiraishi, Y.; Kimura, A.; Takeshita, K. Handgrip strength correlates with walking in lumbar spinal stenosis. Eur. Spine J. 2020, 29, 2198–2204. [Google Scholar] [CrossRef]
- Kwon, J.-W.; Lee, B.H.; Lee, S.-B.; Sung, S.; Lee, C.-U.; Yang, J.-H.; Park, M.-S.; Byun, J.; Lee, H.-M.; Moon, S.-H. Hand grip strength can predict clinical outcomes and risk of falls after decompression and instrumented posterolateral fusion for lumbar spinal stenosis. Spine J. 2020, 20, 1960–1967. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, S.; Kawakami, M.; Sumiya, T.; Nakagawa, Y.; Minetama, M.; Nakagawa, M.; Teraguchi, M.; Kagotani, R.; Mera, Y.; Yamamoto, Y.; et al. Clinical features of sarcopenia in patients with lumbar spinal stenosis. Spine 2020, 45, E1105–E1110. [Google Scholar] [CrossRef]
- Park, S.; Kim, H.J.; Ko, B.G.; Chung, J.W.; Kim, S.H.; Park, S.H.; Lee, M.H.; Yeom, J.S. The prevalence and impact of sarcopenia on degen-erative lumbar spinal stenosis. Bone Joint J. 2016, 98, 1093–1098. [Google Scholar] [CrossRef]
- Sakai, Y.; Wakao, N.; Matsui, H.; Tomita, K.; Watanabe, T.; Iida, H. Surgical results in older patients with lumbar spinal stenosis according to gait speed in relation to the diagnosis for sarcopenia. J. Orthop. Surg. 2020, 28. [Google Scholar] [CrossRef]
- Shen, F.; Kim, H.-J.; Lee, N.-K.; Chun, H.-J.; Chang, B.-S.; Lee, C.-K.; Yeom, J.S. The influence of hand grip strength on surgical outcomes after surgery for degenerative lumbar spinal stenosis: A preliminary result. Spine J. 2018, 18, 2018–2024. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, H.; Hoshino, M.; Nakamura, H.; Ohyama, S.; Terai, H.; Suzuki, A.; Yamada, K.; Takahashi, S.; Hayashi, K.; Tamai, K.; et al. Impact of sarcopenia on clinical outcomes of minimally invasive lumbar decompression surgery. Sci. Rep. 2019, 9, 16619. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Tanishima, S.; Osaki, M.; Nagashima, H.; Hagino, H. Relationship between sarcopenia and pain catastrophizing in patients with lumbar spinal stenosis: A cross-sectional study. Osteoporos. Sarcopenia 2019, 5, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Zakaria, H.M.; Schultz, L.; Mossa-Basha, F.; Griffith, B.; Chang, V. Morphometrics as a predictor of perioperative morbidity after lumbar spine surgery. Neurosurg. Focus 2015, 39, E5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadopoulou, S.K.; Tsintavis, P.; Potsaki, G.; Papandreou, D. Differences in the prevalence of sarcopenia in community-dwelling, nursing home and hospitalized individuals. A systematic review and meta-analysis. J. Nutr. Heal. Aging 2020, 24, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Pacifico, J.; Geerlings, M.A.; Reijnierse, E.M.; Phassouliotis, C.; Lim, W.K.; Maier, A.B. Prevalence of sarcopenia as a comorbid disease: A systematic review and meta-analysis. Exp. Gerontol. 2020, 131, 110801. [Google Scholar] [CrossRef]
- Chang, K.V.; Chen, Y.C.; Wu, W.T.; Shen, H.J.; Huang, K.C.; Chu, H.P.; Han, D.S. Expression of telomeric repeat-containing RNA de-creases in sarcopenia and increases after exercise and nutrition intervention. Nutrients 2020, 12, 3766. [Google Scholar] [CrossRef]
- Faraone, S.V. Interpreting estimates of treatment effects: Implications for managed care. Pharm. Ther. 2008, 33, 700–711. [Google Scholar]
- Pipek, L.Z.; Baptista, C.G.; Meyer, A.; Andraus, W.; Nascimento, R.F.V.; Taba, J.V.; Suzuki, M.O.; Nascimento, F.S.D.; Martines, D.R.; Nii, F.; et al. The impact of properly diagnosed sarcopenia on postoperative outcomes after gastrointestinal surgery: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0237740. [Google Scholar] [CrossRef]
- Guo, Z.; Gu, C.; Gan, S.; Li, Y.; Xiang, S.; Gong, L.; Chan, F.L.; Wang, S. Sarcopenia as a predictor of postoperative outcomes after urologic oncology surgery: A systematic review and meta-analysis. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 560–573. [Google Scholar] [CrossRef]
- Sousa-Victor, P.; Muñoz-Cánoves, P. Regenerative decline of stem cells in sarcopenia. Mol. Asp. Med. 2016, 50, 109–117. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Design | Patient Characteristic | Type of Lumbar Spine Surgery | Outcome | n Total | Age (Year) | Sex Ratio: M/F | Data Collection Period | Country |
|---|---|---|---|---|---|---|---|---|---|
| Inoue et al. (2020) [26] | Cross-sectional | Patients with LSS | Not specified | Intermittent claudication(m), PMI, BMI, Comorbidity | 183 | 70.5 ± 8.6 | 128/55 | 2015/06–2018/03 | Japan |
| Kwon et al. (2020) [27] | Cross-sectional | Patients with LSS w or w/o spondylolisthesis | Decompression surgery, TLIF | ODI, EQ-5D, VAS (back/leg pain), AST, SMT, STS, TUGT | 200 | 69.5 ± 6.5 (sarcopenia, F) 69.9 ± 6.5 (sarcopenia, M) 64.5 ± 7.1 (non-sarcopenic, F) 65.4 ± 9.7 (non-sarcopenic, M) | 74/126 | 2014/04–2016/04 | Korea |
| Matsuo et al. (2020) [28] | Cross-sectional | Patients with degenerative LSS | Nil | VAS (back/leg pain and numbness), SF36, JOABPEQ, BMD (lumbar, femoral), Spinal alignment | 178 | 79.0 ± 1.2 (sarcopenic) 72.6 ± 0.6 (non-sarcopenic) | 77/101 | 2017/09–2018/08 | Japan |
| Sakai et al. (2020) [30] | Retrospective cohort | Patients with LSS w or w/o spondylolisthesis | Decompression surgery, PLIF | RDQ, SF36 PCS, EQ-5D, BMI, BMD, Spinal alignment | 235 | 73.2 + 5.8 | 135/100 | 2014/04–2017/03 | Japan |
| Wada et al. (2019) [33] | Cross-sectional | Patients with LSS | Nil | VAS (back/leg pain), JOA score (lower back dysfunction), PCS, HADS, FABQ | 72 | 70.4 ± 6.9 | 38/34 | 2015/10–2018/04 | Japan |
| Toyoda et al. (2019) [32] | Cross-sectional | Patients with LSS, degenerative lumbar spondylolisthesis, degenerative lumbar scoliosis | Minimally invasive lumbar decompression surgery | JOA score, VAS (back/leg pain and numbness) | 130 | 76.9 ± 6.4 | 70/60 | 2015/10–2016/07 | Japan |
| Charest-Morin et al. (2018) [22] | Retrospective cohort | Patients with LSS w or w/o spondylolisthesis, disc herniation | Decompression or fusion surgery | ASA, surgical factors, mFI, SSII, major complications, LOS | 102 | 72 (IQR:68-78) | 51/51 | 2009/01/01–2013/13/31 | Canada |
| Eguchi et al. (2018) [24] | Retrospective cohort | Patients with LSS | Laminectomy, TLIF, OLIF | JOA score, RDQ, BMD, spinal alignment | 34 | 74.4 | Nil | 2014/04–2016/10 | Japan |
| Shen et al. (2018) [31] | Retrospective cohort | Patient with LSS w or w/o spondylolisthesis | Decompressive surgery w or w/o fusion (PLIF, TLIF) | PRO, ODI, EQ-5D, VAS (back/leg pain) | 170 | 72.3 ± 6.6 (sarcopenic) 68.1± 9.2 (non-sarcopenic) | 14/34 (sarcopenic) 63/61(non-sarcopenic) | 2016/10–2017/06 | Korea |
| Inose et al. (2018) [25] | Retrospective cohort | Patients with LSS, lumbar compression fracture, lumbar kyphosis | Wide fenestration, PLIF, vertebral column resection, Pedicle subtraction osteotomies | JOA score, VAS (back/leg and numbness) | 91 | 74.8 ± 0.9 (sarcopenic) 73.0 ± 1.0 (non-sarcopenic) | 17/20 (sarcopenic) 16/32 (non-sarcopenic) | 2014/1/1–2015/12/31 | Japan |
| Eguchi et al. (2017) [23] | Cross-sectional | Patients with LSS, lumbar scoliosis, | Laminectomies, corrective surgery | BMD, lean mass in body parts, JOA, RDQ Spinal alignment | 40 | 74.0 ± 1.0 | 0/40 | nil | Japan |
| Park et al.(2016) [29] | Cross-sectional | Patients with LSS | Nil | EQ-5D, BMI, STS, TUG, ODI, EQ5D | 77 | 67.88 ± 6.91 | 18/59 | 2014/08–2014/11 | Korea |
| Bokshan et al. (2016) [21] | Retrospective cohort | Patients with LSS, scoliosis, epidural abscess, discitis, acute fracture | Decompression w or w/o fusion | CCI, MSII, SII, postoperative complications, LOS, disposition at discharge | 46 | 76.4 ± 8.8 (sarcopenic) 69.9 ± 10.95 (non-sarcopenic) | 22/24 | 2003–2015/09 | U.S. |
| Zakaria et al.(2015) [34] | Retrospective cohort | Patients receiving lumbar surgery | Laminectomy, OLIF, PLIF, MIS | LOS, disposition at discharge, any 90 day postoperative complications | 395 | 63.30 ± 12.48 | 192/203 | 2013–2014 | U.S. |
| Author, Year | Muscle Strength | Muscle Volume | Muscle Function | Diagnostic Algorithm |
|---|---|---|---|---|
| Cut-Off Points | ||||
| Inoue et al. (2020) [26] | handheld dynamometer | CT: Bilateral psoas muscle and skeletal muscle (at the third lumbar vertebra) | 10 m walk test | AWGS: low HGS + low gait speed + low PMI |
| ① | PMI Male: <6.36 cm2/m2, Female: <3.92 cm2/m2 | ④ | ||
| Kwon et al. (2020) [27] | JAMAR plus + hand grip dynamometer | Nil | Alternative step test, 6 m walk test, sit-to-stand test, time up and go test | AWGS: low HGS |
| ① | Nil | Nil | ||
| Matsuo et al. (2020) [28] | T.K.K.5001 dynamometer | BIA | 5 m walk test | AWGS: low HGS + low gait speed + low SMI |
| ① | ② | ④ | ||
| Sakai et al. (2020) [30] | Jamar-type dynamometer | BIA | 10 m walk test | AWGS: low SMI + Low HGS + low gait speed |
| ① | ② | ④ | ||
| Wada et al. (2019) [33] | T.K.K. 5401 dynamometer | BIA | 10 m walk test | AWGS: low SMI |
| Nil | Nil | |||
| Toyoda et al. (2019) [32] | T.K.K.5401 dynamometer | BIA | 5 m walk test | AWGS: Severe sarcopenia: low SMI + low HGS + low gait speed |
| ① | ② | ④ | ||
| Charest-Morin et al. (2018) [22] | Nil | CT: total psoas area (L3 transverse process) | Nil | Normalized total psoas area (NTPA) |
| Nil | NTPA: lowest quartile | Nil | ||
| Eguchi et al. (2018) [24] | Nil | DEXA | Nil | SMI |
| Nil | ③ | Nil | ||
| Shen et al. (2018) [31] | hand dynamometer | Nil | Nil | AWGS: low HGS |
| ① | Nil | Nil | ||
| Inose et al. (2018) [25] | Nil | DEXA | Nil | AWGS: low SMI |
| Nil | ② | Nil | ||
| Eguchi et al. (2017) [23] | Nil | DEXA | Nil | SMI |
| Nil | ③ | Nil | ||
| Park et al. (2016) [29] | dynamometer | BIA | sit-to-stand test, time up and go test | AWGS: low HGS (defined as sarcopenia in our meta-analysis) or low SMI |
| ① | ② | Nil | ||
| Bokshan et al. (2016) [21] | Nil | CT: bilateral psoas muscle at the fourth lumbar transverse process | Nil | TPA (lowest third) |
| Nil | TPA: lowest third | NIl | ||
| Zakaria et al. (2015) [34] | Nil | MRI: bilateral psoas muscle area at the fourth lumbar vertebra | Nil | TPA (lowest third) |
| Nil | TPA: lowest third | Nil | ||
| Representative of Sarcopenia Patients | Selection of Control | Ascertain of Sarcopenia Measurement | Outcome of Interest not Present at Start | Comparability of Cohorts | Assessment of Outcome | Enough Follow-Up Period | Adequacy of Follow Up | Total Point | |
|---|---|---|---|---|---|---|---|---|---|
| Inoue et al. (2020) [26] | ★ | - | ★ | ★ | ★★ | ★ | - | ★ | 7 |
| Kwon et al. (2020) [27] | ★ | - | ★ | ★ | ★★ | ★ | - | ★ | 7 |
| Matsuo et al. (2020) [28] | ★ | - | ★ | ★ | ★★ | ★ | - | ★ | 7 |
| Sakai et al. (2020) [30] | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ★ | 9 |
| Wada et al. (2019) [33] | ★ | - | ★ | ★ | ★★ | ★ | - | ★ | 7 |
| Toyoda et al. (2019) [32] | ★ | - | ★ | ★ | ★★ | ★ | - | ★ | 7 |
| Charest-Morin et al. (2018) [22] | ★ | - | ★ | ★ | ★★ | ★ | ★ | ★ | 8 |
| Eguchi et al. (2018) [24] | ★ | - | ★ | ★ | ★★ | ★ | ★ | ★ | 8 |
| Shen et al. (2018) [31] | ★ | - | ★ | ★ | ★★ | ★ | ★ | ★ | 8 |
| Inose et al. (2018) [25] | ★ | - | ★ | ★ | ★★ | ★ | ★ | ★ | 8 |
| Eguchi et al. (2017) [23] | - | - | ★ | ★ | ★★ | ★ | - | ★ | 6 |
| Park et al. (2016) [29] | ★ | ★ | ★ | ★ | ★★ | ★ | - | ★ | 8 |
| Bokshan et al. (2016) [21] | ★ | - | ★ | ★ | ★★ | ★ | ★ | ★ | 8 |
| Zakaria et al. (2015) [34] | ★ | - | ★ | ★ | ★★ | ★ | ★ | ★ | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, W.-T.; Lee, T.-M.; Han, D.-S.; Chang, K.-V. The Prevalence of Sarcopenia and Its Impact on Clinical Outcomes in Lumbar Degenerative Spine Disease—A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 773. https://doi.org/10.3390/jcm10040773
Wu W-T, Lee T-M, Han D-S, Chang K-V. The Prevalence of Sarcopenia and Its Impact on Clinical Outcomes in Lumbar Degenerative Spine Disease—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(4):773. https://doi.org/10.3390/jcm10040773
Chicago/Turabian StyleWu, Wei-Ting, Tsung-Min Lee, Der-Sheng Han, and Ke-Vin Chang. 2021. "The Prevalence of Sarcopenia and Its Impact on Clinical Outcomes in Lumbar Degenerative Spine Disease—A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 4: 773. https://doi.org/10.3390/jcm10040773