
SP-D Serum Levels Reveal Distinct Epithelial Damage in Direct Human ARDS

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients
2.2. Biomarker Measurement
2.3. Statistics
3. Results
3.1. Patient Characteristics
3.2. Epithelial Damage Differs between Different Etiologies of ARDS
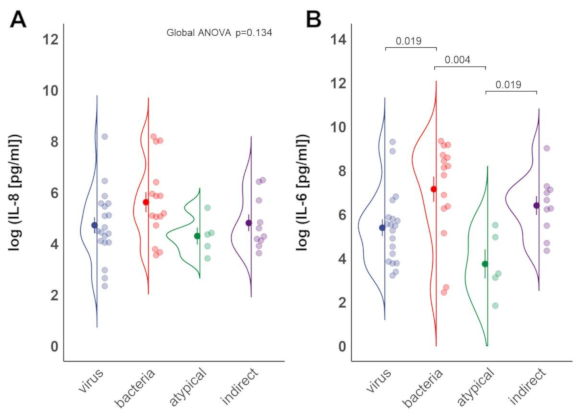
3.3. Inflammation Differs between Sub-Groups of ARDS
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Calfee, C.S.; Janz, D.R.; Bernard, G.R.; May, A.K.; Kangelaris, K.N.; Matthay, M.A.; Ware, L.B. Distinct Molecular Phenotypes of Direct vs. Indirect ARDS in Single-Center and Multicenter Studies. Chest 2015, 147, 1539–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walter, J.M.; Wilson, J.; Ware, L.B. Biomarkers in Acute Respiratory Distress Syndrome: From Pathobiology to Improving Patient Care. Expert Rev. Respir. Med. 2014, 8, 573–586. [Google Scholar] [CrossRef]
- Wilson, J.G.; Calfee, C.S. ARDS Subphenotypes: Understanding a Heterogeneous Syndrome. Crit. Care 2020, 24, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Matthay, M.A.; Brower, R.G.; Carson, S.; Douglas, I.S.; Eisner, M.; Hite, D.; Holets, S.; Kallet, R.H.; Liu, K.D.; et al. (Eds.) Randomized, Placebo-Controlled Clinical Trial of an Aerosolized Β₂-Agonist for Treatment of Acute Lung Injury. Am. J. Respir. Crit. Care Med. 2011, 184, 561–568. [Google Scholar] [CrossRef] [Green Version]
- Jabaudon, M.; Blondonnet, R.; Pereira, B.; Cartin-Ceba, R.; Lichtenstern, C.; Mauri, T.; Determann, R.M.; Drabek, T.; Hubmayr, R.D.; Gajic, O.; et al. Plasma SRAGE Is Independently Associated with Increased Mortality in ARDS: A Meta-Analysis of Individual Patient Data. Intensive Care Med. 2018, 44, 1388–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisner, M.D.; Parsons, P.; Matthay, M.A.; Ware, L.; Greene, K. Acute Respiratory Distress Syndrome Network Plasma Surfactant Protein Levels and Clinical Outcomes in Patients with Acute Lung Injury. Thorax 2003, 58, 983–988. [Google Scholar] [CrossRef] [Green Version]
- Delgado, C.; Krötzsch, E.; Jiménez-Alvarez, L.A.; Ramírez-Martínez, G.; Márquez-García, J.E.; Cruz-Lagunas, A.; Morán, J.; Hernández, C.; Sierra-Vargas, P.; Avila-Moreno, F.; et al. Serum Surfactant Protein D (SP-D) Is a Prognostic Marker of Poor Outcome in Patients with A/H1N1 Virus Infection. Lung 2015, 193, 25–30. [Google Scholar] [CrossRef]
- Mogensen, T.H. Pathogen Recognition and Inflammatory Signaling in Innate Immune Defenses. Clin. Microbiol. Rev. 2009, 22, 240–273, Table of Contents. [Google Scholar] [CrossRef] [Green Version]
- Schütte, H.; Lohmeyer, J.; Rosseau, S.; Ziegler, S.; Siebert, C.; Kielisch, H.; Pralle, H.; Grimminger, F.; Morr, H.; Seeger, W. Bronchoalveolar and Systemic Cytokine Profiles in Patients with ARDS, Severe Pneumonia and Cardiogenic Pulmonary Oedema. Eur. Respir. J. 1996, 9, 1858–1867. [Google Scholar] [CrossRef] [Green Version]
- Bouros, D.; Alexandrakis, M.G.; Antoniou, K.M.; Agouridakis, P.; Pneumatikos, I.; Anevlavis, S.; Pataka, A.; Patlakas, G.; Karkavitsas, N.; Kyriakou, D. The Clinical Significance of Serum and Bronchoalveolar Lavage Inflammatory Cytokines in Patients at Risk for Acute Respiratory Distress Syndrome. BMC Pulm. Med. 2004, 4, 6. [Google Scholar] [CrossRef] [Green Version]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Chow, A.W.; Liang, J.F.; Wong, J.S.; Fu, Y.; Tang, N.L.; Ko, W. Polarized Secretion of Interleukin (IL)-6 and IL-8 by Human Airway Epithelia 16HBE14o- Cells in Response to Cationic Polypeptide Challenge. PLoS ONE 2010, 5, e12091. [Google Scholar] [CrossRef]
- Leth-Larsen, R.; Nordenbaek, C.; Tornoe, I.; Moeller, V.; Schlosser, A.; Koch, C.; Teisner, B.; Junker, P.; Holmskov, U. Surfactant Protein D (SP-D) Serum Levels in Patients with Community-Acquired Pneumonia. Clin. Immunol. 2003, 108, 29–37. [Google Scholar] [CrossRef]
- Spoorenberg, S.M.C.; Vestjens, S.M.T.; Voorn, G.P.; van Moorsel, C.H.M.; Meek, B.; Zanen, P.; Rijkers, G.T.; Bos, W.J.W.; Grutters, J.C. Ovidius study group Course of SP-D, YKL-40, CCL18 and CA 15-3 in Adult Patients Hospitalised with Community-Acquired Pneumonia and Their Association with Disease Severity and Aetiology: A Post-Hoc Analysis. PLoS ONE 2018, 13, e0190575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krammer, F.; Smith, G.J.D.; Fouchier, R.A.M.; Peiris, M.; Kedzierska, K.; Doherty, P.C.; Palese, P.; Shaw, M.L.; Treanor, J.; Webster, R.G.; et al. Influenza. Nat. Rev. Dis. Primers 2018, 4, 3. [Google Scholar] [CrossRef] [PubMed]
- Arnold, F.W.; Summersgill, J.T.; Ramirez, J.A. Role of Atypical Pathogens in the Etiology of Community-Acquired Pneumonia. Semin. Respir. Crit. Care Med. 2016, 37, 819–828. [Google Scholar] [CrossRef]
- YKL-40, CCL18 and SP-D Predict Mortality in Patients Hospitalized with Community-Acquired Pneumonia—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/27782361/ (accessed on 20 October 2020).
- Gaunsbaek, M.Q.; Rasmussen, K.J.; Beers, M.F.; Atochina-Vasserman, E.N.; Hansen, S. Lung Surfactant Protein D (SP-D) Response and Regulation during Acute and Chronic Lung Injury. Lung 2013, 191, 295–303. [Google Scholar] [CrossRef]
- Fujita, M.; Shannon, J.M.; Ouchi, H.; Voelker, D.R.; Nakanishi, Y.; Mason, R.J. Serum Surfactant Protein D Is Increased in Acute and Chronic Inflammation in Mice. Cytokine 2005, 31, 25–33. [Google Scholar] [CrossRef]
- Blondonnet, R.; Audard, J.; Belville, C.; Clairefond, G.; Lutz, J.; Bouvier, D.; Roszyk, L.; Gross, C.; Lavergne, M.; Fournet, M.; et al. RAGE Inhibition Reduces Acute Lung Injury in Mice. Sci. Rep. 2017, 7, 7208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuire, V.A.; Arthur, J.S.C. Subverting Toll-Like Receptor Signaling by Bacterial Pathogens. Front. Immunol. 2015, 6, 607. [Google Scholar] [CrossRef] [Green Version]
- Kraft, M.; Adler, K.B.; Ingram, J.L.; Crews, A.L.; Atkinson, T.P.; Cairns, C.B.; Krause, D.C.; Chu, H.W. Mycoplasma Pneumoniae Induces Airway Epithelial Cell Expression of MUC5AC in Asthma. Eur. Respir. J. 2008, 31, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Simon, R. Clinical Trial Designs for Evaluating the Medical Utility of Prognostic and Predictive Biomarkers in Oncology. Pers. Med. 2010, 7, 33–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theuerkauf, N.; Weismüller, T.; Weißbrich, C.; Schewe, J.-C.; Putensen, C.; Bode, C. Direct Acute Respiratory Distress Syndrome after Gastric Perforation Caused by an Intragastric Balloon: A Case Report. BMC Anesthesiol. 2020, 20, 182. [Google Scholar] [CrossRef] [PubMed]
- Remmelts, H.H.F.; Meijvis, S.C.A.; Heijligenberg, R.; Rijkers, G.T.; Oosterheert, J.J.; Bos, W.J.W.; Endeman, H.; Grutters, J.C.; Hoepelman, A.I.M.; Biesma, D.H. Biomarkers Define the Clinical Response to Dexamethasone in Community-Acquired Pneumonia. J. Infect. 2012, 65, 25–31. [Google Scholar] [CrossRef]
- Steinberg, K.P.; Hudson, L.D.; Goodman, R.B.; Hough, C.L.; Lanken, P.N.; Hyzy, R.; Thompson, B.T.; Ancukiewicz, M. National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Efficacy and Safety of Corticosteroids for Persistent Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2006, 354, 1671–1684. [Google Scholar] [CrossRef]
- Thompson, B.T.; Chambers, R.C.; Liu, K.D. Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2017, 377, 562–572. [Google Scholar] [CrossRef]
- Barnett, N.; Ware, L.B. Biomarkers in Acute Lung Injury—Marking Forward Progress. Crit. Care Clin. 2011, 27, 661–683. [Google Scholar] [CrossRef] [Green Version]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.-H.; Dugas, A. The Frequency of Influenza and Bacterial Coinfection: A Systematic Review and Meta-Analysis. Influenza Other Respir. Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Virus (n = 19) | Bacteria (n = 15) | Atypical Pathogens (n = 5) | Indirect (n = 10) | p | ||||
|---|---|---|---|---|---|---|---|---|---|
| Age (y) | 56.5 | (48–63) | 59 | (37–70) | 67 | (61–71) | 50 | (43–55) | 0.063 |
| Male (%) | 14 | (74) | 12 | (80) | 3 | (60) | 9 | (90) | 0.512 |
| BMI (kg/m²) | 32.6 | (27.0–37.2) | 27.7 | (24.6–36.7) | 26.1 | (25–29.4) | 28.3 | (27.8–33.2) | 0.301 |
| Diabetes (%) | 3 | (16) | 3 | (20) | 1 | (20) | 3 | (30) | 0.785 |
| Immunosuppression (%) | 5 | (26) | 2 | (13.3) | 1 | (20) | 1 | (10) | 0.824 |
| Community acquired pneumonia (%) | 19 | (100) | 11 | (73) | 5 | (100) | N/A | 0.061 | |
| Steroids (%) | 4 | (21) | 5 | (33) | 1 | (20) | 6 | (60) | 0.164 |
| PaO2/FiO2 ratio (mmHg) | 72 | (60–99) | 86 | (73–147) | 95 | (90–162) | 129 | (72–158) | 0.131 |
| PEEP (cmH2O) | 19 | (14–20) | 18 | (14–20) | 18 | (16–20) | 17 | (14–18) | 0.723 |
| Driving pressure (cmH2O) | 9 | (7–14) | 9 | (6–14) | 10 | (9–11) | 10 | (8–12) | 0.946 |
| Tidal volume (ml/kg predicted body weight) | 3.5 | (2.4–6.7) | 2.7 | (2–6.4) | 1.9 | (1.4–3.8) | 4.1 | (2.6–7) | 0.389 |
| Procalcitonin (PCT_ (µg/L) | 1.9 | (0.9–17.6) | 27.2 | (6.3–70.1) | 0.4 | (0.4–3.4) | 11.3 | (2.1–67.9) | 0.024 * |
| Lactate (mmol/L) | 1.4 | (1.2–2.3) | 2.8 | (1.8–4.7) | 1.3 | (1.0–1.8) | 1.6 | (1.3–4.6) | 0.170 |
| SOFA score | 10 | (8–12) | 8 | (5–10) | 8 | (8–10) | 9 | (6–10) | 0.131 |
| ICU mortality (%) | 6 | (32) | 5 | (33) | 3 | (60) | 3 | (30) | 0.673 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peukert, K.; Seeliger, B.; Fox, M.; Feuerborn, C.; Sauer, A.; Schuss, P.; Schneider, M.; David, S.; Welte, T.; Putensen, C.; et al. SP-D Serum Levels Reveal Distinct Epithelial Damage in Direct Human ARDS. J. Clin. Med. 2021, 10, 737. https://doi.org/10.3390/jcm10040737
Peukert K, Seeliger B, Fox M, Feuerborn C, Sauer A, Schuss P, Schneider M, David S, Welte T, Putensen C, et al. SP-D Serum Levels Reveal Distinct Epithelial Damage in Direct Human ARDS. Journal of Clinical Medicine. 2021; 10(4):737. https://doi.org/10.3390/jcm10040737
Chicago/Turabian StylePeukert, Konrad, Benjamin Seeliger, Mario Fox, Caroline Feuerborn, Andrea Sauer, Patrick Schuss, Matthias Schneider, Sascha David, Tobias Welte, Christian Putensen, and et al. 2021. "SP-D Serum Levels Reveal Distinct Epithelial Damage in Direct Human ARDS" Journal of Clinical Medicine 10, no. 4: 737. https://doi.org/10.3390/jcm10040737