Severity by National Institute of Health Stroke Scale Score and Clinical Features of Stroke Patients with Patent Foramen Ovale Stroke and Atrial Fibrillation

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Evaluations
2.3. Baseline Study Assessment
2.4. Statistical Analysis
3. Results
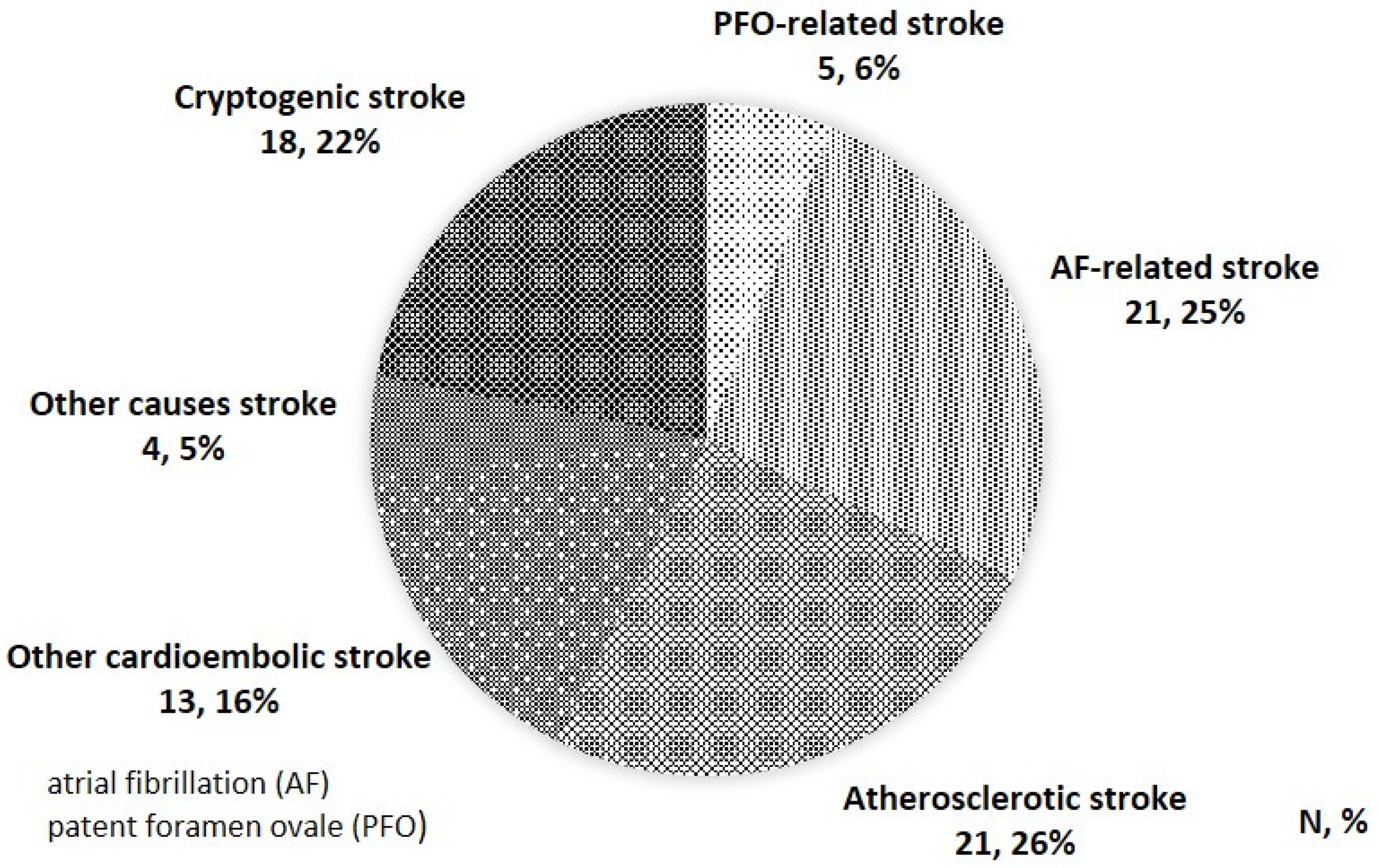
3.1. Stroke Classification
3.2. Study Population and Patient Features
3.3. PFO Characteristics of This Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mir, H.; Siemieniuk, R.A.C.; Ge, L.C.; Foroutan, F.; Fralick, M.; Syed, T.; Lopes, L.C.; Kuijpers, T.; Mas, J.-L.; Vandvik, P.O.; et al. Patent foramen ovale closure, antiplatelet therapy or anticoagulation in patients with patent foramen ovale and cryptogenic stroke: A systematic review and network meta-analysis incorporating complementary external evidence. BMJ Open 2018, 8, e023761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, H.P.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepi, M.; Evangelista, A.; Nihoyannopoulos, P.; Flachskampf, F.A.; Athanassopoulos, G.; Colonna, P.; Habib, G.; Ringelstein, E.B.; Sicari, R.; Zamorano, J.L.; et al. Recommendations for echocardiography use in the diagnosis and management of cardiac sources of embolism: European Association of Echocardiography (EAE) (a registered branch of the ESC). Eur. J. Echocardiogr. 2010, 11, 461–476. [Google Scholar] [CrossRef] [Green Version]
- Osteraas, N.D.; Vargas, A.; Cherian, L.; Song, S. Role of PFO Closure in Ischemic Stroke Prevention. Curr. Treat. Options Cardiovasc. Med. 2019, 21, 63. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Hylek, E.M.; Phillips, K.A.; Chang, Y.; Henault, L.E.; Selby, J.V.; Singer, D.E. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001, 285, 2370–2375. [Google Scholar] [CrossRef]
- Gage, B.F.; Waterman, A.D.; Shannon, W.; Boechler, M.; Rich, M.W.; Radford, M.J. Validation of clinical classification schemes for predicting stroke: Results from the National Registry of Atrial Fibrillation. JAMA 2001, 285, 2864–2870. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J.G.M. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef]
- Ono, K.; Iwasaki, Y.; Shimizu, W.; Akao, M.; Ikeda, T.; Ishii, K.; Inden, Y.; Kusano, K.; Kobayashi, Y.; Koretsune, Y.; et al. JCS/JHRS 2020 Guideline on Pharmacotherapy of Cardiac Arrhythmias. Available online: https://www.j-circ.or.jp/cms/wp-content/uploads/2020/01/JCS2020_Ono.pdf (accessed on 28 August 2020).
- Majule, D.N.; Jing, C.; Rutahoile, W.M.; Shonyela, F.S. The Efficacy and Safety of the WATCHMAN Device in LAA Occlusion in Patients with Non-Valvular Atrial Fibrillation Contraindicated to Oral Anticoagulation: A Focused Review. Ann. Thorac. Cardiovasc. Surg. 2018, 24, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Kent, D.M.; Ruthazer, R.; Weimar, C.; Mas, J.-L.; Serena, J.; Homma, S.; Di Angelantonio, E.; Di Tullio, M.R.; Lutz, J.S.; Elkind, M.S.V.; et al. An index to identify stroke-related vs incidental patent foramen ovale in cryptogenic stroke. Neurology 2013, 81, 619–625. [Google Scholar] [CrossRef] [Green Version]
- Homma, S.; Sacco, R.L. Patent foramen ovale and stroke. Circulation 2005, 112, 1063–1072. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Song, J.-K.; Kim, J.S.; Heo, R.; Lee, S.; Kim, D.-H.; Song, J.-M.; Kang, D.-H.; Kwon, S.U.; Kang, D.-W.; et al. Cryptogenic Stroke and High-Risk Patent Foramen Ovale: The DEFENSE-PFO Trial. J. Am. Coll. Cardiol. 2018, 71, 2335–2342. [Google Scholar] [CrossRef] [PubMed]
- Søndergaard, L.; Kasner, S.E.; Rhodes, J.F.; Andersen, G.; Iversen, H.K.; Nielsen-Kudsk, J.E.; Settergren, M.; Sjöstrand, C.; Roine, R.O.; Hildick-Smith, D.; et al. Patent Foramen Ovale Closure or Antiplatelet Therapy for Cryptogenic Stroke. N. Engl. J. Med. 2017, 377, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Mas, J.-L.; Derumeaux, G.; Guillon, B.; Massardier, E.; Hosseini, H.; Mechtouff, L.; Arquizan, C.; Béjot, Y.; Vuillier, F.; Detante, O.; et al. Patent Foramen Ovale Closure or Anticoagulation vs. Antiplatelets after Stroke. N. Engl. J. Med. 2017, 377, 1011–1021. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.C.; Picard, M.H.; Carbone, A.; Arruda, A.L.; Flores, T.; Klohn, J.; Furtado, M.; Lira-Filho, E.B.; Cerri, G.G.; Andrade, J.L. Importance of adequately performed Valsalva maneuver to detect patent foramen ovale during transesophageal echocardiography. J. Am. Soc. Echocardiogr. 2013, 26, 1337–1343. [Google Scholar] [CrossRef]
- Consoli, D.; Paciaroni, M.; Galati, F.; Aguggia, M.; Melis, M.; Malferrari, G.; Consoli, A.; Vidale, S.; Bosco, D.; Cerrato, P.; et al. Prevalence of Patent Foramen Ovale in Ischaemic Stroke in Italy: Results of SISIFO Study. Cerebrovasc. Dis. 2015, 39, 162–169. [Google Scholar] [CrossRef]
- Sahin, O.; Savas, G. Relationship between presence of spontaneous echo contrast and platelet-to-lymphocyte ratio in patients with mitral stenosis. Echocardiography 2019, 36, 924–929. [Google Scholar] [CrossRef]
- Katz, E.S.; Tunick, P.A.; Rusinek, H.; Ribakove, G.; Spencer, F.C.; Kronzon, I. Protruding aortic atheromas predict stroke in elderly patients undergoing cardiopulmonary bypass: Experience with intraoperative transesophageal echocardiography. J. Am. Coll. Cardiol. 1992, 20, 70–77. [Google Scholar] [CrossRef] [Green Version]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; De Vos, C.B.; Crijns, H.J.G.M.; Lip, G.Y.H. A Novel User-Friendly Score (HAS-BLED) To Assess 1-Year Risk of Major Bleeding in Patients with Atrial Fibrillation. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef] [Green Version]
- Brott, T.; Adams, H.P.; Olinger, C.P.; Marler, J.R.; Barsan, W.G.; Biller, J.; Spilker, J.; Holleran, R.; Eberle, R.; Hertzberg, V. Measurements of acute cerebral infarction: A clinical examination scale. Stroke 1989, 20, 864–870. [Google Scholar] [CrossRef] [Green Version]
- Vitarelli, A.; Mangieri, E.; Capotosto, L.; Tanzilli, G.; D’Angeli, I.; Toni, D.; Azzano, A.; Ricci, S.; Placanica, A.; Rinaldi, E.; et al. Echocardiographic findings in simple and complex patent foramen ovale before and after transcatheter closure. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 1377–1385. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | PFO-Related Stroke | AF-Related Stroke | p-Value | |
|---|---|---|---|---|
| (n = 5) | (n = 21) | |||
| Age | y.o | 58.2 ± 23.4 | 77.9 ± 7.6 | n.s * |
| Sex (Male) | n (%) | 4 (80%) | 14 (66.7%) | n.s † |
| Height | cm | 166.4 ± 7.3 | 162.0 ± 8.0 | n.s |
| Body Weight | kg | 59.9 ± 10.7 | 58.9 ± 11.0 | n.s |
| Smoking Habit | n (%) | 5 (100%) | 11 (52.4%) | n.s † |
| Hypertension | n (%) | 1 (20%) | 18 (85.7%) | 0.01 † |
| Dyslipidemia | n (%) | 3 (60%) | 11 (52.4%) | n.s † |
| Diabetes | n (%) | 0 (0%) | 7 (33.3%) | n.s † |
| OMI | n (%) | 0 (0%) | 2 (9.5%) | n.s † |
| History of Stroke | n (%) | 0 (0%) | 2 (9.5%) | n.s † |
| PFO | n (%) | 5 (100%) | 0 (0%) | <0.01 † |
| AF | n (%) | 0 (0%) | 20 (95.2%) | <0.01 † |
| LA/LAA thrombus | n (%) | 0 (0%) | 10 (47.6%) | n.s † |
| LVEF | % | 69.0 ± 5.2 | 66.0 ± 8.4 | n.s |
| Antiplatet Therapy | n (%) | 2 (40%) | 7 (33.3%) | n.s † |
| Anticoagulant Therapy | n (%) | 0 (0%) | 4 (19%) | |
| DOAC | n (%) | 3 (14.3%) | ||
| Warfarin | n (%) | 1 (4.8%) | ||
| HAS-BLED Score | 2.2 ± 1.6 | 3.3 ± 0.9 | n.s | |
| NIHSS Score | 2.2 ± 2.8 | 11.5 ± 9.2 | <0.01 * | |
| Blood Test Parameters | PFO-Related Stroke | AF-Related Stroke | p-Value | |
|---|---|---|---|---|
| (n = 5) | (n = 21) | |||
| BNP | pg/mL | 39.5 ± 28.1 | 155.4 ± 189.0 | n.s * |
| D-dimer | ug/mL | 3.7 ± 5.6 | 2.0 ± 2.4 | n.s * |
| Hb | g/dL | 14.4 ± 1.3 | 13.8 ± 2.0 | n.s |
| HbA1c | % | 5.5 ± 0.2 | 6.3 ± 1.3 | 0.02 * |
| LDL | mg/dL | 116.0 ± 32.0 | 110.3 ± 42.4 | n.s |
| HDL | mg/dL | 67.2 ± 25.6 | 57.5 ± 17.4 | n.s |
| TG | mg/dL | 112.6 ± 55.6 | 125.1 ± 98.7 | n.s |
| Cre | mg/dL | 0.84 ± 0.2 | 1.01 ± 0.5 | n.s |
| eGFR | ml/min/1.73 m2 | 73.8 ± 17.4 | 58.9 ± 20.6 | n.s |
| CCR | ml/min | 83.2 ± 35.5 | 56.5 ± 23.7 | n.s |
| AST | IU/l | 19.0 ± 4.7 | 23.4 ± 5.8 | n.s |
| ALT | IU/l | 15.6 ± 2.7 | 15.5 ± 6.4 | n.s |
| LDH | IU/l | 178.0 ± 18.4 | 231.0 ± 45.2 | 0.02 |
| T-bil | mg/dL | 0.62 ± 0.23 | 0.77 ± 0.32 | n.s |
| ALP | IU/l | 182.4 ± 70.8 | 237.4 ± 95.3 | n.s |
| PFO Characteristics | PFO-Related Stroke | |
|---|---|---|
| (n = 5) | ||
| PFO Size | ||
| Small | n | 1 |
| Moderate | n | 2 |
| Large | n | 2 |
| Rope Score | 4.8 ± 2.4 | |
| PFO-Attributable Fraction | % | 36.0 ± 37.3 |
| Estimated Two Years Stroke Recurrence Rate | % | 12.2 ± 7.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abe, K.; Hasegawa, F.; Nakajima, R.; Fukui, H.; Shimada, M.; Miyazaki, T.; Doi, H.; Endo, G.; Kanbara, K.; Mochida, Y.; et al. Severity by National Institute of Health Stroke Scale Score and Clinical Features of Stroke Patients with Patent Foramen Ovale Stroke and Atrial Fibrillation. J. Clin. Med. 2021, 10, 332. https://doi.org/10.3390/jcm10020332
Abe K, Hasegawa F, Nakajima R, Fukui H, Shimada M, Miyazaki T, Doi H, Endo G, Kanbara K, Mochida Y, et al. Severity by National Institute of Health Stroke Scale Score and Clinical Features of Stroke Patients with Patent Foramen Ovale Stroke and Atrial Fibrillation. Journal of Clinical Medicine. 2021; 10(2):332. https://doi.org/10.3390/jcm10020332
Chicago/Turabian StyleAbe, Kaito, Fumiya Hasegawa, Ryota Nakajima, Hidetoshi Fukui, Moto Shimada, Takahiro Miyazaki, Hiroshi Doi, Goro Endo, Kaori Kanbara, Yasuyuki Mochida, and et al. 2021. "Severity by National Institute of Health Stroke Scale Score and Clinical Features of Stroke Patients with Patent Foramen Ovale Stroke and Atrial Fibrillation" Journal of Clinical Medicine 10, no. 2: 332. https://doi.org/10.3390/jcm10020332