Correlation between PlateletWorks® and PFA-100® for Measuring Platelet Function before Urgent Surgery in Patients with Chronic Antiplatelet Therapy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
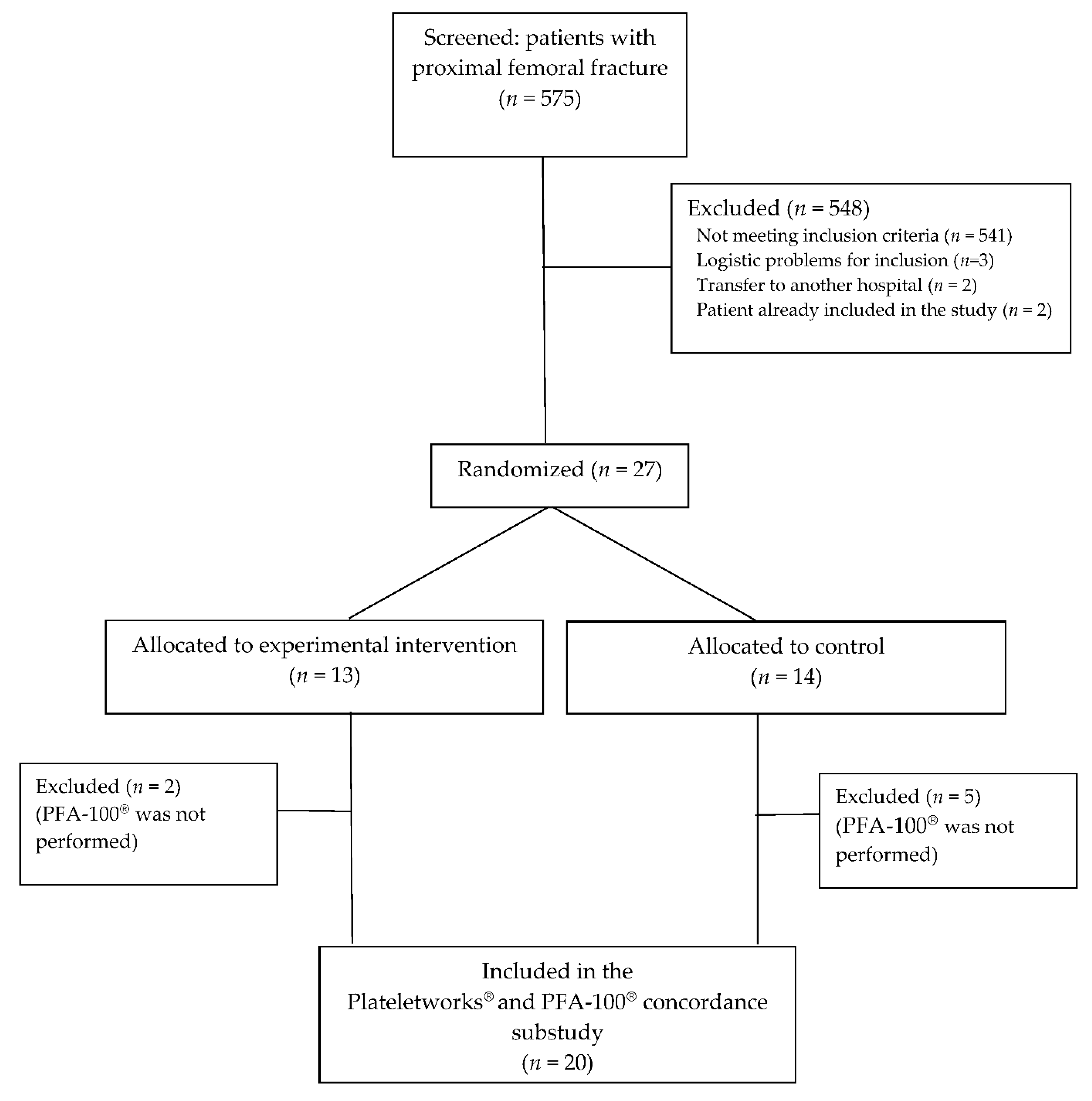
2.1. Patients
2.2. Platelet Function Tests
2.3. Statistical Analysis
3. Results
Agreement between PFA-100® and Plateletworks® Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Agarwal, S. Platelet function testing in cardiac surgery. Transfus. Med. 2016, 26, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Shore-Lesserson, L.; Manspeizer, H.E.; DePerio, M.; Francis, S.; Vela-Cantos, F.; Ergin, M.A. Thromboelastography-guided transfusion algorithm reduces transfusions in complex cardiac surgery. Anesth. Analg. 1999, 88, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Ranucci, M.; Baryshnikova, E.; Soro, G.; Ballotta, A.; De Benedetti, D.; Conti, D.; Surgical and Clinical Outcome Research (SCORE) Group. Multiple electrode whole-blood aggregometry and bleeding in cardiac surgery patients receiving thienopyridines. Ann. Thorac. Surg. 2011, 91, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Ferraris, V.A.; Saha, S.P.; Oestreich, J.H.; Song, H.K.; Rosengart, T.; Reece, T.B.; Mazer, C.D.; Bridges, C.R.; Despotis, G.J.; Jointer, K.; et al. Update to the Society of Thoracic Surgeons guideline on use of antiplatelet drugs in patients having cardiac and noncardiac operations. Ann. Thorac. Surg. 2012, 94, 1761–1781. [Google Scholar] [CrossRef] [PubMed]
- Hvas, A.-M.; Favaloro, E.J. Platelet Function Analyzed by Light Transmission Aggregometry. Methods Mol. Biol. 2017, 1646, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Hayward, C.P.M.; Harrison, P.; Cattaneo, M.; Ortel, T.L.; Rao, A.K. Platelet Physiology Subcommittee of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Platelet function analyzer (PFA)-100 closure time in the evaluation of platelet disorders and platelet function. J. Thromb. Haemost. 2006, 4, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Rafael, A.; Mireia, R.; María, G.J.; Victoria, M.; Angélica, M.; Noèlia, V.; Erica, D.C.; María, A.R.; Francesca, R.; Patricia, G.; et al. Evaluation of a strategy to shorten the time to surgery in patients on antiplatelet therapy with a proximal femur fracture (AFFEcT Study): Study protocol for a multicenter randomized controlled clinical trial. Medicine 2019, 98, e15514. [Google Scholar] [CrossRef] [PubMed]
- Van Veen, J.J.; Nokes, T.J.; Makris, M. The risk of spinal haematoma following neuraxial anaesthesia or lumbar puncture in thrombocytopenic individuals. Br. J. Haematol. 2010, 148, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Nagrebetsky, A.; Al-Samkari, H.; Davis, N.M.; Kuter, D.J.; Wiener-Kronish, J.P. Perioperative thrombocytopenia: Evidence, evaluation, and emerging therapies. Br. J. Anaesth. 2019, 122, 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar] [PubMed]
- Mammen, E.F.; Comp, P.C.; Gosselin, R.; Hoots, W.K.; Kessler, C.M.; Larkin, E.C.; Liles, D.; Nugent, D.J. PFA-100 system: A new method for assessment of platelet dysfunction. Semin. Thromb. Hemost. 1998, 24, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Favaloro, E.J. Clinical utility of the PFA-100. Semin. Thromb. Hemost. 2008, 34, 709–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, P.; Segal, H.; Blasbery, K.; Furtado, C.; Silver, L.; Rothwell, P.M. Screening for aspirin responsiveness after transient ischemic attack and stroke: Comparison of 2 point-of-care platelet function tests with optical aggregometry. Stroke 2005, 36, 1001–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Werkum, J.W.; Kleibeuker, M.; Postma, S.; Bouman, H.J.; Elsenberg, E.H.; Jurriën, M.; Hackeng, C.M. A comparison between the Plateletworks™-assay and light transmittance aggregometry for monitoring the inhibitory effects of clopidogrel. Int. J. Cardiol. 2010, 140, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Paniccia, R.; Martínez, B.; Prisco, D. General aspects of platelet function. In Point-of-Care Tests for Severe Hemorrhage, 1st ed.; Ranucci, M., Simioni, P., Eds.; Springer: Cham, Switzerland, 2016; pp. 44–46. [Google Scholar]
- Zupan, I.P.; Sabovic, M.; Salobir, B.; Ponikvar, J.B.; Cernelc, P.; Lavre, J.; Vujkovac, B. The study of anaemia-related haemostasis impairment in haemodialysis patients by in vitro closure time test. Thromb. Haemost. 2005, 93, 375–379. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Case | Age | Sex | Allocated Group | Antiplatelet Drug | Hb at Admission (g/dL) | Hct at Admission (%) | Time from Blood Extraction to Analysis (min) | Total Platelet Count (×109/L) | Active Platelets Count with PLATELETWORK® (×109/L) | Closure Time with PFA-100®-ADP (s) | Closure Time with PFA-100®EPI (s) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 89 | Woman | Experimental | Clopidogrel | 10.9 | 34 | 9 | 101 | 71 | 88 | 251 |
| 2 | 82 | Man | Control | Clopidogrel | 13.3 | 39 | 7 | 92 | 74 | 249 | 299 |
| 3 | 90 | Woman | Experimental | AAS 300 mg | 13.6 | 41 | 6 | 461 | 53 | 130 | 300 |
| 4 | 81 | Woman | Experimental | Clopidogrel | 11.9 | 33 | 6 | 193 | 50 | 300 | 154 |
| 5 | 81 | Man | Control | AAS 300 mg and Clopidogrel | 9.9 | 30 | 6 | 197 | 88 | 147 | 144 |
| 6 | 89 | Woman | Control | Clopidogrel | 10.1 | 32 | 7 | 146 | 108 | 105 | 285 |
| 7 | 97 | Man | Experimental | Clopidogrel | 10.3 | 30 | 6 | 151 | 126 | 109 | 92 |
| 8 | 91 | Woman | Experimental | AAS 300 mg | 10.3 | 31 | 5 | 212 | 193 | 80 | 143 |
| 9 | 86 | Woman | Experimental | Clopidogrel | 9.5 | 30 | 6 | 269 | 123 | 90 | 119 |
| 10 | 91 | Woman | Control | Clopidogrel | 9.7 | 31 | 4 | 274 | 210 | 126 | 300 |
| 11 | 89 | Woman | Experimental | Clopidogrel | 11.7 | 32 | 8 | 147 | 89 | 124 | 247 |
| 12 | 91 | Woman | Experimental | Clopidogrel | 12.4 | 37 | 11 | 155 | 92 | 97 | 256 |
| 13 | 77 | Man | Control | AAS 300 mg | 10.0 | 30 | 6 | 261 | 166 | 75 | 86 |
| 14 | 83 | Woman | Control | Clopidogrel | 10.2 | 33 | 4 | 198 | 159 | 57 | 94 |
| 15 | 91 | Woman | Control | Clopidogrel | 12.0 | 36 | 5 | 168 | 142 | 79 | 196 |
| 16 | 90 | Woman | Experimental | Clopidogrel | 11.2 | 33 | 4 | 315 | 94 | 69 | 173 |
| 17 | 80 | Man | Experimental | Clopidogrel | 14.2 | 42 | 6 | 187 | 32 | 126 | 300 |
| 18 | 88 | Woman | Control | Clopidogrel | 10.4 | 31 | 6 | 207 | 85 | 36 | 72 |
| 19 | 70 | Man | Experimental | Clopidogrel | 12.9 | 38 | 6 | 249 | 118 | 300 | 254 |
| 20 | 88 | Man | Control | Clopidogrel | 10.8 | 32 | 5 | 89 | 73 | 239 | 155 |
| PFA-100® ADP | PFA-100® EPI | ||||||
|---|---|---|---|---|---|---|---|
| Normal | Pathologic | Kappa Coefficient | Normal | Pathologic | Kappa Coefficient | ||
| PlateletWork® | Normal | 8 | 6 | 0.327 | 8 | 6 | 0.200 |
| Pathologic | 1 | 5 | 2 | 4 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anaya, R.; Rodriguez, M.; Gil, J.M.; Vilalta, N.; Merchan-Galvis, A.; Moral, V.; Mateo, J.; Martinez-Zapata, M.J. Correlation between PlateletWorks® and PFA-100® for Measuring Platelet Function before Urgent Surgery in Patients with Chronic Antiplatelet Therapy. J. Clin. Med. 2021, 10, 255. https://doi.org/10.3390/jcm10020255
Anaya R, Rodriguez M, Gil JM, Vilalta N, Merchan-Galvis A, Moral V, Mateo J, Martinez-Zapata MJ. Correlation between PlateletWorks® and PFA-100® for Measuring Platelet Function before Urgent Surgery in Patients with Chronic Antiplatelet Therapy. Journal of Clinical Medicine. 2021; 10(2):255. https://doi.org/10.3390/jcm10020255
Chicago/Turabian StyleAnaya, Rafael, Mireia Rodriguez, José María Gil, Noelia Vilalta, Angela Merchan-Galvis, Victoria Moral, José Mateo, and María José Martinez-Zapata. 2021. "Correlation between PlateletWorks® and PFA-100® for Measuring Platelet Function before Urgent Surgery in Patients with Chronic Antiplatelet Therapy" Journal of Clinical Medicine 10, no. 2: 255. https://doi.org/10.3390/jcm10020255