
Integrin β Expression as a New Diagnostic Marker for Arteriovenous Thrombosis: A Single-Center Prospective Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Exclusion Criteria
2.3. Flow Cytometry
2.4. Statistical Analysis
3. Results
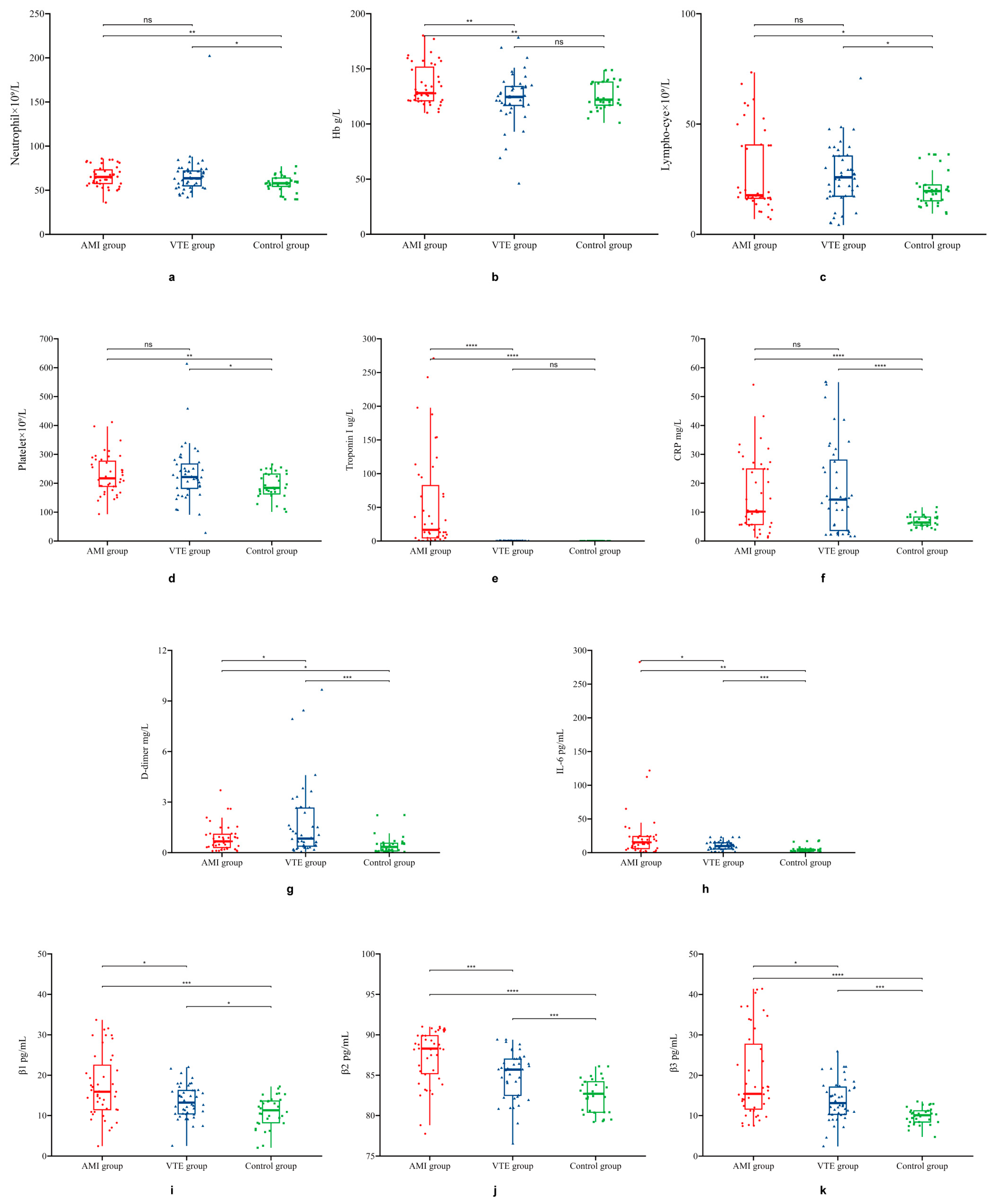
3.1. General Clinical Characteristics and Laboratory Testing Indicators
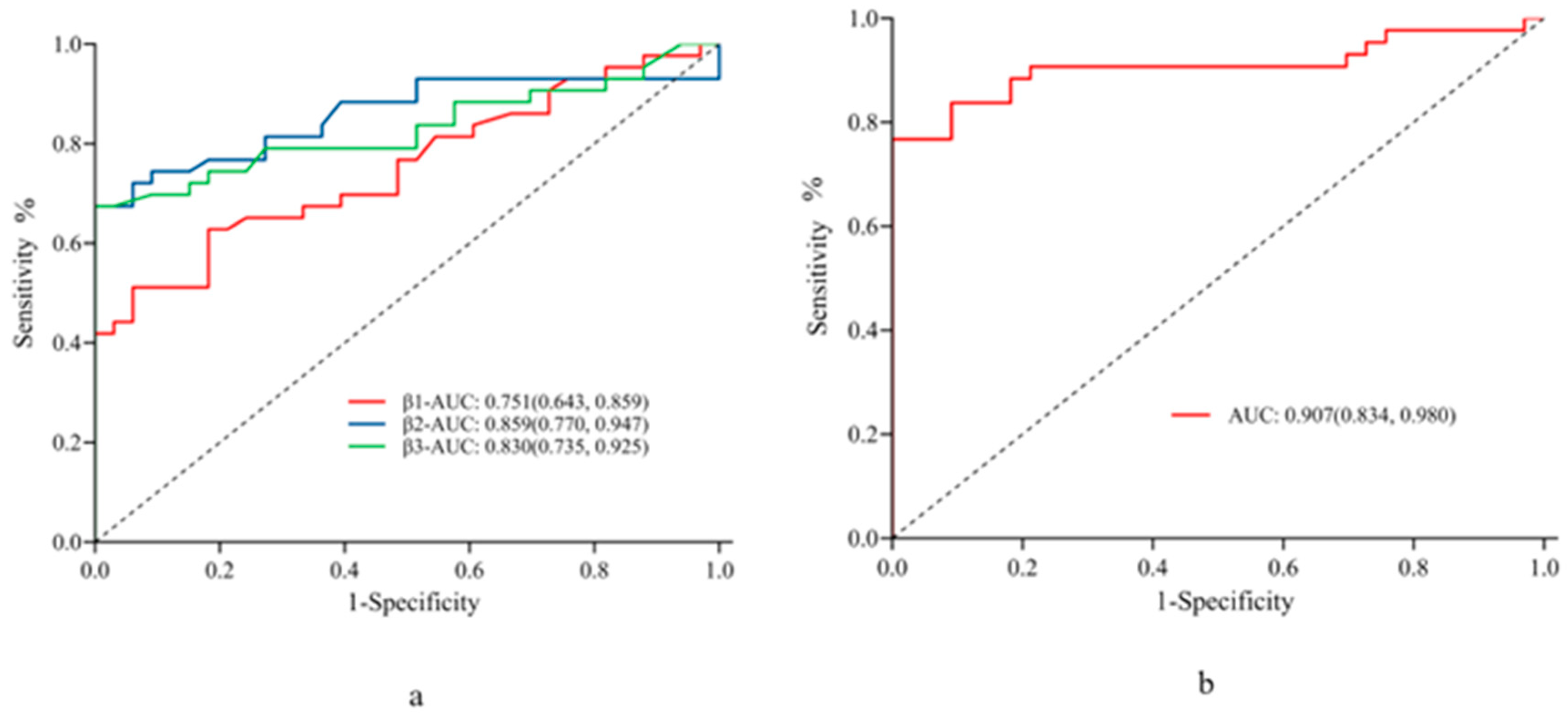
3.2. Factors Influencing Arterial Thrombosis and Diagnostic Performance in AMI
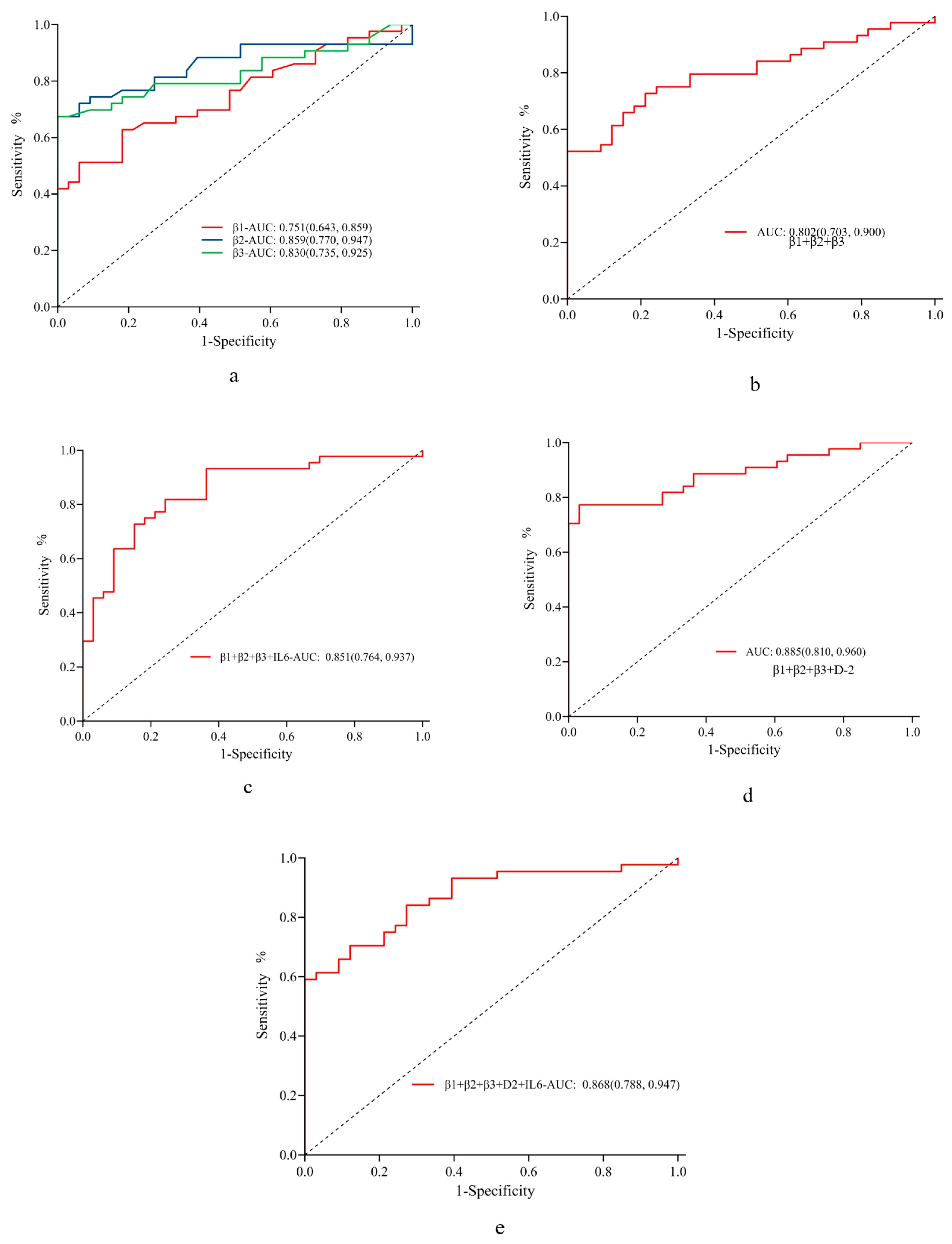
3.3. Factors Influencing Venous Thrombosis and Diagnostic Performance in VTE
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deguchi, H.; Pecheniuk, N.M.; Elias, D.J.; Averell, P.M.; Griffin, J.H. High-density lipoprotein deficiency and dyslipoproteinemia associated with venous thrombosis in men. Circulation 2005, 112, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Prandoni, P.; Bilora, F.; Marchiori, A.; Bernardi, E.; Petrobelli, F.; Lensing, A.W.A.; Prins, M.H.; Girolami, A. An association between atherosclerosis and venous thrombosis. N. Engl. J. Med. 2003, 348, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Kabrhel, C.; Varraso, R.; Goldhaber, S.Z.; Rimm, E.B.; Camargo, C.A. Prospective study of BMI and the risk of pulmonary embolism in women. Obesity 2009, 17, 2040–2046. [Google Scholar] [CrossRef] [PubMed]
- Ageno, W.; Becattini, C.; Brighton, T.; Selby, R.; Kamphuisen, P.W. Cardiovascular risk factors and venous thromboembolism: A meta-analysis. Circulation 2008, 117, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Brighton, T.A.; Eikelboom, J.W.; Mann, K.; Mister, R.; Gallus, A.; Ockelford, P.; Gibbs, H.; Hague, W.; Xavier, D.; Diaz, R.; et al. Low-dose aspirin for preventing recurrent venous thromboembolism. N. Engl. J. Med. 2012, 367, 1979–1987. [Google Scholar] [CrossRef] [PubMed]
- Cavallari, I.; Morrow, D.A.; Creager, M.A.; Olin, J.; Bhatt, D.L.; Steg, P.G.; Storey, R.F.; Cohen, M.; Scirica, B.S.; Piazza, G.; et al. Frequency, predictors, and impact of combined antiplatelet therapy on venous thromboembolism in patients with symptomatic atherosclerosis. Circulation 2018, 137, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Stark, K.; Massberg, S. Interplay between inflammation and thrombosis in cardiovascular pathology. Nat. Rev. Cardiol. 2021, 18, 666–682. [Google Scholar] [CrossRef]
- Steven, S.; Frenis, K.; Oelze, M.; Kalinovic, S.; Kuntic, M.; Bayo Jimenez, M.T.; Vujacic-Mirski, K.; Helmstädter, J.; Kröller-Schön, S.; Münzel, T.; et al. Vascular inflammation and oxidative stress: Major triggers for cardiovascular disease. Oxidative Med. Cell. Longev. 2019, 2019, 7092151. [Google Scholar] [CrossRef]
- Quillard, T.; Araújo, H.A.; Franck, G.; Shvartz, E.; Sukhova, G.; Libby, P. TLR2 and neutrophils potentiate endothelial stress, apoptosis and detachment: Implications for superficial erosion. Eur. Heart J. 2015, 36, 1394–1404. [Google Scholar] [CrossRef]
- Seino, Y.; Ikeda, U.; Ikeda, M.; Yamamoto, K.; Misawa, Y.; Hasegawa, T.; Kano, S.; Shimada, K. Interleukin 6 gene transcripts are expressed in human atherosclerotic lesions. Cytokine 1994, 6, 87–91. [Google Scholar] [CrossRef]
- Goldin, M.; Koulas, I.; Weitz, J.I.; Spyropoulos, A.C. State-of-the-art mini review: Dual-pathway inhibition to reduce arterial and venous thromboembolism. Thromb. Haemost. 2022, 122, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.C.; Castaneda, G.; Li, W.T.; Chen, C.; Shende, N.; Chakladar, J.; Taub, P.R.; Chang, E.Y.; Ongkeko, W.M. COVID-19 severity potentially modulated by cardiovascular-disease-associated immune dysregulation. Viruses 2021, 13, 1018. [Google Scholar] [CrossRef] [PubMed]
- Su, J.H.; Luo, M.Y.; Liang, N.; Gong, S.X.; Chen, W.; Huang, W.Q.; Tian, Y.; Wang, A.P. Interleukin-6: A novel target for cardio-cerebrovascular diseases. Front. Pharmacol. 2021, 12, 745061. [Google Scholar] [CrossRef]
- Franck, G.; Mawson, T.; Sausen, G.; Salinas, M.; Masson, G.S.; Cole, A.; Beltrami-Moreira, M.; Chatzizisis, Y.; Quillard, T.; Tesmenitsky, Y.; et al. Flow perturbation mediates neutrophil recruitment and potentiates endothelial injury via TLR2 in mice: Implications for superficial erosion. Circ. Res. 2017, 121, 31–42. [Google Scholar] [CrossRef]
- Soehnlein, O.; Libby, P. Targeting inflammation in atherosclerosis—From experimental insights to the clinic. Nat. Rev. Drug Discov. 2021, 20, 589–610. [Google Scholar] [CrossRef]
- Kapopara, P.R.; Safikhan, N.S.; Huang, J.L.; Meixner, S.C.; Gonzalez, K.; Loghmani, H.; Ruf, W.; Mast, A.E.; Lei, V.; Pryzdial, E.L.G.; et al. CD248 enhances tissue factor procoagulant function, promoting arterial and venous thrombosis in mouse models. J. Thromb. Haemost. 2021, 19, 1932–1947. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wang, C.; Zhang, L.; Lu, Y.; Duan, Q.; Gong, Z.; Liang, A.; Song, H.; Wang, L. Analysis of the protein-protein interaction networks of differentially expressed genes in pulmonary embolism. Mol. Med. Rep. 2015, 11, 2527–2533. [Google Scholar] [CrossRef]
- Cron, R.Q.; Caricchio, R.; Chatham, W.W. Calming the cytokine storm in COVID-19. Nat. Med. 2021, 27, 1674–1675. [Google Scholar] [CrossRef]
- Calabro, P.; Willerson, J.T.; Yeh, E.T. Inflammatory cytokines stimulated C-reactive protein production by human coronary artery smooth muscle cells. Circulation 2003, 108, 1930–1932. [Google Scholar] [CrossRef]
- Zhou, L.; Mao, Y.; Wang, L.; Jiang, J.; Xu, W.; Xu, J.; Song, H. Comparison of peripheral blood T lymphocyte immune function among venous thromboembolism patients with and without infection and patients with simple infection. Int. J. Clin. Exp. Med. 2015, 8, 6585–6591. [Google Scholar]
- Canobbio, I.; Visconte, C.; Momi, S.; Guidetti, G.F.; Zarà, M.; Canino, J.; Falcinelli, E.; Gresele, P.; Torti, M. Platelet amyloid precursor protein is a modulator of venous thromboembolism in mice. Blood 2017, 130, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Abdelmaseih, R.; Alsamman, M.M.; Faluk, M.; Hasan, S.M. Cardiovascular outcomes with anti-inflammatory therapies: Review of literature. Curr. Probl. Cardiol. 2022, 47, 100840. [Google Scholar] [CrossRef] [PubMed]
- Duan, Q.; Wang, L.; Yang, F.; Li, J.; Song, Y.; Gong, Z.; Li, G.; Song, H.; Zhang, X.; Shen, Z.; et al. Internal relationship between symptomatic venous thromboembolism and risk factors: Up-regulation of integrin β1, β2 and β3 levels. Am. J. Transl. Res. 2015, 7, 624–631. [Google Scholar]
- Song, Y.; Yang, F.; Wang, L.; Duan, Q.; Jin, Y.; Gong, Z. ‘Increased expressions of integrin subunit β1, β2 and β3 in patients with venous thromboembolism: New markers for venous thromboembolism. Int. J. Clin. Exp. Med. 2014, 7, 2578–2584. [Google Scholar] [PubMed]
- Wang, Y.; Gao, H.; Shi, C.; Erhardt, P.W.; Pavlovsky, A.; Soloviev, D.A.; Bledzka, K.; Ustinov, V.; Zhu, L.; Qin, J.; et al. Leukocyte integrin Mac-1 regulates thrombosis via interaction with platelet GPIbα. Nat. Commun. 2017, 8, 15559. [Google Scholar] [CrossRef]
- Estevez, B.; Shen, B.; Du, X. Targeting integrin and integrin signaling in treating thrombosis. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 24–29. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total n = 120 | AMI Group n = 43 | VTE Group n = 44 | Control Group n = 33 | p (Overall) | p (AMI vs. VTE) | p (AMI vs. Control) | p (VTE vs. Control) | |
|---|---|---|---|---|---|---|---|---|
| Age | 66.84 ± 11.94 | 65.21 ± 12.29 | 67.07 ± 13.22 | 68.67 ± 9.51 | 0.455 | 0.499 | 0.171 | 0.539 |
| Number of men (%) | 59 (49.17%) | 25 (58.14%) | 20 (45.45%) | 14 (42.42%) | 0.328 | 0.332 | 0.260 | 0.974 |
| Neutrophil | 63.72 ± 17.15 | 65.40 ± 11.82 | 66.86 ± 23.84 | 57.37 ± 9.39 | 0.039 | 0.717 | 0.001 | 0.019 |
| Hb | 128.12 ± 19.80 | 135.14 ± 18.27 | 123.14 ± 23.58 | 125.61 ± 12.87 | 0.012 | 0.009 | 0.009 | 0.559 |
| Lymphocyte | 25.70 ± 15.19 | 28.75 ± 19.63 | 26.34 ± 13.62 | 20.87 ± 8.09 | 0.075 | 0.509 | 0.020 | 0.031 |
| Platelet | 219.31 ± 76.06 | 229.40 ± 67.81 | 231.11 ± 95.06 | 190.42 ± 46.38 | 0.036 | 0.923 | 0.004 | 0.016 |
| Troponin I | 21.00 ± 51.32 | 53.71 ± 70.98 | 0.02 ± 0.04 | 0.01 ± 0.01 | <0.001 | <0.001 | <0.001 | 0.265 |
| CRP | 14.22 ± 13.14 | 15.78 ± 12.61 | 18.15 ± 16.15 | 6.93 ± 1.90 | <0.001 | 0.446 | <0.001 | <0.001 |
| D-dimer | 1.08 ± 1.54 | 0.86 ± 0.77 | 1.76 ± 2.23 | 0.46 ± 0.53 | <0.001 | 0.014 | 0.011 | 0.001 |
| IL-6 | 14.58 ± 29.92 | 26.51 ± 47.30 | 10.10 ± 6.46 | 5.00 ± 4.81 | 0.003 | 0.029 | 0.005 | <0.001 |
| Integrin β1 | 14.20 ± 6.25 | 17.38 ± 7.93 | 13.53 ± 4.14 | 10.96 ± 3.84 | <0.001 | 0.006 | <0.001 | 0.006 |
| Integrin β2 | 84.70 ± 4.12 | 86.98 ± 4.07 | 84.17 ± 4.26 | 82.44 ± 2.08 | <0.001 | 0.002 | <0.001 | 0.021 |
| Integrin β3 | 14.84 ± 8.14 | 19.70 ± 10.69 | 13.80 ± 4.99 | 9.90 ± 2.05 | <0.001 | 0.002 | <0.001 | <0.001 |
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| Hb | 1.040 (1.009, 1.077) | 0.018 |
| Neutrophil | 1.073 (1.026, 1.132) | 0.004 |
| Lymphocyte | 0.938(0.891, 0.982) | 0.009 |
| Platelet | 1.012 (1.004, 1.022) | 0.010 |
| CRP | 1.171 (1.074, 1.330) | 0.003 |
| D-dimer | 2.952 (1.282, 8.629) | 0.025 |
| IL-6 | 1.169 (1.083, 1.288) | <0.001 |
| Integrin β1 | 1.205 (1.094, 1.366) | 0.001 |
| Integrin β2 | 1.485 (1.257, 1.826) | <0.001 |
| Integrin β3 | 1.477 (1.221, 1.892) | <0.001 |
| Variable | Cut-Off Value | AUC (95% CI) | p-Value | Sensitivity (95% CI) | Specificity (95% CI) | Accuracy (95% CI) | Positive Predictive Value (95% CI) | Negative Predictive Value (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Integrin β1 | 15.700 | 0.751 (0.643, 0.859) | <0.001 | 0.512 (0.362, 0.661) | 0.939 (0.858, 1.000) | 0.697 (0.692, 0.703) | 0.917 (0.806, 1.027) | 0.596 (0.463, 0.730) |
| Integrin β2 | 86.150 | 0.859 (0.770, 0.947) | <0.001 | 0.674 (0.534, 0.814) | 1.000 (1.000, 1.000) | 0.816 (0.812, 0.820) | 1.000 (1.000, 1.000) | 0.702 (0.571, 0.833) |
| Integrin β3 | 13.550 | 0.830 (0.735, 0.925) | <0.001 | 0.674 (0.534, 0.814) | 1.000 (1.000, 1.000) | 0.816 (0.812, 0.820) | 1.000 (1.000, 1.000) | 0.702 (0.571, 0.833) |
| Variables | OR (95% CI) | p-Value |
|---|---|---|
| Hb | 0.993 (0.969, 1.017) | 0.584 |
| Neutrophil | 1.058 (1.013, 1.111) | 0.017 |
| Lymphocyte | 0.960 (0.919, 0.998) | 0.051 |
| Platelet | 1.008 (1.001, 1.017) | 0.034 |
| CRP | 1.138 (1.059, 1.262) | 0.004 |
| D-dimer | 3.187 (1.604, 8.471) | 0.006 |
| IL-6 | 1.176 (1.075, 1.309) | 0.001 |
| Integrin β1 | 1.178 (1.046, 1.348) | 0.010 |
| Integrin β2 | 1.156 (1.012, 1.345) | 0.042 |
| Integrin β3 | 1.336 (1.150, 1.617) | 0.001 |
| Variable | Cut-Off Value | AUC (95% CI) | p-Value | Sensitivity (95% CI) | Specificity (95% CI) | Accuracy (95% CI) | Positive Predictive Value (95% CI) | Negative Predictive Value (95% CI) |
|---|---|---|---|---|---|---|---|---|
| D-2 | 0.605 | 0.758 (0.651, 0.864) | <0.001 | 0.636 (0.494, 0.779) | 0.788 (0.648, 0.927) | 0.701 (0.696, 0.707) | 0.800 (0.667, 0.933) | 0.619 (0.472, 0.766) |
| β1 | 14.300 | 0.666 (0.546, 0.787) | 0.007 | 0.477 (0.330, 0.625) | 0.818 (0.687, 0.950) | 0.623 (0.617, 0.629) | 0.778 (0.621, 0.935) | 0.540 (0.402, 0.678) |
| β2 | 85.400 | 0.722 (0.606, 0.838) | <0.001 | 0.545 (0.398, 0.693) | 0.939 (0.858, 1.000) | 0.714 (0.709, 0.719) | 0.923 (0.821, 1.026) | 0.608 (0.474, 0.742) |
| β3 | 13.550 | 0.758 (0.650, 0.866) | <0.001 | 0.500 (0.352, 0.648) | 1.000 (1.000, 1.000) | 0.714 (0.709, 0.719) | 1.000 (1.000, 1.000) | 0.600 (0.471, 0.729) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xi, Y.; Mao, Y.; Yang, F.; Xi, P.; Zhu, W.; Song, Y.; Yan, W.; Liao, X.; Zhou, L. Integrin β Expression as a New Diagnostic Marker for Arteriovenous Thrombosis: A Single-Center Prospective Study. J. Cardiovasc. Dev. Dis. 2023, 10, 461. https://doi.org/10.3390/jcdd10110461
Xi Y, Mao Y, Yang F, Xi P, Zhu W, Song Y, Yan W, Liao X, Zhou L. Integrin β Expression as a New Diagnostic Marker for Arteriovenous Thrombosis: A Single-Center Prospective Study. Journal of Cardiovascular Development and Disease. 2023; 10(11):461. https://doi.org/10.3390/jcdd10110461
Chicago/Turabian StyleXi, Yan, Yu Mao, Fan Yang, Peng Xi, Wei Zhu, Yanli Song, Wenwen Yan, Xudong Liao, and Lin Zhou. 2023. "Integrin β Expression as a New Diagnostic Marker for Arteriovenous Thrombosis: A Single-Center Prospective Study" Journal of Cardiovascular Development and Disease 10, no. 11: 461. https://doi.org/10.3390/jcdd10110461