
MRI/RNA-Seq-Based Radiogenomics and Artificial Intelligence for More Accurate Staging of Muscle-Invasive Bladder Cancer
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
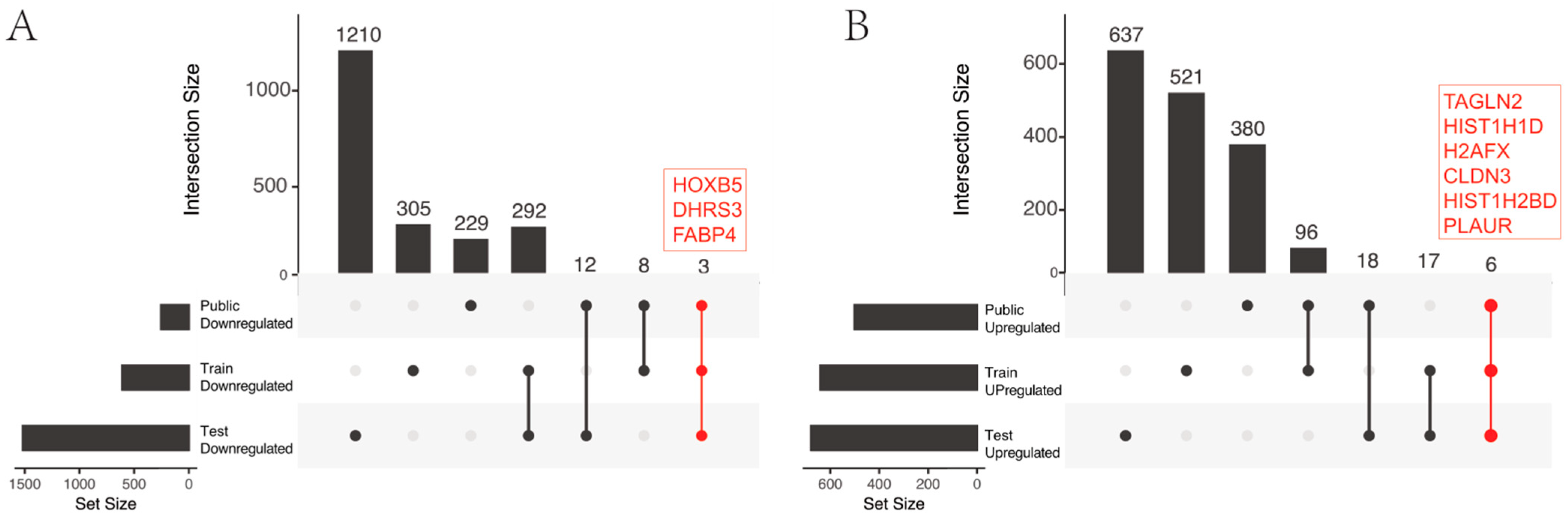
2.1. Identification of Genomics Features
2.2. Identification of Radiomics Features
2.3. Integration of Radiomics and Genomics Features Improves Bladder Cancer Staging
3. Discussion
Limitations and Future Work
4. Materials and Methods
4.1. Study Data
4.2. Radiogenomic Staging of Bladder Cancer
4.2.1. Genomic Analysis of MIBC Staging
4.2.2. Radiomic Analysis of Bladder Cancer Staging
4.2.3. Radiogenomic Modeling for Bladder Cancer Staging
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.M.; Krapcho, M.; Garshell, J.; Neyman, N.; Altekruse, S.F.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; et al. SEER Cancer Statistics Review, 1975–2010. Available online: http://seer.cancer.gov/csr/1975_2010/ (accessed on 1 May 2014).
- Brausi, M.; Witjes, J.A.; Lamm, D.; Persad, R.; Palou, J.; Colombel, M.; Buckley, R.; Soloway, M.; Akaza, H.; Bohle, A. A review of current guidelines and best practice recommendations for the management of nonmuscle invasive bladder cancer by the International Bladder Cancer Group. J. Urol. 2011, 186, 2158–2167. [Google Scholar] [CrossRef] [PubMed]
- Stenzl, A.; Cowan, N.C.; De Santis, M.; Kuczyk, M.A.; Merseburger, A.S.; Ribal, M.J.; Sherif, A.; Witjes, J.A.; European Association of Urology. Treatment of muscle-invasive and metastatic bladder cancer: Update of the EAU guidelines. Eur. Urol. 2011, 59, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Calabro, F.; Sternberg, C.N. Metastatic bladder cancer: Anything new? Curr. Opin. Support. Palliat. Care 2012, 6, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M.; et al. Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1054 patients. J. Clin. Oncol. 2001, 19, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Dhar, N.B.; Klein, E.A.; Reuther, A.M.; Thalmann, G.N.; Madersbacher, S.; Studer, U.E. Outcome after radical cystectomy with limited or extended pelvic lymph node dissection. J. Urol. 2008, 179, 873–878; discussion 878. [Google Scholar] [CrossRef] [PubMed]
- Efstathiou, J.A.; Spiegel, D.Y.; Shipley, W.U.; Heney, N.M.; Kaufman, D.S.; Niemierko, A.; Coen, J.J.; Skowronski, R.Y.; Paly, J.J.; McGovern, F.J.; et al. Long-term outcomes of selective bladder preservation by combined-modality therapy for invasive bladder cancer: The MGH experience. Eur. Urol. 2012, 61, 705–711. [Google Scholar] [CrossRef]
- Mak, R.H.; Hunt, D.; Shipley, W.U.; Efstathiou, J.A.; Tester, W.J.; Hagan, M.P.; Kaufman, D.S.; Heney, N.M.; Zietman, A.L. Long-term outcomes in patients with muscle-invasive bladder cancer after selective bladder-preserving combined-modality therapy: A pooled analysis of Radiation Therapy Oncology Group protocols 8802, 8903, 9506, 9706, 9906, and 0233. J. Clin. Oncol. 2014, 32, 3801–3809. [Google Scholar] [CrossRef]
- Nepple, K.G.; O’Donnell, M.A. The optimal management of T1 high-grade bladder cancer. Can. Urol. Assoc. J. 2009, 3, S188–S192. [Google Scholar] [CrossRef]
- Batista, R.; Vinagre, N.; Meireles, S.; Vinagre, J.; Prazeres, H.; Leao, R.; Maximo, V.; Soares, P. Biomarkers for Bladder Cancer Diagnosis and Surveillance: A Comprehensive Review. Diagnostics 2020, 10, 39. [Google Scholar] [CrossRef]
- Kamoun, A.; de Reynies, A.; Allory, Y.; Sjodahl, G.; Robertson, A.G.; Seiler, R.; Hoadley, K.A.; Groeneveld, C.S.; Al-Ahmadie, H.; Choi, W.; et al. A Consensus Molecular Classification of Muscle-invasive Bladder Cancer. Eur. Urol. 2020, 77, 420–433. [Google Scholar] [CrossRef] [PubMed]
- Chamie, K.; Ballon-Landa, E.; Bassett, J.C.; Daskivich, T.J.; Leventhal, M.; Deapen, D.; Litwin, M.S. Quality of diagnostic staging in patients with bladder cancer: A process-outcomes link. Cancer 2015, 121, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Ozaydin, S.; Atas, E.; Karadurmus, N.; Emirzeoglu, L.; Arpaci, F. Outcomes of bladder preservation therapy on survival in patients with muscle-invasive bladder cancer. Arch. Esp. Urol. 2020, 73, 41–46. [Google Scholar] [PubMed]
- Wang, H.; Luo, C.; Zhang, F.; Guan, J.; Li, S.; Yao, H.; Chen, J.; Luo, J.; Chen, L.; Guo, Y. Multiparametric MRI for Bladder Cancer: Validation of VI-RADS for the Detection of Detrusor Muscle Invasion. Radiology 2019, 291, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Trivizakis, E.; Papadakis, G.Z.; Souglakos, I.; Papanikolaou, N.; Koumakis, L.; Spandidos, D.A.; Tsatsakis, A.; Karantanas, A.H.; Marias, K. Artificial intelligence radiogenomics for advancing precision and effectiveness in oncologic care (Review). Int. J. Oncol. 2020, 57, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Saxena, S.; Jena, B.; Gupta, N.; Das, S.; Sarmah, D.; Bhattacharya, P.; Nath, T.; Paul, S.; Fouda, M.M.; Kalra, M.; et al. Role of Artificial Intelligence in Radiogenomics for Cancers in the Era of Precision Medicine. Cancers 2022, 14, 2860. [Google Scholar] [CrossRef]
- Qureshi, T.A.; Gaddam, S.; Wachsman, A.M.; Wang, L.; Azab, L.; Asadpour, V.; Chen, W.; Xie, Y.; Wu, B.; Pandol, S.J.; et al. Predicting pancreatic ductal adenocarcinoma using artificial intelligence analysis of pre-diagnostic computed tomography images. Cancer Biomark. 2022, 33, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, A.; Sahu, A.; Ashtekar, R.; Kulkarni, T.; Shukla, S.; Agarwal, U.; Bhattacharya, K. Glioma radiogenomics and artificial intelligence: Road to precision cancer medicine. Clin. Radiol. 2023, 78, 137–149. [Google Scholar] [CrossRef]
- Ninatti, G.; Kirienko, M.; Neri, E.; Sollini, M.; Chiti, A. Imaging-Based Prediction of Molecular Therapy Targets in NSCLC by Radiogenomics and AI Approaches: A Systematic Review. Diagnostics 2020, 10, 359. [Google Scholar] [CrossRef]
- Perez-Johnston, R.; Araujo-Filho, J.A.; Connolly, J.G.; Caso, R.; Whiting, K.; Tan, K.S.; Zhou, J.; Gibbs, P.; Rekhtman, N.; Ginsberg, M.S.; et al. CT-based Radiogenomic Analysis of Clinical Stage I Lung Adenocarcinoma with Histopathologic Features and Oncologic Outcomes. Radiology 2022, 303, 664–672. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.; Guo, C.; Xie, X.; Liang, S.; Zhang, R.; Pang, W.; Huang, L. Cancer genotypes prediction and associations analysis from imaging phenotypes: A survey on radiogenomics. Biomark. Med. 2020, 14, 1151–1164. [Google Scholar] [CrossRef] [PubMed]
- Gallivanone, F.; Bertoli, G.; Porro, D. Radiogenomics, Breast Cancer Diagnosis and Characterization: Current Status and Future Directions. Methods Protoc. 2022, 5, 78. [Google Scholar] [CrossRef] [PubMed]
- Flaig, T.W.; Spiess, P.E.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Chang, S.; Downs, T.M.; Efstathiou, J.A.; Friedlander, T.; et al. Bladder Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc Netw. 2020, 18, 329–354. [Google Scholar] [CrossRef] [PubMed]
- Trinh, T.W.; Glazer, D.I.; Sadow, C.A.; Sahni, V.A.; Geller, N.L.; Silverman, S.G. Bladder cancer diagnosis with CT urography: Test characteristics and reasons for false-positive and false-negative results. Abdom. Radiol. 2018, 43, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Tan, C.H.; Faria, S.C.; Kundra, V. Role of Imaging in the Local Staging of Urothelial Carcinoma of the Bladder. AJR Am. J. Roentgenol. 2017, 208, 1193–1205. [Google Scholar] [CrossRef] [PubMed]
- Sadow, C.A.; Silverman, S.G.; O’Leary, M.P.; Signorovitch, J.E. Bladder cancer detection with CT urography in an Academic Medical Center. Radiology 2008, 249, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Barentsz, J.O.; Jager, G.J.; Witjes, J.A.; Ruijs, J.H. Primary staging of urinary bladder carcinoma: The role of MRI and a comparison with CT. Eur. Radiol. 1996, 6, 129–133. [Google Scholar] [CrossRef]
- National Cancer Institute. Bladder Cancer Stages. Available online: https://www.cancer.gov/types/bladder/stages (accessed on 1 November 2023).
- Aldousari, S.; Kassouf, W. Update on the management of non-muscle invasive bladder cancer. Can. Urol. Assoc. J. 2010, 4, 56–64. [Google Scholar] [CrossRef]
- Babjuk, M.; Bohle, A.; Burger, M.; Capoun, O.; Cohen, D.; Comperat, E.M.; Hernandez, V.; Kaasinen, E.; Palou, J.; Roupret, M.; et al. EAU Guidelines on Non-Muscle-invasive Urothelial Carcinoma of the Bladder: Update 2016. Eur. Urol. 2017, 71, 447–461. [Google Scholar] [CrossRef]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Rancati, T.; Lee, S.; Oh, J.H.; Kerns, S.L.; Scott, J.G.; Schwartz, R.; Kim, S.; Rosenstein, B.S. Machine Learning and Radiogenomics: Lessons Learned and Future Directions. Front. Oncol. 2018, 8, 228. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Noon, A.P.; Aguiar Cabeza, E.; Shen, J.; Kuk, C.; Ilczynski, C.; Ni, R.; Sukhu, B.; Chan, K.; Barbosa-Morais, N.L.; et al. Next-generation RNA sequencing of archival formalin-fixed paraffin-embedded urothelial bladder cancer. Eur. Urol. 2014, 66, 982–986. [Google Scholar] [CrossRef] [PubMed]
- Bondaruk, J.; Jaksik, R.; Wang, Z.; Cogdell, D.; Lee, S.; Chen, Y.; Dinh, K.N.; Majewski, T.; Zhang, L.; Cao, S.; et al. The origin of bladder cancer from mucosal field effects. iScience 2022, 25, 104551. [Google Scholar] [CrossRef] [PubMed]
- Robertson, A.G.; Kim, J.; Al-Ahmadie, H.; Bellmunt, J.; Guo, G.; Cherniack, A.D.; Hinoue, T.; Laird, P.W.; Hoadley, K.A.; Akbani, R.; et al. Comprehensive Molecular Characterization of Muscle-Invasive Bladder Cancer. Cell 2017, 171, 540–556. [Google Scholar] [CrossRef]
- Gouin, K.H.; Ing, N.; Plummer, J.T.; Rosser, C.J.; Ben Cheikh, B.; Oh, C.; Chen, S.S.; Chan, K.S.; Furuya, H.; Tourtellotte, W.G.; et al. An N-Cadherin 2 expressing epithelial cell subpopulation predicts response to surgery, chemotherapy and immunotherapy in bladder cancer. Nat. Commun. 2021, 12, 4906. [Google Scholar] [CrossRef]
- Umutlu, L.; Nensa, F.; Demircioglu, A.; Antoch, G.; Herrmann, K.; Forsting, M.; Grueneisen, J.S. Radiomics Analysis of Multiparametric PET/MRI for N- and M-Staging in Patients with Primary Cervical Cancer. Rofo 2020, 192, 754–763. [Google Scholar] [CrossRef]
- Liu, Q.; Li, J.; Xin, B.; Sun, Y.; Feng, D.; Fulham, M.J.; Wang, X.; Song, S. (18)F-FDG PET/CT Radiomics for Preoperative Prediction of Lymph Node Metastases and Nodal Staging in Gastric Cancer. Front. Oncol. 2021, 11, 723345. [Google Scholar] [CrossRef]
- Lin, X.; Zhao, S.; Jiang, H.; Jia, F.; Wang, G.; He, B.; Jiang, H.; Ma, X.; Li, J.; Shi, Z. A radiomics-based nomogram for preoperative T staging prediction of rectal cancer. Abdom. Radiol. 2021, 46, 4525–4535. [Google Scholar] [CrossRef]
- Huang, Y.; Liu, Z.; He, L.; Chen, X.; Pan, D.; Ma, Z.; Liang, C.; Tian, J.; Liang, C. Radiomics Signature: A Potential Biomarker for the Prediction of Disease-Free Survival in Early-Stage (I or II) Non-Small Cell Lung Cancer. Radiology 2016, 281, 947–957. [Google Scholar] [CrossRef]
- Xu, Y.; Ju, L.; Tong, J.; Zhou, C.M.; Yang, J.J. Machine Learning Algorithms for Predicting the Recurrence of Stage IV Colorectal Cancer After Tumor Resection. Sci. Rep. 2020, 10, 2519. [Google Scholar] [CrossRef] [PubMed]
- Cascianelli, S.; Molineris, I.; Isella, C.; Masseroli, M.; Medico, E. Machine learning for RNA sequencing-based intrinsic subtyping of breast cancer. Sci. Rep. 2020, 10, 14071. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Classifier | Validation (DataN) | ||
|---|---|---|---|
| Sen. | Spe. | Acc. | |
| NB | 0.94 | 0.88 | 0.92 |
| SVM | 0.88 | 0.78 | 0.83 |
| DT | 0.89 | 0.72 | 0.80 |
| KNN | 0.78 | 0.72 | 0.75 |
| LR | 0.72 | 0.78 | 0.75 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qureshi, T.A.; Chen, X.; Xie, Y.; Murakami, K.; Sakatani, T.; Kita, Y.; Kobayashi, T.; Miyake, M.; Knott, S.R.V.; Li, D.; et al. MRI/RNA-Seq-Based Radiogenomics and Artificial Intelligence for More Accurate Staging of Muscle-Invasive Bladder Cancer. Int. J. Mol. Sci. 2024, 25, 88. https://doi.org/10.3390/ijms25010088
Qureshi TA, Chen X, Xie Y, Murakami K, Sakatani T, Kita Y, Kobayashi T, Miyake M, Knott SRV, Li D, et al. MRI/RNA-Seq-Based Radiogenomics and Artificial Intelligence for More Accurate Staging of Muscle-Invasive Bladder Cancer. International Journal of Molecular Sciences. 2024; 25(1):88. https://doi.org/10.3390/ijms25010088
Chicago/Turabian StyleQureshi, Touseef Ahmad, Xingyu Chen, Yibin Xie, Kaoru Murakami, Toru Sakatani, Yuki Kita, Takashi Kobayashi, Makito Miyake, Simon R. V. Knott, Debiao Li, and et al. 2024. "MRI/RNA-Seq-Based Radiogenomics and Artificial Intelligence for More Accurate Staging of Muscle-Invasive Bladder Cancer" International Journal of Molecular Sciences 25, no. 1: 88. https://doi.org/10.3390/ijms25010088