
Association between HLA DNA Variants and Long-Term Response to Anti-TNF Drugs in a Spanish Pediatric Inflammatory Bowel Disease Cohort
 , , , , , , , , , add
Show full author list
, , , , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Results
2.1. Patients
2.2. Genotyping and Frequencies
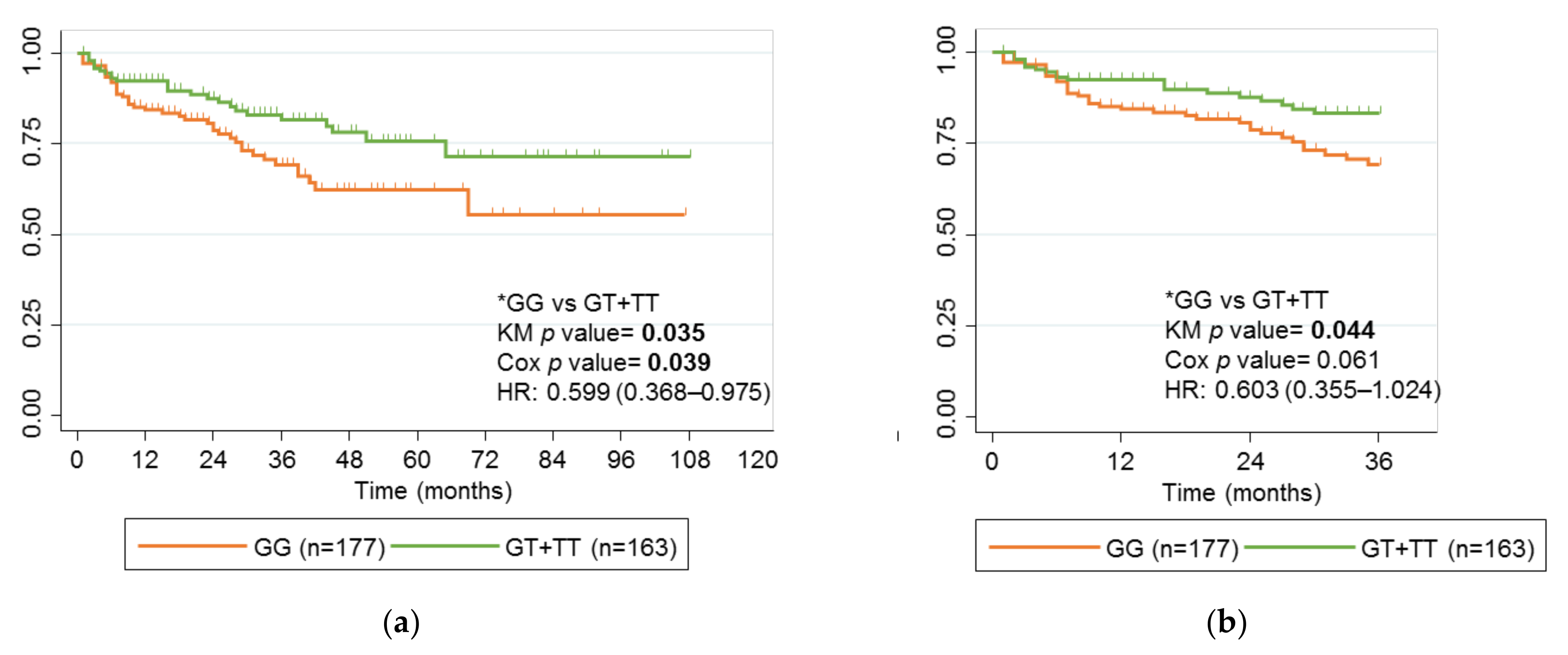
2.3. Association of rs2097432 with Response to Anti-TNF Drugs
2.4. Association between rs2395185 and Response to Anti-TNF Drugs
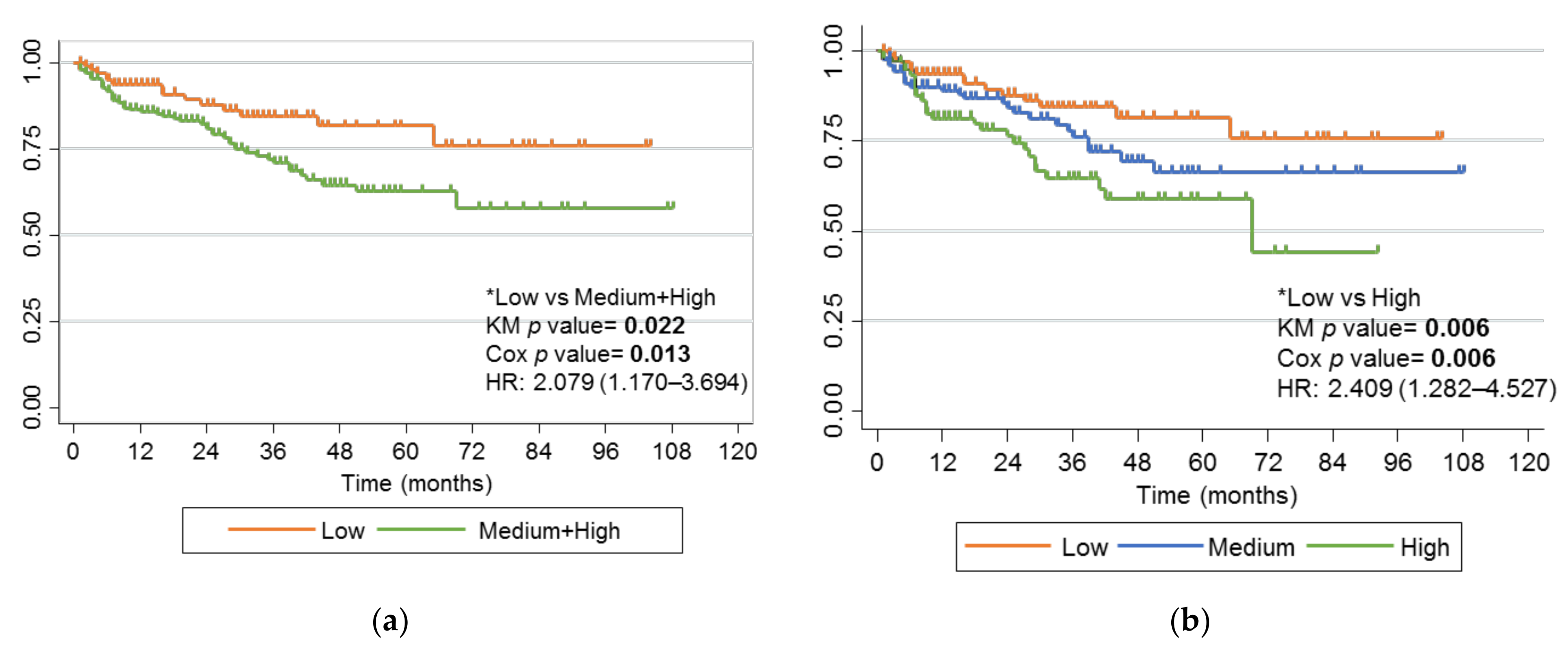
2.5. Haplotypes of rs2395185 and rs2097432 with Response to Anti-TNF Drugs
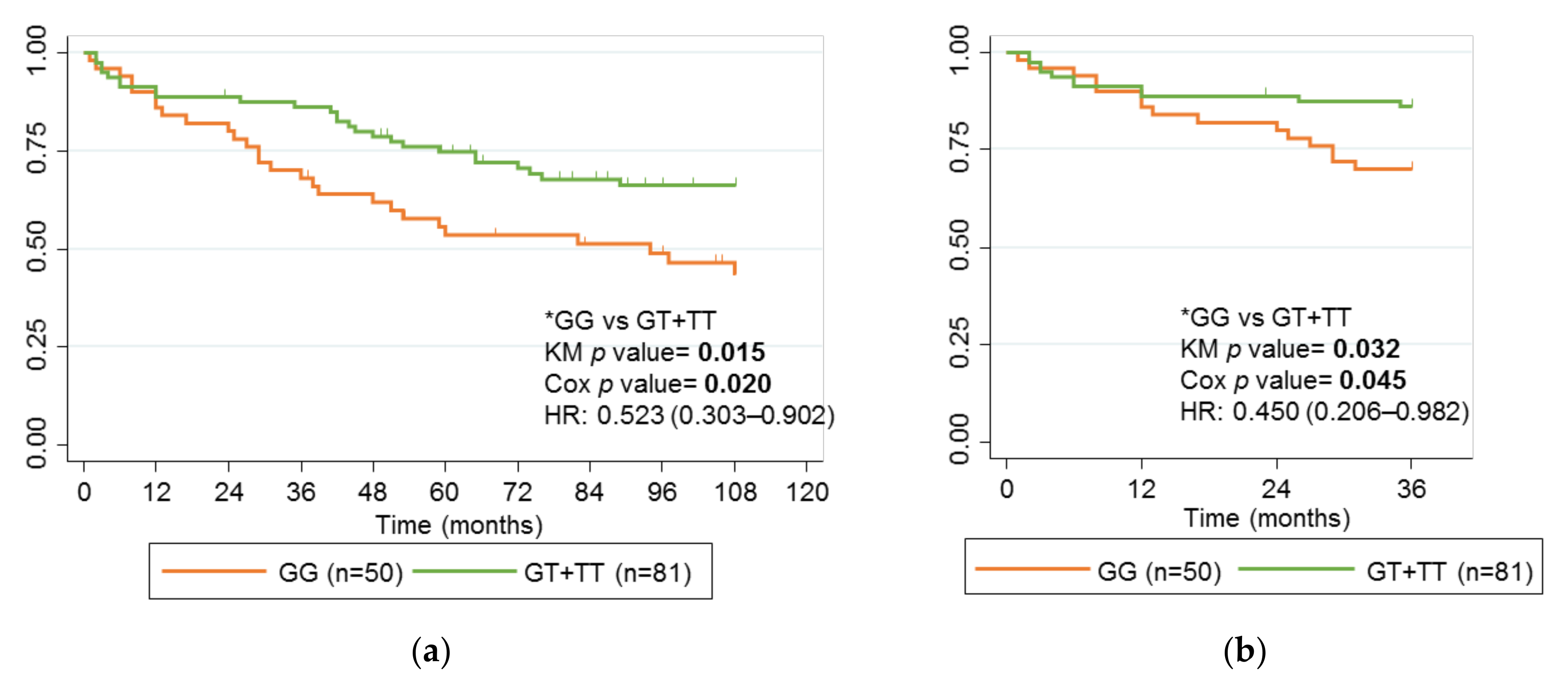
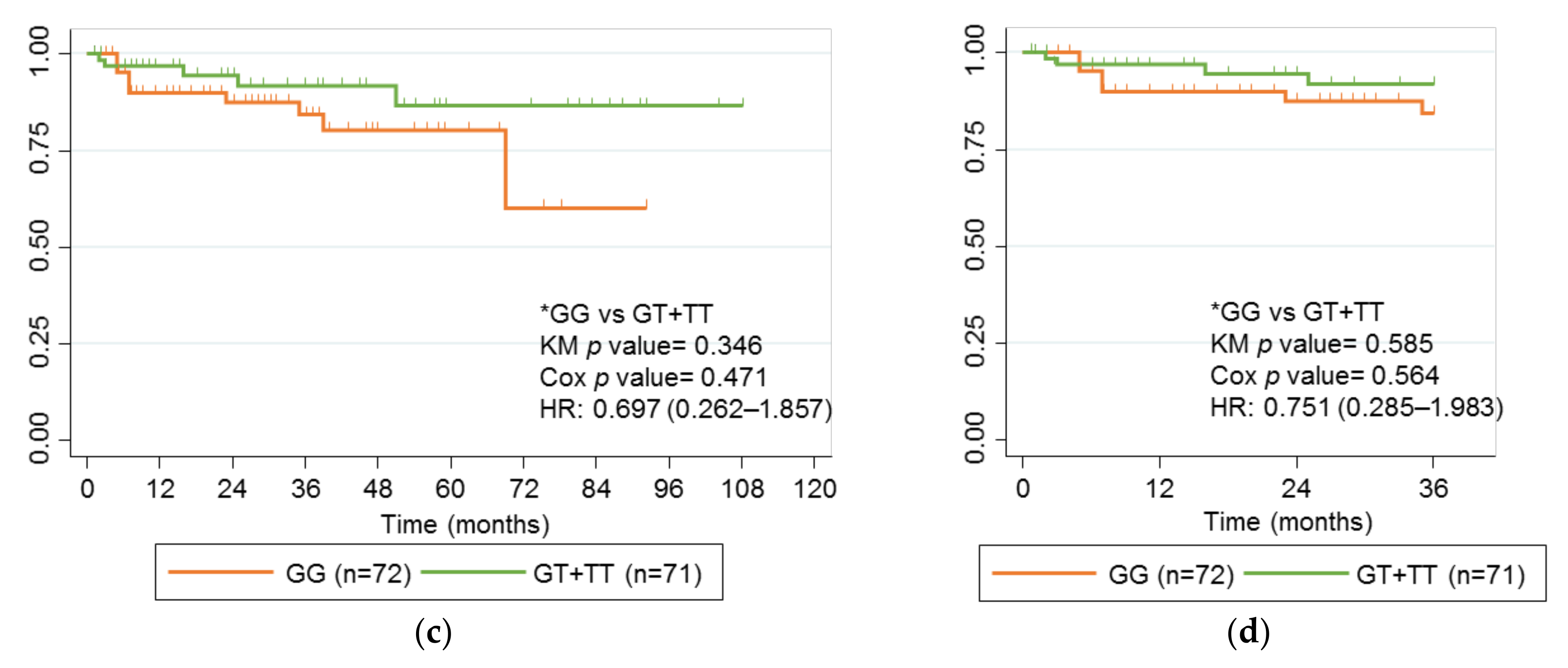
2.6. Comparison of Children with Adults with Crohn’s Disease and Treated with IFX
3. Discussion
4. Materials and Methods
4.1. Study Design and Patient Characteristics
4.2. DNA Isolation and Genotyping
4.3. Statistical Analysis
4.4. Ethics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, S.C.; Ferry, G.D. Inflammatory bowel diseases in pediatric and adolescent patients: Clinical, therapeutic, and psychosocial considerations. Gastroenterology 2004, 126, 1550–1560. [Google Scholar] [CrossRef] [PubMed]
- Jeong, D.Y.; Kim, S.; Son, M.J.; Son, C.Y.; Kim, J.Y.; Kronbichler, A.; Lee, K.H.; Shin, J. Il Induction and maintenance treatment of inflammatory bowel disease: A comprehensive review. Autoimmun. Rev. 2019, 18, 439–454. [Google Scholar] [CrossRef]
- Salvador-Martín, S.; López-Cauce, B.; Nuñez, O.; Laserna-Mendieta, E.J.; García, M.I.; Lobato, E.; Abarca-Zabalía, J.; Sanjurjo-Saez, M.; Lucendo, A.J.; Marín-Jiménez, I.; et al. Genetic predictors of long-term response and trough levels of infliximab in crohn’s disease. Pharmacol. Res. 2019, 149, 104478. [Google Scholar] [CrossRef] [PubMed]
- Salvador-Martín, S.; Bossacoma, F.; Pujol-Muncunill, G.; Navas-López, V.M.; Gallego-Fernández, C.; Viada, J.; Muñoz-Codoceo, R.; Magallares, L.; Martínez-Ojinaga, E.; Moreno-Álvarez, A.; et al. Genetic Predictors of Long-term Response to Antitumor Necrosis Factor Agents in Pediatric Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2020, 71, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Jongsma, M.M.E.; Winter, D.A.; Huynh, H.Q.; Norsa, L.; Hussey, S.; Kolho, K.-L.; Bronsky, J.; Assa, A.; Cohen, S.; Lev-Tzion, R.; et al. Infliximab in young paediatric IBD patients: It is all about the dosing. Eur. J. Pediatr. 2020, 179, 1935–1944. [Google Scholar] [CrossRef] [PubMed]
- Salvador-Martín, S.; Melgarejo-Ortuño, A.; López-Fernández, L.A. Biomarkers for Optimization and Personalization of Anti-TNFs in Pediatric Inflammatory Bowel Disease. Pharmaceutics 2021, 13, 1786. [Google Scholar] [CrossRef]
- Ungar, B.; Levy, I.; Yavne, Y.; Yavzori, M.; Picard, O.; Fudim, E.; Loebstein, R.; Chowers, Y.; Eliakim, R.; Kopylov, U.; et al. Optimizing Anti-TNF-α Therapy: Serum Levels of Infliximab and Adalimumab Are Associated With Mucosal Healing in Patients With Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2016, 14, 550–557.e2. [Google Scholar] [CrossRef] [Green Version]
- Ding, N.S.; Hart, A.; De Cruz, P. Systematic review: Predicting and optimising response to anti-TNF therapy in Crohn’s disease—Algorithm for practical management. Aliment. Pharmacol. Ther. 2016, 43, 30–51. [Google Scholar] [CrossRef]
- Naviglio, S.; Giuffrida, P.; Stocco, G.; Lenti, M.V.; Ventura, A.; Corazza, G.R.; Di Sabatino, A. How to predict response to anti-tumour necrosis factor agents in inflammatory bowel disease. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 797–810. [Google Scholar] [CrossRef]
- Membrive Jiménez, C.; Pérez Ramírez, C.; Sánchez Martín, A.; Vieira Maroun, S.; Arias Santiago, S.A.; Ramírez Tortosa, M.D.C.; Jiménez Morales, A. Influence of Genetic Polymorphisms on Response to Biologics in Moderate-to-Severe Psoriasis. J. Pers. Med. 2021, 11, 293. [Google Scholar] [CrossRef]
- Dand, N.; Duckworth, M.; Baudry, D.; Russell, A.; Curtis, C.J.; Lee, S.H.; Evans, I.; Mason, K.J.; Alsharqi, A.; Becher, G.; et al. HLA-C*06:02 genotype is a predictive biomarker of biologic treatment response in psoriasis. J. Allergy Clin. Immunol. 2019, 143, 2120–2130. [Google Scholar] [CrossRef] [Green Version]
- Gibson, D.S.; McGeough, C.M.; Watterson, S.; Blayney, J.; Wright, G.D.; Pendleton, A.; Gardiner, P.; Small, D.; Eakin, A.J.; Ahmed, T.; et al. Anti-tumour necrosis factor-alpha response associated with combined CD226 and HLA-DRB1[*]0404 haplotype in rheumatoid arthritis. Clin. Exp. Rheumatol. 2021, 39, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.; Peel, C.; Wang, Q.; Pananos, A.D.; Kim, R.B. HLADQA1*05 genotype predicts anti-drug antibody formation and loss of response during infliximab therapy for inflammatory bowel disease. Aliment. Pharmacol. Ther. 2020, 51, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Sazonovs, A.; Kennedy, N.A.; Moutsianas, L.; Heap, G.A.; Rice, D.L.; Reppell, M.; Bewshea, C.M.; Chanchlani, N.; Walker, G.J.; Perry, M.H.; et al. HLA-DQA1*05 Carriage Associated With Development of Anti-Drug Antibodies to Infliximab and Adalimumab in Patients With Crohn’s Disease. Gastroenterology 2020, 158, 189–199. [Google Scholar] [CrossRef] [Green Version]
- Dubinsky, M.C.; Mei, L.; Friedman, M.; Dhere, T.; Haritunians, T.; Hakonarson, H.; Kim, C.; Glessner, J.; Targan, S.R.; McGovern, D.P.; et al. Genome wide association (GWA) predictors of anti-TNFalpha therapeutic responsiveness in pediatric inflammatory bowel disease. Inflamm. Bowel Dis. 2010, 16, 1357–1366. [Google Scholar] [CrossRef] [PubMed]
- Karczewski, K.J.; Francioli, L.C.; Tiao, G.; Cummings, B.B.; Alföldi, J.; Wang, Q.; Collins, R.L.; Laricchia, K.M.; Ganna, A.; Birnbaum, D.P.; et al. The mutational constraint spectrum quantified from variation in 141,456 humans. Nature 2020, 581, 434–443. [Google Scholar] [CrossRef]
- Lauro, R.; Mannino, F.; Irrera, N.; Squadrito, F.; Altavilla, D.; Squadrito, G.; Pallio, G.; Bitto, A. Pharmacogenetics of Biological Agents Used in Inflammatory Bowel Disease: A Systematic Review. Biomedicines 2021, 9, 1748. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.; Battat, R.; Lukin, D.; Scherl, E.J.; Pola, S.; Kumar, A.; Okada, L.; Yang, L.; Jain, A.; Siegel, C.A. Immunogenicity of Tumor Necrosis Factor Antagonists and Effect of Dose Escalation on Anti-Drug Antibodies and Serum Drug Concentrations in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2021, 27, 1443–1451. [Google Scholar]
- Hässler, S.; Bachelet, D.; Duhaze, J.; Szely, N.; Gleizes, A.; Abina, S.H.B.; Aktas, O.; Auer, M.; Avouac, J.; Birchler, M.; et al. Clinicogenomic factors of biotherapy immunogenicity in autoimmune disease: A prospective multicohort study of the ABIRISK consortium. PLoS Med. 2020, 17, e1003348. [Google Scholar] [CrossRef]
- Mosch, R.; Guchelaar, H.J. Immunogenicity of Monoclonal Antibodies and the Potential Use of HLA Haplotypes to Predict Vulnerable Patients. Front. Immunol. 2022, 13, 885672. [Google Scholar] [CrossRef]
- Colman, R.J.; Xiong, Y.; Mizuno, T.; Hyams, J.S.; Noe, J.D.; Boyle, B.; D’Haens, G.R.; van Limbergen, J.; Chun, K.; Yang, J.; et al. Antibodies-to-infliximab accelerate clearance while dose intensification reverses immunogenicity and recaptures clinical response in paediatric Crohn’s disease. Aliment. Pharmacol. Ther. 2022, 55, 593–603. [Google Scholar] [CrossRef]
- Powell Doherty, R.D.; Liao, H.; Satsangi, J.J.; Ternette, N. Extended Analysis Identifies Drug-Specific Association of 2 Distinct HLA Class II Haplotypes for Development of Immunogenicity to Adalimumab and Infliximab. Gastroenterology 2020, 159, 784–787. [Google Scholar] [CrossRef]
- Sazonovs, A.; Ahmad, T.; Anderson, C.A. Underpowered PANTS: A Response to the Conclusions of Extended Analysis Identifies Drug-Specific Association of Two Distinct HLA Class II Haplotypes for Development of Immunogenicity to Adalimumab and Infliximab. Gastroenterology 2021, 160, 470–471. [Google Scholar] [CrossRef]
- Salvador-Martín, S.; Pujol-Muncunill, G.; Bossacoma, F.; Navas-López, V.M.; Gallego-Fernández, C.; Segarra, O.; Clemente, S.; Muñoz-Codoceo, R.; Viada, J.; Magallares, L.; et al. Pharmacogenetics of trough serum anti-TNF levels in paediatric inflammatory bowel disease. Br. J. Clin. Pharmacol. 2021, 87, 447–457. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, M.S.; Cho, J.H.; Rioux, J.D.; McGovern, D.P.B.; Wu, J.; Annese, V.; Achkar, J.P.; Goyette, P.; Scott, R.; Xu, W.; et al. Ulcerative colitis-risk loci on chromosomes 1p36 and 12q15 found by genome-wide association study. Nat. Genet. 2009, 41, 216–220. [Google Scholar] [CrossRef]
- McGovern, D.P.B.; Gardet, A.; Törkvist, L.; Goyette, P.; Essers, J.; Taylor, K.D.; Neale, B.M.; Ong, R.T.H.; Lagacé, C.; Li, C.; et al. Genome-wide association identifies multiple ulcerative colitis susceptibility loci. Nat. Genet. 2010, 42, 332–337. [Google Scholar] [CrossRef] [Green Version]
- Latiano, A.; Palmieri, O.; Latiano, T.; Corritore, G.; Bossa, F.; Martino, G.; Biscaglia, G.; Scimeca, D.; Valvano, M.R.; Pastore, M.; et al. Investigation of multiple susceptibility loci for inflammatory bowel disease in an Italian cohort of patients. PLoS ONE 2011, 6, e22688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laserna-Mendieta, E.J.; Salvador-Martín, S.; Arias, A.; López-Cauce, B.; Marín-Jiménez, I.; Menchén, L.A.; Marín-Rubio, L.; Ontañón Rodríguez, J.; López-Fernández, L.A.; Lucendo, A.J. Single nucleotide polymorphisms in ADAM17, IL23R and SLCO1C1 genes protect against infliximab failure in adults with Crohn’s disease. Biomed. Pharmacother. 2023, 159, 114225. [Google Scholar] [CrossRef] [PubMed]
- Labarile, N.; Ghosh, S.; Ng, S.C.; Walters, J.; Iacucci, M. Tests that now deserve to be more widely adopted in IBD clinical practice. Ther. Adv. Gastroenterol. 2020, 13, 1756284820944088. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103308. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall (n = 340) | Responders (n = 270) | Non-Responders (n = 70) | p Value |
|---|---|---|---|---|
| Sex | ||||
| Male, n (%) | 205 (60.3%) | 168 (82.0%) | 37 (18.0%) | 0.171 |
| Female, n (%) | 135 (39.7%) | 102 (75.6%) | 33 (24.4%) | |
| Age (years) | ||||
| At diagnosis, median (IQR, range) | 11.2 (4.0, 0.7–17.3) | 11.2 (3.8, 0.9–17.3) | 11.0 (5.8, 0.7–16.0) | 0.109 |
| At start of treatment, median (IQR, range) | 12.2 (4.1, 1.1–17.5) | 12.3 (4.1, 1.4–17.5) | 12.0 (4.3, 1.1–17.3) | 0.251 |
| Months from diagnosis to initiation of therapy, median (IQR, range) | 6.1 (15.9, 0.0–129.6) | 6.1 (15.3, 0–129.6) | 8.9 (18.2, 0.0–125.8) | 0.202 |
| Type of IBD | ||||
| CD, n (%) | 240 (70.5%) | 201 (83.8%) | 39 (16.3%) | |
| UC, n (%) | 93 (27.4%) | 63 (67.7%) | 30 (32.3%) | 0.012 |
| IC, n (%) | 7 (2.1%) | 6 (85.7%) | 1 (14.3%) | |
| First or second biological treatment | ||||
| 1st, n (%) | 318 (93.5%) | 259 (81.4%) | 59 (18.6%) | 0.001 |
| 2nd, n (%) | 22 (6.5%) | 11 (50.0%) | 11 (50.0%) | |
| Drug | ||||
| Infliximab, n (%) | 228 (67.1%) | 185 (81.1%) | 43 (18.9%) | 0.318 |
| Adalimumab, n (%) | 112 (32.9%) | 85 (75.9%) | 27 (24.1%) | |
| Concomitant immunomodulator (n = 330) | ||||
| Yes, n (%) | 286 (86.7%) | 229 (80.1%) | 57 (19.9%) | 0.843 |
| No, n (%) | 44/13.3%) | 36 (81.8%) | 8 (18.2%) | 0.843 |
| Type of immunotherapy (n = 283) | ||||
| Azathioprine | 266 (81.6%) | 215 (80.8%) | 51 (19.2%) | |
| Mercaptopurine | 3 (0.9%) | 2 (66.7%) | 1 (33.3%) | 0.947 |
| Methotrexate | 14 (4.3%) | 10 (71.4%) | 4 (28.6%) | |
| Characteristics | Overall (n = 131) | Responders (n = 77) | Non-Responders (n = 54) | p Value |
|---|---|---|---|---|
| Sex | ||||
| Male, n (%) | 66 (50.4%) | 41 (62.1%) | 25 (37.9%) | 0.480 |
| Female, n (%) | 65 (49.6%) | 36 (55.4%) | 29 (44.6%) | |
| Age (years) | ||||
| At diagnosis, median (IQR, range) | 27.2 (16.4; 10.8–76.7) | 27.7 (18.2; 10.8–76.7) | 26.7 (15.9; 11.7–58.7) | 0.359 |
| At start of treatment, median (IQR, range) | 37.4 (18.5; 12.5–81.4) | 36.6 (19; 12.5–81.4) | 35.5 (18.2; 16.2–64.5) | 0.818 |
| First or second biological treatment | ||||
| 1st, n (%) | 119 (90.8%) | 73 (60.3%) | 48 (39.7%) | 0.317 |
| 2nd, n (%) | 12 (9.2%) | 4 (40%) | 6 (60%) | |
| Concomitant immunomodulator (n = 128) | ||||
| Yes, n (%) | 68 (51.9%) | 47 (69.1%) | 21 (30.9%) | 0.045 |
| No, n (%) | 60 (45.8%) | 30 (50%) | 30 (50%) | |
| Type of immunotherapy | ||||
| Azathioprine | 54 (79.4%) | 39 (72.2%) | 15 (27.8%) | 0.870 |
| Mercaptopurine | 4 (5.9%) | 4 (100%) | 0 (0%) | |
| Methotrexate | 7 (10.3%) | 2 (28.6%) | 5 (71.4%) | |
| Mycophenolate | 3 (4.4%) | 2 (66.7%) | 1 (33.3%) | |
| rs2097432 | rs2395185 | Risk Group |
|---|---|---|
| TT | TT or GT | Low |
| CC 1 or CT 1 | TT or GT | Medium |
| TT | GG 1 | Medium |
| CC 1 or CT 1 | GG 1 | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvador-Martín, S.; Zapata-Cobo, P.; Velasco, M.; Palomino, L.M.; Clemente, S.; Segarra, O.; Sánchez, C.; Tolín, M.; Moreno-Álvarez, A.; Fernández-Lorenzo, A.; et al. Association between HLA DNA Variants and Long-Term Response to Anti-TNF Drugs in a Spanish Pediatric Inflammatory Bowel Disease Cohort. Int. J. Mol. Sci. 2023, 24, 1797. https://doi.org/10.3390/ijms24021797
Salvador-Martín S, Zapata-Cobo P, Velasco M, Palomino LM, Clemente S, Segarra O, Sánchez C, Tolín M, Moreno-Álvarez A, Fernández-Lorenzo A, et al. Association between HLA DNA Variants and Long-Term Response to Anti-TNF Drugs in a Spanish Pediatric Inflammatory Bowel Disease Cohort. International Journal of Molecular Sciences. 2023; 24(2):1797. https://doi.org/10.3390/ijms24021797
Chicago/Turabian StyleSalvador-Martín, Sara, Paula Zapata-Cobo, Marta Velasco, Laura M. Palomino, Susana Clemente, Oscar Segarra, Cesar Sánchez, Mar Tolín, Ana Moreno-Álvarez, Ana Fernández-Lorenzo, and et al. 2023. "Association between HLA DNA Variants and Long-Term Response to Anti-TNF Drugs in a Spanish Pediatric Inflammatory Bowel Disease Cohort" International Journal of Molecular Sciences 24, no. 2: 1797. https://doi.org/10.3390/ijms24021797