
Shock-Driven Endotheliopathy in Trauma Patients Is Associated with Leucocyte Derived Extracellular Vesicles
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics and Outcome
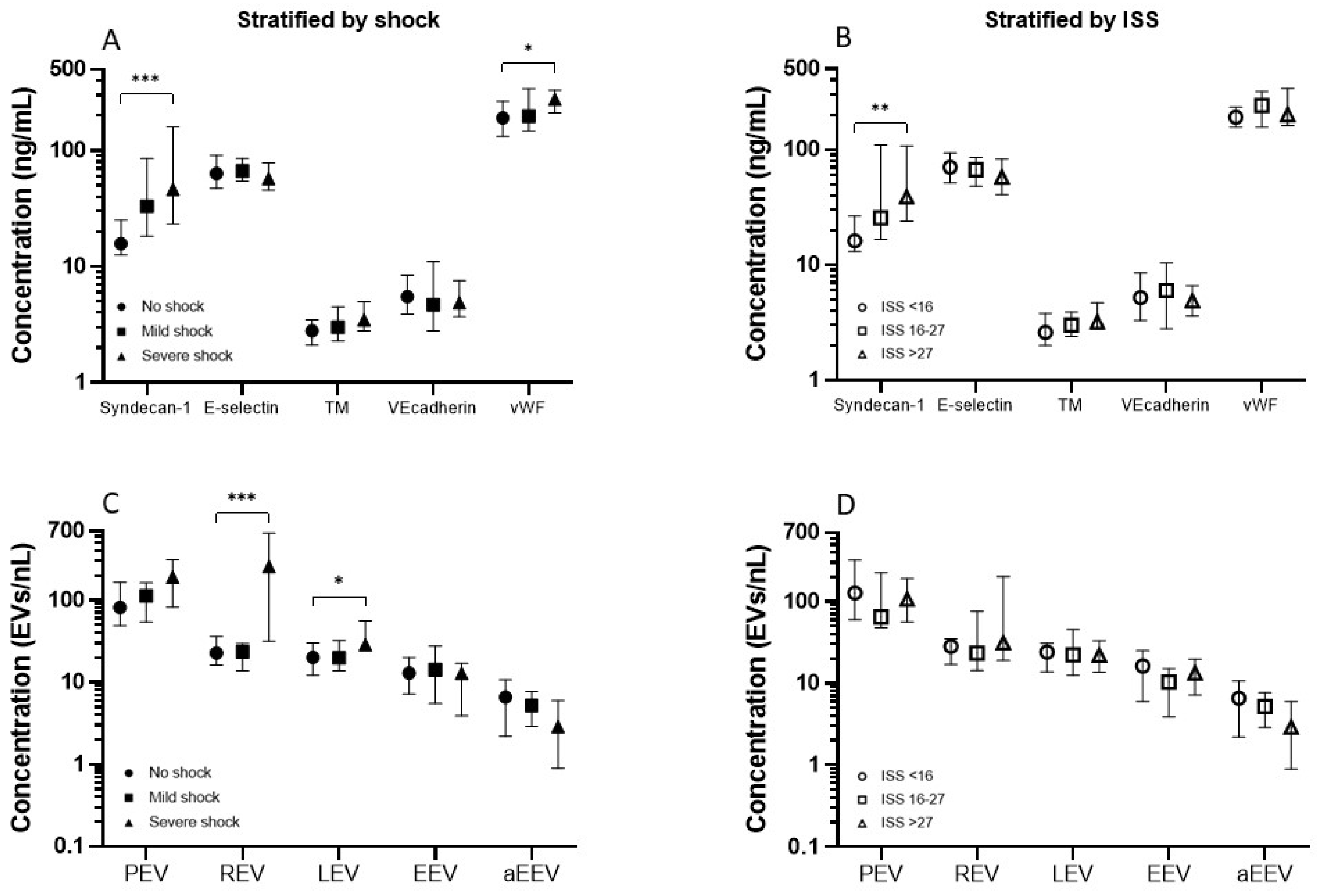
2.2. Endothelial Activation
2.3. Extracellular Vesicles
2.4. The Effect of Transfusion on Endothelial Activation and Extracellular Vesicles
2.5. The Relation between Endothelial Activation and Extracellular Vesicles
3. Discussion
4. Materials and Methods
4.1. Study Design and Participants
4.2. Patient Selection and Stratification
4.3. Data Collection and Outcome Measures
4.4. Sample Processing
4.5. Endothelial Activation Markers
4.6. Extracellular Vesicles and Flow Cytometry
4.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Norton, R.; Kobusingye, O. Injuries. N. Engl. J. Med. 2013, 368, 1723–1730. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.A.; van Wessem, K.J.; McDougall, D.; Lee, K.A.; Lyons, T.; Balogh, Z.J. Epidemiology of traumatic deaths: Comprehensive population-based assessment. World J. Surg. 2010, 34, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Callcut, R.A.; Kornblith, L.Z.; Conroy, A.S.; Robles, A.J.; Meizoso, J.P.; Namias, N.; Meyer, D.E.; Haymaker, A.; Truitt, M.S.; Agrawal, V.; et al. The why and how our trauma patients die: A prospective Multicenter Western Trauma Association study. J. Trauma Acute Care Surg. 2019, 86, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.E.; Moore, H.B.; Kornblith, L.Z.; Neal, M.D.; Hoffman, M.; Mutch, N.J.; Schochl, H.; Hunt, B.J.; Sauaia, A. Trauma-induced coagulopathy. Nat. Rev. Dis. Prim. 2021, 7, 30. [Google Scholar] [CrossRef]
- Gimbrone, M.A., Jr. Vascular endothelium: Nature’s blood-compatible container. Ann. N. Y. Acad. Sci. 1987, 516, 5–11. [Google Scholar] [CrossRef]
- Naumann, D.N.; Hazeldine, J.; Midwinter, M.J.; Hutchings, S.D.; Harrison, P. Poor microcirculatory flow dynamics are associated with endothelial cell damage and glycocalyx shedding after traumatic hemorrhagic shock. J. Trauma Acute Care Surg. 2018, 84, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Sun, D.; Song, J.W.; Zullo, J.; Lipphardt, M.; Coneh-Gould, L.; Goligorsky, M.S. Endothelial cell dysfunction and glycocalyx—A vicious circle. Matrix Biol. 2018, 71–72, 421–431. [Google Scholar] [CrossRef]
- Gonzalez Rodriguez, E.; Ostrowski, S.R.; Cardenas, J.C.; Baer, L.A.; Tomasek, J.S.; Henriksen, H.H.; Stensballe, J.; Cotton, B.A.; Holcomb, J.B.; Johansson, P.I.; et al. Syndecan-1: A Quantitative Marker for the Endotheliopathy of Trauma. J. Am. Coll. Surg. 2017, 225, 419–427. [Google Scholar] [CrossRef] [Green Version]
- Nair, A.B.; Schreiber, M.A.; Pati, S. Defining and Assessing the Endotheliopathy of Trauma and Its Implications on Trauma-Induced Coagulopathy and Trauma-Related Outcomes. In Trauma Induced Coagulopathy; Moore, H.B., Neal, M.D., Moore, E.E., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 117–133. [Google Scholar]
- Johansson, P.I.; Stensballe, J.; Rasmussen, L.S.; Ostrowski, S.R. A high admission syndecan-1 level, a marker of endothelial glycocalyx degradation, is associated with inflammation, protein C depletion, fibrinolysis, and increased mortality in trauma patients. Ann. Surg. 2011, 254, 194–200. [Google Scholar] [CrossRef]
- Naumann, D.N.; Hazeldine, J.; Davies, D.J.; Bishop, J.; Midwinter, M.J.; Belli, A.; Harrison, P.; Lord, J.M. Endotheliopathy of Trauma is an on-Scene Phenomenon, and is Associated with Multiple Organ Dysfunction Syndrome: A Prospective Observational Study. Shock 2018, 49, 420–428. [Google Scholar] [CrossRef]
- Dunne, J.R.; Malone, D.L.; Tracy, J.K.; Napolitano, L.M. Allogenic blood transfusion in the first 24 hours after trauma is associated with increased systemic inflammatory response syndrome (SIRS) and death. Surg. Infect. (Larchmt) 2004, 5, 395–404. [Google Scholar] [CrossRef]
- Yuana, Y.; Sturk, A.; Nieuwland, R. Extracellular vesicles in physiological and pathological conditions. Blood Rev. 2013, 27, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Fröhlich, M.; Schäfer, N.; Caspers, M.; Böhm, J.K.; Stürmer, E.K.; Bouillon, B.; Maegele, M. Temporal phenotyping of circulating microparticles after trauma: A prospective cohort study. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 33. [Google Scholar] [CrossRef] [Green Version]
- Straat, M.; Böing, A.N.; Tuip-De Boer, A.; Nieuwland, R.; Juffermans, N.P. Extracellular Vesicles from Red Blood Cell Products Induce a Strong Pro-Inflammatory Host Response, Dependent on Both Numbers and Storage Duration. Transfus. Med. Hemother. 2016, 43, 302–305. [Google Scholar] [CrossRef] [Green Version]
- Gamonet, C.; Desmarets, M.; Mourey, G.; Biichle, S.; Aupet, S.; Laheurte, C.; François, A.; Resch, E.; Bigey, F.; Binda, D.; et al. Processing methods and storage duration impact extracellular vesicle counts in red blood cell units. Blood Adv. 2020, 4, 5527–5539. [Google Scholar] [CrossRef]
- Johansson, P.I.; Henriksen, H.H.; Stensballe, J.; Gybel-Brask, M.; Cardenas, J.C.; Baer, L.A.; Cotton, B.A.; Holcomb, J.B.; Wade, C.E.; Ostrowski, S.R. Traumatic Endotheliopathy: A Prospective Observational Study of 424 Severely Injured Patients. Ann. Surg. 2017, 265, 597–603. [Google Scholar] [CrossRef] [Green Version]
- Rahbar, E.; Cardenas, J.C.; Baimukanova, G.; Usadi, B.; Bruhn, R.; Pati, S.; Ostrowski, S.R.; Johansson, P.I.; Holcomb, J.B.; Wade, C.E. Endothelial glycocalyx shedding and vascular permeability in severely injured trauma patients. J. Transl. Med. 2015, 13, 117. [Google Scholar] [CrossRef] [Green Version]
- Haywood-Watson, R.J.; Holcomb, J.B.; Gonzalez, E.A.; Peng, Z.; Pati, S.; Park, P.W.; Wang, W.; Zaske, A.M.; Menge, T.; Kozar, R.A. Modulation of syndecan-1 shedding after hemorrhagic shock and resuscitation. PLoS ONE 2011, 6, e23530. [Google Scholar] [CrossRef] [Green Version]
- Matijevic, N.; Wang, Y.W.; Wade, C.E.; Holcomb, J.B.; Cotton, B.A.; Schreiber, M.A.; Muskat, P.; Fox, E.E.; Del Junco, D.J.; Cardenas, J.C.; et al. Cellular microparticle and thrombogram phenotypes in the Prospective Observational Multicenter Major Trauma Transfusion (PROMMTT) study: Correlation with coagulopathy. Thromb. Res. 2014, 134, 652–658. [Google Scholar] [CrossRef] [Green Version]
- Teng, Y.H.; Aquino, R.S.; Park, P.W. Molecular functions of syndecan-1 in disease. Matrix Biol. 2012, 31, 3–16. [Google Scholar] [CrossRef]
- Glance, L.G.; Stone, P.W.; Mukamel, D.B.; Dick, A.W. Increases in mortality, length of stay, and cost associated with hospital-acquired infections in trauma patients. Arch. Surg. 2011, 146, 794–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lord, J.M.; Midwinter, M.J.; Chen, Y.F.; Belli, A.; Brohi, K.; Kovacs, E.J.; Koenderman, L.; Kubes, P.; Lilford, R.J. The systemic immune response to trauma: An overview of pathophysiology and treatment. Lancet 2014, 384, 1455–1465. [Google Scholar] [CrossRef] [Green Version]
- Botha, A.J.; Moore, F.A.; Moore, E.E.; Kim, F.J.; Banerjee, A.; Peterson, V.M. Postinjury neutrophil priming and activation: An early vulnerable window. Surgery 1995, 118, 358–364; discussion 364-355. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.; Thiemermann, C.; Brohi, K. Trauma alarmins as activators of damage-induced inflammation. Br. J. Surg. 2012, 99 (Suppl. S1), 12–20. [Google Scholar] [CrossRef] [PubMed]
- Mortaz, E.; Zadian, S.S.; Shahir, M.; Folkerts, G.; Garssen, J.; Mumby, S.; Adcock, I.M. Does Neutrophil Phenotype Predict the Survival of Trauma Patients? Front. Immunol. 2019, 10, 2122. [Google Scholar] [CrossRef] [PubMed]
- Botha, A.J.; Moore, F.A.; Moore, E.E.; Peterson, V.M.; Goode, A.W. Base deficit after major trauma directly relates to neutrophil CD11b expression: A proposed mechanism of shock-induced organ injury. Intensive Care Med. 1997, 23, 504–509. [Google Scholar] [CrossRef]
- Rangarajan, S.; Richter, J.R.; Richter, R.P.; Bandari, S.K.; Tripathi, K.; Vlodavsky, I.; Sanderson, R.D. Heparanase-enhanced Shedding of Syndecan-1 and Its Role in Driving Disease Pathogenesis and Progression. J. Histochem. Cytochem. 2020, 68, 823–840. [Google Scholar] [CrossRef]
- Wirtz, M.R.; Jurgens, J.; Zuurbier, C.J.; Roelofs, J.; Spinella, P.C.; Muszynski, J.A.; Carel Goslings, J.; Juffermans, N.P. Washing or filtering of blood products does not improve outcome in a rat model of trauma and multiple transfusion. Transfusion 2019, 59, 134–145. [Google Scholar] [CrossRef] [Green Version]
- Rubin, O.; Crettaz, D.; Canellini, G.; Tissot, J.D.; Lion, N. Microparticles in stored red blood cells: An approach using flow cytometry and proteomic tools. Vox Sang. 2008, 95, 288–297. [Google Scholar] [CrossRef] [Green Version]
- Tzounakas, V.L.; Stamoulis, K.E.; Anastasiadi, A.T.; Papassideri, I.S.; Kriebardis, A.G.; Rinalducci, S.; Antonelou, M.H. Leukoreduction makes a difference: A pair proteomics study of extracellular vesicles in red blood cell units. Transfus. Apher. Sci. 2021, 60, 103166. [Google Scholar] [CrossRef]
- Lacroix, R.; Judicone, C.; Mooberry, M.; Boucekine, M.; Key, N.S.; Dignat-George, F. Standardization of pre-analytical variables in plasma microparticle determination: Results of the International Society on Thrombosis and Haemostasis SSC Collaborative workshop. J. Thromb. Haemost. 2013. [Google Scholar] [CrossRef]
- Welsh, J.A.; Van Der Pol, E.; Arkesteijn, G.J.A.; Bremer, M.; Brisson, A.; Coumans, F.; Dignat-George, F.; Duggan, E.; Ghiran, I.; Giebel, B.; et al. MIFlowCyt-EV: A framework for standardized reporting of extracellular vesicle flow cytometry experiments. J. Extracell. Vesicles 2020, 9, 1713526. [Google Scholar] [CrossRef]
- Juffermans, N.P.; Wirtz, M.R.; Balvers, K.; Baksaas-Aasen, K.; van Dieren, S.; Gaarder, C.; Naess, P.A.; Stanworth, S.; Johansson, P.I.; Stensballe, J.; et al. Towards patient-specific management of trauma hemorrhage: The effect of resuscitation therapy on parameters of thromboelastometry. J. Thromb. Haemost. 2019, 17, 441–448. [Google Scholar] [CrossRef] [Green Version]
- Mutschler, M.; Nienaber, U.; Brockamp, T.; Wafaisade, A.; Fabian, T.; Paffrath, T.; Bouillon, B.; Maegele, M. Renaissance of base deficit for the initial assessment of trauma patients: A base deficit-based classification for hypovolemic shock developed on data from 16,305 patients derived from the TraumaRegister DGU®. Crit. Care 2013, 17, R42. [Google Scholar] [CrossRef] [Green Version]
- Van der Pol, E.; de Rond, L.; Coumans, F.A.W.; Gool, E.L.; Böing, A.N.; Sturk, A.; Nieuwland, R.; van Leeuwen, T.G. Absolute sizing and label-free identification of extracellular vesicles by flow cytometry. Nanomedicine 2018, 14, 801–810. [Google Scholar] [CrossRef]
- De Rond, L.; Libregts, S.; Rikkert, L.G.; Hau, C.M.; van der Pol, E.; Nieuwland, R.; van Leeuwen, T.G.; Coumans, F.A.W. Refractive index to evaluate staining specificity of extracellular vesicles by flow cytometry. J. Extracell. Vesicles 2019, 8, 1643671. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Whole Cohort N = 75 | No Shock N = 30 | Mild Shock N = 26 | Severe Shock N = 19 | p Value | |
|---|---|---|---|---|---|
| Age (years) | 43 (27–57) | 50 (35–62) | 32 (21–48) | 43 (31–58) | 0.023 |
| Male n (%) | 54 (72%) | 23 (77%) | 19 (73%) | 12 (63%) | 0.584 |
| Blunt injury n (%) | 65 (87%) | 28 (93%) | 24 (92%) | 13 (70%) | 0.025 |
| Coagulopathic n (%) | 20 (27%) | 4 (13%) | 7 (27%) | 9 (47%) | 0.008 |
| Transfusion group n (%) | 25 (33%) | 3 (10%) | 5 (19%) | 17 (90%) | <0.001 |
| Clinical Variables | |||||
| ISS (0–75) | 22 (10–30) | 10 (8–23) | 26 (16–39) | 27 (22–33) | <0.001 |
| TBI n (%) | 30 (40%) | 9 (30%) | 11 (42%) | 10 (53%) | 0.321 |
| Polytrauma n (%) | 29 (38.7%) | 5 (16.7%) | 13 (30.0%) | 11 (57.9%) | 0.005 |
| GCS (1–15) | 13 (5–15) | 15 (12–15) | 9 (4–15) | 10 (3–13) | 0.035 |
| SBP (mmHg) | 127 (103–143) | 141 (130–151) | 123 (71–105) | 94 (70–114) | <0.001 |
| HR (beats/min) | 83 (75–106) | 80 (73–89) | 80 (71–105) | 120 (90–142) | <0.001 |
| Mortality at day 28 n (%) | 11 (15%) | 0 (0%) | 6 (23%) | 5 (26%) | 0.013 |
| Biochemical variables | |||||
| Lactate (mmol/L) | 2.6 (1.6–3.8) | 2.1 (1.5–2.8) | 2.1 (1.4–3.8) | 4.6 (3.6–8.4) | <0.001 |
| Base excess (mEq/L) | −2.6 (−6.2 to −0.8) | −0.25 (−1.3 to 1.1) | −3.8 (−4.5 to −2.5) | −9.6 (−15.5 to −7.4) | <0.001 |
| Haemoglobin (mmol/L) | 13.1 (12.0–15.3) | 13.8 (13.0–14.5) | 12.8 (11.8–14.0) | 13.0 (11.4–15.0) | 0.127 |
| Platelet count (×109/L) | 223 (185–271) | 244 (190–278) | 234 (185–264) | 214 (136–290) | 0.336 |
| aPTT (seconds) | 25 (23–29) | 24 (22–26) | 26 (23–30) | 30 (24–44) | 0.005 |
| INR (ratio) | 1.1 (1.0–1.2) | 1.0 (0.9–1.1) | 1.1 (1.0–1.2) | 1.2 (1.1–1.3) | <0.001 |
| Fibrinogen level (g/L) | 2.2 (1.6–2.7) | 2.6 (2.1–3.3) | 2.1 (1.5–2.5) | 1.8 (1.4–2.8) | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dujardin, R.W.G.; Kisters, J.E.C.; Wirtz, M.R.; Hajji, N.; Tuip-de Boer, A.M.; Stensballe, J.; Johansson, P.I.; Brohi, K.; Davenport, R.A.; Gaarder, C.; et al. Shock-Driven Endotheliopathy in Trauma Patients Is Associated with Leucocyte Derived Extracellular Vesicles. Int. J. Mol. Sci. 2022, 23, 15990. https://doi.org/10.3390/ijms232415990
Dujardin RWG, Kisters JEC, Wirtz MR, Hajji N, Tuip-de Boer AM, Stensballe J, Johansson PI, Brohi K, Davenport RA, Gaarder C, et al. Shock-Driven Endotheliopathy in Trauma Patients Is Associated with Leucocyte Derived Extracellular Vesicles. International Journal of Molecular Sciences. 2022; 23(24):15990. https://doi.org/10.3390/ijms232415990
Chicago/Turabian StyleDujardin, Romein W. G., Jeske E. C. Kisters, Mathijs R. Wirtz, Najat Hajji, Anita M. Tuip-de Boer, Jakob Stensballe, Pär I. Johansson, Karim Brohi, Ross A. Davenport, Christine Gaarder, and et al. 2022. "Shock-Driven Endotheliopathy in Trauma Patients Is Associated with Leucocyte Derived Extracellular Vesicles" International Journal of Molecular Sciences 23, no. 24: 15990. https://doi.org/10.3390/ijms232415990