
Therapeutic Approaches for Age-Related Macular Degeneration

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
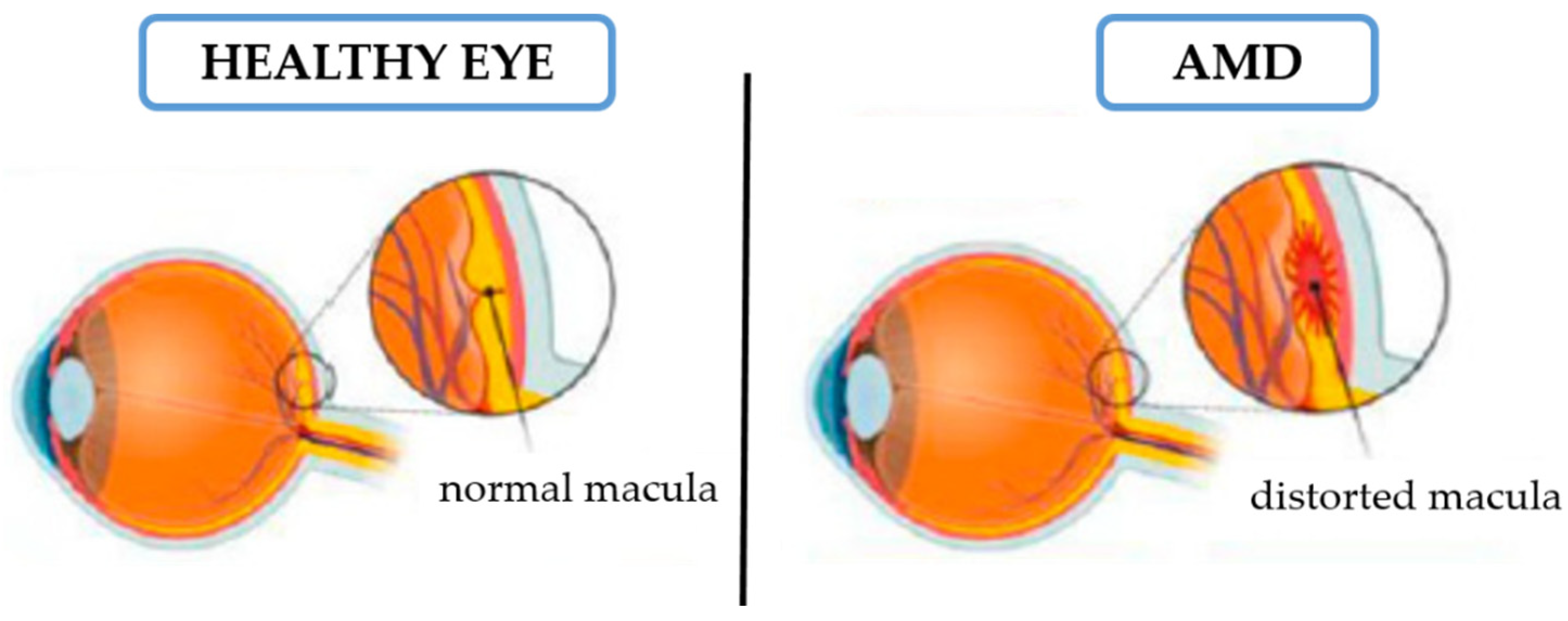
2. AMD Signs and Symptoms
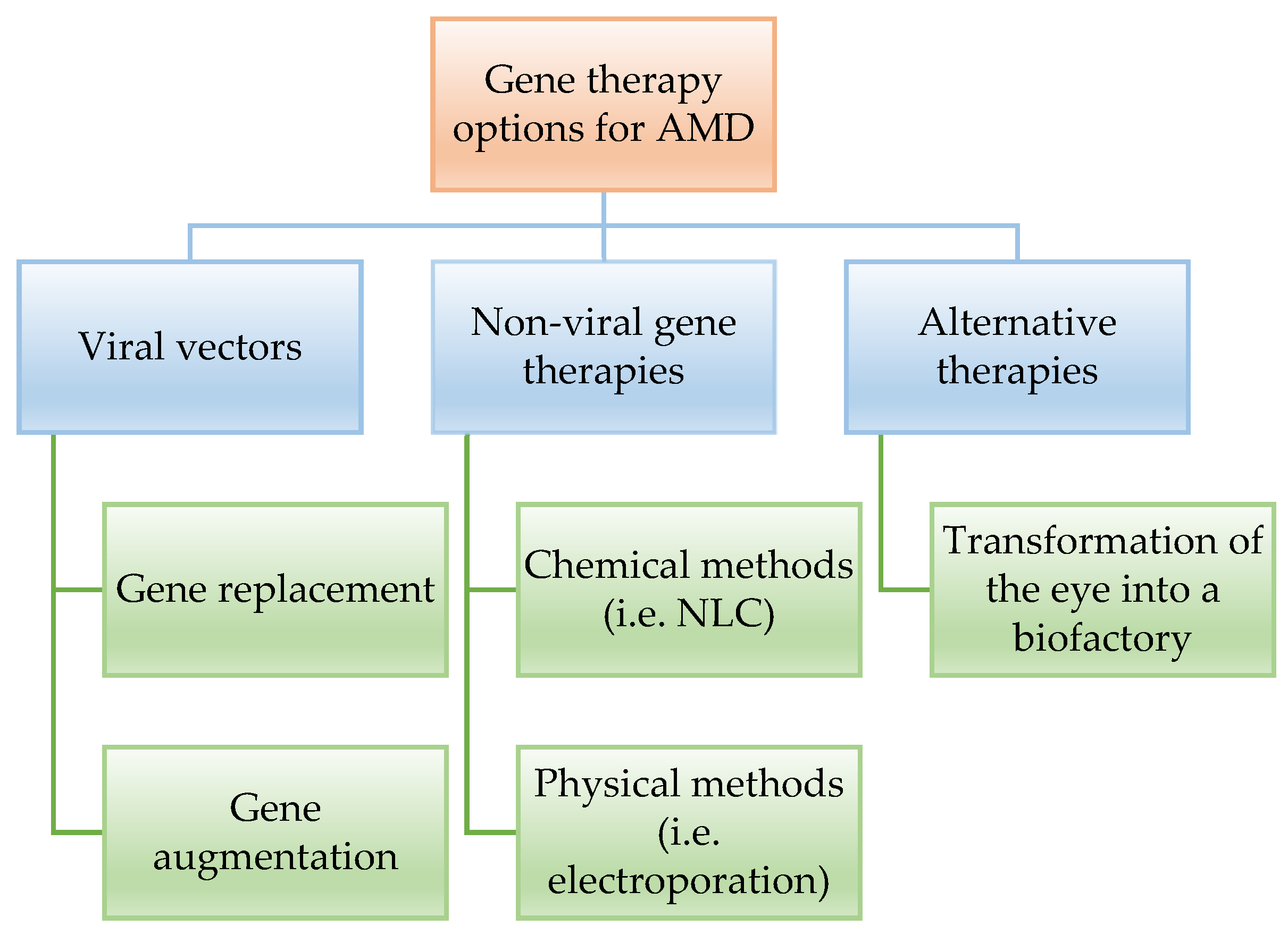
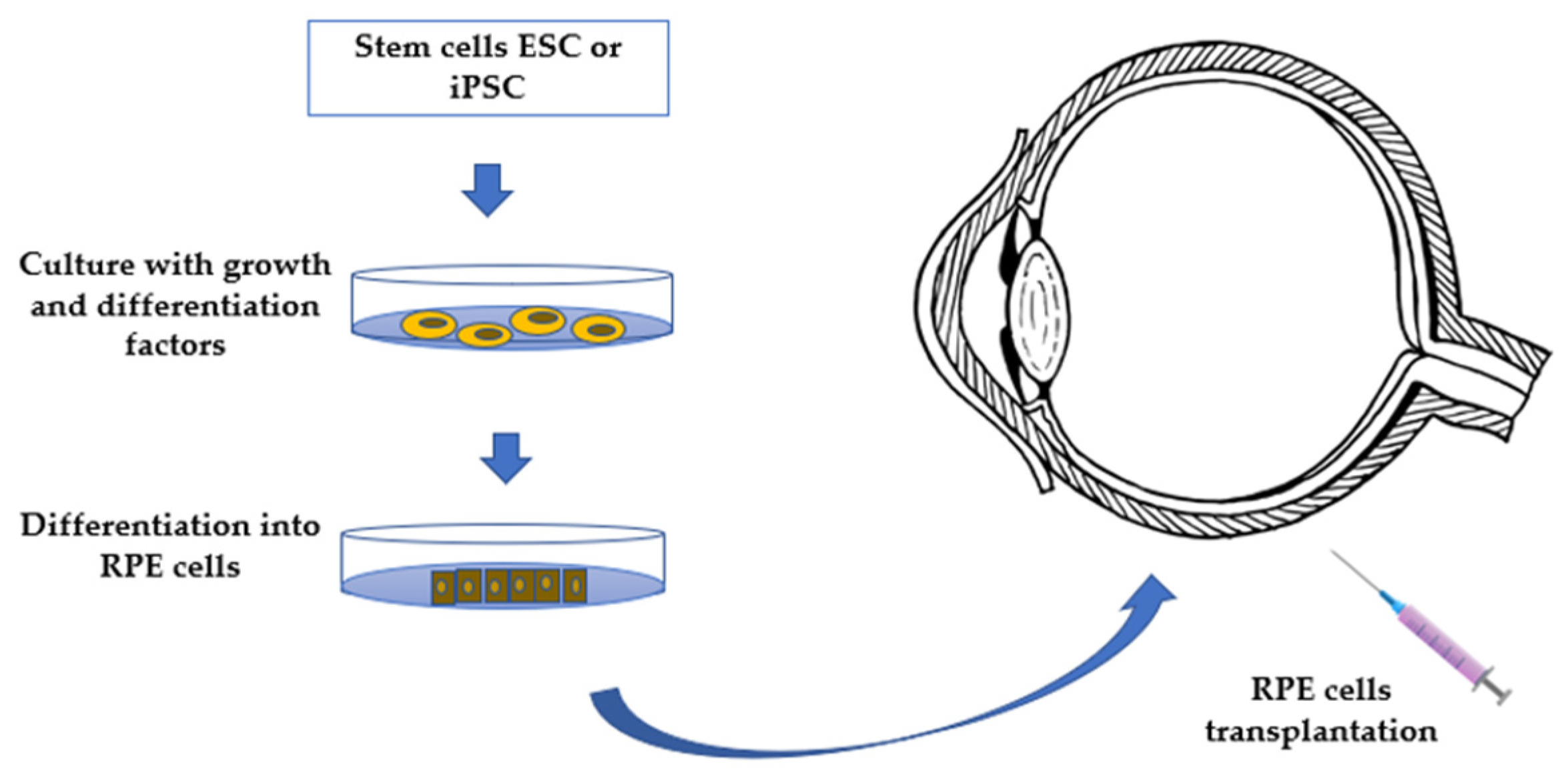
3. Biological Therapies for the Treatment of AMD
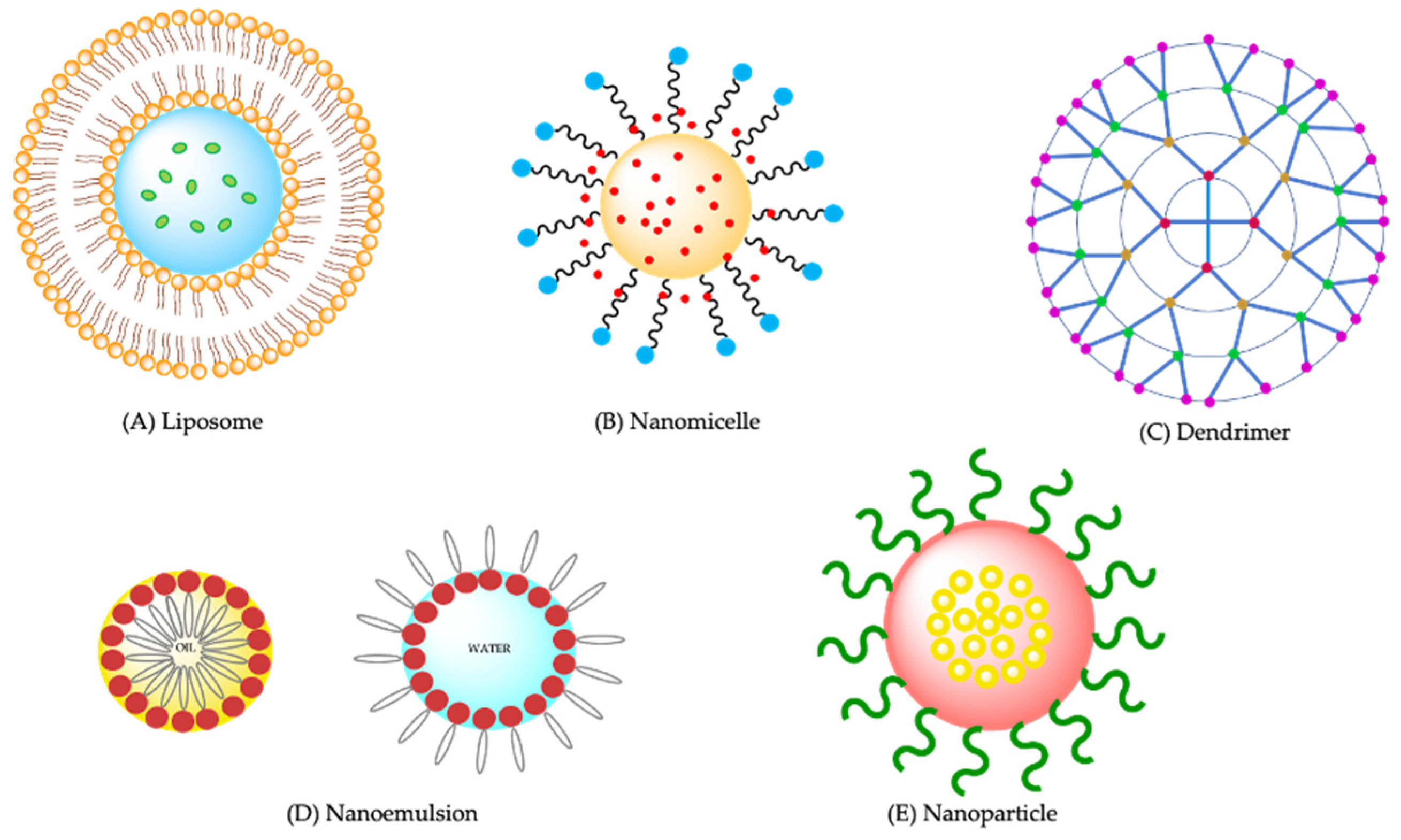
4. Drug Delivery Systems Proposed for AMD
5. Three Dimensional (3D) Bioprinting Treatment for AMD
6. Conclusions

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Loaded Molecule | Matrix | Surfactant | AS | PDI | ZP (mV) | Assay Model | Results | Ref. |
|---|---|---|---|---|---|---|---|---|
| Atorvastatin | Compritol® 888 ATO | PEG 400/Poloxamer 188 | 256.3 ± 10.5 | 0.26 ± 0.02 | −2.65 | Retinal pigment epithelial cells (ARPE-19)/rats | NPs were more bioavailable in the aqueous and vitreous humor than the free drug. Successful administration as eye drops was obtained in in vivo tests. | [83] |
| Resveratrol | PLGA | - | 102.7 ± 2.8 | 0.095 ± 0.003 | −47.30 ± 0.9 | ARPE-19, human retinal pigment epithelial cell line (ATCC® CRL2302TM) | The resveratrol-encapsulated PLGA nanoparticles were non-cytotoxic to the cells and exhibited effective inhibition of VEGF expression levels. | [113] |
| Sirolimus | PLGA (chitosan decorated) | PVA | 265.9 ± 6.30 | 0.215 ± 0.12 | +24.832 ± 2.12 | Goat eyes/chick embryo chorioallantoic membrane [114] | The subconjunctival route has the greatest potential to surpass intravitreal injection as the preferred treatment option for AMD. | [115] |
| Lutein | PLGA (biotin-decorated) | PVA | 208.0 ± 3.38 | 0.206 ± 0.016 | 27.2 ± 2.04 | ARPE-19 cells | Biotin-conjugated nanoparticles may be an appropriate formulation for targeted drug delivery in the treatment of AMD and other retinal diseases | [116] |
| Axitinib | PLGA | PVA | 131.33 ± 31.20 | 0.108 ± 0.005 | −4.63 ± 0.76 | ARPE-19, human retinal pigment epithelial cell line (ATCC® CRL2302™) | This formulation may present an important approach to treating wet AMD due to its capability to ensure a sustained release of the drug and a potential in inhibiting VEGF expression. | [117] |
| DXM/Bevacizumab | PLGA/PEI | PVA | 201.3 ± 7.2 | 0.318 ± 0.084 | 0.31 ± 1.15 | Human umbilical vein endothelial cells (HUVECs)/chick embryo chorioallantoic membrane | The formulation provided a strong inhibitory effect on VEGF secretion from HUVECs. Moreover, in vivo chick embryo chorioallantoic membrane assay showed nanoparticles greatly reduced the amount of blood vessels. | [118] |
| Doxorubicin | PEG-PLA chain with Tat-C (CPP) | - | 29.4 ± 4.1 | - | −1.0 ± 0.2 | Human umbilical vein endothelial cells (HUVECs)/adult female C57BL/6 mice | Doxorubicin-loaded NPs-CPP significantly reduces neovascular lesion size, proposing a strategy for non-invasive treatment of CNV, and enhancing drug accumulation specifically in diseased areas of the eye. | [119] |
| Fenofibrate | PLGA | PVA | 265 ± 10 | 0.03 ± 0.01 | −1.2 ± 0.1 | Male Brown Norway and Vldlr−/− mice | Ameliorated retinal dysfunctions, reduced retinal vascular leakage, inhibited retinal leukostasis, and downregulation of the overexpression of VEGF were observed. Furthermore, Fenofibrate NPs reduced retinal vascular leakage and CNV formation in both animal models. | [120] |
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parmeggiani, F.; Romano, M.R.; Costagliola, C.; Semeraro, F.; Incorvaia, C.; D’Angelo, S.; Perri, P.; De Palma, P.; De Nadai, K.; Sebastiani, A. Mechanism of Inflammation in Age-Related Macular Degeneration. Mediat. Inflamm. 2012, 2012, 546786. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, A.R.; Zielińska, A.; Sanchez-Lopez, E.; dos Santos, T.; Garcia, M.L.; Silva, A.M.; Karczewski, J.; Souto, E.B. Exudative versus Nonexudative Age-Related Macular Degeneration: Physiopathology and Treatment Options. Int. J. Mol. Sci. 2022, 23, 2592. [Google Scholar] [CrossRef]
- Mitchell, P.; Liew, G.; Gopinath, B.; Wong, T.Y. Age-related macular degeneration. Lancet 2018, 392, 1147–1159. [Google Scholar] [CrossRef]
- Blasiak, J.; Reiter, R.J.; Kaarniranta, K. Melatonin in Retinal Physiology and Pathology: The Case of Age-Related Macular Degeneration. Oxidative Med. Cell. Longev. 2016, 2016, 6819736. [Google Scholar] [CrossRef] [Green Version]
- Yeh, C.C.; Wu, M.M.; Wu, C.M.; Sung, F.C.; Muo, C.H.; Te, A.; Su, F.H. Increased Risk of Age-Related Macular Degeneration with Chronic Hepatitis C Virus Infection: A Nationwide Population-Based Propensity Score-Matched Cohort Study in Taiwan. Viruses 2021, 13, 790. [Google Scholar] [CrossRef]
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet. Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [Green Version]
- Heesterbeek, T.J.; Lorés-Motta, L.; Hoyng, C.B.; Lechanteur, Y.T.E.; den Hollander, A.I. Risk factors for progression of age-related macular degeneration. Ophthalmic Physiol. Opt. J. Br. Coll. Ophthalmic Opt. (Optom.) 2020, 40, 140–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, M.; Duan, P.-C.; Liang, J.-H.; Zhang, X.-F.; Pan, C.-W. Geographic distributions of age-related macular degeneration incidence: A systematic review and meta-analysis. Br. J. Ophthalmol. 2021, 105, 1427. [Google Scholar] [CrossRef]
- Wang, J.J.; Jones, M.; Holliday, E.; Tan, A.G.; Oldmeadow, C.; van Dam, R.M.; Sim, X.; Flood, V.; Whitton, C.; Klein, R.; et al. Exploring factors underlying ethnic differences in age-related macular degeneration (AMD) prevalence. Investig. Ophthalmol. Vis. Sci. 2018, 59, 6008. [Google Scholar]
- Jager, R.D.; Mieler, W.F.; Miller, J.W. Age-related macular degeneration. N. Engl. J. Med. 2008, 358, 2606–2617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrasco-León, A.; Amundarain, A.; Gómez-Echarte, N.; Prósper, F.; Agirre, X. The Role of lncRNAs in the Pathobiology and Clinical Behavior of Multiple Myeloma. Cancers 2021, 13, 1976. [Google Scholar] [CrossRef]
- Spaide, R.F.; Jaffe, G.J.; Sarraf, D.; Freund, K.B.; Sadda, S.R.; Staurenghi, G.; Waheed, N.K.; Chakravarthy, U.; Rosenfeld, P.J.; Holz, F.G.; et al. Consensus Nomenclature for Reporting Neovascular Age-Related Macular Degeneration Data: Consensus on Neovascular Age-Related Macular Degeneration Nomenclature Study Group. Ophthalmology 2020, 127, 616–636. [Google Scholar] [CrossRef]
- A Das, R.; Romano, A.; Chiosi, F.; Menzione, M.; Rinaldi, M. Combined treatment modalities for age related macular degeneration. Curr. Drug Targets 2011, 12, 182–189. [Google Scholar] [CrossRef]
- Khan, K.N.; Mahroo, O.A.; Khan, R.S.; Mohamed, M.D.; McKibbin, M.; Bird, A.; Michaelides, M.; Tufail, A.; Moore, A.T. Differentiating drusen: Drusen and drusen-like appearances associated with ageing, age-related macular degeneration, inherited eye disease and other pathological processes. Prog. Retin. Eye Res. 2016, 53, 70–106. [Google Scholar] [CrossRef] [Green Version]
- Bressler, N.M.; Munoz, B.; Maguire, M.G.; Vitale, S.E.; Schein, O.D.; Taylor, H.R.; West, S.K. Five-year incidence and disappearance of drusen and retinal pigment epithelial abnormalities. Waterman study. Arch. Ophthalmol. 1995, 113, 301–308. [Google Scholar] [CrossRef]
- Hadziahmetovic, M.; Malek, G. Age-Related Macular Degeneration Revisited: From Pathology and Cellular Stress to Potential Therapies. Front. Cell Dev. Biol. 2021, 8, 612812. [Google Scholar] [CrossRef]
- Ding, X.; Patel, M.; Chan, C.-C. Molecular pathology of age-related macular degeneration. Prog. Retin. Eye Res. 2009, 28, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Thomas, C.J.; Mirza, R.G.; Gill, M.K. Age-Related Macular Degeneration. Med. Clin. N. Am. 2021, 105, 473–491. [Google Scholar] [CrossRef]
- She, K.; Su, J.; Wang, Q.; Liu, Y.; Zhong, X.; Jin, X.; Zhao, Q.; Xiao, J.; Li, R.; Deng, H.; et al. Delivery of nVEGFi using AAV8 for the treatment of neovascular age-related macular degeneration. Mol. Methods Clin. Dev. 2022, 24, 210–221. [Google Scholar] [CrossRef]
- Fernandes, A.R.; Dos Santos, T.; Granja, P.L.; Sanchez-Lopez, E.; Garcia, M.L.; Silva, A.M.; Souto, E.B. Permeability, anti-inflammatory and anti-VEGF profiles of steroidal-loaded cationic nanoemulsions in retinal pigment epithelial cells under oxidative stress. Int. J. Pharm. 2022, 617, 121615. [Google Scholar] [CrossRef]
- Poor, S.H.; Weissgerber, G.; Adams, C.M.; Harit, B.; Browning, D.J.; Chastain, J.; Ciulla, T.A.; Ferriere, M.; Gedif, K.; Louis, C.G.; et al. A randomized, double-masked, multicenter trial of topical acrizanib (LHA510), a tyrosine kinase VEGF-receptor inhibitor, in treatment-experienced subjects with neovascular age-related macular degeneration. Am. J. Ophthalmol. 2022, 239, 180–189. [Google Scholar] [CrossRef]
- Alis, A.; Guler Alis, M. Long-term effect of intravitreal aflibercept treatment on choroidal vascularity index in neovascular age-related macular degeneration. Photodiagnosis Photodyn. 2021, 36, 102582. [Google Scholar] [CrossRef] [PubMed]
- Al-Zamil, W.M.; Yassin, S.A. Recent developments in age-related macular degeneration: A review. Clin. Interv. Aging 2017, 12, 1313–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, H.J.; Yoon, W.; Yoon, J.; Na, S.K.; Lee, J.; Kim, J.; Kim, C.G.; Kim, J.W. Development of Intraretinal Fluid in Neovascular Age-Related Macular Degeneration During Anti-Vascular Endothelial Growth Factor Treatment. Am. J. Ophthalmol. 2022, 234, 6–14. [Google Scholar] [CrossRef]
- Deng, Y.; Qiao, L.; Du, M.; Qu, C.; Wan, L.; Li, J.; Huang, L. Age-related macular degeneration: Epidemiology, genetics, pathophysiology, diagnosis, and targeted therapy. Genes Dis. 2022, 9, 62–79. [Google Scholar] [CrossRef]
- Nguyen, Q.D.; Das, A.; Do, D.V.; Dugel, P.U.; Gomes, A.; Holz, F.G.; Koh, A.; Pan, C.K.; Sepah, Y.J.; Patel, N.; et al. Brolucizumab: Evolution through Preclinical and Clinical Studies and the Implications for the Management of Neovascular Age-Related Macular Degeneration. Ophthalmology 2020, 127, 963–976. [Google Scholar] [CrossRef]
- Rezende, F.A.; Lapalme, E.; Qian, C.X.; Smith, L.E.; SanGiovanni, J.P.; Sapieha, P. Omega-3 supplementation combined with anti-vascular endothelial growth factor lowers vitreal levels of vascular endothelial growth factor in wet age-related macular degeneration. Am. J. Ophthalmol. 2014, 158, 1071–1078. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.N.; Lai, C.C.; Wang, J.K.; Choi, H.Y.; Kuo, C.N.; Tsai, C.Y.; Wang, H.I.; Yang, C.M. Ranibizumab reimbursement and treatment patterns for neovascular age-related macular degeneration in Taiwan-Results from the 12-month, observational RENOWNED study. J. Formos. Med. Assoc. 2022, 121, 2020–2027. [Google Scholar] [CrossRef]
- Brilliant, M.H.; Vaziri, K.; Connor, T.B.; Schwartz, S.G.; Carroll, J.J.; McCarty, C.A.; Schrodi, S.J.; Hebbring, S.J.; Kishor, K.S.; Flynn, H.W.; et al. Mining Retrospective Data for Virtual Prospective Drug Repurposing: L-DOPA and Age-related Macular Degeneration. Am. J. Med. 2016, 129, 292–298. [Google Scholar] [CrossRef] [Green Version]
- Figueroa, A.G.; Boyd, B.M.; Christensen, C.A.; Javid, C.G.; McKay, B.S.; Fagan, T.C.; Snyder, R.W. Levodopa Positively Affects Neovascular Age-Related Macular Degeneration. Am. J. Med. 2021, 134, 122–128.e123. [Google Scholar] [CrossRef]
- Jabbehdari, S.; Handa, J.T. Oxidative stress as a therapeutic target for the prevention and treatment of early age-related macular degeneration. Surv. Ophthalmol. 2021, 66, 423–440. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, X.; Li, X.; Zeng, Z.; Strang, N.; Shu, X.; Tan, Z. Non-neglectable therapeutic options for age-related macular degeneration: A promising perspective from traditional Chinese medicine. J. Ethnopharmacol. 2022, 282, 114531. [Google Scholar] [CrossRef] [PubMed]
- Suri, R.; Neupane, Y.R.; Jain, G.K.; Kohli, K. Recent theranostic paradigms for the management of Age-related macular degeneration. Eur. J. Pharm. Sci. 2020, 153, 105489. [Google Scholar] [CrossRef]
- Tuo, J.; Ross, R.J.; Herzlich, A.A.; Shen, D.; Ding, X.; Zhou, M.; Coon, S.L.; Hussein, N.; Salem, N., Jr.; Chan, C.C. A high omega-3 fatty acid diet reduces retinal lesions in a murine model of macular degeneration. Am. J. Pathol. 2009, 175, 799–807. [Google Scholar] [CrossRef] [Green Version]
- Georgiou, T.; Neokleous, A.; Nicolaou, D.; Sears, B. Pilot study for treating dry age-related macular degeneration (AMD) with high-dose omega-3 fatty acids. Pharma Nutrition 2014, 2, 8–11. [Google Scholar] [CrossRef]
- van Leeuwen, E.M.; Emri, E.; Merle, B.M.J.; Colijn, J.M.; Kersten, E.; Cougnard-Gregoire, A.; Dammeier, S.; Meester-Smoor, M.; Pool, F.M.; de Jong, E.K.; et al. A new perspective on lipid research in age-related macular degeneration. Prog. Retin. Eye Res. 2018, 67, 56–86. [Google Scholar] [CrossRef]
- Fan, H.; Song, J.T. Potential mechanisms of macular degeneration protection by fatty fish consumption. Curr. Opin. Pharm. 2022, 63, 102186. [Google Scholar] [CrossRef]
- Kaarniranta, K.; Salminen, A. NF-kappaB signaling as a putative target for omega-3 metabolites in the prevention of age-related macular degeneration (AMD). Exp. Gerontol. 2009, 44, 685–688. [Google Scholar] [CrossRef] [PubMed]
- Querques, G.; Souied, E.H. The role of omega-3 and micronutrients in age-related macular degeneration. Surv. Ophthalmol. 2014, 59, 532–539. [Google Scholar] [CrossRef]
- Jiang, H.; Shi, X.; Fan, Y.; Wang, D.; Li, B.; Zhou, J.; Pei, C.; Ma, L. Dietary omega-3 polyunsaturated fatty acids and fish intake and risk of age-related macular degeneration. Clin. Nutr. 2021, 40, 5662–5673. [Google Scholar] [CrossRef]
- McCusker, M.M.; Durrani, K.; Payette, M.J.; Suchecki, J. An eye on nutrition: The role of vitamins, essential fatty acids, and antioxidants in age-related macular degeneration, dry eye syndrome, and cataract. Clin. Derm. 2016, 34, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Gammone, M.A.; Riccioni, G.; D’Orazio, N. Carotenoids: Potential allies of cardiovascular health? Food Nutr. Res. 2015, 59, 26762. [Google Scholar] [CrossRef] [Green Version]
- Mitra, S.; Rauf, A.; Tareq, A.M.; Jahan, S.; Emran, T.B.; Shahriar, T.G.; Dhama, K.; Alhumaydhi, F.A.; Aljohani, A.S.M.; Rebezov, M.; et al. Potential health benefits of carotenoid lutein: An updated review. Food Chem. Toxicol. 2021, 154, 112328. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Kijlstra, A.; Webers, C.A.B.; Berendschot, T. Lutein and Factor D: Two intriguing players in the field of age-related macular degeneration. Arch. Biochem. Biophys. 2015, 572, 49–53. [Google Scholar] [CrossRef]
- Loane, E.; Nolan, J.M.; O’Donovan, O.; Bhosale, P.; Bernstein, P.S.; Beatty, S. Transport and retinal capture of lutein and zeaxanthin with reference to age-related macular degeneration. Surv. Ophthalmol. 2008, 53, 68–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, I.Y. Macular pigment: New clinical methods of detection and the role of carotenoids in age-related macular degeneration. Optometry 2008, 79, 266–272. [Google Scholar] [CrossRef]
- Richer, S.; Stiles, W.; Statkute, L.; Pulido, J.; Frankowski, J.; Rudy, D.; Pei, K.; Tsipursky, M.; Nyland, J. Double-masked, placebo-controlled, randomized trial of lutein and antioxidant supplementation in the intervention of atrophic age-related macular degeneration: The Veterans LAST study (Lutein Antioxidant Supplementation Trial). Optom.-J. Am. Optom. Assoc. 2004, 75, 216–229. [Google Scholar] [CrossRef]
- Robman, L.; Vu, H.; Hodge, A.; Tikellis, G.; Dimitrov, P.; McCarty, C.; Guymer, R. Dietary lutein, zeaxanthin, and fats and the progression of age-related macular degeneration. Can. J. Ophthalmol. 2007, 42, 720–726. [Google Scholar] [CrossRef]
- Peng, M.-L.; Chiu, H.-F.; Chou, H.; Liao, H.-J.; Chen, S.-T.; Wong, Y.-C.; Shen, Y.-C.; Venkatakrishnan, K.; Wang, C.-K. Influence/impact of lutein complex (marigold flower and wolfberry) on visual function with early age-related macular degeneration subjects: A randomized clinical trial. J. Funct. Foods 2016, 24, 122–130. [Google Scholar] [CrossRef]
- Ozawa, Y. Oxidative stress in the light-exposed retina and its implication in age-related macular degeneration. Redox Biol. 2020, 37, 101779. [Google Scholar] [CrossRef] [PubMed]
- Chew, E.Y. Age-related Macular Degeneration: Nutrition, Genes and Deep Learning-The LXXVI Edward Jackson Memorial Lecture. Am. J. Ophthalmol. 2020, 217, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Agrón, E.; Mares, J.; Clemons, T.E.; Swaroop, A.; Chew, E.Y.; Keenan, T.D.L. Dietary Nutrient Intake and Progression to Late Age-Related Macular Degeneration in the Age-Related Eye Disease Studies 1 and 2. Ophthalmology 2021, 128, 425–442. [Google Scholar] [CrossRef] [PubMed]
- Young, C.M.; Quinn, C.; Trusheim, M.R. Durable cell and gene therapy potential patient and financial impact: US projections of product approvals, patients treated, and product revenues. Drug Discov. Today 2022, 27, 17–30. [Google Scholar] [CrossRef]
- Sanie-Jahromi, F.; Nowroozzadeh, M.H. RPE based gene and cell therapy for inherited retinal diseases: A review. Exp. Eye Res. 2022, 217, 108961. [Google Scholar] [CrossRef] [PubMed]
- Potilinski, M.C.; Tate, P.S.; Lorenc, V.E.; Gallo, J.E. New insights into oxidative stress and immune mechanisms involved in age-related macular degeneration tackled by novel therapies. Neuropharmacology 2021, 188, 108513. [Google Scholar] [CrossRef]
- Gorin, M.B.; daSilva, M.J. Predictive genetics for AMD: Hype and hopes for genetics-based strategies for treatment and prevention. Exp. Eye Res. 2020, 191, 107894. [Google Scholar] [CrossRef]
- Kumar Dubey, S.; Pradhan, R.; Hejmady, S.; Singhvi, G.; Choudhury, H.; Gorain, B.; Kesharwani, P. Emerging innovations in nano-enabled therapy against age-related macular degeneration: A paradigm shift. Int. J. Pharm. 2021, 600, 120499. [Google Scholar] [CrossRef]
- Pan, X.; Veroniaina, H.; Su, N.; Sha, K.; Jiang, F.; Wu, Z.; Qi, X. Applications and developments of gene therapy drug delivery systems for genetic diseases. Asian J. Pharm. Sci. 2021, 16, 687–703. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Alu, A.; Liu, H.; Shi, Y.; Wei, X.; Cai, L.; Wei, Y. Biomaterial-assisted biotherapy: A brief review of biomaterials used in drug delivery, vaccine development, gene therapy, and stem cell therapy. Bioact. Mater. 2022, 17, 29–48. [Google Scholar] [CrossRef] [PubMed]
- Lores-Motta, L.; van Beek, A.E.; Willems, E.; Zandstra, J.; van Mierlo, G.; Einhaus, A.; Mary, J.L.; Stucki, C.; Bakker, B.; Hoyng, C.B.; et al. Common haplotypes at the CFH locus and low-frequency variants in CFHR2 and CFHR5 associate with systemic FHR concentrations and age-related macular degeneration. Am. J. Hum. Genet. 2021, 108, 1367–1384. [Google Scholar] [CrossRef] [PubMed]
- Colijn, J.M.; Meester-Smoor, M.; Verzijden, T.; de Breuk, A.; Silva, R.; Merle, B.M.J.; Cougnard-Grégoire, A.; Hoyng, C.B.; Fauser, S.; Coolen, A.; et al. Genetic Risk, Lifestyle, and Age-Related Macular Degeneration in Europe: The EYE-RISK Consortium. Ophthalmology 2021, 128, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Ohno, Y.; Yako, T.; Satoh, K.; Nagase, H.; Shitara, A.; Hara, H.; Kashimata, M. Retinal damage alters gene expression profile in lacrimal glands of mice. J. Pharm. Sci. 2022, 149, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Iejima, D.; Nakayama, M.; Suga, A.; Noda, T.; Kaur, I.; Das, T.; Chakrabarti, S.; Guymer, R.H.; DeAngelis, M.M.; et al. Binding of Gtf2i-beta/delta transcription factors to the ARMS2 gene leads to increased circulating HTRA1 in AMD patients and in vitro. J. Biol. Chem. 2021, 296, 100456. [Google Scholar] [CrossRef] [PubMed]
- Mettu, P.S.; Allingham, M.J.; Cousins, S.W. Incomplete response to Anti-VEGF therapy in neovascular AMD: Exploring disease mechanisms and therapeutic opportunities. Prog. Retin. Eye Res. 2021, 82, 100906. [Google Scholar] [CrossRef]
- Bordet, T.; Behar-Cohen, F. Ocular gene therapies in clinical practice: Viral vectors and nonviral alternatives. Drug Discov. Today 2019, 24, 1685–1693. [Google Scholar] [CrossRef] [PubMed]
- Dewell, T.E.; Gjoni, K.; Liu, A.Z.; Libby, A.R.G.; Moore, A.T.; So, P.L.; Conklin, B.R. Transcription factor overexpression drives reliable differentiation of retinal pigment epithelium from human induced pluripotent stem cells. Stem. Cell Res. 2021, 53, 102368. [Google Scholar] [CrossRef]
- Hyttinen, J.M.T.; Blasiak, J.; Felszeghy, S.; Kaarniranta, K. MicroRNAs in the regulation of autophagy and their possible use in age-related macular degeneration therapy. Ageing Res. Rev. 2021, 67, 101260. [Google Scholar] [CrossRef]
- Lin, F.L.; Wang, P.Y.; Chuang, Y.F.; Wang, J.H.; Wong, V.H.Y.; Bui, B.V.; Liu, G.S. Gene Therapy Intervention in Neovascular Eye Disease: A Recent Update. Mol. Ther. 2020, 28, 2120–2138. [Google Scholar] [CrossRef] [PubMed]
- Sharma, K.; Sharma, N.K.; Singh, R.; Sharma, S.K.; Anand, A. Gene networks determine predisposition to AMD. Genomics 2021, 113, 514–522. [Google Scholar] [CrossRef]
- Xu, D.; Khan, M.A.; Ho, A.C. Creating an Ocular Biofactory: Surgical Approaches in Gene Therapy for Acquired Retinal Diseases. Asia-Pac. J. Ophthalmol. 2021, 10, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Truong, V.; Viken, K.; Geng, Z.; Barkan, S.; Johnson, B.; Ebeling, M.C.; Montezuma, S.R.; Ferrington, D.A.; Dutton, J.R. Automating Human Induced Pluripotent Stem Cell Culture and Differentiation of iPSC-Derived Retinal Pigment Epithelium for Personalized Drug Testing. SLAS Technol. 2021, 26, 287–299. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Shang, B.; Yang, P.; Cao, Z.; Pan, Y.; Zhou, Q. Induced pluripotent stem cell consensus genes: Implication for the risk of tumorigenesis and cancers in induced pluripotent stem cell therapy. Stem. Cells Dev. 2012, 21, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Wuputra, K.; Ku, C.-C.; Wu, D.-C.; Lin, Y.-C.; Saito, S.; Yokoyama, K.K. Prevention of tumor risk associated with the reprogramming of human pluripotent stem cells. J. Exp. Clin. Cancer Res. 2020, 39, 100. [Google Scholar] [CrossRef]
- Wang, G.; Heimendinger, P.; Ramelmeier, R.A.; Wang, W. Pluripotent stem cell-based cell therapies: Current applications and future prospects. Curr. Opin. Biomed. Eng. 2022, 22, 100390. [Google Scholar] [CrossRef]
- Maeda, T.; Mandai, M.; Sugita, S.; Kime, C.; Takahashi, M. Strategies of pluripotent stem cell-based therapy for retinal degeneration: Update and challenges. Trends Mol. Med. 2022, 28, 388–404. [Google Scholar] [CrossRef]
- Fernandes, A.R.; Santos, T.D.; Granja, P.L.; Sanchez-Lopez, E.; Santini, A.; Garcia, M.L.; Silva, A.M.; Souto, E.B. DABCO-Customized Nanoemulsions: Characterization, Cell Viability and Genotoxicity in Retinal Pigmented Epithelium and Microglia Cells. Pharmaceutics 2021, 13, 1652. [Google Scholar] [CrossRef]
- Fernandes, A.R.; Sanchez-Lopez, E.; Santos, T.D.; Garcia, M.L.; Silva, A.M.; Souto, E.B. Development and Characterization of Nanoemulsions for Ophthalmic Applications: Role of Cationic Surfactants. Materials 2021, 14, 7541. [Google Scholar] [CrossRef]
- Yang, B.; Li, G.; Liu, J.; Li, X.; Zhang, S.; Sun, F.; Liu, W. Nanotechnology for Age-Related Macular Degeneration. Pharmaceutics 2021, 13, 2035. [Google Scholar] [CrossRef]
- Al-Halafi, A.M. Nanocarriers of nanotechnology in retinal diseases. Saudi. J. Ophthalmol. 2014, 28, 304–309. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-López, E.; Espina, M.; Doktorovova, S.; Souto, E.B.; García, M.L. Lipid nanoparticles (SLN, NLC): Overcoming the anatomical and physiological barriers of the eye-Part I-Barriers and determining factors in ocular delivery. Eur. J. Pharm. Biopharm. 2017, 110, 70–75. [Google Scholar] [CrossRef]
- Bohley, M.; Dillinger, A.E.; Tamm, E.R.; Goepferich, A. Targeted drug delivery to the retinal pigment epithelium: Untapped therapeutic potential for retinal diseases. Drug Discov. Today 2022, 27, 2497–2509. [Google Scholar] [CrossRef]
- Kesharwani, P.; Choudhury, H.; Meher, J.G.; Pandey, M.; Gorain, B. Dendrimer-entrapped gold nanoparticles as promising nanocarriers for anticancer therapeutics and imaging. Prog. Mater. Sci. 2019, 103, 484–508. [Google Scholar] [CrossRef]
- Yadav, M.; Schiavone, N.; Guzman-Aranguez, A.; Giansanti, F.; Papucci, L.; Perez de Lara, M.J.; Singh, M.; Kaur, I.P. Atorvastatin-loaded solid lipid nanoparticles as eye drops: Proposed treatment option for age-related macular degeneration (AMD). Drug Deliv. Transl. Res. 2020, 10, 919–944. [Google Scholar] [CrossRef] [PubMed]
- Moghassemi, S.; Dadashzadeh, A.; Azevedo, R.B.; Feron, O.; Amorim, C.A. Photodynamic cancer therapy using liposomes as an advanced vesicular photosensitizer delivery system. J. Control. Release 2021, 339, 75–90. [Google Scholar] [CrossRef] [PubMed]
- Qiao, H.; Xu, Z.; Sun, M.; Fu, S.; Zhao, F.; Wang, D.; He, Z.; Zhai, Y.; Sun, J. Rebamipide liposome as an effective ocular delivery system for the management of dry eye disease. J. Drug Deliv. Sci. Technol. 2022, 75, 103654. [Google Scholar] [CrossRef]
- Suri, R.; Neupane, Y.R.; Mehra, N.; Jain, G.K.; Kohli, K. Sirolimus loaded polyol modified liposomes for the treatment of Posterior Segment Eye Diseases. Med. Hypotheses 2020, 136, 109518. [Google Scholar] [CrossRef] [PubMed]
- Karumanchi, D.K.; Skrypai, Y.; Thomas, A.; Gaillard, E.R. Rational design of liposomes for sustained release drug delivery of bevacizumab to treat ocular angiogenesis. J. Drug Deliv. Sci. Technol. 2018, 47, 275–282. [Google Scholar] [CrossRef]
- Ghezzi, M.; Ferraboschi, I.; Delledonne, A.; Pescina, S.; Padula, C.; Santi, P.; Sissa, C.; Terenziani, F.; Nicoli, S. Cyclosporine-loaded micelles for ocular delivery: Investigating the penetration mechanisms. J. Control. Release 2022, 349, 744–755. [Google Scholar] [CrossRef]
- Alshamrani, M.; Sikder, S.; Coulibaly, F.; Mandal, A.; Pal, D.; Mitra, A.K. Self-Assembling Topical Nanomicellar Formulation to Improve Curcumin Absorption Across Ocular Tissues. AAPS PharmSciTech. 2019, 20, 254. [Google Scholar] [CrossRef]
- Gote, V.; Mandal, A.; Alshamrani, M.; Pal, D. Self-Assembling Tacrolimus Nanomicelles for Retinal Drug Delivery. Pharmaceutics 2020, 12, 1072. [Google Scholar] [CrossRef]
- Patel, V.; Patel, P.; Patel, J.V.; Patel, P.M. Dendrimer as a versatile platform for biomedical application: A review. J. Indian Chem. Soc. 2022, 99, 100516. [Google Scholar] [CrossRef]
- Lai, S.; Wei, Y.; Wu, Q.; Zhou, K.; Liu, T.; Zhang, Y.; Jiang, N.; Xiao, W.; Chen, J.; Liu, Q.; et al. Liposomes for effective drug delivery to the ocular posterior chamber. J. Nanobiotechnol. 2019, 17, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ge, Y.; Zhang, A.; Sun, R.; Xu, J.; Yin, T.; He, H.; Gou, J.; Kong, J.; Zhang, Y.; Tang, X. Penetratin-modified lutein nanoemulsion in-situ gel for the treatment of age-related macular degeneration. Expert Opin. Drug Deliv. 2020, 17, 603–619. [Google Scholar] [CrossRef] [PubMed]
- Laradji, A.M.; Kolesnikov, A.V.; Karakoçak, B.B.; Kefalov, V.J.; Ravi, N. Redox-Responsive Hyaluronic Acid-Based Nanogels for the Topical Delivery of the Visual Chromophore to Retinal Photoreceptors. ACS Omega 2021, 6, 6172–6184. [Google Scholar] [CrossRef]
- Fernandes, A.R.; Vidal, L.B.; Sánchez-López, E.; dos Santos, T.; Granja, P.L.; Silva, A.M.; Garcia, M.L.; Souto, E.B. Customized cationic nanoemulsions loading triamcinolone acetonide for corneal neovascularization secondary to inflammatory processes. Int. J. Pharm. 2022, 623, 121938. [Google Scholar] [CrossRef]
- Araujo, J.; Garcia, M.L.; Mallandrich, M.; Souto, E.B.; Calpena, A.C. Release profile and transscleral permeation of triamcinolone acetonide loaded nanostructured lipid carriers (TA-NLC): In vitro and ex vivo studies. Nanomedicine 2012, 8, 1034–1041. [Google Scholar] [CrossRef]
- Araujo, J.; Gonzalez-Mira, E.; Egea, M.A.; Garcia, M.L.; Souto, E.B. Optimization and physicochemical characterization of a triamcinolone acetonide-loaded NLC for ocular antiangiogenic applications. Int. J. Pharm. 2010, 393, 167–175. [Google Scholar] [CrossRef]
- Sanchez-Lopez, E.; Esteruelas, G.; Ortiz, A.; Espina, M.; Prat, J.; Munoz, M.; Cano, A.; Calpena, A.C.; Ettcheto, M.; Camins, A.; et al. Dexibuprofen Biodegradable Nanoparticles: One Step Closer towards a Better Ocular Interaction Study. Nanomaterials 2020, 10, 720. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Lopez, E.; Egea, M.A.; Davis, B.M.; Guo, L.; Espina, M.; Silva, A.M.; Calpena, A.C.; Souto, E.M.B.; Ravindran, N.; Ettcheto, M.; et al. Memantine-Loaded PEGylated Biodegradable Nanoparticles for the Treatment of Glaucoma. Small 2018, 14, 1808. [Google Scholar] [CrossRef]
- Sanchez-Lopez, E.; Egea, M.A.; Cano, A.; Espina, M.; Calpena, A.C.; Ettcheto, M.; Camins, A.; Souto, E.B.; Silva, A.M.; Garcia, M.L. PEGylated PLGA nanospheres optimized by design of experiments for ocular administration of dexibuprofen-in vitro, ex vivo and in vivo characterization. Colloids Surf. B Biointerfaces 2016, 145, 241–250. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Mittal, S. Nanotechnology: Revolutionizing the delivery of drugs to treat age-related macular degeneration. Expert Opin Drug Deliv 2021, 18, 1131–1149. [Google Scholar] [CrossRef] [PubMed]
- Abedin Zadeh, M.; Khoder, M.; Al-Kinani, A.A.; Younes, H.M.; Alany, R.G. Retinal cell regeneration using tissue engineered polymeric scaffolds. Drug Discov. Today 2019, 24, 1669–1678. [Google Scholar] [CrossRef] [PubMed]
- Tan, G.; Ioannou, N.; Mathew, E.; Tagalakis, A.D.; Lamprou, D.A.; Yu-Wai-Man, C. 3D printing in Ophthalmology: From medical implants to personalised medicine. Int. J. Pharm. 2022, 625, 122094. [Google Scholar] [CrossRef] [PubMed]
- Lorber, B.; Hsiao, W.K.; Martin, K.R. Three-dimensional printing of the retina. Curr. Opin. Ophthalmol. 2016, 27, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Shi, P.; Edgar, T.Y.S.; Yeong, W.Y.; Laude, A. Hybrid three-dimensional (3D) bioprinting of retina equivalent for ocular research. Int. J. Bioprint. 2017, 3, 008. [Google Scholar] [CrossRef] [Green Version]
- Masaeli, E.; Forster, V.; Picaud, S.; Karamali, F.; Nasr-Esfahani, M.H.; Marquette, C. Tissue engineering of retina through high resolution 3-dimensional inkjet bioprinting. Biofabrication 2020, 12, 025006. [Google Scholar] [CrossRef]
- Ueda-Arakawa, N.; Ooto, S.; Tsujikawa, A.; Yamashiro, K.; Oishi, A.; Yoshimura, N. Sensitivity and specificity of detecting reticular pseudodrusen in multimodal imaging in Japanese patients. Retina 2013, 33, 490–497. [Google Scholar] [CrossRef]
- Cicinelli, M.V.; Rabiolo, A.; Sacconi, R.; Carnevali, A.; Querques, L.; Bandello, F.; Querques, G. Optical coherence tomography angiography in dry age-related macular degeneration. Surv. Ophthalmol. 2018, 63, 236–244. [Google Scholar] [CrossRef]
- Toto, L.; Borrelli, E.; Di Antonio, L.; Carpineto, P.; Mastropasqua, R. Retinal vascular plexuses’ changes in dry age-related macular degeneration, evaluated by means of optical coherence tomography angiography. Retina 2016, 36, 1566–1572. [Google Scholar] [CrossRef]
- Mokwa, N.F.; Ristau, T.; Keane, P.A.; Kirchhof, B.; Sadda, S.R.; Liakopoulos, S. Grading of age-related macular degeneration: Comparison between color fundus photography, fluorescein angiography, and spectral domain optical coherence tomography. J. Ophthalmol. 2013, 2013, 385915. [Google Scholar] [CrossRef] [Green Version]
- Ly, A.; Nivison-Smith, L.; Zangerl, B.; Assaad, N.; Kalloniatis, M. Advanced imaging for the diagnosis of age-related macular degeneration: A case vignettes study. Clin. Exp. Optom. 2018, 101, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Ly, A.; Nivison-Smith, L.; Assaad, N.; Kalloniatis, M. Fundus autofluorescence in age-related macular degeneration. Optom. Vis. Sci. 2017, 94, 246. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, P.; Fnu, G.; Bhatia, D.; Shahid, A.; Sutariya, V. Nanodelivery of Resveratrol-Loaded PLGA Nanoparticles for Age-Related Macular Degeneration. AAPS PharmSciTech. 2020, 21, 291. [Google Scholar] [CrossRef] [PubMed]
- Galindo, R.; Sánchez-López, E.; Gómara, M.J.; Espina, M.; Ettcheto, M.; Cano, A.; Haro, I.; Camins, A.; García, M.L. Development of Peptide Targeted PLGA-PEGylated Nanoparticles Loading Licochalcone-A for Ocular Inflammation. Pharmaceutics 2022, 14, 285. [Google Scholar] [CrossRef]
- Suri, R.; Neupane, Y.R.; Mehra, N.; Nematullah, M.; Khan, F.; Alam, O.; Iqubal, A.; Jain, G.K.; Kohli, K. Sirolimus loaded chitosan functionalized poly (lactic-co-glycolic acid) (PLGA) nanoparticles for potential treatment of age-related macular degeneration. Int. J. Biol. Macromol. 2021, 191, 548–559. [Google Scholar] [CrossRef]
- Bolla, P.K.; Gote, V.; Singh, M.; Patel, M.; Clark, B.A.; Renukuntla, J. Lutein-Loaded, Biotin-Decorated Polymeric Nanoparticles Enhance Lutein Uptake in Retinal Cells. Pharmaceutics 2020, 12, 798. [Google Scholar] [CrossRef] [PubMed]
- Narvekar, P.; Bhatt, P.; Fnu, G.; Sutariya, V. Axitinib-Loaded Poly(Lactic-Co-Glycolic Acid) Nanoparticles for Age-Related Macular Degeneration: Formulation Development and In Vitro Characterization. Assay Drug Dev. Technol. 2019, 17, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhang, X.; Li, G.; Xu, F.; Li, S.; Teng, L.; Li, Y.; Sun, F. Anti-Angiogenic Activity Of Bevacizumab-Bearing Dexamethasone-Loaded PLGA Nanoparticles For Potential Intravitreal Applications. Int. J. Nanomed. 2019, 14, 8819–8834. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Liu, C.H.; Ji, T.; Mehta, M.; Wang, W.; Marino, E.; Chen, J.; Kohane, D.S. Intravenous treatment of choroidal neovascularization by photo-targeted nanoparticles. Nat. Commun. 2019, 10, 804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, F.; Meng, T.; Chen, Q.; Zhou, K.; Shao, Y.; Matlock, G.; Ma, X.; Wu, W.; Du, Y.; Wang, X.; et al. Fenofibrate-Loaded Biodegradable Nanoparticles for the Treatment of Experimental Diabetic Retinopathy and Neovascular Age-Related Macular Degeneration. Mol. Pharm. 2019, 16, 1958–1970. [Google Scholar] [CrossRef] [PubMed]




| Drug | Clinical Dose for AMD (mg) | Structure | MOA | Limitations | FDA Approval |
|---|---|---|---|---|---|
| Ranibizumab® | 0.5 | Fab fragment | Anti–VEGF-A | Time intervals between injections lower than Faricimab®. | 2006 |
| Bevacizumab® | 1.25 | Full antibody (IgG1) | Anti–VEGF-A | Not approved by FDA. Higher dose required than Ranibizumab®. | Not approved |
| Aflibercept® | 2.0 | VEGFR1/2-Fc fusion protein | Anti–VEGF-A/PIGF/VEGF-B | Lower safety and efficacy than Brolucizumab®. | 2011 |
| Ziv-Aflibercept® | 1.25 | VEGFR1/2-Fc fusion protein | Anti–VEGF-A/PIGF/VEGF-B | Not approved by FDA Higher dose required than Ranibizumab®. | Not approved |
| Conbercept® | 0.5 | VEGFR1/2-Fc fusion protein | Anti–VEGF-A/VEGF-B/VEGF-C/and PIGF | Not approved by FDA Higher dose required than Ranibizumab®. | Not approved |
| Brolucizumab® | 6.0 | scFv | Anti–VEGF-A | Higher dose required than Ranibizumab®. | 2019 |
| Faricimab® | 6.0 | Angiopoietin-2 | Anti–VEGF-A | Higher dose required than Ranibizumab®. | 2022 |
| Drug | MOA | Retinal Findings | Limitations | References |
|---|---|---|---|---|
| Lutein, β-carotene and zeaxanthin | Protection of RPE from oxidative stress. |
| In large doses, β-carotene can cause lung and gastric cancer in smokers. This is the reason why it isn’t recommended in these patients. | [42,43,44,46,47,48,49] |
| Antioxidant supplement containing lutein, vitamins A, C and E | Antioxidant activity, Protection of RPE from oxidative stress. | Lutein and zeaxanthin were the most strongly associated with AMD. | No effectiveness in advanced macular degeneration in both eyes. | [18] |
| EPA and DHA | Antiangiogenic and anti-inflammatory effects, protecting the retina against oxidative stress. | Significant improvement in vision acuity occurred was observed in AMD patients after Omega-3 supplementation. | More clinical studies are needed to confirm its effectiveness. | [34,35,36,38,39,40] |
| Omega-3 + anti-VEFG | VEGF limited via anti-VEGF molecules, antiangiogenic and anti-inflammatory effects, lowering oxidative stress in the retina. | Omega-3 supplementation combined with anti-VEGF treatment was associated with decreased vitreal VEGF-A levels in wet AMD patients. | More clinical studies are needed to confirm its effectiveness. | [27] |
| Drug | MOA | Retinal Findings | Limitations | References |
|---|---|---|---|---|
| Cerium oxide nanoparticles | Simulation of the activity of superoxide dismutase and catalase preventing retinal function loss and preserving retinal morphology. |
| Further evaluation is needed beyond these in vitro studies. | [25,31,32,50] |
| Curcumin | Regulation of the expression of oxidative stress biomarkers and apoptosis-associated proteins such as AKT, Nrf2, cytokines, and NF-kB. | Treatment with curcumin can regulate oxidative stress and apoptosis in in vitro studies. | Further studies are needed to fully assess curcumin’s potential as an antioxidant therapy for early AMD. | [31,32] |
| Fucoidan | Reduction of the expression of VEGF in RPE and choroidal cells that could decrease angiogenesis. Downregulation hypoxia inducible factor-1a/VEGF and PI3K/Akt signaling. | Promising results in in vitro studies. Further evaluation is needed for treating early AMD. | Further evaluation is needed beyond these in vitro studies. | [31,32] |
| Flavonoids | Inhibition of NF-kB and activation of AP-1 and Nrf2. Regulation of IL-6/JAK2/ STAT3 signaling pathway in RPE cells, which has been implicated in AMD pathobiology. |
| Further evaluation is needed. | [31,32] |
| Quercetin | Activation of the intracellular redox system including Nrf2 signaling, the caveolin-1 pathway, proinflammatory cytokines, and apoptosis. | Inhibition of a VEGF-induced inflammatory response through MAPK/Akt signaling, NF-kB translocation in mouse RPE cells, and the formation of choroidal neovascularization in both in vitro and in vivo models of AMD treatment of both dry and wet AMD. | Further evaluation is needed beyond these in vitro studies. | [31,32] |
| Coenzyme Q10 | Essential component of the electron transport chain necessary for respiration with ROS-scavenging ability |
| Further evaluation is needed. | [23,31,32,51] |
| Nutrient | AREDS Formula * | AREDS2 Formula |
|---|---|---|
| Vitamin C | 500 mg | 500 mg |
| Vitamin E | 400 IU | 400 IU |
| Beta-carotene | 15 mg | - |
| Copper (cupric oxide) ** | 2 mg | 2 mg |
| Lutein | - | 10 mg |
| Zeaxanthin | - | 2 mg |
| Zinc | 80 mg | 80 mg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galindo-Camacho, R.M.; Blanco-Llamero, C.; da Ana, R.; Fuertes, M.A.; Señoráns, F.J.; Silva, A.M.; García, M.L.; Souto, E.B. Therapeutic Approaches for Age-Related Macular Degeneration. Int. J. Mol. Sci. 2022, 23, 11769. https://doi.org/10.3390/ijms231911769
Galindo-Camacho RM, Blanco-Llamero C, da Ana R, Fuertes MA, Señoráns FJ, Silva AM, García ML, Souto EB. Therapeutic Approaches for Age-Related Macular Degeneration. International Journal of Molecular Sciences. 2022; 23(19):11769. https://doi.org/10.3390/ijms231911769
Chicago/Turabian StyleGalindo-Camacho, Ruth M., Cristina Blanco-Llamero, Raquel da Ana, Mayra A. Fuertes, Francisco J. Señoráns, Amélia M. Silva, María L. García, and Eliana B. Souto. 2022. "Therapeutic Approaches for Age-Related Macular Degeneration" International Journal of Molecular Sciences 23, no. 19: 11769. https://doi.org/10.3390/ijms231911769