
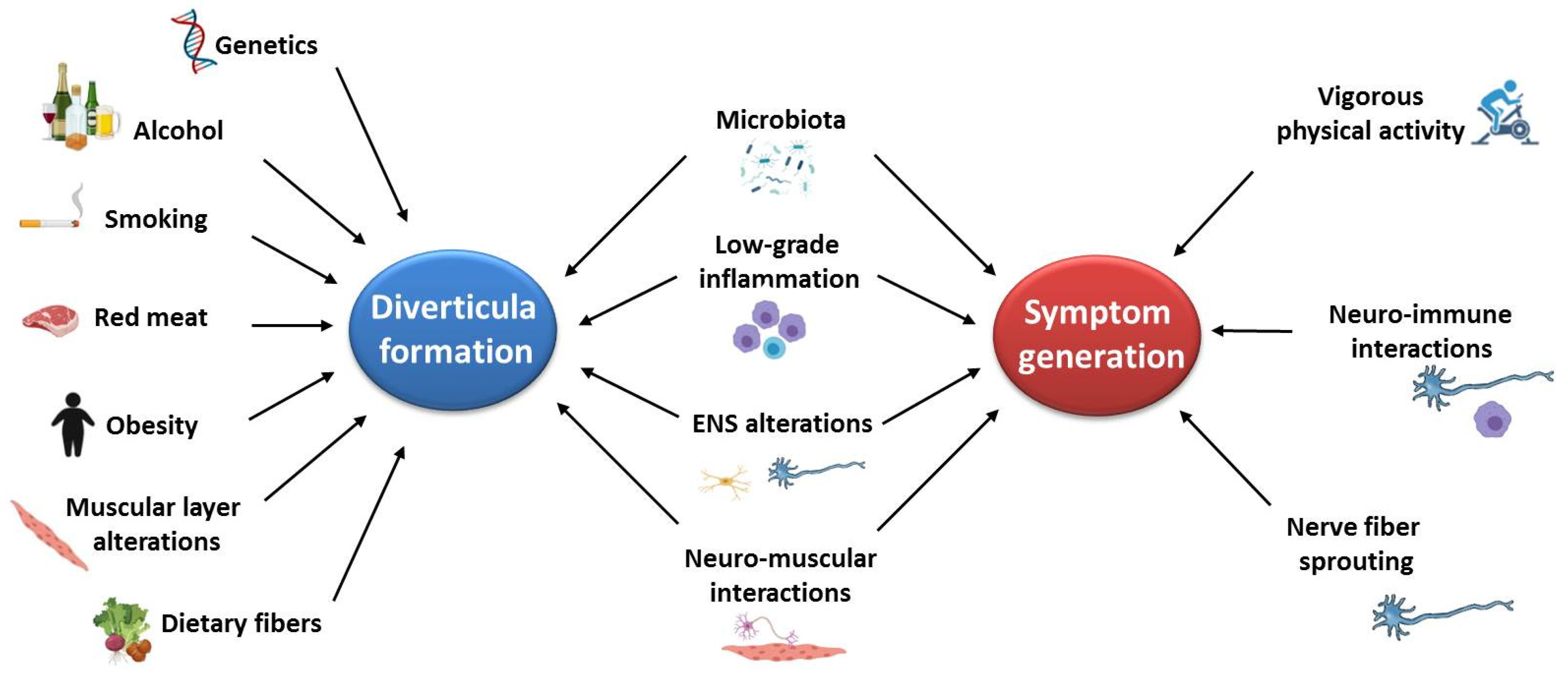
Pathophysiology of Diverticular Disease: From Diverticula Formation to Symptom Generation

 , and
, and
Abstract
:1. Introduction
2. Genetic Factors
3. Environmental Factors
3.1. Dietary Fibers
3.2. Red Meat Intake, Alcohol, Smoking, and Lifestyle
4. Microenvironment
4.1. Microbiota

{kind=link}
{kind=link}
| Authors | Subjects (n) | Samples | Microbial Profiling Method | Outcomes |
|---|---|---|---|---|
| Kvasnovisky et al., 2018 [74] | SUDD (30) | Stools | 16S ribosomal RNA gene sequencing | Positive association between bloating severity score and the relative abundance of Ruminococcus, and a negative correlation between bloating and Roseburia amount. The intensity of pain was significantly associated with Cyanobacterium number. |
| Barbara et al., 2017 [67] | HC (14) Diverticulosis (16) SUDD (8) | Stools Mucosal biopsies | high taxonomic fingerprint (HTF)-Microbi.Array | ↓ Clostridium cluster IV DD vs. HC in stool samples ↓ Clostridium cluster IX SUDD vs. Diverticulosis in stool samples ↓ Fusobacterium spp SUDD vs. Diverticulosis in stool samples ↓ Lactobacillaceae SUDD vs. Diverticulosis in stool samples ↓ Akkermansia muciniphila in SUDD in mucosal biopsy close to diverticula vs. mucosal biopsy far from diverticula |
| Tursi et al., 2016 [68]. | HC (16) Diverticulosis (13) SUDD (15) | Stools | RT-PCR | ↑ Akkermansia muciniphila DD vs. HC |
| Lopetuso et al., 2017 [71] | HC (8) DD (4) IBS (3) UC (5) CD (10) | Stools | 16S ribosomal RNA gene sequencing | ↓ Bacteroides fragilis DD vs. HC ↓ Collinsella aerofaciens DD vs. HC ↓ Collinsella stercoris DD vs. HC |
| Jones et al., 2018 [72] | HC (309) Diverticulosis (226) | Mucosal biopsies | 16S ribosomal RNA gene sequencing | ↓ Proteobacteria vs. HC ↓ Comamonadaceae vs. HC |
4.2. Low-Grade Inflammation
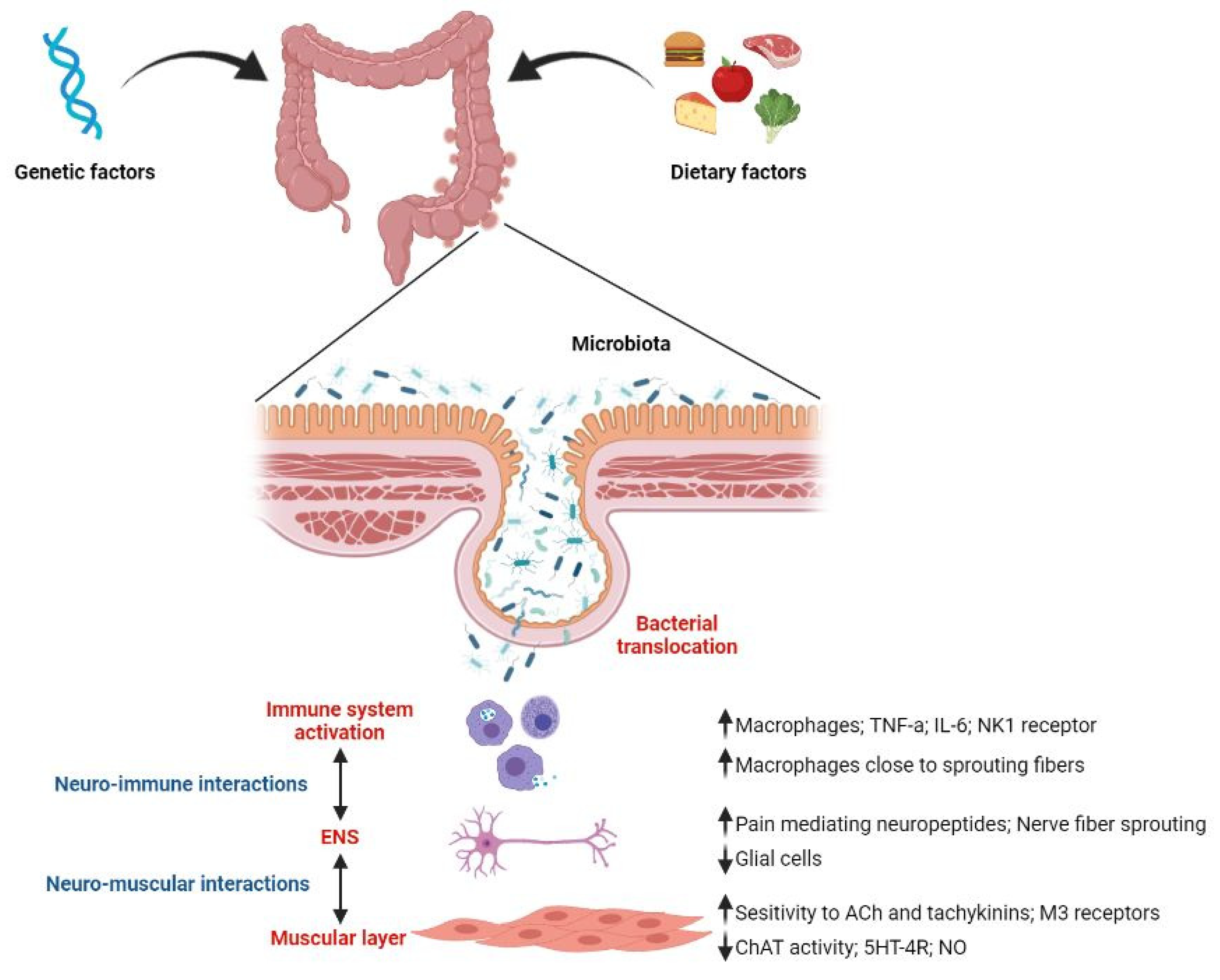
4.3. Enteric Nervous System and Neuro-Immune Interactions
4.4. Muscular Layer and Neuro-Muscular Interactions
5. Future Perspectives
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Cuomo, R.; Barbara, G.; Pace, F.; Annese, V.; Bassotti, G.; Binda, G.A.; Casetti, T.; Colecchia, A.; Festi, D.; Fiocca, R.; et al. Italian consensus conference for colonic diverticulosis and diverticular disease. United Eur. Gastroenterol. J. 2014, 2, 413–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peery, A.F.; Crockett, S.D.; Barritt, A.S.; Dellon, E.S.; Eluri, S.; Gangarosa, L.M.; Jensen, E.T.; Lund, J.L.; Pasricha, S.; Runge, T.; et al. Burden of Gastrointestinal, Liver, and Pancreatic Diseases in the United States. Gastroenterology 2015, 149, 1731–1741.e3. [Google Scholar] [CrossRef] [Green Version]
- Etzioni, D.A.; Mack, T.M.; Beart, R.W., Jr.; Kaiser, A.M. Diverticulitis in the United States: 1998–2005: Changing patterns of disease and treatment. Ann. Surg. 2009, 249, 210–217. [Google Scholar] [CrossRef]
- Everhart, J.E.; Ruhl, C.E. Burden of digestive diseases in the United States part II: Lower gastrointestinal diseases. Gastroenterology 2009, 136, 741–754. [Google Scholar] [CrossRef]
- Tursi, A. Diverticulosis today: Unfashionable and still under-researched. Ther. Adv. Gastroenterol. 2016, 9, 213–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiller, R. Is it diverticular disease or is it irritable bowel syndrome? Dig. Dis. 2012, 30, 64–69. [Google Scholar] [CrossRef]
- Strate, L.L.; Modi, R.; Cohen, E.; Spiegel, B.M. Diverticular disease as a chronic illness: Evolving epidemiologic and clinical insights. Am. J. Gastroenterol. 2012, 107, 1486–1493. [Google Scholar] [CrossRef] [PubMed]
- Violi, A.; Cambie, G.; Miraglia, C.; Barchi, A.; Nouvenne, A.; Capasso, M.; Leandro, G.; Meschi, T.; De’ Angelis, G.L.; Di Mario, F. Epidemiology and risk factors for diverticular disease. Acta Biomed. 2018, 89, 107–112. [Google Scholar] [CrossRef]
- Peery, A.F.; Sandler, R.S. Diverticular disease: Reconsidering conventional wisdom. Clin. Gastroenterol. Hepatol. 2013, 11, 1532–1537. [Google Scholar] [CrossRef] [Green Version]
- Schieffer, K.M.; Kline, B.P.; Yochum, G.S.; Koltun, W.A. Pathophysiology of diverticular disease. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 683–692. [Google Scholar] [CrossRef]
- Rezapour, M.; Ali, S.; Stollman, N. Diverticular Disease: An Update on Pathogenesis and Management. Gut Liver 2018, 12, 125–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young-Fadok, T.M. Diverticulitis. N. Engl. J. Med. 2018, 379, 1635–1642. [Google Scholar] [CrossRef] [PubMed]
- Peery, A.F.; Shaukat, A.; Strate, L.L. AGA Clinical Practice Update on Medical Management of Colonic Diverticulitis: Expert Review. Gastroenterology 2021, 160, 906–911.e1. [Google Scholar] [CrossRef] [PubMed]
- Hjern, F.; Johansson, C.; Mellgren, A.; Baxter, N.N.; Hjern, A. Diverticular disease and migration–the influence of acculturation to a Western lifestyle on diverticular disease. Aliment. Pharmacol. Ther. 2006, 23, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Stemmermann, G.N. Patterns of disease among Japanese living in Hawaii. Arch. Environ. Health 1970, 20, 266–273. [Google Scholar] [CrossRef]
- Lahiri, R.P.; Abeles, A.; Burnand, K.M.; Alazawi, W.; Bhattacharya, S.; Foster, G.R.; Knowles, C.H. A cross sectional study of colonic diverticulosis in the London Bangladeshi population. United Eur. Gastroenterol. J. 2013, 1, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Loffeld, R.J. Diverticulosis of the colon is rare amongst immigrants living in the Zaanstreek region in the Netherlands. Colorectal Dis. 2005, 7, 559–562. [Google Scholar] [CrossRef]
- Beighton, P.H.; Murdoch, J.L.; Votteler, T. Gastrointestinal complications of the Ehlers-Danlos syndrome. Gut 1969, 10, 1004–1008. [Google Scholar] [CrossRef] [Green Version]
- Stagi, S.; Lapi, E.; Chiarelli, F.; de Martino, M. Incidence of diverticular disease and complicated diverticular disease in young patients with Williams syndrome. Pediatric Surg. Int. 2010, 26, 943–944. [Google Scholar] [CrossRef]
- Tursi, A. Current and Evolving Concepts on the Pathogenesis of Diverticular Disease. J. Gastrointest. Liver Dis. 2019, 28, 225–235. [Google Scholar] [CrossRef]
- Granlund, J.; Svensson, T.; Olen, O.; Hjern, F.; Pedersen, N.L.; Magnusson, P.K.; Schmidt, P.T. The genetic influence on diverticular disease—A twin study. Aliment. Pharmacol. Ther. 2012, 35, 1103–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strate, L.L.; Erichsen, R.; Baron, J.A.; Mortensen, J.; Pedersen, J.K.; Riis, A.H.; Christensen, K.; Sorensen, H.T. Heritability and familial aggregation of diverticular disease: A population-based study of twins and siblings. Gastroenterology 2013, 144, 736–742.e1. [Google Scholar] [CrossRef]
- Reichert, M.C.; Kupcinskas, J.; Krawczyk, M.; Jungst, C.; Casper, M.; Grunhage, F.; Appenrodt, B.; Zimmer, V.; Weber, S.N.; Tamelis, A.; et al. A Variant of COL3A1 (rs3134646) Is Associated With Risk of Developing Diverticulosis in White Men. Dis. Colon Rectum 2018, 61, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Connelly, T.M.; Berg, A.S.; Hegarty, J.P.; Deiling, S.; Brinton, D.; Poritz, L.S.; Koltun, W.A. The TNFSF15 gene single nucleotide polymorphism rs7848647 is associated with surgical diverticulitis. Ann. Surg. 2014, 259, 1132–1137. [Google Scholar] [CrossRef]
- Sigurdsson, S.; Alexandersson, K.F.; Sulem, P.; Feenstra, B.; Gudmundsdottir, S.; Halldorsson, G.H.; Olafsson, S.; Sigurdsson, A.; Rafnar, T.; Thorgeirsson, T.; et al. Sequence variants in ARHGAP15, COLQ and FAM155A associate with diverticular disease and diverticulitis. Nat. Commun. 2017, 8, 15789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coble, J.L.; Sheldon, K.E.; Yue, F.; Salameh, T.J.; Harris, L.R., III; Deiling, S.; Ruggiero, F.M.; Eshelman, M.A.; Yochum, G.S.; Koltun, W.A.; et al. Identification of a rare LAMB4 variant associated with familial diverticulitis through exome sequencing. Hum. Mol. Genet. 2017, 26, 3212–3220. [Google Scholar] [CrossRef]
- Nehring, P.; Gromadzka, G.; Giermaziak, A.; Jastrzebski, M.; Przybylkowski, A. Genetic variants of tissue inhibitors of matrix metalloproteinase 1 (rs4898) and 2 (rs8179090) in diverticulosis. Eur. J. Gastroenterol. Hepatol. 2021, 33, e431–e434. [Google Scholar] [CrossRef]
- Mittal, R.; Patel, A.P.; Debs, L.H.; Nguyen, D.; Patel, K.; Grati, M.; Mittal, J.; Yan, D.; Chapagain, P.; Liu, X.Z. Intricate Functions of Matrix Metalloproteinases in Physiological and Pathological Conditions. J. Cell. Physiol. 2016, 231, 2599–2621. [Google Scholar] [CrossRef]
- Reichert, M.C.; Kupcinskas, J.; Schulz, A.; Schramm, C.; Weber, S.N.; Krawczyk, M.; Jungst, C.; Casper, M.; Grunhage, F.; Appenrodt, B.; et al. Common variation in FAM155A is associated with diverticulitis but not diverticulosis. Sci. Rep. 2020, 10, 1658. [Google Scholar] [CrossRef]
- Strate, L.L.; Morris, A.M. Epidemiology, Pathophysiology, and Treatment of Diverticulitis. Gastroenterology 2019, 156, 1282–1298.e1. [Google Scholar] [CrossRef] [Green Version]
- Camilleri, M.; Sandler, R.S.; Peery, A.F. Etiopathogenetic Mechanisms in Diverticular Disease of the Colon. Cell. Mol. Gastroenterol. Hepatol. 2020, 9, 15–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chua, H.C.; Wulf, M.; Weidling, C.; Rasmussen, L.P.; Pless, S.A. The NALCN channel complex is voltage sensitive and directly modulated by extracellular calcium. Sci. Adv. 2020, 6, eaaz3154. [Google Scholar] [CrossRef] [Green Version]
- Ren, D. Sodium leak channels in neuronal excitability and rhythmic behaviors. Neuron 2011, 72, 899–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nash, H.A.; Scott, R.L.; Lear, B.C.; Allada, R. An unusual cation channel mediates photic control of locomotion in Drosophila. Curr. Biol. 2002, 12, 2152–2158. [Google Scholar] [CrossRef] [Green Version]
- Lu, B.; Su, Y.; Das, S.; Liu, J.; Xia, J.; Ren, D. The neuronal channel NALCN contributes resting sodium permeability and is required for normal respiratory rhythm. Cell 2007, 129, 371–383. [Google Scholar] [CrossRef] [Green Version]
- Xie, L.; Gao, S.; Alcaire, S.M.; Aoyagi, K.; Wang, Y.; Griffin, J.K.; Stagljar, I.; Nagamatsu, S.; Zhen, M. NLF-1 delivers a sodium leak channel to regulate neuronal excitability and modulate rhythmic locomotion. Neuron 2013, 77, 1069–1082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maguire, L.H.; Handelman, S.K.; Du, X.; Chen, Y.; Pers, T.H.; Speliotes, E.K. Genome-wide association analyses identify 39 new susceptibility loci for diverticular disease. Nat. Genet. 2018, 50, 1359–1365. [Google Scholar] [CrossRef]
- Schafmayer, C.; Harrison, J.W.; Buch, S.; Lange, C.; Reichert, M.C.; Hofer, P.; Cossais, F.; Kupcinskas, J.; von Schonfels, W.; Schniewind, B.; et al. Genome-wide association analysis of diverticular disease points towards neuromuscular, connective tissue and epithelial pathomechanisms. Gut 2019, 68, 854–865. [Google Scholar] [CrossRef] [Green Version]
- Choe, E.K.; Lee, J.E.; Chung, S.J.; Yang, S.Y.; Kim, Y.S.; Shin, E.S.; Choi, S.H.; Bae, J.H. Genome-wide association study of right-sided colonic diverticulosis in a Korean population. Sci. Rep. 2019, 9, 7360. [Google Scholar] [CrossRef]
- De Santa Barbara, P.; van den Brink, G.R.; Roberts, D.J. Development and differentiation of the intestinal epithelium. Cell. Mol. Life Sci. 2003, 60, 1322–1332. [Google Scholar] [CrossRef]
- Gregorieff, A.; Pinto, D.; Begthel, H.; Destree, O.; Kielman, M.; Clevers, H. Expression pattern of Wnt signaling components in the adult intestine. Gastroenterology 2005, 129, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Di Liddo, R.; Bertalot, T.; Schuster, A.; Schrenk, S.; Tasso, A.; Zanusso, I.; Conconi, M.T.; Schafer, K.H. Anti-inflammatory activity of Wnt signaling in enteric nervous system: In vitro preliminary evidences in rat primary cultures. J. Neuroinflammation 2015, 12, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, G.; Mancl, M.E.; Barnes, B.J. Signaling through IFN regulatory factor-5 sensitizes p53-deficient tumors to DNA damage-induced apoptosis and cell death. Cancer Res. 2005, 65, 7403–7412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burkitt, D.P.; Walker, A.R.; Painter, N.S. Effect of dietary fibre on stools and the transit-times, and its role in the causation of disease. Lancet 1972, 7792, 1408–1411. [Google Scholar] [CrossRef]
- Aldoori, W.H.; Giovannucci, E.L.; Rockett, H.R.; Sampson, L.; Rimm, E.B.; Willett, W.C. A prospective study of dietary fiber types and symptomatic diverticular disease in men. J. Nutr. 1998, 128, 714–719. [Google Scholar] [CrossRef] [Green Version]
- Crowe, F.L.; Appleby, P.N.; Allen, N.E.; Key, T.J. Diet and risk of diverticular disease in Oxford cohort of European Prospective Investigation into Cancer and Nutrition (EPIC): Prospective study of British vegetarians and non-vegetarians. BMJ 2011, 343, d4131. [Google Scholar] [CrossRef] [Green Version]
- Peery, A.F.; Sandler, R.S.; Ahnen, D.J.; Galanko, J.A.; Holm, A.N.; Shaukat, A.; Mott, L.A.; Barry, E.L.; Fried, D.A.; Baron, J.A. Constipation and a low-fiber diet are not associated with diverticulosis. Clin. Gastroenterol. Hepatol. 2013, 11, 1622–1627. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Sen, A.; Norat, T.; Riboli, E. Dietary fibre intake and the risk of diverticular disease: A systematic review and meta-analysis of prospective studies. Eur. J. Nutr. 2020, 59, 421–432. [Google Scholar] [CrossRef] [Green Version]
- Cotillard, A.; Kennedy, S.P.; Kong, L.C.; Prifti, E.; Pons, N.; Le Chatelier, E.; Almeida, M.; Quinquis, B.; Levenez, F.; Galleron, N.; et al. Dietary intervention impact on gut microbial gene richness. Nature 2013, 500, 585–588. [Google Scholar] [CrossRef]
- Makki, K.; Deehan, E.C.; Walter, J.; Backhed, F. The Impact of Dietary Fiber on Gut Microbiota in Host Health and Disease. Cell Host Microbe 2018, 23, 705–715. [Google Scholar] [CrossRef] [Green Version]
- Koh, A.; De Vadder, F.; Kovatcheva-Datchary, P.; Backhed, F. From Dietary Fiber to Host Physiology: Short-Chain Fatty Acids as Key Bacterial Metabolites. Cell 2016, 165, 1332–1345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aldoori, W.H.; Giovannucci, E.L.; Rimm, E.B.; Wing, A.L.; Trichopoulos, D.V.; Willett, W.C. A prospective study of diet and the risk of symptomatic diverticular disease in men. Am. J. Clin. Nutr. 1994, 60, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Peery, A.F.; Barrett, P.R.; Park, D.; Rogers, A.J.; Galanko, J.A.; Martin, C.F.; Sandler, R.S. A high-fiber diet does not protect against asymptomatic diverticulosis. Gastroenterology 2012, 142, 266–272.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coode, P.E.; Chan, K.W.; Chan, Y.T. Polyps and diverticula of the large intestine: A necropsy survey in Hong Kong. Gut 1985, 26, 1045–1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rustom, L.B.O.; Sharara, A.I. The Natural History of Colonic Diverticulosis: Much Ado about Nothing? Inflamm. Intest. Dis. 2018, 3, 69–74. [Google Scholar] [CrossRef]
- Yamada, E.; Inamori, M.; Uchida, E.; Tanida, E.; Izumi, M.; Takeshita, K.; Fujii, T.; Komatsu, K.; Hamanaka, J.; Maeda, S.; et al. Association between the location of diverticular disease and the irritable bowel syndrome: A multicenter study in Japan. Am. J. Gastroenterol. 2014, 109, 1900–1905. [Google Scholar] [CrossRef] [Green Version]
- Tursi, A.; Scarpignato, C.; Strate, L.L.; Lanas, A.; Kruis, W.; Lahat, A.; Danese, S. Colonic diverticular disease. Nat. Rev. Dis. Primers 2020, 6, 20. [Google Scholar] [CrossRef]
- Nagata, N.; Niikura, R.; Shimbo, T.; Kishida, Y.; Sekine, K.; Tanaka, S.; Aoki, T.; Watanabe, K.; Akiyama, J.; Yanase, M.; et al. Alcohol and smoking affect risk of uncomplicated colonic diverticulosis in Japan. PLoS ONE 2013, 8, e81137. [Google Scholar] [CrossRef]
- Yamamichi, N.; Shimamoto, T.; Takahashi, Y.; Sakaguchi, Y.; Kakimoto, H.; Matsuda, R.; Kataoka, Y.; Saito, I.; Tsuji, Y.; Yakabi, S.; et al. Trend and risk factors of diverticulosis in Japan: Age, gender, and lifestyle/metabolic-related factors may cooperatively affect on the colorectal diverticula formation. PLoS ONE 2015, 10, e0123688. [Google Scholar] [CrossRef] [Green Version]
- Peery, A.F.; Keil, A.; Jicha, K.; Galanko, J.A.; Sandler, R.S. Association of Obesity With Colonic Diverticulosis in Women. Clin. Gastroenterol. Hepatol. 2020, 18, 107–114.e1. [Google Scholar] [CrossRef]
- Aldoori, W.H.; Giovannucci, E.L.; Rimm, E.B.; Wing, A.L.; Trichopoulos, D.V.; Willett, W.C. A prospective study of alcohol, smoking, caffeine, and the risk of symptomatic diverticular disease in men. Ann. Epidemiol. 1995, 5, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Jovani, M.; Liu, P.H.; Nguyen, L.H.; Cao, Y.; Tam, I.; Wu, K.; Giovannucci, E.L.; Strate, L.L.; Chan, A.T. Association Between Obesity and Weight Change and Risk of Diverticulitis in Women. Gastroenterology 2018, 155, 58–66.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turnbaugh, P.J.; Gordon, J.I. The core gut microbiome, energy balance and obesity. J. Physiol. 2009, 587, 4153–4158. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Medina, M.; Denizot, J.; Dreux, N.; Robin, F.; Billard, E.; Bonnet, R.; Darfeuille-Michaud, A.; Barnich, N. Western diet induces dysbiosis with increased E coli in CEABAC10 mice, alters host barrier function favouring AIEC colonisation. Gut 2014, 63, 116–124. [Google Scholar] [CrossRef]
- Turnbaugh, P.J.; Backhed, F.; Fulton, L.; Gordon, J.I. Diet-induced obesity is linked to marked but reversible alterations in the mouse distal gut microbiome. Cell Host Microbe 2008, 3, 213–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claesson, M.J.; Jeffery, I.B.; Conde, S.; Power, S.E.; O’Connor, E.M.; Cusack, S.; Harris, H.M.; Coakley, M.; Lakshminarayanan, B.; O’Sullivan, O.; et al. Gut microbiota composition correlates with diet and health in the elderly. Nature 2012, 488, 178–184. [Google Scholar] [CrossRef]
- Barbara, G.; Scaioli, E.; Barbaro, M.R.; Biagi, E.; Laghi, L.; Cremon, C.; Marasco, G.; Colecchia, A.; Picone, G.; Salfi, N.; et al. Gut microbiota, metabolome and immune signatures in patients with uncomplicated diverticular disease. Gut 2017, 66, 1252–1261. [Google Scholar] [CrossRef]
- Tursi, A.; Mastromarino, P.; Capobianco, D.; Elisei, W.; Miccheli, A.; Capuani, G.; Tomassini, A.; Campagna, G.; Picchio, M.; Giorgetti, G.; et al. Assessment of Fecal Microbiota and Fecal Metabolome in Symptomatic Uncomplicated Diverticular Disease of the Colon. J. Clin. Gastroenterol. 2016, 50 (Suppl. S1), S9–S12. [Google Scholar] [CrossRef] [Green Version]
- Dao, M.C.; Everard, A.; Aron-Wisnewsky, J.; Sokolovska, N.; Prifti, E.; Verger, E.O.; Kayser, B.D.; Levenez, F.; Chilloux, J.; Hoyles, L.; et al. Akkermansia muciniphila and improved metabolic health during a dietary intervention in obesity: Relationship with gut microbiome richness and ecology. Gut 2016, 65, 426–436. [Google Scholar] [CrossRef] [Green Version]
- Earley, H.; Lennon, G.; Balfe, A.; Coffey, J.C.; Winter, D.C.; O’Connell, P.R. The abundance of Akkermansia muciniphila and its relationship with sulphated colonic mucins in health and ulcerative colitis. Sci. Rep. 2019, 9, 15683. [Google Scholar] [CrossRef] [Green Version]
- Lopetuso, L.R.; Petito, V.; Graziani, C.; Schiavoni, E.; Paroni Sterbini, F.; Poscia, A.; Gaetani, E.; Franceschi, F.; Cammarota, G.; Sanguinetti, M.; et al. Gut Microbiota in Health, Diverticular Disease, Irritable Bowel Syndrome, and Inflammatory Bowel Diseases: Time for Microbial Marker of Gastrointestinal Disorders. Dig. Dis. 2018, 36, 56–65. [Google Scholar] [CrossRef]
- Jones, R.B.; Fodor, A.A.; Peery, A.F.; Tsilimigras, M.C.B.; Winglee, K.; McCoy, A.; Sioda, M.; Sandler, R.S.; Keku, T.O. An Aberrant Microbiota is not Strongly Associated with Incidental Colonic Diverticulosis. Sci. Rep. 2018, 8, 4951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Rossen, T.M.; Ooijevaar, R.E.; Kuyvenhoven, J.P.; Eck, A.; Bril, H.; Buijsman, R.; Boermeester, M.A.; Stockmann, H.; de Korte, N.; Budding, A.E. Microbiota composition and mucosal immunity in patients with asymptomatic diverticulosis and controls. PLoS ONE 2021, 16, e0256657. [Google Scholar] [CrossRef] [PubMed]
- Kvasnovsky, C.L.; Leong, L.E.X.; Choo, J.M.; Abell, G.C.J.; Papagrigoriadis, S.; Bruce, K.D.; Rogers, G.B. Clinical and symptom scores are significantly correlated with fecal microbiota features in patients with symptomatic uncomplicated diverticular disease: A pilot study. Eur. J. Gastroenterol. Hepatol. 2018, 30, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Tursi, A.; Mastromarino, P.; Capobianco, D.; Elisei, W.; Picchio, M.; Brandimarte, G. No changes in Interleukin-10 expression in symptomatic uncomplicated diverticular disease of the colon. J. Gastrointest. Liver Dis. 2018, 27, 476–477. [Google Scholar] [CrossRef]
- Tursi, A.; Brandimarte, G.; Elisei, W.; Giorgetti, G.M.; Inchingolo, C.D.; Danese, S.; Aiello, F. Assessment and grading of mucosal inflammation in colonic diverticular disease. J. Clin. Gastroenterol. 2008, 42, 699–703. [Google Scholar] [CrossRef]
- Peery, A.F.; Keku, T.O.; Addamo, C.; McCoy, A.N.; Martin, C.F.; Galanko, J.A.; Sandler, R.S. Colonic Diverticula Are Not Associated With Mucosal Inflammation or Chronic Gastrointestinal Symptoms. Clin. Gastroenterol. Hepatol. 2018, 16, 884–891.e1. [Google Scholar] [CrossRef] [Green Version]
- Jarbrink-Sehgal, M.E.; Rassam, L.; Jasim, A.; Walker, M.M.; Talley, N.J.; Agreus, L.; Andreasson, A.; Schmidt, P.T. Diverticulosis, Symptoms and Colonic Inflammation: A Population-Based Colonoscopy Study. Am. J. Gastroenterol. 2019, 114, 500–510. [Google Scholar] [CrossRef]
- Horgan, A.F.; McConnell, E.J.; Wolff, B.G.; The, S.; Paterson, C. Atypical diverticular disease: Surgical results. Dis. Colon Rectum 2001, 44, 1315–1318. [Google Scholar] [CrossRef]
- Tursi, A.; Brandimarte, G.; Elisei, W.; Giorgetti, G.M.; Inchingolo, C.D.; Aiello, F. Faecal calprotectin in colonic diverticular disease: A case-control study. Int. J. Colorectal Dis. 2009, 24, 49–55. [Google Scholar] [CrossRef]
- Humes, D.J.; Simpson, J.; Smith, J.; Sutton, P.; Zaitoun, A.; Bush, D.; Bennett, A.; Scholefield, J.H.; Spiller, R.C. Visceral hypersensitivity in symptomatic diverticular disease and the role of neuropeptides and low grade inflammation. Neurogastroenterol. Motil. 2012, 24, 318-e163. [Google Scholar] [CrossRef] [PubMed]
- Turco, F.; Andreozzi, P.; Palumbo, I.; Zito, F.P.; Cargiolli, M.; Fiore, W.; Gennarelli, N.; De Palma, G.D.; Sarnelli, G.; Cuomo, R. Bacterial stimuli activate nitric oxide colonic mucosal production in diverticular disease. Protective effects of L. casei DG(R) (Lactobacillus paracasei CNCM I-1572). United Eur. Gastroenterol. J. 2017, 5, 715–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tursi, A.; Elisei, W.; Brandimarte, G.; Giorgetti, G.M.; Inchingolo, C.D.; Nenna, R.; Ierardi, E. Tumour necrosis factor-alpha expression in segmental colitis associated with diverticulosis down-regulates after treatment. J. Gastrointestin Liver Dis. 2011, 20, 365–370. [Google Scholar] [PubMed]
- Macbeth, W.A.; Hawthorne, J.H. Intramural Ganglia in Diverticular Disease of the Colon. J. Clin. Pathol. 1965, 18, 40–42. [Google Scholar] [CrossRef] [Green Version]
- Wedel, T.; Busing, V.; Heinrichs, G.; Nohroudi, K.; Bruch, H.P.; Roblick, U.J.; Bottner, M. Diverticular disease is associated with an enteric neuropathy as revealed by morphometric analysis. Neurogastroenterol. Motil. 2010, 22, 407-e94. [Google Scholar] [CrossRef]
- Deduchovas, O.; Saladzinskas, Z.; Tamelis, A.; Pavalkis, D.; Pauziene, N.; Pauza, D.H. Morphologic pattern of myenteric neural plexus in colonic diverticular disease. A whole-mount study employing histochemical staining for acetylcholinesterase. Ann. Anat. 2008, 190, 525–530. [Google Scholar] [CrossRef]
- Iwase, H.; Sadahiro, S.; Mukoyama, S.; Makuuchi, H.; Yasuda, M. Morphology of myenteric plexuses in the human large intestine: Comparison between large intestines with and without colonic diverticula. J. Clin. Gastroenterol. 2005, 39, 674–678. [Google Scholar] [CrossRef]
- Gallego, D.; Espin, F.; Mikulka, J.; Smirg, O.; Gil, V.; Faundez-Zanuy, M.; Jimenez, M.; Clave, P. In vitro motor patterns and electrophysiological changes in patients with colonic diverticular disease. Int. J. Colorectal Dis. 2013, 28, 1413–1422. [Google Scholar] [CrossRef]
- Bassotti, G.; Battaglia, E.; Bellone, G.; Dughera, L.; Fisogni, S.; Zambelli, C.; Morelli, A.; Mioli, P.; Emanuelli, G.; Villanacci, V. Interstitial cells of Cajal, enteric nerves, and glial cells in colonic diverticular disease. J. Clin. Pathol. 2005, 58, 973–977. [Google Scholar] [CrossRef] [Green Version]
- Bottner, M.; Barrenschee, M.; Hellwig, I.; Harde, J.; Egberts, J.H.; Becker, T.; Zorenkov, D.; Schafer, K.H.; Wedel, T. The GDNF System Is Altered in Diverticular Disease—Implications for Pathogenesis. PLoS ONE 2013, 8, e66290. [Google Scholar] [CrossRef] [Green Version]
- Barrenschee, M.; Wedel, T.; Lange, C.; Hohmeier, I.; Cossais, F.; Ebsen, M.; Vogel, I.; Bottner, M. No neuronal loss, but alterations of the GDNF system in asymptomatic diverticulosis. PLoS ONE 2017, 12, e0171416. [Google Scholar] [CrossRef]
- Bottner, M.; Harde, J.; Barrenschee, M.; Hellwig, I.; Vogel, I.; Ebsen, M.; Wedel, T. GDNF induces synaptic vesicle markers in enteric neurons. Neurosci. Res. 2013, 77, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, M.R.; Cremon, C.; Fuschi, D.; Scaioli, E.; Veneziano, A.; Marasco, G.; Festi, D.; Stanghellini, V.; Barbara, G. Nerve fiber overgrowth in patients with symptomatic diverticular disease. Neurogastroenterol. Motil. 2019, 31, e13575. [Google Scholar] [CrossRef]
- Simpson, J.; Sundler, F.; Humes, D.J.; Jenkins, D.; Scholefield, J.H.; Spiller, R.C. Post inflammatory damage to the enteric nervous system in diverticular disease and its relationship to symptoms. Neurogastroenterol. Motil. 2009, 21, 847-e58. [Google Scholar] [CrossRef] [PubMed]
- Bassotti, G.; Villanacci, V.; Bernardini, N.; Dore, M.P. Diverticular Disease of the Colon: Neuromuscular Function Abnormalities. J. Clin. Gastroenterol. 2016, 50 (Suppl. S1), S6–S8. [Google Scholar] [CrossRef] [Green Version]
- Golder, M.; Burleigh, D.E.; Ghali, L.; Feakins, R.M.; Lunniss, P.J.; Williams, N.S.; Navsaria, H.A. Longitudinal muscle shows abnormal relaxation responses to nitric oxide and contains altered levels of NOS1 and elastin in uncomplicated diverticular disease. Colorectal Dis. 2007, 9, 218–228. [Google Scholar] [CrossRef]
- Golder, M.; Burleigh, D.E.; Belai, A.; Ghali, L.; Ashby, D.; Lunniss, P.J.; Navsaria, H.A.; Williams, N.S. Smooth muscle cholinergic denervation hypersensitivity in diverticular disease. Lancet 2003, 361, 1945–1951. [Google Scholar] [CrossRef]
- Tomita, R.; Fujisaki, S.; Tanjoh, K.; Fukuzawa, M. Role of nitric oxide in the left-sided colon of patients with diverticular disease. Hepatogastroenterology 2000, 47, 692–696. [Google Scholar]
- Tomita, R.; Munakata, K.; Aoki, N.; Tanjoh, K.; Kurosu, Y. A study on the peptidergic nerves (VIP, substance P) in the colon of patients with diverticular disease. Regul. Pept. 1993, 46, 244–246. [Google Scholar] [CrossRef]
- Dothel, G.; Barbaro, M.R.; Boudin, H.; Vasina, V.; Cremon, C.; Gargano, L.; Bellacosa, L.; De Giorgio, R.; Le Berre-Scoul, C.; Aubert, P.; et al. Nerve fiber outgrowth is increased in the intestinal mucosa of patients with irritable bowel syndrome. Gastroenterology 2015, 148, 1002–1011.e4. [Google Scholar] [CrossRef]
- Demir, I.E.; Schafer, K.H.; Tieftrunk, E.; Friess, H.; Ceyhan, G.O. Neural plasticity in the gastrointestinal tract: Chronic inflammation, neurotrophic signals, and hypersensitivity. Acta Neuropathol. 2013, 125, 491–509. [Google Scholar] [CrossRef]
- Wu, F.; Miao, X.; Chen, J.; Liu, Z.; Tao, Y.; Yu, W.; Sun, Y. Inhibition of GAP-43 by propentofylline in a rat model of neuropathic pain. Int. J. Clin. Exp. Pathol. 2013, 6, 1516–1522. [Google Scholar]
- Wedel, T.; Barrenschee, M.; Lange, C.; Cossais, F.; Bottner, M. Morphologic Basis for Developing Diverticular Disease, Diverticulitis, and Diverticular Bleeding. Viszeralmedizin 2015, 31, 76–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattii, L.; Ippolito, C.; Segnani, C.; Battolla, B.; Colucci, R.; Dolfi, A.; Bassotti, G.; Blandizzi, C.; Bernardini, N. Altered expression pattern of molecular factors involved in colonic smooth muscle functions: An immunohistochemical study in patients with diverticular disease. PLoS ONE 2013, 8, e57023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellwig, I.; Bottner, M.; Barrenschee, M.; Harde, J.; Egberts, J.H.; Becker, T.; Wedel, T. Alterations of the enteric smooth musculature in diverticular disease. J. Gastroenterol. 2014, 49, 1241–1252. [Google Scholar] [CrossRef]
- Hughes, L.E. Postmortem survey of diverticular disease of the colon. II. The muscular abnormality of the sigmoid colon. Gut 1969, 10, 344–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomita, R. Are there any functional differences of the enteric nervous system between the right-sided diverticular colon and the left-sided diverticular colon? An in vitro study. Int. J. Colorectal Dis. 2014, 29, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Espin, F.; Rofes, L.; Ortega, O.; Clave, P.; Gallego, D. Nitrergic neuro-muscular transmission is up-regulated in patients with diverticulosis. Neurogastroenterol. Motil. 2014, 26, 1458–1468. [Google Scholar] [CrossRef]
- Bottner, M.; Barrenschee, M.; Hellwig, I.; Harde, J.; Egberts, J.H.; Becker, T.; Zorenkov, D.; Wedel, T. The enteric serotonergic system is altered in patients with diverticular disease. Gut 2013, 62, 1753–1762. [Google Scholar] [CrossRef]
- Maselli, M.A.; Piepoli, A.L.; Guerra, V.; Caruso, M.L.; Pezzolla, F.; Lorusso, D.; Demma, I.; De Ponti, F. Colonic smooth muscle responses in patients with diverticular disease of the colon: Effect of the NK2 receptor antagonist SR48968. Dig. Liver Dis. 2004, 36, 348–354. [Google Scholar] [CrossRef]
- Alvarez-Berdugo, D.; Espin, F.; Arenas, C.; Lopez, I.; Clave, P.; Gallego, D. Changes in the response to excitatory antagonists, agonists, and spasmolytic agents in circular colonic smooth muscle strips from patients with diverticulosis. Neurogastroenterol. Motil. 2015, 27, 1600–1612. [Google Scholar] [CrossRef] [PubMed]
- Ruhl, A. Glial cells in the gut. Neurogastroenterol. Motil. 2005, 17, 777–790. [Google Scholar] [CrossRef] [PubMed]
- Stollman, N.; Raskin, J.B. Diverticular disease of the colon. Lancet 2004, 363, 631–639. [Google Scholar] [CrossRef] [Green Version]
- Clemens, C.H.; Samsom, M.; Roelofs, J.; van Berge Henegouwen, G.P.; Smout, A.J. Colorectal visceral perception in diverticular disease. Gut 2004, 53, 717–722. [Google Scholar] [CrossRef] [Green Version]


| Authors | Subjects (n) | Genome Profiling Method | Outcomes |
|---|---|---|---|
| Reichert et al., 2018 [23] | Diverticulosis (422) HC (285) | TaqMan assays | Positive association between the COL3A1 variant and the risk of developing diverticulosis. |
| Connelly et al., 2014 [24] | Diverticulosis (21) HC (21) | TaqMan assay | Positive association of the single nucleotide polymorphism rs7848647 in the TNFSF15 gene with diverticulitis requiring surgical intervention. |
| Sigurdsson et al., 2017 [25] | DD (11′396) HC (248′971) | GWAS | Variants in introns of the ARHGAP15, COLQ and FAM155A associate with diverticular disease or diverticulitis. |
| Coble et al., 2017 [26] | Diverticulitis (153) | Exome sequencing | LAMB4 variants were identified in patients with diverticulitis. |
| Nehring et al., 2021 [27] | Diverticulosis (100) HC (120) | PCR–restriction fragments | The SNP rs4898 in TMP1 gene correlates with an increased risk of diverticulosis. |
| Reichert et al., 2020 [29] | Diverticulosis (856) HC (479) Diverticulitis (198) | Taqman assays | Association of ARHGAP15 and COLQ variants with uncomplicated DD and FAM155 mutation with diverticulitis, but not with diverticulosis. |
| Maguire et al., 2018 [37] | DD (27,444) HC (382,284) | GWAS | DD is associated with 42 loci localized in genes implicated in immunity (ARHGAP15, FADD, HLX), cell adhesion (BMPR1B, CLSTN2, COL6A1, CRISPLD2, EFEMP1, ELN, ENPP2, HAS2, IGSF10, LIMK1, LRRC17, NOV, PCSK5, S100A11, SHFM1, TCHH), membrane transport and signaling (ANO1, CACNB2, CALCA, CALCB, CHRNB1, COLQ, CUTC, S100A10, SLC25A28, SLC35F3, SPINT2), and intestinal motility (ANO1, CHRNB1, COLQ, PPP1R14A). |
| Schafmayer et al., 2019 [38] | DD (31,964) HC (419,135) | GWAS | Discovered 48 risk loci close genes (ARHGAP15, FAM155A, COLQ, GPR158, ABO, ANO1/FADS, ELN, BMPR1B, SLC35F3, SEM1/SHFM1, CTAGE1, NOV, CALCB, S100A10, DISP2, CACNB2, HLX, EDEM1, EFEMP1, LYPLAL1-AS1, SLC25A28, CWC27, SLC4A1, AC103796.1, CRISPLD2, WDR70, HAS2, PCSK5, NT5C1B, TRPS1) impaired in intestinal neuromuscular function, mesenteric vascular, smooth muscle, and connective fiber support associate with DD. |
| Choe et al., 2019 [39] | Diverticulosis (893) HC (1075) | GWAS | Identified 9 SNPs located in WNT4, RHOU, and OAS1/3 genes. |
| Author | Subjects (n) | Diet | Outcomes |
|---|---|---|---|
| Burkitt DP et al., 1972 [44] | General population (1200) | Low-fibers Western diet vs. high-fiber diet | Low-fiber Western diet produces smaller stool volumes and longer transit time, with the consequent increase of intraluminal pressure predisposing to diverticular herniation. |
| Aldoori et al., 1998 [45] Aldoori et al., 1994 [52] | General population (male) (43,881) | High soluble fiber assumption | Decrease risk to develop DD. |
| Crowe et al., 2011 [46] | General population (47,033) | Vegetarian diet and dietary fiber assumption | Vegetarians had a risk reduction of 30% to develop DD compared to subjects consuming meat. Individuals consuming more than 25 g of fibers/day had a decrease of 40% in the hospitalization risk compared to subjects consuming less than 14 g/day. |
| Peery et al., 2012 [53] | General population (2104) | High-fiber diet | High fiber diet associates with a higher prevalence of diverticulosis. |
| Peery et al., 2013 [47] | Diverticulosis and controls (2108) | Low-fiber diet | No association between constipation and the risk of diverticulosis. |
| Aune et al., 2020 [48] | General population (876,111; 19,282 cases and 856,829 participants) | Free diet | Subjects consuming a high fiber diet (30 g per day) had a reduction of 41% of the risk to develop DD, compared to subjects with a low fiber diet. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbaro, M.R.; Cremon, C.; Fuschi, D.; Marasco, G.; Palombo, M.; Stanghellini, V.; Barbara, G. Pathophysiology of Diverticular Disease: From Diverticula Formation to Symptom Generation. Int. J. Mol. Sci. 2022, 23, 6698. https://doi.org/10.3390/ijms23126698
Barbaro MR, Cremon C, Fuschi D, Marasco G, Palombo M, Stanghellini V, Barbara G. Pathophysiology of Diverticular Disease: From Diverticula Formation to Symptom Generation. International Journal of Molecular Sciences. 2022; 23(12):6698. https://doi.org/10.3390/ijms23126698
Chicago/Turabian StyleBarbaro, Maria Raffaella, Cesare Cremon, Daniele Fuschi, Giovanni Marasco, Marta Palombo, Vincenzo Stanghellini, and Giovanni Barbara. 2022. "Pathophysiology of Diverticular Disease: From Diverticula Formation to Symptom Generation" International Journal of Molecular Sciences 23, no. 12: 6698. https://doi.org/10.3390/ijms23126698