
Fertility-Sparing Approach in Women Affected by Stage I and Low-Grade Endometrial Carcinoma: An Updated Overview

 ,
, 
 , , ,
, , ,
Abstract
:1. Introduction
2. Discussion
2.1. Target Patients for Fertility-Sparing Treatment
2.2. Hormonal Approach for Fertility Sparing
2.3. Metformin in Fertility Sparing
2.4. Surgical Treatment by Hysteroscopy
2.5. Follow-Up
2.6. Consideration about Psychological Impact
2.7. New Molecules on Endometrial Cancer Supplementation
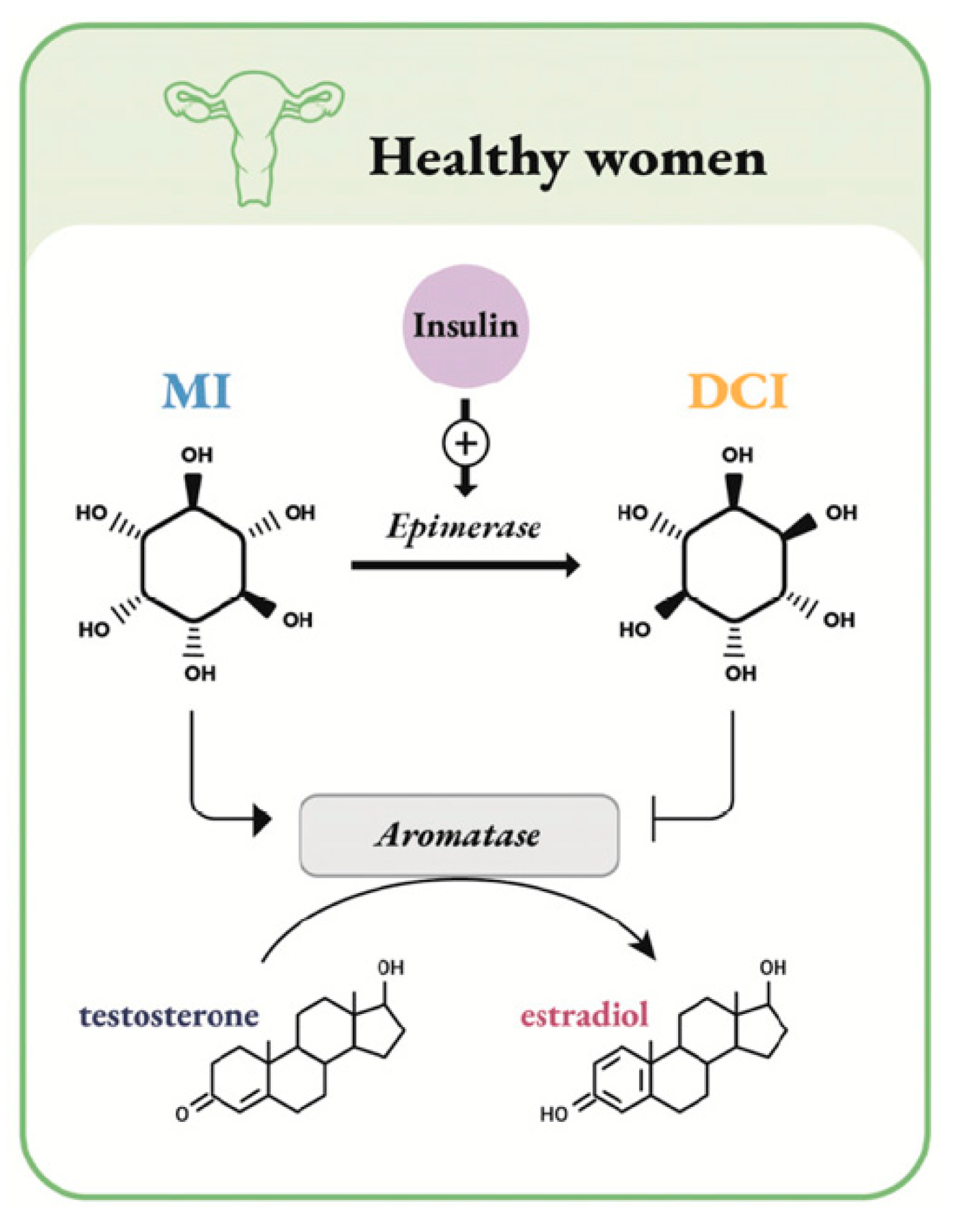
- an indirect steroidogenic effect mediated by the insulin pathway;
- an independent steroidogenic direct effect through downregulation of the aromatase gene expression and cytochrome P450 side-chain cleavage (P450scc) genes. These actions lead to an increase of testosterone synthesis.
2.8. The Molecular Role in EC
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Koh, W.J.; Abu-Rustum, N.R.; Bean, S.; Bradley, K.; Campos, S.M.; Cho, K.R.; Chon, H.S.; Chu, C.; Cohn, D.; Crispens, M.A.; et al. Uterine neoplasms, version 1.2018, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2018, 16, 170–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, J.; Zhang, W.; Feng, L.; Gao, W. Comparison of fertility-sparing treatments in patients with early endometrial cancer and atypical complex hyperplasia: A meta-analysis and systematic review. Medicine 2017, 96, e8034. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.C.; Won, Y.J.; Ko, M.J.; Kim, M.; Shim, S.H.; Suh, D.H.; Kim, J.W. Incidence of cervical, endometrial, and ovarian cancer in Korea during 1999–2015. J. Gynecol. Oncol. 2019, 30, e38. [Google Scholar] [CrossRef]
- Tabor, A.; Watt, H.C.; Wald, N.J. Endometrial thickness as a test for endometrial cancer in women with postmenopausal vaginal bleeding. Obstet. Gynecol. 2002, 99, 663–670. [Google Scholar] [PubMed]
- Webb, P.M. Environmental (nongenetic) factors in gynecological cancers: Update and future perspectives. Future Oncol. 2015, 11, 295–307. [Google Scholar] [CrossRef] [PubMed]
- Felix, A.S.; Weissfeld, J.L.; Stone, R.A.; Bowser, R.; Chivukula, M.; Edwards, R.P.; Linkov, F. Factors associated with Type I and Type II endometrial cancer. Cancer Causes Control 2010, 21, 1851–1856. [Google Scholar] [CrossRef] [Green Version]
- Setiawan, V.W.; Yang, H.P.; Pike, M.C.; McCann, S.E.; Yu, H.; Xiang, Y.B.; Wolk, A.; Wentzensen, N.; Weiss, N.S.; Webb, P.M.; et al. Type I and II endometrial cancers: Have they different risk factors? J. Clin. Oncol. 2013, 31, 2607. [Google Scholar] [CrossRef]
- Win, A.K.; Reece, J.C.; Ryan, S. Family history and risk of endometrial cancer: A systematic review and meta-analysis. Obstet. Gynecol. 2015, 125, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Loiacono, R.M.; Trojano, G.; Del Gaudio, N.; Kardhashi, A.; Deliso, M.A.; Falco, G.; Sforza, R.; Laera, A.F.; Galise, I.; Trojano, V. Hysteroscopy as a Valid Tool for Endometrial Pathology in Patients with Postmenopausal Bleeding or Asymptomatic Patients with a Thickened Endometrium: Hysteroscopic and Histological Results. Gynecol. Obstet. Investig. 2015, 79, 210–216. [Google Scholar] [CrossRef]
- Visser, N.C.M.; Reijnen, C.; Massuger, L.F.A.G.; Nagtegaal, I.D.; Bulten, J.; Pijnenborg, J.M.A. Accuracy of Endometrial Sampling in Endometrial Carcinoma: A Systematic Review and Meta-analysis. Obstet. Gynecol. 2017, 130, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Bourdel, N.; Chauvet, P.; Tognazza, E.; Pereira, B.; Botchorishvili, R.; Canis, M. Sampling in Atypical Endometrial Hyperplasia: Which Method Results in the Lowest Underestimation of Endometrial Cancer? A Systematic Review and Meta-analysis. J Minim. Invasive Gynecol. 2016, 23, 692–701. [Google Scholar] [CrossRef]
- Capozzi, V.A.; Rosati, A.; Rumolo, V.; Ferrari, F.; Gullo, G.; Karaman, E.; Karaaslan, O.; HacioĞlu, L. Novelties of ultrasound imaging for endometrial cancer preoperative workup. Minerva Med. 2021, 112, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.I.; Lee, J.W.; Lee, N.; Lee, M.; Kim, H.S.; Chung, H.H.; Kim, J.W.; Park, N.H.; Song, Y.S.; Seo, J.S. LYL1 gene amplification predicts poor survival of patients with uterine corpus endometrial carcinoma: Analysis of the cancer genome atlas data. BMC Cancer 2018, 18, 494. [Google Scholar] [CrossRef] [Green Version]
- Bonadona, V.; Bonaïti, B.; Olschwang, S.; Grandjouan, S.; Huiart, L.; Longy, M.; Guimbaud, R.; Buecher, B.; Bignon, Y.J.; Caron, O.; et al. Cancer risks associated with germline mutations in MLH1, MSH2, and MSH6 genes in Lynch syndrome. JAMA 2011, 305, 2304–2310. [Google Scholar] [CrossRef]
- Laganà, A.S.; La Rosa, V.L.; Rapisarda, A.M.; Vitale, S.G. Comment on: “Needs and priorities of women with endometrial and cervical cancer”. J. Psychosom. Obstet. Gynaecol. 2017, 38, 85–86. [Google Scholar] [CrossRef] [PubMed]
- Obermair, A.; Baxter, E.; Brennan, D.J.; McAlpine, J.N.; Muellerer, J.J.; Amant, F.; van Gent, M.D.J.M.; Coleman, R.L.; Westin, S.N.; Yates, M.S.; et al. Fertility-sparing treatment in early endometrial cancer: Current state and future strategies. Obstet. Gynecol. Sci. 2020, 63, 417–431. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Kim, D.Y.; Kim, T.J.; Kim, J.W.; Kim, J.H.; Kim, Y.M.; Kim, Y.T.; Bae, D.S.; Nam, J.H. Hormonal therapy for women with stage IA endometrial cancer of all grades. Obstet. Gynecol. 2013, 122, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Chae, S.H.; Shim, S.H.; Lee, S.J.; Lee, J.Y.; Kim, S.N.; Kang, S.B. Pregnancy and oncologic outcomes after fertility-sparing management for early stage endometrioid endometrial cancer. Int. J. Gynecol. Cancer 2019, 29, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhu, Q.; Yang, B.; Ning, C.; Liu, X.; Luo, X.; Chen, X. Risk factors for ovarian involvement in young and premenopausal endometrioid endometrial cancer patients. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 222, 151–154. [Google Scholar] [CrossRef] [PubMed]
- SGO Clinical Practice Endometrial Cancer Working Group; Burke, W.M.; Orr, J.; Leitao, M.; Salom, E.; Gehrig, P.; Olawaiye, A.B.; Brewer, M.; Boruta, D.; Herzog, T.J.; et al. Society of Gynecologic Oncology Clinical Practice Committee. Endometrial cancer: A review and current management strategies: Part II. Gynecol. Oncol. 2014, 134, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Sundar, S.; Balega, J.; Crosbie, E.; Drake, A.; Edmondson, R.; Fotopoulou, C.; Gallos, I.; Ganesan, R.; Gupta, J.; Johnson, N.; et al. BGCS uterine cancer guidelines: Recommendations for practice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 213, 71–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinkel, K.; Kaji, Y.; Yu, K.K.; Segal, M.R.; Lu, Y.; Powell, C.B.; Hricak, H. Radiologic staging in patients with endometrial cancer: A meta-analysis. Radiology 1999, 212, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Morice, P.; Leary, A.; Creutzberg, C.; Abu-Rustum, N.; Darai, E. Endometrial cancer. Lancet 2016, 387, 1094–1108. [Google Scholar] [CrossRef]
- Wright, J.D.; Buck, A.M.; Shah, M.; Burke, W.M.; Schiff, P.B.; Herzog, T.J. Safety of ovarian preservation in premenopausal women with endometrial cancer. J. Clin. Oncol. 2009, 27, 1214–1219. [Google Scholar] [CrossRef] [PubMed]
- Gotlieb, W.H.; Beiner, M.E.; Shalmon, B.; Korach, Y.; Segal, Y.; Zmira, N.; Koupolovic, J.; Ben-Baruch, G. Outcome of fertility-sparing treatment with progestins in young patients with endometrial cancer. Obstet. Gynecol. 2003, 102, 718–725. [Google Scholar]
- Lowe, M.P.; Bender, D.; Sood, A.K.; Davis, W.; Syrop, C.H.; Sorosky, J.I. Two successful pregnancies after conservative treatment of endometrial cancer and assisted reproduction. Fertil. Steril. 2002, 77, 188–189. [Google Scholar] [CrossRef]
- Yamazawa, K.; Hirai, M.; Fujito, A.; Nishi, H.; Terauchi, F.; Ishikura, H.; Shozu, M.; Isaka, K. Fertility-preserving treatment with progestin, and pathological criteria to predict responses, in young women with endometrial cancer. Hum. Reprod. 2007, 22, 1953–1958. [Google Scholar] [CrossRef]
- Park, J.Y.; Kim, D.Y.; Kim, J.H.; Kim, Y.M.; Kim, K.R.; Kim, Y.T.; Seong, S.J.; Kim, T.J.; Kim, J.W.; Kim, S.M.; et al. Long-term oncologic outcomes after fertility-sparing management using oral progestin for young women with endometrial cancer (KGOG 2002). Eur. J. Cancer 2013, 49, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Koskas, M.; Uzan, J.; Luton, D.; Rouzier, R.; Daraï, E. Prognostic factors of oncologic and reproductive outcomes in fertility-sparing management of endometrial atypical hyperplasia and adenocarcinoma: Systematic review and meta-analysis. Fertil. Steril. 2014, 101, 785–794. [Google Scholar] [CrossRef]
- Laganà, A.S.; Palmara, V.; Granese, R.; Ciancimino, L.; Chiofalo, B.; Triolo, O. Desogestrel versus danazol as preoperative treatment for hysteroscopic surgery: A prospective, randomized evaluation. Gynecol. Endocrinol. 2014, 30, 794–797. [Google Scholar] [CrossRef] [PubMed]
- Laganà, A.S.; Giacobbe, V.; Triolo, O.; Granese, R.; Ban Frangež, H.; Vrtačnik-Bokal, E.; Ietto, C.; Palmara, V.I. Dienogest as preoperative treatment of submucous myomas for hysteroscopic surgery: A prospective, randomized study. Gynecol. Endocrinol. 2016, 32, 408–411. [Google Scholar] [CrossRef] [PubMed]
- Laganà, A.S.; Vitale, S.G.; Granese, R.; Palmara, V.; Ban Frangež, H.; Vrtačnik-Bokal, E.; Chiofalo, B.; Triolo, O. S.; Vitale, S.G.; Granese, R.; Palmara, V.; Ban, Frangež, H.; Vrtačnik-Bokal, E.; Chiofalo, B.; Triolo, O. Clinical dynamics of Dienogest for the treatment of endometriosis: From bench to bedside. Expert Opin. Drug Metab. Toxicol. 2017, 13, 593–596. [Google Scholar] [CrossRef] [Green Version]
- Lagana, A.S.; Vitale, S.G.; Muscia, V.; Rossetti, P.; Buscema, M.; Triolo, O.; Rapisarda, A.M.C.; Giunta, L.; Palmara, V.; Granese, R.; et al. Endometrial preparation with Dienogest before hysteroscopic surgery: A systematic review. Arch. Gynecol. Obstet. 2017, 295, 661–667. [Google Scholar] [CrossRef]
- Perino, A.; Quartararo, P.; Catinella, E.; Genova, G.; Cittadini, E. Treatment of endometrial hyperplasia with levonorgestrel releasing intrauterine devices. Acta Eur. Fertil. 1987, 18, 137–140. [Google Scholar] [PubMed]
- Yuk, J.S.; Song, J.Y.; Lee, J.H.; Park, W.I.; Ahn, H.S.; Kim, H.J. Levonorgestrel-releasing intrauterine systems versus oral cyclic medroxyprogesterone acetate in endometrial hyperplasia therapy: A meta-analysis. Ann. Surg. Oncol. 2017, 24, 1322–1329. [Google Scholar] [CrossRef]
- Pal, N.; Broaddus, R.R.; Urbauer, D.L.; Balakrishnan, N.; Milbourne, A.; Schmeler, K.M.; Meyer, L.A.; Soliman, P.T.; Lu, K.H.; Ramirez, P.T.; et al. Treatment of low-risk endometrial cancer and complex atypical hyperplasia with the levonorgestrel-releasing intrauterine device. Obstet. Gynecol. 2018, 131, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Seong, S.J.; Lee, T.S.; Kim, J.W.; Nam, B.H.; Hong, S.R.; Suh, K.S. Treatment with medroxyprogesterone acetate plus levonorgestrel-releasing intrauterine system for early-stage endometrial cancer in young women: Single-arm, prospective multicenter study: Korean gynecologic oncology group study (KGOG2009). Jpn. J. Clin. Oncol. 2012, 42, 1215–1218. [Google Scholar] [CrossRef] [Green Version]
- Pronin, S.M.; Novikova, O.V.; Andreeva, J.Y.; Novikova, E.G. Fertility-sparing treatment of early endometrial cancer and complex atypical hyperplasia in young women of childbearing potential. Int. J. Gynecol. Cancer 2015, 25, 1010–1014. [Google Scholar] [CrossRef]
- Dhar, K.K.; NeedhiRajan, T.; Koslowski, M.; Woolas, R.P. Is levonorgestrel intrauterine system effective for treatment of early endometrial cancer? Report of four cases and review of the literature. Gynecol. Oncol. 2005, 97, 924–927. [Google Scholar] [CrossRef] [PubMed]
- Kliemann, N.; Murphy, N.; Viallon, V.; Freisling, H.; Tsilidis, K.K.; Rinaldi, S.; Mancini, F.R.; Fagherazzi, G.; Boutron-Ruault, M.C.; Boeing, H.; et al. Predicted basal metabolic rate and cancer risk in the European prospective investigation into cancer and nutrition. Int. J. Cancer 2020, 147, 648–661. [Google Scholar] [CrossRef]
- Park, J.Y.; Seong, S.J.; Kim, T.J.; Kim, J.W.; Bae, D.S.; Nam, J.H. Significance of body weight change during fertility-sparing progestin therapy in young women with early endometrial cancer. Gynecol. Oncol. 2017, 146, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Mallik, R.; Chowdhury, T.A. Metformin in cancer. Diabetes Res. Clin. Pract. 2018, 143, 409–419. [Google Scholar] [CrossRef]
- Lee, J.; Yesilkanal, A.E.; Wynne, J.P.; Frankenberger, C.; Liu, J.; Yan, J.; Elbaz, M.; Rabe, D.C.; Rustandy, F.D.; Tiwari, P.; et al. Effective breast cancer combination therapy targeting BACH1 and mitochondrial metabolism. Nature 2019, 568, 254–258. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.S.; Kwon, A.R.; Lee, Y.K.; Oh, S.W. Circulating adipokines and risk of obesity related cancers: A systematic review and meta-analysis. Obes. Res. Clin. Pract. 2019, 13, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Hua, S.; Tian, W.; Zhang, L.; Zhao, J.; Zhang, H.; Zhang, W.; Xue, F. Mitogenic and anti-apoptotic effects of insulin in endometrial cancer are phosphatidylinositol 3-kinase/Akt dependent. Gynecol. Oncol. 2012, 125, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Gunter, M.J.; Hoover, D.R.; Yu, H.; Wassertheil-Smoller, S.; Manson, J.E.; Li, J.; Harris, T.G.; Rohan, T.E.; Xue, X.; Ho, G.Y.; et al. A prospective evaluation of insulin and insulin-like growth factor-I as risk factors for endometrial cancer. Cancer Epidemiol. Biomark. Prev. 2008, 17, 921–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mu, N.; Zhu, Y.; Wang, Y.; Zhang, H.; Xue, F. Insulin resistance: A significant risk factor of endometrial cancer. Gynecol. Oncol. 2012, 125, 751–757. [Google Scholar] [CrossRef]
- Yates, M.S.; Coletta, A.M.; Zhang, Q.; Schmandt, R.E.; Medepalli, M.; Nebgen, D.; Soletsky, B.; Milbourne, A.; Levy, E.; Fellman, B.; et al. Prospective randomized biomarker study of metformin and lifestyle intervention for prevention in obese women at increased risk for endometrial cancer. Cancer Prev. Res. 2018, 11, 477–490. [Google Scholar] [CrossRef] [Green Version]
- Yang, B.; Xie, L.; Zhang, H.; Zhu, Q.; Du, Y.; Luo, X.; Chen, X. Insulin resistance and overweight prolonged fertility-sparing treatment duration in endometrial atypical hyperplasia patients. J. Gynecol. Oncol. 2018, 29, e35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitsuhashi, A.; Habu, Y.; Kobayashi, T.; Kawarai, Y.; Ishikawa, H.; Usui, H.; Shozu, M. Long-term outcomes of progestin plus metformin as a fertility-sparing treatment for atypical endometrial hyperplasia and endometrial cancer patients. J. Gynecol. Oncol. 2019, 30, e90. [Google Scholar] [CrossRef]
- Alonso, S.; Castellanos, T.; Lapuente, F.; Chiva, L. Hysteroscopic surgery for conservative management in endometrial cancer: A review of the literature. Ecancermedicalscience 2015, 9, 505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzon, I.; Corrado, G.; Masciullo, V.; Morricone, D.; Ferrandina, G.; Scambia, G. Conservative surgical management of stage 1A endometrial carcinoma for fertility preservation. Fertil. Steril. 2010, 93, 1286–1289. [Google Scholar] [CrossRef] [PubMed]
- Laurelli, G.; Di Vagno, G.; Scaffa, C.; Losito, S.; Del Giudice, M.; Greggi, S. Conservative treatment of early endometrial cancer: Preliminary results of a pilot study. Gynecol. Oncol. 2011, 120, 43–46. [Google Scholar] [CrossRef]
- Giampaolino, P.; Di Spiezio Sardo, A.; Mollo, A.; Raffone, A.; Travaglino, A.; Boccellino, A.; Zizolfi, B.; Insabato, L.; Zullo, F.; De Placido, G.; et al. Hysteroscopic endometrial focal resection followed by levonorgestrel intrauterine device insertion as a fertility-sparing treatment of atypical endometrial hyperplasia and early endometrial cancer: A retrospective study. J. Minim. Invasive Gynecol. 2019, 26, 648–656. [Google Scholar] [CrossRef]
- Park, H.; Seong, S.J.; Yoon, B.S. The effect of operative hysteroscopy conducted befote progestins treatment in early stage endometrial cancer from the view of fertility. Gynecol. Oncol. 2011, 123, 427–428. [Google Scholar] [CrossRef]
- Jadoul, P.; Donnez, J. Conservative treatment may be beneficial for young women with atypical endometrial hyperplasia or endometrial adenocarcinoma. Fertil. Steril. 2003, 80, 1315–1324. [Google Scholar] [CrossRef]
- Ramirez, P.T.; Frumovitz, M.; Bodurka, D.C.; Sun, C.C.; Levenback, C. Hormonal therapy for the management of grade 1 endometrial adenocarcinoma: A literature review. Gynecol. Oncol. 2004, 95, 133–138. [Google Scholar] [CrossRef]
- American Cancer Society. Surgery for Endometrial Cancer; American Cancer Society: Atlanta, GA, USA, 2019. [Google Scholar]
- La Rosa, V.L.; Garzon, S.; Gullo, G.; Fichera, M.; Sisti, G.; Gallo, P.; Riemma, G.; Schiattarella, A. Fertility preservation in women affected by gynaecological cancer: The importance of an integrated gynaecological and psychological approach. Ecancermedicalscience. 2020, 14, 1035. [Google Scholar] [CrossRef]
- La Rosa, V.L.; De Franciscis, P.; Barra, F.; Schiattarella, A.; Török, P.; Shah, M.; Karaman, E.; Marques Cerentini, T.; Di Guardo, F.; Gullo, G.; et al. Quality of life in women with endometriosis: A narrative overview. Minerva Med. 2020, 111, 68–78. [Google Scholar] [CrossRef]
- Gullo, G.; Cucinella, G.; Perino, A.; Gullo, D.; Segreto, D.; Laganà, A.S.; Buzzaccarini, G.; Donarelli, Z.; Marino, A.; Allegra, A.; et al. The Gender Gap in the Diagnostic-Therapeutic Journey of the Infertile Couple. Int. J. Environ. Res. Public Health 2021, 18, 6184. [Google Scholar] [CrossRef]
- Huang, B.; Warner, M.; Gustafsson, J.Å. Estrogen receptors in breast carcinogenesis and endocrine therapy. Mol. Cell Endocrinol. 2015, 418 Pt 3, 240–244. [Google Scholar] [CrossRef]
- Tian, W.; Teng, F.; Zhao, J.; Gao, J.; Gao, C.; Sun, D.; Liu, G.; Zhang, Y.; Yu, S.; Zhang, W.; et al. Estrogen and insulin synergistically promote type 1 endometrial cancer progression. Cancer Biol. Ther. 2017, 18, 1000–1010. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Aromatase inhibitors versus tamoxifen in early breast cancer: Patient-level meta-analysis of the randomised trials. Lancet 2015, 386, 1341–1352. [Google Scholar] [CrossRef]
- Thomas, M.P.; Mills, S.J.; Potter, B.V. The “other” inositols and their phosphates: Synthesis, biology, and medicine (with recent advances in myo-inositol chemistry). Angew. Chem. Int. Ed. Eng. 2016, 55, 1614–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heimark, D.; McAllister, J.; Larner, J. Decreased myo-inositol to chiro-inositol (M/C) ratios and increased M/C epimerase activity in PCOS theca cells demonstrate increased insulin sensitivity compared to controls. Endocr. J. 2014, 61, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Nestler, J.E.; Unfer, V. Reflections on inositol(s) for PCOS therapy: Steps toward success. Gynecol. Endocrinol. 2015, 31, 501–505. [Google Scholar] [CrossRef]
- Sun, T.H.; Heimark, D.B.; Nguygen, T.; Nadler, J.L.; Larner, J. Both myo-inositol to chiro-inositol epimerase activities and chiro-inositol to myo-inositol ratios are decreased in tissues of GK type 2 diabetic rats compared to Wistar controls. Biochem. Biophys. Res. Commun. 2002, 293, 1092–1098. [Google Scholar] [CrossRef]
- Facchinetti, F.; Espinola, M.S.B.; Dewailly, D.; Ozay, A.C.; Prapas, N.; Vazquez-Levin, M.; Wdowiak, A.; Unfer, V. Expert Group on Inositols in Preclinical and Clinical Research. Breakthroughs in the Use of Inositols for Assisted Reproductive Treatment (ART). Trends Endocrinol. Metab. 2020. [Google Scholar] [CrossRef]
- Unfer, V.; Dinicola, S.; Laganà, A.S.; Bizzarri, M. Altered Ovarian Inositol Ratios May Account for Pathological Steroidogenesis in PCOS. Int. J. Mol. Sci. 2020, 21, 7157. [Google Scholar] [CrossRef]
- Facchinetti, F.; Dante, G.; Neri, I. The Ratio of MI to DCI and Its Impact in the Treatment of Polycystic Ovary Syndrome: Experimental and Literature Evidences. In Frontiers in Gynecological Endocrinology; ISGE Series; Genazzani, A., Tarlatzis, B., Eds.; Springer: Cham, Switzerland, 2016; pp. 103–109. [Google Scholar]
- Artini, P.G.; Obino, M.E.R.; Micelli, E.; Malacarne, E.; Vacca, C.; Papini, F.; Cela, V. Effect of d-chiro-inositol and alpha-lipoic acid combination on COH outcomes in overweight/obese PCOS women. Gynecol. Endocrinol. 2020. [Google Scholar] [CrossRef]
- Laganà, A.S.; Barbaro, L.; Pizzo, A. Evaluation of ovarian function and metabolic factors in women affected by polycystic ovary syndrome after treatment with D-Chiro-Inositol. Arch. Gynecol. Obstet. 2015, 291, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Cheang, K.I.; Baillargeon, J.P.; Essah, P.A.; Ostlund, R.E., Jr.; Apridonize, T.; Islam, L.; Nestler, J.E. Insulin-stimulated release of D-chiro-inositol-containing inositolphosphoglycan mediator correlates with insulin sensitivity in women with polycystic ovary syndrome. Metabolism 2008, 57, 1390–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurman, R.J.; Kaminski, P.F.; Norris, H.J. The behavior of endometrial hyperplasia. A long-term study of “untreated” hyperplasia in 170 patients. Cancer 1985, 56, 403–412. [Google Scholar] [CrossRef]
- Zhao, P.L.; Zhang, Q.F.; Yan, L.Y.; Huang, S.; Chen, Y.; Qiao, J. Functional investigation on aromatase in endometrial hyperplasia in polycystic ovary syndrome cases. Asian Pac. J. Cancer Prev. 2014, 15, 8975–8979. [Google Scholar] [CrossRef] [Green Version]
- Agorastos, T.; Vaitsi, V.; Pantazis, K.; Efstathiadis, E.; Vavilis, D.; Bontis, J.N. Aromatase inhibitor anastrozole for treating endometrial hyperplasia in obese postmenopausal women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 118, 239–240. [Google Scholar] [CrossRef]
- Iervolino, M.; Lepore, E.; Forte, G.; Laganà, A.S.; Buzzaccarini, G.; Unfer, V. Natural Molecules in the Management of Polycystic Ovary Syndrome (PCOS): An Analytical Review. Nutrients 2021, 13, 1677. [Google Scholar] [CrossRef]
- Gambioli, R.; Forte, G.; Buzzaccarini, G.; Unfer, V.; Laganà, A.S. Myo-Inositol as a Key Supporter of Fertility and Physiological Gestation. Pharmaceuticals 2021, 14, 504. [Google Scholar] [CrossRef] [PubMed]
- Gullo, G.; Carlomagno, G.; Unfer, V.; D’Anna, R. Myo-inositol: From induction of ovulation to menopausal disorder management. Minerva Ginecol. 2015, 67, 485–486. [Google Scholar]
- Urick, M.E.; Bell, D.W. Clinical actionability of molecular targets in endometrial cancer. Nat. Rev. Cancer 2019, 19, 510–521. [Google Scholar] [CrossRef]
- Cavaliere, A.F.; Perelli, F.; Zaami, S.; Piergentili, R.; Mattei, A.; Vizzielli, G.; Scambia, G.; Straface, G.; Restaino, S.; Signore, F. Towards Personalized Medicine: Non-Coding RNAs and Endometrial Cancer. Healthcare 2021, 9, 965. [Google Scholar] [CrossRef] [PubMed]
- Piergentili, R.; Zaami, S.; Cavaliere, A.F.; Signore, F.; Scambia, G.; Mattei, A.; Marinelli, E.; Gulia, C.; Perelli, F. Non-Coding RNAs as Prognostic Markers for Endometrial Cancer. Int. J. Mol. Sci. 2021, 22, 3151. [Google Scholar] [CrossRef] [PubMed]
- De Vincenzo, R.; Tortorella, L.; Ricci, C.; Cavaliere, A.F.; Zannoni, G.F.; Cefalo, M.G.; Scambia, G.; Fagotti, A. Locally advanced cervical cancer complicating pregnancy: A case of competing risks from the Catholic University of the Sacred Heart in Rome. Gynecol. Oncol. 2018, 150, 398–405. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Risk Factor | Endometrial Cancer | Ovarian Cancer | Cervical Cancer |
|---|---|---|---|
| Medical History | |||
| HPV infection | Necessary | ||
| Hysterectomy | ↓↓↓ | ? | |
| Tubal sterilization | ↓ | ||
| Endometriosis | – | ↑ CCC and END | |
| Diabetes | ↑ | ||
| Polycystic ovary syndrome | ↑ | ||
| Reproductive history and hormones | |||
| Older age at menarche | ↓ | – | |
| Younger age at menopause | ↓ | ↓ | |
| Parity | ↓↓↓ | ↓↓↓ | ↑ |
| Breastfeeding | – | ↓ | |
| Oral contraceptive pill | ↓↓↓ | ↓↓↓ | ↑ (recent use) |
| HRT: | |||
| –E only | ↑↑↑ | ↑↑ | |
| –Combined E + P | ↓? (continuous) | ↑ | |
| Fertility drugs | –? | –? | –? |
| Lifestyle | |||
| Overweight and obesity | ↑↑↑ | ↑ (not SER?) | – |
| Physical activity | ↓ | ? | |
| Diet | ↑ Glycemic index | ? | |
| Coffee | ↓ coffee | – | |
| Tea | ↓? green tea | ↓? green tea | |
| Smoking | ↓ | ↑↑ MUC | ↑ |
| Alcohol | – | – | |
| NSAIDs | ↓? | ? | |
| Talcum powder | –? | ↑ | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gullo, G.; Etrusco, A.; Cucinella, G.; Perino, A.; Chiantera, V.; Laganà, A.S.; Tomaiuolo, R.; Vitagliano, A.; Giampaolino, P.; Noventa, M.; et al. Fertility-Sparing Approach in Women Affected by Stage I and Low-Grade Endometrial Carcinoma: An Updated Overview. Int. J. Mol. Sci. 2021, 22, 11825. https://doi.org/10.3390/ijms222111825
Gullo G, Etrusco A, Cucinella G, Perino A, Chiantera V, Laganà AS, Tomaiuolo R, Vitagliano A, Giampaolino P, Noventa M, et al. Fertility-Sparing Approach in Women Affected by Stage I and Low-Grade Endometrial Carcinoma: An Updated Overview. International Journal of Molecular Sciences. 2021; 22(21):11825. https://doi.org/10.3390/ijms222111825
Chicago/Turabian StyleGullo, Giuseppe, Andrea Etrusco, Gaspare Cucinella, Antonino Perino, Vito Chiantera, Antonio Simone Laganà, Rossella Tomaiuolo, Amerigo Vitagliano, Pierluigi Giampaolino, Marco Noventa, and et al. 2021. "Fertility-Sparing Approach in Women Affected by Stage I and Low-Grade Endometrial Carcinoma: An Updated Overview" International Journal of Molecular Sciences 22, no. 21: 11825. https://doi.org/10.3390/ijms222111825