
Bladder Hyperactivity Induced by Oxidative Stress and Bladder Ischemia: A Review of Treatment Strategies with Antioxidants

 , and
, and
Abstract
:1. Overactive Bladder (OAB)
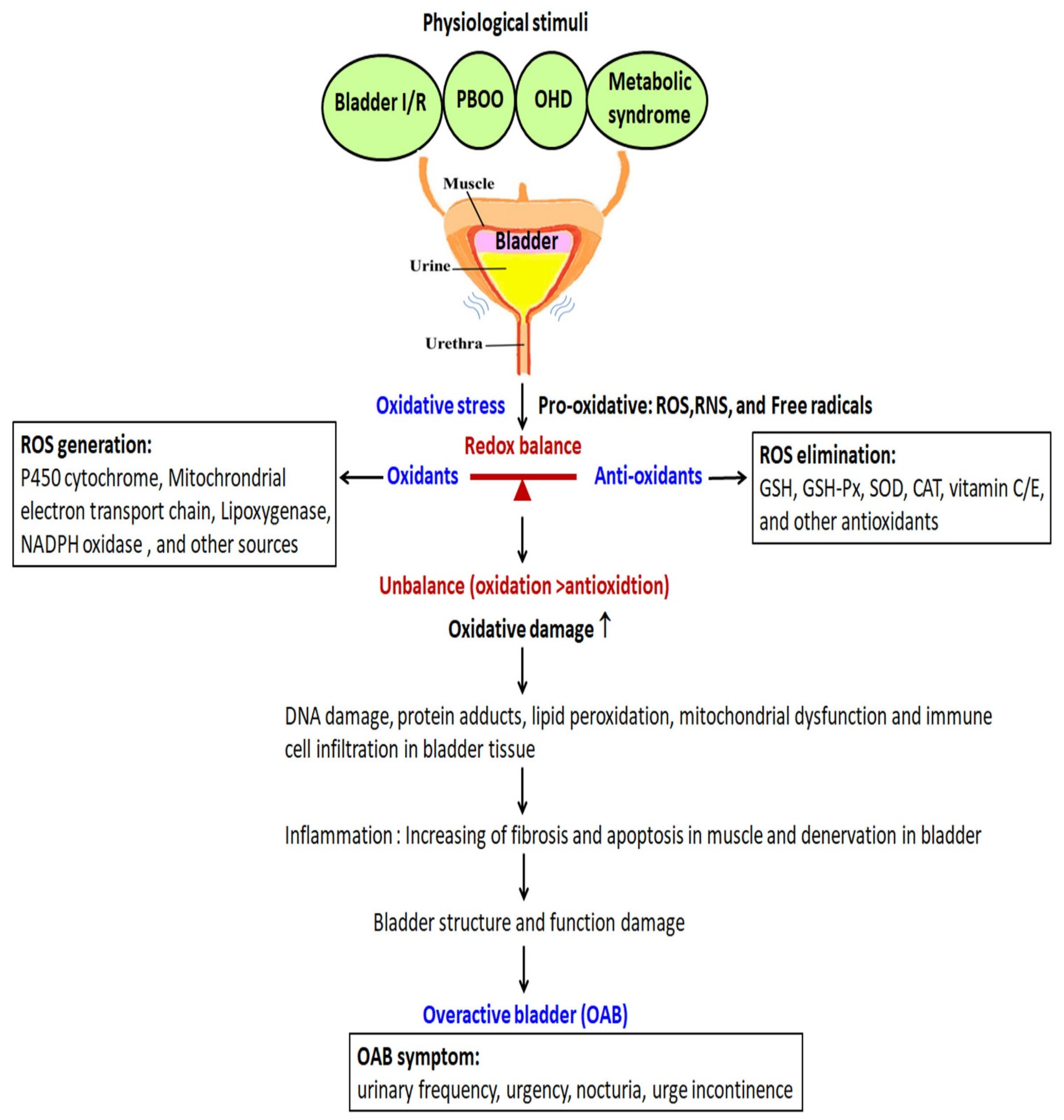
2. Pathophysiology of OAB and Its Relation with Oxidative Stress
3. Medical Management of OAB
4. Oxidative Stress and the Antioxidant Defense System
5. Redox Signaling and the Nrf2/ARE Pathway
6. Antioxidant Defense Systems
7. Oxidative Stress in OAB and Biomarkers of OAB
7.1. 8-Hydroxy-2′-Deoxyguanosine (8-OHdG)
7.2. Malondialdehyde (MDA)
7.3. Isoprostanes (IsoPs)
8. OAB Animal Model
8.1. OAB in a PBOO Model
8.2. OAB in Chronic Ischemia and Ischemia/Reperfusion Bladder Model
8.3. OAB in Metabolic Syndrome (MetS) Model
8.4. OAB in Menopause and Ovarian Hormone Deficiency (OHD) Model
9. Antioxidant Treatment in OAB
9.1. Epigallocatechin-3-Gallate (EGCG)
9.2. Coenzyme Q10 (CoQ10)
9.3. Melatonin
9.4. Omega-3 Fatty Acid
9.5. Eviprostat
9.6. Sulforaphane
9.7. Hydrogen Water
10. Problems to Be Solved in the Future
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ARE | antioxidant response element |
| α1-AR | α1- adrenoceptor |
| β -AR | β-adrenoceptor |
| BDNF | brain-derived neurotrophic factor |
| BPH | benign prostatic hyperplasia |
| CAT | catalases |
| COX-2 | cyclooxygenase-2 |
| CRP | C-reactive protein |
| DO | detrusor overactivity |
| EGCG | epigallocatechin-3-gallate |
| F2-IsoPs | F2-isoprostanes |
| GSH | glutathione |
| GSH-Px | glutathione peroxidase |
| HFHS | high fat high sugar |
| HO-1 | hemeoxygenase-1 |
| IC/PBS | interstitial cystitis/painful bladder syndrome |
| I/R | ischemia/reperfusion |
| Keap1 | Kelch-like ECH-associated protein 1 |
| LUTS | lower urinary tract symptoms |
| MDA | malondialdehyde |
| NGF | nerve growth factor |
| Nrf2 | nuclear transcription factor E2-related factor 2 |
| NOS | nitric oxide synthase |
| NOX | nicotinamide adenine dinucleotide phosphate (NADPH) oxidase |
| OAB | overactive bladder |
| OVX | ovariectomy |
| OHD | ovarian hormone depletion (deficiency) |
| 8-OHdG | 8-hydroxy-2′-deoxyguanosine |
| PBOO | partial bladder outlet obstruction |
| PGE2 | prostaglandin E2 |
| ROS | reactive oxygen species |
| SOD | superoxide dismutase |
| UTI | urinary tract infection |
References
- Przydacz, M.; Golabek, T.; Dudek, P.; Lipinski, M.; Chlosta, P. Prevalence and bother of lower urinary tract symptoms and overactive bladder in Poland, an Eastern European Study. Sci. Rep. 2020, 10, 19819. [Google Scholar] [CrossRef] [PubMed]
- Haylen, B.T.; de Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K.; et al. An international urogynecological association (IUGA)/international continence society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol. Urodyn. 2010, 29, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Lapitan, M.C.; Chye, P.L.; Asia-Pacific Continence Advisory, B. The epidemiology of overactive bladder among females in Asia: A questionnaire survey. Int. Urogynecol. J. Pelvic Floor Dysfunct. 2001, 12, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Moorthy, P.; Lapitan, M.C.; Quek, P.L.; Lim, P.H. Prevalence of overactive bladder in Asian men: An epidemiological survey. BJU Int. 2004, 93, 528–531. [Google Scholar] [CrossRef] [Green Version]
- Chuang, Y.-C.; Liu, S.-P.; Lee, K.-S.; Liao, L.; Wang, J.; Yoo, T.K.; Chu, R.; Sumarsono, B. Prevalence of overactive bladder in China, Taiwan and South Korea: Results from a cross-sectional, population-based study. LUTS Low. Urin. Tract Symptoms 2019, 11, 48–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenks, J.C. Overactive bladder in women. Nurs. Stand. 2016, 31, 52–63. [Google Scholar] [CrossRef]
- Al-Zahrani, A.A.; Gajewski, J. Urodynamic findings in women with refractory overactive bladder symptoms. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2016, 23, 75–79. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.S.; Vittinghoff, E.; Wyman, J.F.; Stone, K.L.; Nevitt, M.C.; Ensrud, K.; Grady, D. Urinary Incontinence: Does it Increase Risk for Falls and Fractures? J. Am. Geriatr. Soc. 2000, 48, 721–725. [Google Scholar] [CrossRef]
- Chu, F.M.; Dmochowski, R. Pathophysiology of overactive bladder. Am. J. Med. 2006, 119, 3–8. [Google Scholar] [CrossRef]
- Yoshimura, N.; Kaiho, Y.; Miyazato, M.; Yunoki, T.; Tai, C.; Chancellor, M.B.; Tyagi, P. Therapeutic receptor targets for lower urinary tract dysfunction. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2008, 377, 437–448. [Google Scholar] [CrossRef]
- Azadzoi, K.M.; Shinde, V.M.; Tarcan, T.; Kozlowski, R.; Siroky, M.B. Increased leukotriene and prostaglandin release, and overactivity in the chronically ischemic bladder. J. Urol. 2003, 169, 1885–1891. [Google Scholar] [CrossRef]
- Apostolidis, A.; Brady, C.M.; Yiangou, Y.; Davis, J.; Fowler, C.J.; Anand, P. Capsaicin receptor TRPV1 in urothelium of neurogenic human bladders and effect of intravesical resiniferatoxin. Urology 2005, 65, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Chai, T.C. Up-regulation of P2 × 3 receptor during stretch of bladder urothelial cells from patients with interstitial cystitis. J. Urol. 2004, 171, 448–452. [Google Scholar] [CrossRef]
- Yokoyama, T.; Nozaki, K.; Fujita, O.; Nose, H.; Inoue, M.; Kumon, H. Role of c afferent fibers and monitoring of intravesical resiniferatoxin therapy for patients with idiopathic detrusor overactivity. J. Urol. 2004, 172, 596–600. [Google Scholar] [CrossRef] [PubMed]
- Birder, L.A.; de Groat, W.C. Mechanisms of disease: Involvement of the urothelium in bladder dysfunction. Nat. Clin. Pract. Urol. 2007, 4, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Munoz, A.; Smith, C.P.; Boone, T.B.; Somogyi, G.T. Overactive and underactive bladder dysfunction is reflected by alterations in urothelial ATP and NO release. Neurochem. Int. 2011, 58, 295–300. [Google Scholar] [CrossRef] [Green Version]
- Masuda, H.; Kihara, K.; Saito, K.; Matsuoka, Y.; Yoshida, S.; Chancellor, M.B.; De Groat, W.C.; Yoshimura, N. Reactive oxygen species mediate detrusor overactivity via sensitization of afferent pathway in the bladder of anaesthetized rats. BJU Int. 2008, 101, 775–780. [Google Scholar] [CrossRef]
- Azadzoi, K.M.; Tarcan, T.; Kozlowski, R.; Krane, R.J.; Siroky, M.B. Overactivity and structural changes in the chronically ischemic bladder. J. Urol. 1999, 162, 1768–1778. [Google Scholar] [CrossRef]
- Nomiya, M.; Yamaguchi, O.; Andersson, K.-E.; Sagawa, K.; Aikawa, K.; Shishido, K.; Yanagida, T.; Kushida, N.; Yazaki, J.; Takahashi, N. The effect of atherosclerosis-induced chronic bladder ischemia on bladder function in the rat. Neurourol. Urodynamics 2012, 31, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Chapple, C.R.; Nazir, J.; Hakimi, Z.; Bowditch, S.; Fatoye, F.; Guelfucci, F.; Khemiri, A.; Siddiqui, E.; Wagg, A. Persistence and Adherence with Mirabegron versus Antimuscarinic Agents in Patients with Overactive Bladder: A Retrospective Observational Study in UK Clinical Practice. Eur. Urol. 2017, 72, 389–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapple, C.R.; Khullar, V.; Gabriel, Z.; Muston, D.; Bitoun, C.E.; Weinstein, D. The Effects of Antimuscarinic Treatments in Overactive Bladder: An Update of a Systematic Review and Meta-Analysis. Eur. Urol. 2008, 54, 543–562. [Google Scholar] [CrossRef] [PubMed]
- Carrière, I.; Fourrier-Reglat, A.; Dartigues, J.-F.; Rouaud, O.; Pasquier, F.; Ritchie, K.; Ancelin, M.-L. Drugs With Anticholinergic Properties, Cognitive Decline, and Dementia in an Elderly General Population. Arch. Intern. Med. 2009, 169, 1317–1324. [Google Scholar] [CrossRef] [Green Version]
- Orasanu, B.; Mahajan, S.T. The use of botulinum toxin for the treatment of overactive bladder syndrome. Indian J. Urol. 2013, 29, 2–11. [Google Scholar] [CrossRef]
- Marcelissen, T.; Cornu, J.-N.; Antunes-Lopes, T.; Geavlete, B.; Delongchamps, N.B.; Rashid, T.; Rieken, M.; Rahnama’I, M.S. Management of Idiopathic Overactive Bladder Syndrome: What Is the Optimal Strategy After Failure of Conservative Treatment? Eur. Urol. Focus 2018, 4, 760–767. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.H.; Yu, W.R.; Kuo, H.C. Therapeutic Effect of Botulinum Toxin A on Sensory Bladder Disorders-From Bench to Bedside. Toxins 2020, 12, 166. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-C.; Chuang, S.-M.; Lin, K.-L.; Chen, W.-C.; Lu, J.-H.; Chueh, K.-S.; Shen, M.-C.; Liu, L.-W.; Long, C.-Y.; Juan, Y.-S. Low-Intensity Extracorporeal Shock Wave Therapy Ameliorates the Overactive Bladder: A Prospective Pilot Study. BioMed Res. Int. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Sies, H. Hydrogen peroxide as a central redox signaling molecule in physiological oxidative stress: Oxidative eustress. Redox Biol. 2017, 11, 613–619. [Google Scholar] [CrossRef]
- Lambeth, J.D. NOX enzymes and the biology of reactive oxygen. Nat. Rev. Immunol. 2004, 4, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Brand, M.D. The sites and topology of mitochondrial superoxide production. Exp. Gerontol. 2010, 45, 466–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nocchi, L.; Daly, D.M.; Chapple, C.; Grundy, D. Induction of oxidative stress causes functional alterations in mouse urothelium via a TRPM8-mediated mechanism: Implications for aging. Aging Cell 2014, 13, 540–550. [Google Scholar] [CrossRef]
- Nguyen, T.; Nioi, P.; Pickett, C.B. The Nrf2-antioxidant response element signaling pathway and its activation by oxidative stress. J. Biol. Chem. 2009, 284, 13291–13295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levonen, A.-L.; Landar, A.; Ramachandran, A.; Ceaser, E.K.; Dickinson, D.A.; Zanoni, G.; Morrow, J.D.; Darley-Usmar, V.M. Cellular mechanisms of redox cell signalling: Role of cysteine modification in controlling antioxidant defences in response to electrophilic lipid oxidation products. Biochem. J. 2004, 378, 373–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, K.; Luo, M.; Wei, S. The Bioprotective Effects of Polyphenols on Metabolic Syndrome against Oxidative Stress: Evidences and Perspectives. Oxid. Med. Cell Longev. 2019, 2019, 6713194. [Google Scholar] [CrossRef] [Green Version]
- Baird, L.; Yamamoto, M. The Molecular Mechanisms Regulating the KEAP1-NRF2 Pathway. Mol. Cell. Biol. 2020, 40. [Google Scholar] [CrossRef] [PubMed]
- Hyung, J.H.; Ahn, C.B.; Il Kim, B.; Kim, K.; Je, J.Y. Involvement of Nrf2-mediated heme oxygenase-1 expression in anti-inflammatory action of chitosan oligosaccharides through MAPK activation in murine macrophages. Eur. J. Pharm. 2016, 793, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Teng, H.; Zhang, K.Y.; Skalicka-Woźniak, K.; Georgiev, M.I.; Xiao, J. Agrimonolide and Desmethylagrimonolide Induced HO-1 Expression in HepG2 Cells through Nrf2-Transduction and p38 Inactivation. Front. Pharmacol. 2017, 7, 513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Costa, L.A.; Badawi, A.; El-Sohemy, A. Nutrigenetics and modulation of oxidative stress. Ann. Nutr. Metab. 2012, 60 (Suppl. S3), 27–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fridovich, I. Superoxide anion radical (O2-.), superoxide dismutases, and related matters. J. Biol. Chem. 1997, 272, 18515–18517. [Google Scholar] [CrossRef] [Green Version]
- Guven, A.; Kalorin, C.; Onal, B.; Whitbeck, C.; Chichester, P.; Kogan, B.A.; Levin, R.M.; Mannikarottu, A. Novel biomarkers of bladder decompensation after partial bladder obstruction. Neurourol. Urodynamics 2007, 26, 1036–1042. [Google Scholar] [CrossRef]
- Zelko, I.N.; Mariani, T.J.; Folz, R.J. Superoxide dismutase multigene family: A comparison of the CuZn-SOD (SOD1), Mn-SOD (SOD2), and EC-SOD (SOD3) gene structures, evolution, and expression. Free Radic. Biol. Med. 2002, 33, 337–349. [Google Scholar] [CrossRef]
- Bhide, A.A.; Cartwright, R.; Khullar, V.; Digesu, G.A. Biomarkers in overactive bladder. Int. Urogynecol. J. 2013, 24, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, J.-T.; Kuo, K.-L.; Liu, S.-H.; Shi, C.-S.; Chang, H.-C.; Lin, W.-C.; Chou, C.-T.; Hsu, C.-H.; Liao, S.-M.; Wang, Z.-H.; et al. Epigallocatechin Gallate Attenuates Partial Bladder Outlet Obstruction-induced Bladder Injury via Suppression of Endoplasmic Reticulum Stress-related Apoptosis—In Vivo Study. Urol. 2016, 91, 242.e1–242.e9. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.; Poirier, C.; Gaspar, T.; Gratzke, C.; Harrison, W.; Busija, D.; Matzuk, M.M.; Andersson, K.-E.; Overbeek, P.; Bishop, C.E. A Mutation in the Inner Mitochondrial Membrane Peptidase 2-Like Gene (Immp2l) Affects Mitochondrial Function and Impairs Fertility in Mice1. Biol. Reprod. 2008, 78, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Soler, R.; Fullhase, C.; Lu, B.; Bishop, C.E.; Andersson, K.E. Bladder dysfunction in a new mutant mouse model with increased superoxide--lack of nitric oxide? J. Urol. 2010, 183, 780–785. [Google Scholar] [CrossRef] [Green Version]
- Andersson, K.E. Oxidative stress and its possible relation to lower urinary tract functional pathology. BJU Int. 2018, 121, 527–533. [Google Scholar] [CrossRef] [Green Version]
- Dalle-Donne, I.; Rossi, R.; Colombo, R.; Giustarini, D.; Milzani, A. Biomarkers of oxidative damage in human disease. Clin. Chem. 2006, 52, 601–623. [Google Scholar] [CrossRef] [PubMed]
- Oka, M.; Fukui, T.; Ueda, M.; Tagaya, M.; Oyama, T.; Tanaka, M. Suppression of Bladder Oxidative Stress and Inflammation by a Phytotherapeutic Agent in a Rat Model of Partial Bladder Outlet Obstruction. J. Urol. 2009, 182, 382–390. [Google Scholar] [CrossRef]
- Lin, W.-Y.; Wu, S.-B.; Lin, Y.-P.; Chang, P.-J.; Levin, R.M.; Wei, Y.-H. Reversing bladder outlet obstruction attenuates systemic and tissue oxidative stress. BJU Int. 2012, 110, 1208–1213. [Google Scholar] [CrossRef]
- Matsumoto, S.; Hanai, T.; Matsui, T.; Oka, M.; Tanaka, M.; Uemura, H. Eviprostat suppresses urinary oxidative stress in a rabbit model of partial bladder outlet obstruction and in patients with benign prostatic hyperplasia. Phytotherapy Res. 2009, 24, 301–303. [Google Scholar] [CrossRef]
- Dokumacioglu, E.; Demiray, O.; Dokumacioglu, A.; Sahin, A.; Sen, T.M.; Cankaya, S. Measuring urinary 8-hydroxy-2′-deoxyguanosine and malondialdehyde levels in women with overactive bladder. Investig. Clin. Urol. 2018, 59, 252–256. [Google Scholar] [CrossRef]
- Lin, W.-Y.; Chen, C.-S.; Wu, S.-B.; Lin, Y.-P.; Levin, R.M.; Wei, Y.-H. Oxidative stress biomarkers in urine and plasma of rabbits with partial bladder outlet obstruction. BJU Int. 2010, 107, 1839–1843. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, N.; Yamaguchi, O.; Nomiya, M.; Aikawa, K.; Kimura, J. Preventive Effect of Hydrogen Water on the Development of Detrusor Overactivity in a Rat Model of Bladder Outlet Obstruction. J. Urol. 2016, 195, 780–787. [Google Scholar] [CrossRef]
- Rada, M.P.; Ciortea, R.; Măluţan, A.M.; Doumouchtsis, S.K.; Bucuri, C.E.; Clim, A.; Roman, A.; Mihu, D. The profile of urinary biomarkers in overactive bladder. Neurourol. Urodynamics 2020, 39, 2305–2313. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, A.; Başeskioğlu, B.; Temel, H.E.; Erkasap, N.; Yenilmez, A.; Uslu, S.; Özer, C.; Ozkurt, M.; Dönmez, T. Effect of αlipoic acid and silymarin on bladder outlet obstruction. Exp. Ther. Med. 2012, 5, 596–602. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Xu, H.; Fu, S.; Chen, Y.; Chen, Q.; Cai, Z.; Zhou, J.; Wang, Z. Sulforaphane Ameliorates Bladder Dysfunction through Activation of the Nrf2-ARE Pathway in a Rat Model of Partial Bladder Outlet Obstruction. Oxidative Med. Cell. Longev. 2016, 2016, 1–12. [Google Scholar] [CrossRef]
- Sener, G.; Sehirli, A.O.; Paskaloglu, K.; Dulger, G.A.; Alican, I. Melatonin treatment protects against ischemia/reperfusion-induced functional and biochemical changes in rat urinary bladder. J. Pineal Res. 2003, 34, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Onur, R.; Tasdemir, C.; Seckin, D.; Ilhan, N.; Kutlu, S.; Akpolat, N. Combined Use of Melatonin and Terazosin Restores Bladder Contractility in Rabbits With Partial Outlet Obstruction. Urology 2008, 72, 439–443. [Google Scholar] [CrossRef]
- Firat, F.; Uluocak, N.; Erdemir, F.; Atilgan, D.; Markoc, F.; Parlaktas, B.S.; Yasar, A. Evaluation of the effects of omega-3 & interferon alpha-2b administration on partial bladder outlet obstruction in a rat model. Indian J. Med Res. 2016, 144, 572–579. [Google Scholar]
- Sezginer, E.K.; Yilmaz-Oral, D.; Lokman, U.; Nebioglu, S.; Aktan, F.; Gur, S. Effects of varying degrees of partial bladder outlet obstruction on urinary bladder function of rats: A novel link to inflammation, oxidative stress and hypoxia. LUTS: Low. Urin. Tract Symptoms 2019, 11, O193–O201. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Shen, W.; An, W.; Li, Q.; Qiu, S.; Jiang, S. A Chinese Medicine Formula “Xian-Jia-Tang” for Treating Bladder Outlet Obstruction by Improving Urodynamics and Inhibiting Oxidative Stress through Potassium Channels. Evidence-Based Complement. Altern. Med. 2017, 2017, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gu, M.; Liu, C.; Wan, X.; Yang, T.; Chen, Y.; Zhou, J.; Chen, Q.; Wang, Z. Epigallocatechin Gallate Attenuates Bladder Dysfunction via Suppression of Oxidative Stress in a Rat Model of Partial Bladder Outlet Obstruction. Oxidative Med. Cell. Longev. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Stephany, H.A.; Strand, D.; Ching, C.B.; Tanaka, S.T.; Milne, G.L.; Cajaiba, M.M.; Thomas, J.C.; Pope, J.C.; Adams, M.C.; Brock, J.W.; et al. Chronic Cyclic Bladder Over Distention Up-Regulates Hypoxia Dependent Pathways. J. Urol. 2013, 190, 1603–1609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clayton, D.B.; Stephany, H.A.; Ching, C.B.; Rahman, S.A.; Tanaka, S.T.; Thomas, J.C.; Pope, J.C.; Adams, M.C.; Brock, J.W.; Clark, P.E.; et al. F 2 -Isoprostanes as a Biomarker of Oxidative Stress in the Mouse Bladder. J. Urol. 2014, 191, 1597–1601. [Google Scholar] [CrossRef]
- Matsui, T.; Oka, M.; Fukui, T.; Tanaka, M.; Oyama, T.; Sagawa, K.; Nomiya, M.; Yamaguchi, O. Suppression of bladder overactivity and oxidative stress by the phytotherapeutic agent, Eviprostat, in a rat model of atherosclerosis-induced chronic bladder ischemia. Int. J. Urol. 2012, 19, 669–675. [Google Scholar] [CrossRef]
- Milne, G.L.; Yin, H.; Hardy, K.D.; Davies, S.S.; Roberts, L.J., 2nd. Isoprostane generation and function. Chem. Rev. 2011, 111, 5973–5996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dambros, M.; Dambros, M.C.; Lorenzetti, F.; Dassen, E.L.; van Koeveringe, G.A. The use of hypochlorous acid as a model for investigating bladder overactivity. Int. Braz. J. Urol. 2014, 40, 408–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, C.H. Benign prostatic hyperplasia is a significant risk factor for bladder cancer in diabetic patients: A population-based cohort study using the National Health Insurance in Taiwan. BMC Cancer 2013, 13, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callaghan, C.M.; Johnson, A.; Neumann, P.; Leggett, R.E.; Schuler, C.; Levin, R.M. The effect of partial outlet obstruction on calpain and phospholipase-2 activities: Analyzed by severity and duration. Mol. Cell. Biochem. 2013, 381, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Levin, S.S.; Wein, A.J.; Levin, R.M. Correlation of ischemia/reperfusion or partial outlet obstruction-induced spectrin proteolysis by calpain with contractile dysfunction in rabbit bladder. Urology 1997, 49, 293–300. [Google Scholar] [CrossRef]
- Kim, J.C.; Yoo, J.S.; Park, E.Y.; Hong, S.H.; Seo, S.I.; Hwang, T.-K. Muscarinic and purinergic receptor expression in the urothelium of rats with detrusor overactivity induced by bladder outlet obstruction. BJU Int. 2008, 101, 371–375. [Google Scholar] [CrossRef]
- Azadzoi, K.M.; Pontari, M.; Vlachiotis, J.; Siroky, M.B. Canine bladder blood flow and oxygenation: Changes induced by filling, contraction and outlet obstruction. J. Urol. 1996, 155, 1459–1465. [Google Scholar] [CrossRef]
- Koritsiadis, G.; Stravodimos, K.; Koutalellis, G.; Agrogiannis, G.; Koritsiadis, S.; Lazaris, A.; Constantinides, C. Immunohistochemical estimation of hypoxia in human obstructed bladder and correlation with clinical variables. BJU Int. 2008, 102, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, C.M.; Schuler, C.; Leggett, R.E.; Levin, R.M. Effect of severity and duration of bladder outlet obstruction on catalase and superoxide dismutase activity. Int. J. Urol. 2013, 20, 1130–1135. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Bai, Y.; Yang, H.; Yang, H.W. Investigation on lower urinary tract symptoms (LUTS) in elderly patients with prostate cancer (PC) received endocrine therapy. Arch. Gerontol. Geriatr. 2015, 60, 535–537. [Google Scholar] [CrossRef]
- Pinggera, G.-M.; Mitterberger, M.; Steiner, E.; Pallwein, L.; Frauscher, F.; Aigner, F.; Bartsch, G.; Strasser, H. Association of lower urinary tract symptoms and chronic ischaemia of the lower urinary tract in elderly women and men: Assessment using colour Doppler ultrasonography. BJU Int. 2008, 102, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, E.C.; Calmasini, F.B.; De Oliveira, M.G.; Silva, F.H.; Da Silva, C.P.; André, D.M.; Leonardo, F.C.; Delbin, M.A.; Antunes, E. Chronic treatment with resveratrol improves overactive bladder in obese mice via antioxidant activity. Eur. J. Pharmacol. 2016, 788, 29–36. [Google Scholar] [CrossRef]
- Juan, Y.-S.; Li, S.; Levin, R.M.; Kogan, B.A.; Schuler, C.; Leggett, R.E.; Huang, C.-H.; Mannikarottu, A. The Effect of Ischemia/Reperfusion on Rabbit Bladder—Role of Rho-kinase and Smooth Muscle Regulatory Proteins. Urology 2009, 73, 1126–1130. [Google Scholar] [CrossRef]
- Andreadou, I.; Iliodromitis, E.K.; Lazou, A.; Görbe, A.; Giricz, Z.; Schulz, R.; Ferdinandy, P. Effect of hypercholesterolaemia on myocardial function, ischaemia-reperfusion injury and cardioprotection by preconditioning, postconditioning and remote conditioning. Br. J. Pharmacol. 2017, 174, 1555–1569. [Google Scholar] [CrossRef]
- Andersson, K.E.; Boedtkjer, D.B.; Forman, A. The link between vascular dysfunction, bladder ischemia, and aging bladder dysfunction. Ther. Adv. Urol. 2017, 9, 11–27. [Google Scholar] [CrossRef]
- De Nunzio, C.; Cindolo, L.; Gacci, M.; Pellegrini, F.; Carini, M.; Lombardo, R.; Franco, G.; Tubaro, A. Metabolic Syndrome and Lower Urinary Tract Symptoms in Patients With Benign Prostatic Enlargement: A Possible Link to Storage Symptoms. Urology 2014, 84, 1181–1187. [Google Scholar] [CrossRef]
- Nomiya, M.; Sagawa, K.; Yazaki, J.; Takahashi, N.; Kushida, N.; Haga, N.; Aikawa, K.; Matsui, T.; Oka, M.; Fukui, T.; et al. Increased bladder activity is associated with elevated oxidative stress markers and proinflammatory cytokines in a rat model of atherosclerosis-induced chronic bladder ischemia. Neurourol. Urodynamics 2011, 31, 185–189. [Google Scholar] [CrossRef]
- Nomiya, M.; Andersson, K.E.; Yamaguchi, O. Chronic bladder ischemia and oxidative stress: New pharmacotherapeutic targets for lower urinary tract symptoms. Int. J. Urol. 2015, 22, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Canada Clinical Practice Guidelines Expert Committee; Punthakee, Z.; Goldenberg, R.; Katz, P. Definition, Classification and Diagnosis of Diabetes, Prediabetes and Metabolic Syndrome. Can. J. Diabetes 2018, 42 (Suppl. S1), S10–S15. [Google Scholar] [CrossRef] [Green Version]
- Hong, G.S.; Shim, B.S.; Chung, W.S.; Yoon, H. Correlation between Metabolic Syndrome and Lower Urinary Tract Symptoms of Males and Females in the Aspect of Gender-Specific Medicine: A Single Institutional Study. Korean J. Urol. 2010, 51, 631–635. [Google Scholar] [CrossRef] [Green Version]
- Uzun, H.; Zorba, O.U. Metabolic syndrome in female patients with overactive bladder. Urology 2012, 79, 72–75. [Google Scholar] [CrossRef]
- Bunn, F.; Kirby, M.; Pinkney, E.; Cardozo, L.; Chapple, C.; Chester, K.; Cruz, F.; Haab, F.; Kelleher, C.; Milsom, I.; et al. Is there a link between overactive bladder and the metabolic syndrome in women? A systematic review of observational studies. Int. J. Clin. Pr. 2015, 69, 199–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, Q.; Wang, Z.; Liu, G.; Daneshgari, F.; MacLennan, G.T.; Gupta, S. Metabolic syndrome, inflammation and lower urinary tract symptoms: Possible translational links. Prostate Cancer Prostatic Dis. 2016, 19, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Peyronnet, B.; Mironska, E.; Chapple, C.; Cardozo, L.; Oelke, M.; Dmochowski, R.; Amarenco, G.; Gamé, X.; Kirby, R.; Van Der Aa, F.; et al. A Comprehensive Review of Overactive Bladder Pathophysiology: On the Way to Tailored Treatment. Eur. Urol. 2019, 75, 988–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankovic, A.; Korac, A.; Buzadzic, B.; Stancic, A.; Otasevic, V.; Ferdinandy, P.; Daiber, A.; Korac, B. Targeting the NO/superoxide ratio in adipose tissue: Relevance to obesity and diabetes management. Br. J. Pharmacol. 2016, 174, 1570–1590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leiria, L.O.; Silva, F.H.; Davel, A.; Alexandre, E.C.; Calixto, M.C.; De Nucci, G.; Mónica, F.Z.; Antunes, E. The Soluble Guanylyl Cyclase Activator BAY 60-2770 Ameliorates Overactive Bladder in Obese Mice. J. Urol. 2014, 191, 539–547. [Google Scholar] [CrossRef]
- Rolo, A.P.; Palmeira, C.M. Diabetes and mitochondrial function: Role of hyperglycemia and oxidative stress. Toxicol. Appl. Pharm. 2006, 212, 167–178. [Google Scholar] [CrossRef] [Green Version]
- Wallace, D.C. A mitochondrial paradigm of metabolic and degenerative diseases, aging, and cancer: A dawn for evolutionary medicine. Annu. Rev. Genet. 2005, 39, 359–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, S.D.; Chien, C.T.; Yu, H.J. Alterations in peripheral purinergic and muscarinic signaling of rat bladder after long-term fructose-induced metabolic syndrome. Eur. J. Nutr. 2013, 52, 347–359. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-L.; Lin, K.-L.; Wu, B.-N.; Chuang, S.-M.; Wu, W.J.; Lee, Y.-C.; Ho, W.-T.; Juan, Y.-S. Epigallocatechin-3-gallate alleviates bladder overactivity in a rat model with metabolic syndrome and ovarian hormone deficiency through mitochondria apoptosis pathways. Sci. Rep. 2018, 8, 1–15. [Google Scholar] [CrossRef]
- Furukawa, S.; Fujita, T.; Shimabukuro, M.; Iwaki, M.; Yamada, Y.; Nakajima, Y.; Nakayama, O.; Makishima, M.; Matsuda, M.; Shimomura, I. Increased oxidative stress in obesity and its impact on metabolic syndrome. J. Clin. Investig. 2004, 114, 1752–1761. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.; Cardozo, L.D. The role of estrogens in female lower urinary tract dysfunction. Urology 2003, 62, 45–51. [Google Scholar] [CrossRef]
- Cardozo, L.; Lose, G.; McClish, D.; Versi, E. A systematic review of the effects of estrogens for symptoms suggestive of overactive bladder. Acta Obs. Gynecol. Scand. 2004, 83, 892–897. [Google Scholar] [CrossRef]
- Nappi, R.E.; Palacios, S.; Panay, N.; Particco, M.; Krychman, M.L. Vulvar and vaginal atrophy in four European countries: Evidence from the European REVIVE Survey. Climacteric J. Int. Menopause Soc. 2016, 19, 188–197. [Google Scholar] [CrossRef] [Green Version]
- Batra, S.C.; Iosif, C.S. Progesterone receptors in the female lower urinary tract. J. Urol. 1987, 138, 1301–1304. [Google Scholar] [CrossRef]
- Blakeman, P.J.; Hilton, P.; Bulmer, J.N. Oestrogen and progesterone receptor expression in the female lower urinary tract, with reference to oestrogen status. BJU Int. 2000, 86, 32–38. [Google Scholar] [CrossRef]
- Cheng, C.L.; Li, J.R.; Lin, C.H.; de Groat, W.C. Positive association of female overactive bladder symptoms and estrogen deprivation: A nationwide population-based cohort study in Taiwan. Medicine 2016, 95, e4107. [Google Scholar] [CrossRef]
- Krause, M.; Wheeler, T.L., 2nd; Snyder, T.E.; Richter, H.E. Local Effects of Vaginally Administered Estrogen Therapy: A Review. J. Pelvic Med. Surg. 2009, 15, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Juan, Y.-S.; Chuang, S.-M.; Long, C.-Y.; Chen, C.-H.; Levin, R.M.; Liu, K.-M. Neuroprotection of green tea catechins on surgical menopause-induced overactive bladder in a rat model. Menopause 2012, 19, 346–354. [Google Scholar] [CrossRef]
- Juan, Y.-S.; Huang, C.-H.; Lee, Y.-L.; Long, C.-Y.; Wu, T.-H.; Chang, W.-C.; Levin, R.M.; Liu, K.-M. Green tea catechins decrease oxidative stress in surgical menopause-induced overactive bladder in a rat model. BJU Int. 2012, 110, E236–E244. [Google Scholar] [CrossRef] [PubMed]
- Weiderpass, E.; A Baron, J.; Adami, H.-O.; Magnusson, C.; Lindgren, A.; Bergström, R.; Correia, N.; Persson, I. Low-potency oestrogen and risk of endometrial cancer: A case-control study. Lancet 1999, 353, 1824–1828. [Google Scholar] [CrossRef]
- Iosif, C.S.; Bekassy, Z. Prevalence of genito-urinary symptoms in the late menopause. Acta Obs. Gynecol. Scand. 1984, 63, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.-Y.; Li, S.; Leggett, R.; Strassner, J.; Sokol, R.; Schuler, C.; Juan, Y.-S.; Javed, Z.; Kogan, B.; Levin, R.M.; et al. Estrogen administration attenuates bladder outlet obstruction induced oxidative stress in the female rabbit. Neurourol. Urodynamics 2009, 28, 95–100. [Google Scholar] [CrossRef]
- Chuang, S.-M.; Long, C.-Y.; Lin, R.-J.; Liu, K.-M.; Levin, R.M.; Chang, C.-Y.; Ho, Y.-W.; Wu, W.J.; Chang, W.-C.; Juan, Y.-S. Protective effects of estrogen on ischemia/reperfusion–induced bladder dysfunction in female rabbits. Menopause 2013, 20, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Roy, J.; Galano, J.M.; Durand, T.; Le Guennec, J.Y.; Lee, J.C. Physiological role of reactive oxygen species as promoters of natural defenses. FASEB J. 2017, 31, 3729–3745. [Google Scholar] [CrossRef] [Green Version]
- Uchiyama, Y.; Suzuki, T.; Mochizuki, K.; Goda, T. Dietary supplementation with a low dose of (-)-epigallocatechin-3-gallate reduces pro-inflammatory responses in peripheral leukocytes of non-obese type 2 diabetic GK rats. J. Nutr. Sci. Vitam. 2013, 59, 541–547. [Google Scholar] [CrossRef] [Green Version]
- Juan, Y.-S.; Hydery, T.; Mannikarottu, A.; Kogan, B.; Schuler, C.; Leggett, R.E.; Lin, W.-Y.; Huang, C.-H.; Levin, R.M. Coenzyme Q10 protect against ischemia/reperfusion induced biochemical and functional changes in rabbit urinary bladder. Mol. Cell. Biochem. 2008, 311, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Jang, H.A.; Bae, J.H.; Lee, J.G. Effects of coenzyme Q10 on bladder dysfunction induced by chronic bladder ischemia in a rat model. J. Urol. 2013, 189, 2371–2376. [Google Scholar] [CrossRef] [PubMed]
- Juan, Y.-S.; Levin, R.M.; Chuang, S.M.; Hydery, T.; Li, S.; Kogan, B.; Schuler, C.; Mannikarottu, A.; Huang, C.-H. The Beneficial Effect of Coenzyme Q10 and Lipoic Acid on Obstructive Bladder Dysfunction in the Rabbit. J. Urol. 2008, 180, 2234–2240. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, S.; Hanai, T.; Shimizu, N.; Sugimoto, K.; Uemura, H. Effect of edaravone on ischemia/reperfusion injury in rat urinary bladder—Changes in smooth muscle cell phenotype and contractile function. Aktuelle Urol. 2010, 41 (Suppl. S1), S46–S49. [Google Scholar] [CrossRef]
- Kajiyama, S.; Hasegawa, G.; Asano, M.; Hosoda, H.; Fukui, M.; Nakamura, N.; Kitawaki, J.; Imai, S.; Nakano, K.; Ohta, M.; et al. Supplementation of hydrogen-rich water improves lipid and glucose metabolism in patients with type 2 diabetes or impaired glucose tolerance. Nutr. Res. 2008, 28, 137–143. [Google Scholar] [CrossRef]
- Chu, C.; Deng, J.; Man, Y.; Qu, Y. Green Tea Extracts Epigallocatechin-3-gallate for Different Treatments. Biomed. Res. Int. 2017, 2017, 5615647. [Google Scholar] [CrossRef] [Green Version]
- Miyata, Y.; ScienMatsuoces, T.; Araki, K.; Nakamura, Y.; Sagara, Y.; Ohba, K.; Sakai, H. Anticancer Effects of Green Tea and the Underlying Molecular Mechanisms in Bladder Cancer. Medicines 2018, 5, 87. [Google Scholar] [CrossRef] [Green Version]
- Miyata, Y.; Shida, Y.; Hakariya, T.; Sakai, H. Anti-Cancer Effects of Green Tea Polyphenols Against Prostate Cancer. Molecules 2019, 24, 193. [Google Scholar] [CrossRef] [Green Version]
- Xing, L.; Zhang, H.; Qi, R.; Tsao, R.; Mine, Y. Recent Advances in the Understanding of the Health Benefits and Molecular Mechanisms Associated with Green Tea Polyphenols. J. Agric. Food Chem. 2019, 67, 1029–1043. [Google Scholar] [CrossRef]
- Liu, Z.; Chen, R.; Jiang, Y.; Yang, Y.; He, L.; Luo, C.; Dong, J.; Rong, L. A meta-analysis of serum osteocalcin level in postmenopausal osteoporotic women compared to controls. BMC Musculoskelet. Disord. 2019, 20, 532–537. [Google Scholar] [CrossRef]
- Chung, J.E.; Kurisawa, M.; Kim, Y.J.; Uyama, H.; Kobayashi, S. Amplification of antioxidant activity of catechin by polycondensation with acetaldehyde. Biomacromolecules 2004, 5, 113–118. [Google Scholar] [CrossRef]
- Tipoe, G.L.; Leung, T.M.; Hung, M.W.; Fung, M.L. Green tea polyphenols as an anti-oxidant and anti-inflammatory agent for cardiovascular protection. Cardiovasc. Hematol. Disord. Drug Targets 2007, 7, 135–144. [Google Scholar] [CrossRef]
- Yuan, T.; Yang, T.; Chen, H.; Fu, D.; Hu, Y.; Wang, J.; Yuan, Q.; Yu, H.; Xu, W.; Xie, X. New insights into oxidative stress and inflammation during diabetes mellitus-accelerated atherosclerosis. Redox Biol. 2019, 20, 247–260. [Google Scholar] [CrossRef]
- Levites, Y.; Weinreb, O.; Maor, G.; Youdim, M.B.; Mandel, S. Green tea polyphenol (-)-epigallocatechin-3-gallate prevents N-methyl-4-phenyl-1,2,3,6-tetrahydropyridine-induced dopaminergic neurodegeneration. J. Neurochem. 2001, 78, 1073–1082. [Google Scholar] [CrossRef]
- Mandel, S.A.; Avramovich-Tirosh, Y.; Reznichenko, L.; Zheng, H.; Weinreb, O.; Amit, T.; Youdim, M.B. Multifunctional Activities of Green Tea Catechins in Neuroprotection. Neurosignals 2005, 14, 46–60. [Google Scholar] [CrossRef]
- Qanungo, S.; Das, M.; Haldar, S.; Basu, A. Epigallocatechin-3-gallate induces mitochondrial membrane depolarization and caspase-dependent apoptosis in pancreatic cancer cells. Carcinogenesis 2005, 26, 958–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coyle, C.H.; Philips, B.J.; Morrisroe, S.N.; Chancellor, M.B.; Yoshimura, N. Antioxidant effects of green tea and its polyphenols on bladder cells. Life Sci. 2008, 83, 12–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, Y.; Lee, K.H.; Park, J.H.; Geum, D.; Kim, K. Mitochondrial membrane depolarization and the selective death of dopaminergic neurons by rotenone: Protective effect of coenzyme Q10. J. Neurochem. 2005, 93, 1199–1208. [Google Scholar] [CrossRef]
- Mancuso, M.; Orsucci, D.; Volpi, L.; Calsolaro, V.; Siciliano, G. Coenzyme Q10 in neuromuscular and neurodegenerative disorders. Curr. Drug Targets 2010, 11, 111–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bubenik, G.A.; Blask, D.E.; Brown, G.M.; Maestroni, G.J.; Pang, S.F.; Reiter, R.J.; Viswanathan, M.; Zisapel, N. Prospects of the Clinical Utilization of Melatonin. Neurosignals 1998, 7, 195–219. [Google Scholar] [CrossRef]
- Tordjman, S.; Chokron, S.; Delorme, R.; Charrier, A.; Bellissant, E.; Jaafari, N.; Fougerou, C. Melatonin: Pharmacology, Functions and Therapeutic Benefits. Curr. Neuropharmacol. 2017, 15, 434–443. [Google Scholar] [CrossRef]
- Han, J.H.; Chang, I.H.; Myung, S.C.; Lee, M.Y.; Kim, W.Y.; Lee, S.Y.; Lee, S.Y.; Lee, S.W.; Kim, K.D. A Novel Pathway Underlying the Inhibitory Effects of Melatonin on Isolated Rat Urinary Bladder Contraction. Korean J. Physiol. Pharmacol. 2012, 16, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Semercioz, A.; Onur, R.; Ayar, A.; Orhan, I. The inhibitory role of melatonin on isolated guinea-pig urinary bladder: An endogenous hormone effect. BJU Int. 2004, 94, 1373–1376. [Google Scholar] [CrossRef]
- Shahidi, F.; Ambigaipalan, P. Omega-3 Polyunsaturated Fatty Acids and Their Health Benefits. Annu. Rev. Food Sci. Technol. 2018, 9, 345–381. [Google Scholar] [CrossRef]
- Farooqui, A.A. n-3 fatty acid-derived lipid mediators in the brain: New weapons against oxidative stress and inflammation. Curr. Med. Chem. 2012, 19, 532–543. [Google Scholar] [CrossRef]
- Jia, X.; Kohli, P.; Virani, S.S. Omega-3 Fatty Acid and Cardiovascular Outcomes: Insights from Recent Clinical Trials. Curr. Atheroscler. Rep. 2019, 21, 1. [Google Scholar] [CrossRef]
- Kobayashi, M.; Nomura, M.; Nishii, H.; Matsumoto, S.; Fujimoto, N.; Matsumoto, T. Effect of eviprostat on bladder overactivity in an experimental cystitis rat model. Int. J. Urol. 2008, 15, 356–360. [Google Scholar] [CrossRef]
- Kawai, Y.; Oka, M.; Kyotani, J.; Oyama, T.; Matsumoto, S.; Kakizaki, H. Effect of the phytotherapeutic agent eviprostat on the bladder in a rat model of bladder overdistension/emptying. Neurourol. Urodynamics 2013, 32, 1031–1037. [Google Scholar] [CrossRef]
- Ishigooka, M.; Hashimoto, T.; Hayami, S.; Tomaru, M.; Nakada, T.; Mitobe, K. Clinical and retrospective evaluation of eviprostat: A non-hormonal and non-neuropharmacological agent for benign prostatic hyperplasia. Int. Urol. Nephrol. 1995, 27, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Nasrin, S.; Masuda, E.; Kugaya, H.; Ito, Y.; Yamada, S. Improvement by phytotherapeutic agent of detrusor overactivity, down-regulation of pharmacological receptors and urinary cytokines in rats with cyclophosphamide induced cystitis. J. Urol. 2013, 189, 1123–1129. [Google Scholar] [CrossRef]
- Oka, M.; Tachibana, M.; Noda, K.; Inoue, N.; Tanaka, M.; Kuwabara, K. Relevance of anti-reactive oxygen species activity to anti-inflammatory activity of components of Eviprostat®, a phytotherapeutic agent for benign prostatic hyperplasia. Phytomedicine 2007, 14, 465–472. [Google Scholar] [CrossRef]
- Liu, C.; Wan, X.; Gu, M.; Chen, Y.; Cai, Z.; Zhou, J.; Chen, Q.; Wang, Z. Effect of Sulforaphane on Bladder Compliance in a Rat Model of Partial Bladder Outlet Obstruction. Oxidative Med. Cell. Longev. 2019, 2019, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.; Cui, W.; Xin, Y.; Miao, X.; Barati, M.T.; Zhang, C.; Chen, Q.; Tan, Y.; Cui, T.; Zheng, Y.; et al. Prevention by sulforaphane of diabetic cardiomyopathy is associated with up-regulation of Nrf2 expression and transcription activation. J. Mol. Cell. Cardiol. 2013, 57, 82–95. [Google Scholar] [CrossRef]
- Lin, C.-F.; Chueh, T.-H.; Chung, C.-H.; Chung, S.-D.; Chang, T.-C.; Chien, C.-T. Sulforaphane improves voiding function via the preserving mitochondrial function in diabetic rats. J. Formos. Med Assoc. 2020, 119, 1422–1430. [Google Scholar] [CrossRef]
- Tai, H.C.; Chung, S.D.; Chien, C.T.; Yu, H.J. Sulforaphane Improves Ischemia-Induced Detrusor Overactivity by Downregulating the Enhancement of Associated Endoplasmic Reticulum Stress, Autophagy, and Apoptosis in Rat Bladder. Sci. Rep. 2016, 6, 36110. [Google Scholar] [CrossRef]
- Iida, A.; Nosaka, N.; Yumoto, T.; Knaup, E.; Naito, H.; Nishiyama, C.; Yamakawa, Y.; Tsukahara, K.; Terado, M.; Sato, K.; et al. The Clinical Application of Hydrogen as a Medical Treatment. Acta Med. Okayama 2016, 70, 331–337. [Google Scholar]
- Ohsawa, I.; Ishikawa, M.; Takahashi, K.; Watanabe, M.; Nishimaki, K.; Yamagata, K.; Katsura, K.-I.; Katayama, Y.; Asoh, S.; Ohta, S. Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat. Med. 2007, 13, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, K.; Sano, M.; Ohsawa, I.; Shinmura, K.; Tamaki, K.; Kimura, K.; Endo, J.; Katayama, T.; Kawamura, A.; Kohsaka, S.; et al. Inhalation of hydrogen gas reduces infarct size in the rat model of myocardial ischemia–reperfusion injury. Biochem. Biophys. Res. Commun. 2008, 373, 30–35. [Google Scholar] [CrossRef]
- Ohta, S. Molecular hydrogen as a preventive and therapeutic medical gas: Initiation, development and potential of hydrogen medicine. Pharmacol. Ther. 2014, 144, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Fu, Y.; Ito, M.; Fujita, Y.; Ito, M.; Ichihara, M.; Masuda, A.; Suzuki, Y.; Maesawa, S.; Kajita, Y.; Hirayama, M.; et al. Molecular hydrogen is protective against 6-hydroxydopamine-induced nigrostriatal degeneration in a rat model of Parkinson’s disease. Neurosci. Lett. 2009, 453, 81–85. [Google Scholar] [CrossRef]
- Lin, W.-Y.; Hsieh, C.C.; Yang, T.-Y.; Chen, M.-L.; Huang, L.Y.; Lin, Y.-P.; Chang, P.-J.; Levin, R.M.; Wei, Y.-H. Transient Increase in Circulating Myeloid-Derived Suppressor Cells after Partial Bladder Outlet Obstruction. J. Urol. 2014, 192, 1569–1573. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.Y.; Lin, Y.P.; Levin, R.M.; Chen, M.L. The relevance of immune responses to partial bladder outlet obstruction and reversal. Neurourol. Urodyn. 2017, 36, 1306–1312. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Biomarkers | Species | Changes | Sample | Animal Model | References | |
|---|---|---|---|---|---|---|
| DNA base oxidation | ||||||
| 8-OHdG | Rat | Increased | Urine | PBOO | [47] | |
| Rabbit | Increased | Urine | PBOO | [47,48,49] | ||
| Human | Increased | Urine | OAB | [50] | ||
| Rabbit | Increased | Urine Plasma | PBOO | [51] | ||
| Rabbit | Increased | Urine Plasma | PBOO | [48] | ||
| Rat | Increased | Urine Bladder tissue | BOO | [52] | ||
| Lipid peroxidation | ||||||
| MDA | Rabbit | Increased | Plasma | PBOO | [51] | |
| Rabbit | Increased | Plasma | PBOO | [48] | ||
| Human Women | Increased | Plasma | OAB | [50] [53] | ||
| Rat | Increased | Serum | BOO | [54] | ||
| Rat | Increased | Plasma Bladder tissue | PBOO | [55] | ||
| Rat | Increased | Bladder tissue | I/R | [56] | ||
| Rabbit | Increased | Bladder tissue | PBOO | [57] | ||
| Rat | Increased | Bladder tissue | PBOO | [47] | ||
| Rat | No change | Serum Bladder tissue | PBOO | [58] | ||
| Rat | Increased | Bladder tissue | PBOO | [52] | ||
| Rat | Increased | Bladder tissue | PBOO | [59] | ||
| Rat | Increased | Bladder tissue | BOO | [60] | ||
| Rat | Increased | Bladder tissue | PBOO | [61] | ||
| F2-IsoP | Mouse | No change | Bladder tissue | PBOO | [62] | |
| Mouse | Increased | Bladder tissue | PBOO | [63] | ||
| Antioxidant | Model | Species | Sample | Changes in Oxidative Biomarkers | Changes in Antioxidants | References |
|---|---|---|---|---|---|---|
| EGCG | PBOO | Rat | Bladder tissue | MDA↓ | CAT↑ tSOD↑ GSH-Px↑ | [61] |
| Type 2 diabetes | Rat | leukocytes | 8-OHdG↓ MDA↓ | – | [110] | |
| CoQ10 | I/R | Rabbit | Bladder tissue | - | CAT↑ SOD↑ | [111] |
| I/R | Rat | Bladder tissue | MDA↓ | – | [112] | |
| PBOO | Rabbit | Bladder tissue | NT↓ DNP↓ | – | [113] | |
| Melatonin | I/R | Rat | Bladder tissue | MDA↓ MPO↓ | GSH↑ | [56] |
| PBOO | Rabbit | Bladder tissue | MDA↓ | CAT↑ SOD↑ GSH↑ | [57] | |
| Omega-3 fatty acid | PBOO PBOO | Rat Rat | Bladder tissue | MDA↑ NO↑ | SOD↓ | [58] |
| Serum | MDA↓ NO↓ | SOD↓ GSH↓ | [58] | |||
| Eviprostat | PBOO | Rat | Urine | 8-OHdG↓ | – | [47,49] |
| Bladder tissue | MDA↓ | – | [47] | |||
| I/R | Rat | Urine | 8-OHdG↓ | – | [64] | |
| Bladder tissue | MDA↓ | – | [64] | |||
| I/R | Rat | Urine | 8-OHdG↓ | – | [114] | |
| Hydrogen water | PBOO | Rat | Urine bladder tissue | 8-OHdG↓ MDA↓ | – | [115] |
| PBOO | Rat | Urine | 8-OHdG↓ | – | [52] | |
| Bladder tissue | 8-OHdG↓ MDA↓ | – | [52] | |||
| Sulforaphane | PBOO | Rat | Bladder tissue | MDA↓ | CAT↑ SOD↑ GSH↑ | [55] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Y.-H.; Chueh, K.-S.; Chuang, S.-M.; Long, C.-Y.; Lu, J.-H.; Juan, Y.-S. Bladder Hyperactivity Induced by Oxidative Stress and Bladder Ischemia: A Review of Treatment Strategies with Antioxidants. Int. J. Mol. Sci. 2021, 22, 6014. https://doi.org/10.3390/ijms22116014
Wu Y-H, Chueh K-S, Chuang S-M, Long C-Y, Lu J-H, Juan Y-S. Bladder Hyperactivity Induced by Oxidative Stress and Bladder Ischemia: A Review of Treatment Strategies with Antioxidants. International Journal of Molecular Sciences. 2021; 22(11):6014. https://doi.org/10.3390/ijms22116014
Chicago/Turabian StyleWu, Yi-Hsuan, Kuang-Shun Chueh, Shu-Mien Chuang, Cheng-Yu Long, Jian-He Lu, and Yung-Shun Juan. 2021. "Bladder Hyperactivity Induced by Oxidative Stress and Bladder Ischemia: A Review of Treatment Strategies with Antioxidants" International Journal of Molecular Sciences 22, no. 11: 6014. https://doi.org/10.3390/ijms22116014