
Management of Cirrhotic Ascites under the Add-on Administration of Tolvaptan

Abstract
:1. Introduction
2. Methods
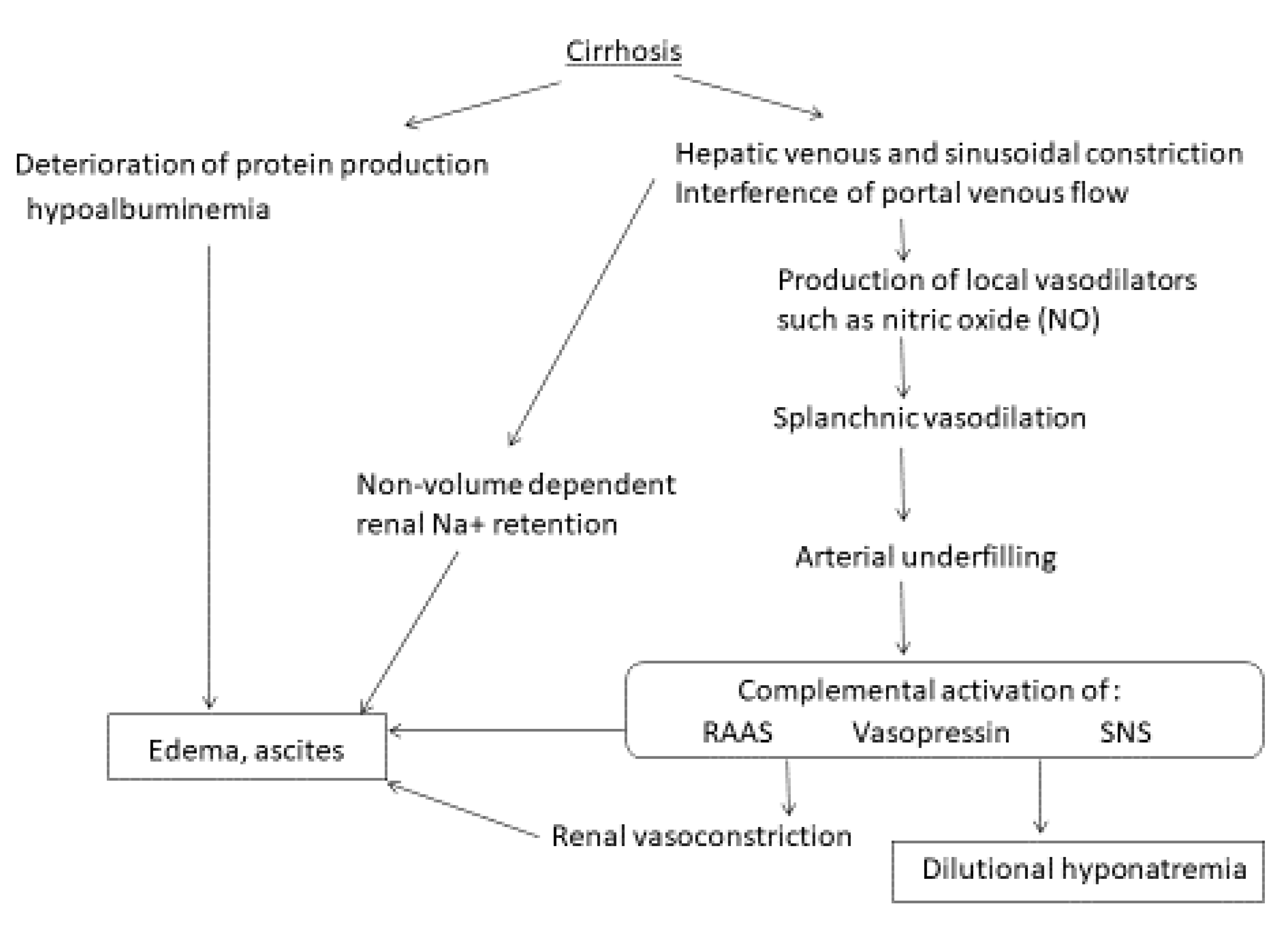
3. The Mechanisms of Ascites in Cirrhosis
4. Management of Ascites
4.1. Ascites Management with Spironolactone and Furosemide
4.2. Ascites Management with AVP Targeting Agents
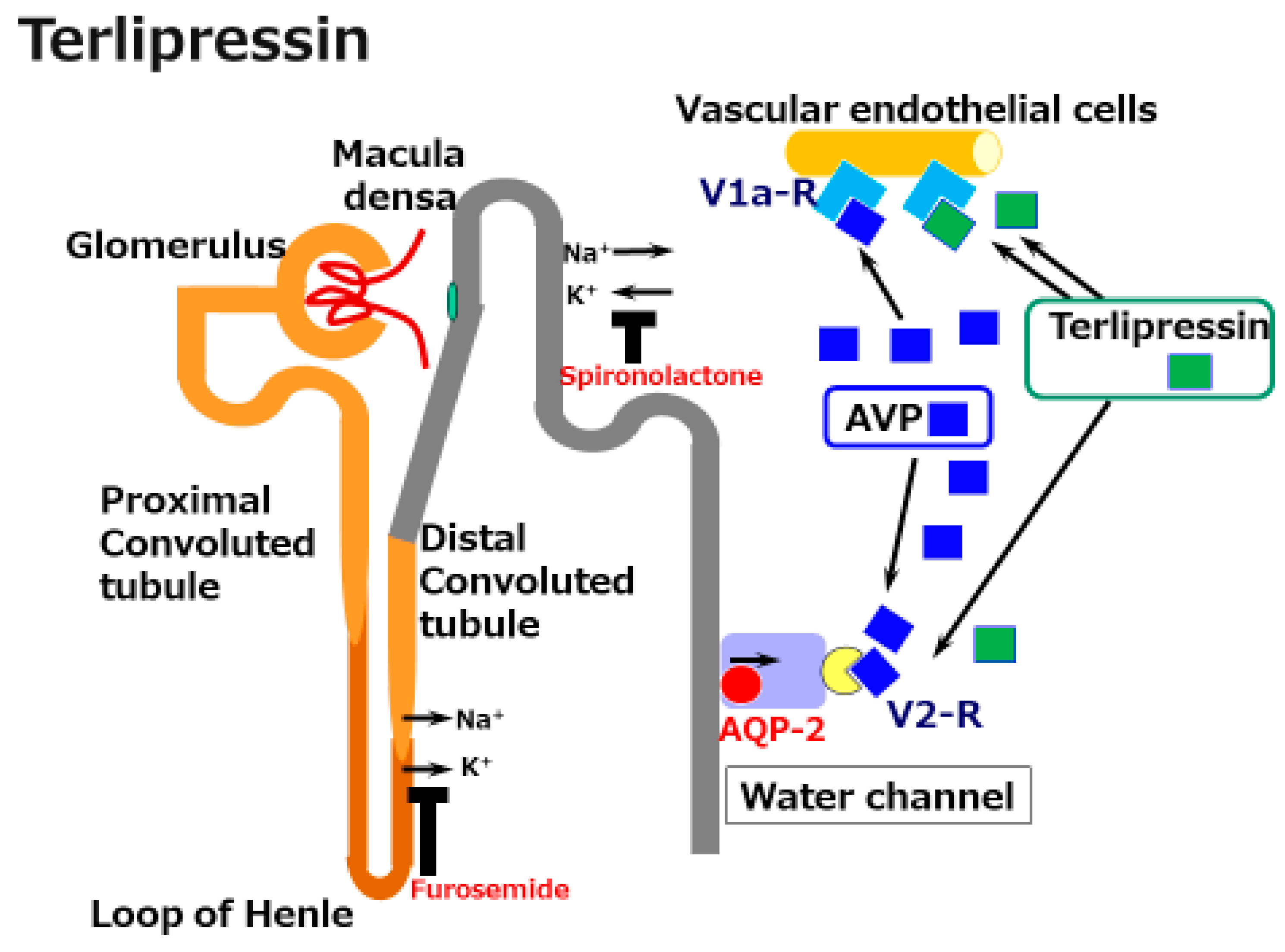
4.2.1. Terlipressin
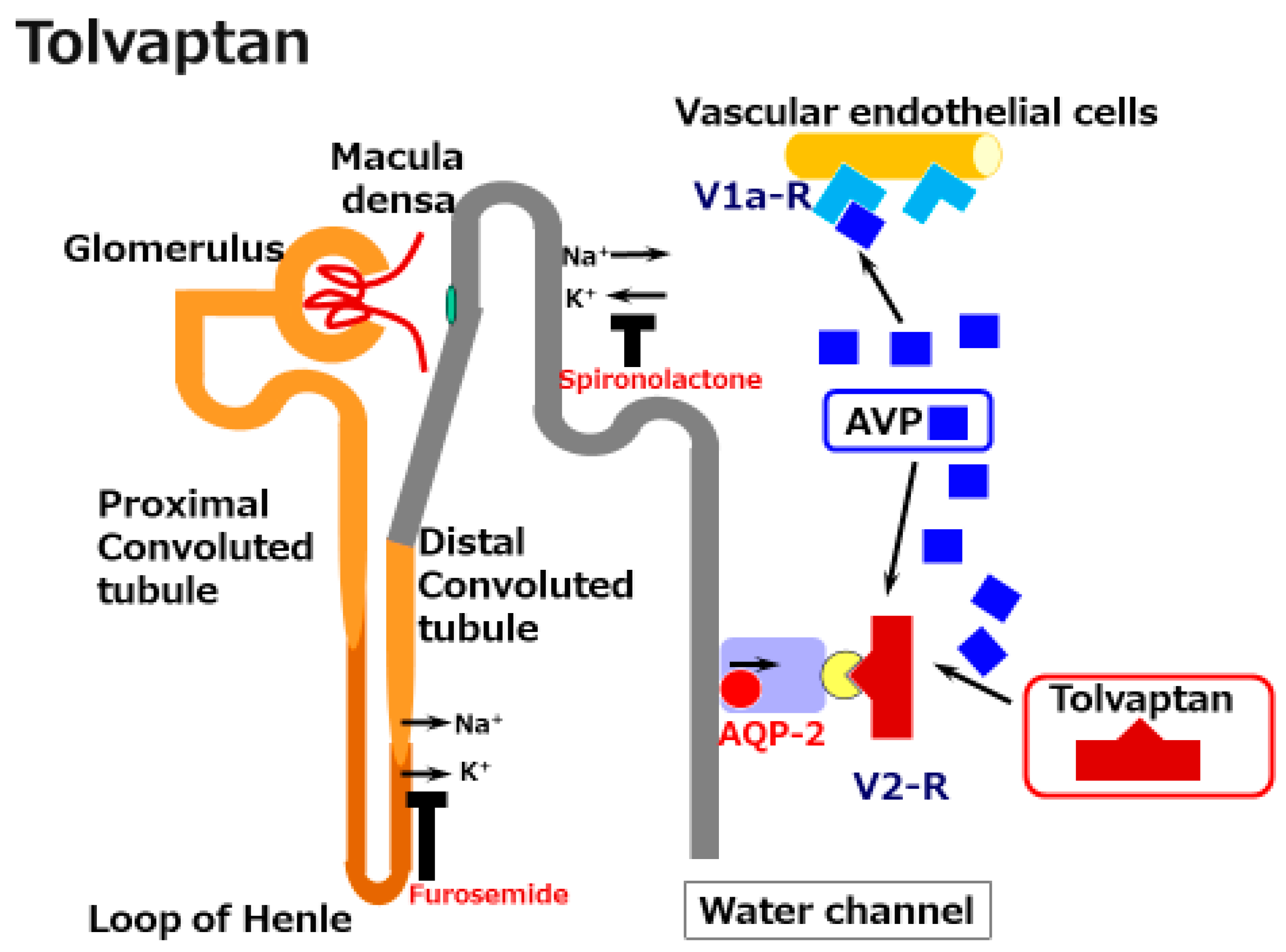
4.2.2. Tolvaptan
The Mechanisms of Tolvaptan
The Clinical Efficacy of Tolvaptan in Cirrhosis
Long-Term Survival after Tolvaptan Administration
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Enomoto, H.; Ueno, Y.; Hiasa, Y.; Nishikawa, H.; Hige, S.; Takikawa, Y.; Taniai, M.; Ishikawa, T.; Yasui, K.; Takaki, A.; et al. Transition in the etiology of liver cirrhosis in Japan: A nationwide survey. J. Gastroenterol. 2020, 55, 353–362. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenner, B.M.; Rector, F.C. Brenner & Rector’s the Kidney, 8th ed.; Saunders Elsevier: Philadelphia, PA, USA, 2008. [Google Scholar]
- Papaluca, T.; Gow, P. Terlipressin: Current and emerging indications in chronic liver disease. J. Gastroenterol. Hepatol. 2018, 33, 591–598. [Google Scholar] [CrossRef]
- Sakaida, I. Tolvaptan for the treatment of liver cirrhosis oedema. Expert Rev. Gastroenterol. Hepatol. 2014, 8, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Brunzel, N.A. Fundamentals of Urine and Body Fluid Analysis, 4th ed.; Elsevier: St. Louis, MO, USA, 2018; Chapter 4. [Google Scholar]
- Durand, F.; Graupera, I.; Gines, P.; Olson, J.C.; Nadim, M.K. Pathogenesis of Hepatorenal Syndrome: Implications for Therapy. Am. J. Kidney Dis. 2016, 67, 318–328. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J. Hepatol. 2010, 53, 397–417. [Google Scholar] [CrossRef] [PubMed]
- Aithal, G.P.; Palaniyappan, N.; China, L.; Harmala, S.; Macken, L.; Ryan, J.M.; Wilkes, E.A.; Moore, K.; Leithead, J.A.; Hayes, P.C.; et al. Guidelines on the management of ascites in cirrhosis. Gut 2021, 70, 9–29. [Google Scholar] [CrossRef]
- Fernandez, M. Molecular pathophysiology of portal hypertension. Hepatology 2015, 61, 1406–1415. [Google Scholar] [CrossRef]
- Skorecki, K.; Chertow, G.M.; Marsden, P.A.; Taal, M.W.; Yu, A.S.L. Brenner & Rector’s the Kidney, 10th ed.; Elsevier: Philadelphia, PA, USA, 2016; Chapter 15. [Google Scholar]
- Hocher, B.; Heiden, S.; von Websky, K.; Arafat, A.M.; Rahnenfuhrer, J.; Alter, M.; Kalk, P.; Ziegler, D.; Fischer, Y.; Pfab, T. Renal effects of the novel selective adenosine A1 receptor blocker SLV329 in experimental liver cirrhosis in rats. PLoS ONE 2011, 6, e17891. [Google Scholar] [CrossRef] [Green Version]
- Ross, E.A. Congestive renal failure: The pathophysiology and treatment of renal venous hypertension. J. Card. Fail. 2012, 18, 930–938. [Google Scholar] [CrossRef]
- Kuiper, J.J.; de Man, R.A.; van Buuren, H.R. Review article: Management of ascites and associated complications in patients with cirrhosis. Aliment. Pharmacol. Ther. 2007, 26 (Suppl. S2), 183–193. [Google Scholar] [CrossRef] [PubMed]
- Bataller, R.; Sancho-Bru, P.; Gines, P.; Lora, J.M.; Al-Garawi, A.; Sole, M.; Colmenero, J.; Nicolas, J.M.; Jimenez, W.; Weich, N.; et al. Activated human hepatic stellate cells express the renin-angiotensin system and synthesize angiotensin II. Gastroenterology 2003, 125, 117–125. [Google Scholar] [CrossRef]
- Jonsson, J.R.; Clouston, A.D.; Ando, Y.; Kelemen, L.I.; Horn, M.J.; Adamson, M.D.; Purdie, D.M.; Powell, E.E. Angiotensin-converting enzyme inhibition attenuates the progression of rat hepatic fibrosis. Gastroenterology 2001, 121, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.Y.; Cho, M.Y.; Baik, S.K.; Jeong, P.H.; Suk, K.T.; Jang, Y.O.; Yea, C.J.; Kim, J.W.; Kim, H.S.; Kwon, S.O.; et al. Beneficial effects of candesartan, an angiotensin-blocking agent, on compensated alcoholic liver fibrosis—A randomized open-label controlled study. Liver Int. 2012, 32, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Yoon, K.T.; Liu, H.; Lee, S.S. Cirrhotic Cardiomyopathy. Curr. Gastroenterol. Rep. 2020, 22, 45. [Google Scholar] [CrossRef]
- Shenoda, B.; Boselli, J. Vascular syndromes in liver cirrhosis. Clin. J. Gastroenterol. 2019, 12, 387–397. [Google Scholar] [CrossRef]
- Fukui, H.; Saito, H.; Ueno, Y.; Uto, H.; Obara, K.; Sakaida, I.; Shibuya, A.; Seike, M.; Nagoshi, S.; Segawa, M.; et al. Evidence-based clinical practice guidelines for liver cirrhosis 2015. J. Gastroenterol. 2016, 51, 629–650. [Google Scholar] [CrossRef] [Green Version]
- Gu, X.B.; Yang, X.J.; Zhu, H.Y.; Xu, B.Y. Effect of a diet with unrestricted sodium on ascites in patients with hepatic cirrhosis. Gut Liver 2012, 6, 355–361. [Google Scholar] [CrossRef] [Green Version]
- Morando, F.; Rosi, S.; Gola, E.; Nardi, M.; Piano, S.; Fasolato, S.; Stanco, M.; Cavallin, M.; Romano, A.; Sticca, A.; et al. Adherence to a moderate sodium restriction diet in outpatients with cirrhosis and ascites: A real-life cross-sectional study. Liver Int. 2015, 35, 1508–1515. [Google Scholar] [CrossRef]
- Bernardi, M.; Servadei, D.; Trevisani, F.; Rusticali, A.G.; Gasbarrini, G. Importance of plasma aldosterone concentration on the natriuretic effect of spironolactone in patients with liver cirrhosis and ascites. Digestion 1985, 31, 189–193. [Google Scholar] [CrossRef]
- Perez-Ayuso, R.M.; Arroyo, V.; Planas, R.; Gaya, J.; Bory, F.; Rimola, A.; Rivera, F.; Rodes, J. Randomized comparative study of efficacy of furosemide versus spironolactone in nonazotemic cirrhosis with ascites. Relationship between the diuretic response and the activity of the renin-aldosterone system. Gastroenterology 1983, 84, 961–968. [Google Scholar] [CrossRef]
- Attar, B. Approach to Hyponatremia in Cirrhosis. Clin. Liver Dis. 2019, 13, 98–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordoba, J.; Ventura-Cots, M.; Simon-Talero, M.; Amoros, A.; Pavesi, M.; Vilstrup, H.; Angeli, P.; Domenicali, M.; Gines, P.; Bernardi, M.; et al. Characteristics, risk factors, and mortality of cirrhotic patients hospitalized for hepatic encephalopathy with and without acute-on-chronic liver failure (ACLF). J. Hepatol. 2014, 60, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Decaux, G.; Soupart, A.; Vassart, G. Non-peptide arginine-vasopressin antagonists: The vaptans. Lancet 2008, 371, 1624–1632. [Google Scholar] [CrossRef]
- Yoshimura, M.; Conway-Campbell, B.; Ueta, Y. Arginine vasopressin: Direct and indirect action on metabolism. Peptides 2021, 142, 170555. [Google Scholar] [CrossRef]
- Gines, P.; Guevara, M. Hyponatremia in cirrhosis: Pathogenesis, clinical significance, and management. Hepatology 2008, 48, 1002–1010. [Google Scholar] [CrossRef]
- Bichet, D.; Szatalowicz, V.; Chaimovitz, C.; Schrier, R.W. Role of vasopressin in abnormal water excretion in cirrhotic patients. Ann. Intern. Med. 1982, 96, 413–417. [Google Scholar] [CrossRef] [PubMed]
- Bichet, D.G.; Groves, B.M.; Schrier, R.W. Mechanisms of improvement of water and sodium excretion by immersion in decompensated cirrhotic patients. Kidney Int. 1983, 24, 788–794. [Google Scholar] [CrossRef] [Green Version]
- Jamil, K.; Pappas, S.C.; Devarakonda, K.R. In vitro binding and receptor-mediated activity of terlipressin at vasopressin receptors V1 and V2. J. Exp. Pharmacol. 2018, 10, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salerno, F.; Gerbes, A.; Gines, P.; Wong, F.; Arroyo, V. Diagnosis, prevention and treatment of hepatorenal syndrome in cirrhosis. Gut 2007, 56, 1310–1318. [Google Scholar] [CrossRef] [Green Version]
- Angeli, P.; Garcia-Tsao, G.; Nadim, M.K.; Parikh, C.R. News in pathophysiology, definition and classification of hepatorenal syndrome: A step beyond the International Club of Ascites (ICA) consensus document. J. Hepatol. 2019, 71, 811–822. [Google Scholar] [CrossRef] [Green Version]
- Fasolato, S.; Angeli, P.; Dallagnese, L.; Maresio, G.; Zola, E.; Mazza, E.; Salinas, F.; Dona, S.; Fagiuoli, S.; Sticca, A.; et al. Renal failure and bacterial infections in patients with cirrhosis: Epidemiology and clinical features. Hepatology 2007, 45, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Gines, A.; Fernandez-Esparrach, G.; Monescillo, A.; Vila, C.; Domenech, E.; Abecasis, R.; Angeli, P.; Ruiz-Del-Arbol, L.; Planas, R.; Sola, R.; et al. Randomized trial comparing albumin, dextran 70, and polygeline in cirrhotic patients with ascites treated by paracentesis. Gastroenterology 1996, 111, 1002–1010. [Google Scholar] [CrossRef]
- Akriviadis, E.; Botla, R.; Briggs, W.; Han, S.; Reynolds, T.; Shakil, O. Pentoxifylline improves short-term survival in severe acute alcoholic hepatitis: A double-blind, placebo-controlled trial. Gastroenterology 2000, 119, 1637–1648. [Google Scholar] [CrossRef] [Green Version]
- Boyer, T.D.; Sanyal, A.J.; Wong, F.; Frederick, R.T.; Lake, J.R.; O’Leary, J.G.; Ganger, D.; Jamil, K.; Pappas, S.C.; Investigators REVERSE Study. Terlipressin Plus Albumin Is More Effective Than Albumin Alone in Improving Renal Function in Patients With Cirrhosis and Hepatorenal Syndrome Type 1. Gastroenterology 2016, 150, 1579–1589.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, F.; Pappas, S.C.; Curry, M.P.; Reddy, K.R.; Rubin, R.A.; Porayko, M.K.; Gonzalez, S.A.; Mumtaz, K.; Lim, N.; Simonetto, D.A.; et al. Terlipressin plus Albumin for the Treatment of Type 1 Hepatorenal Syndrome. N. Engl. J. Med. 2021, 384, 818–828. [Google Scholar] [CrossRef] [PubMed]
- Gheorghiade, M.; Niazi, I.; Ouyang, J.; Czerwiec, F.; Kambayashi, J.; Zampino, M.; Orlandi, C.; Tolvaptan, I. Vasopressin V2-receptor blockade with tolvaptan in patients with chronic heart failure: Results from a double-blind, randomized trial. Circulation 2003, 107, 2690–2696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, V.E.; Chapman, A.B.; Devuyst, O.; Gansevoort, R.T.; Grantham, J.J.; Higashihara, E.; Perrone, R.D.; Krasa, H.B.; Ouyang, J.; Czerwiec, F.S.; et al. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N. Engl. J. Med. 2012, 367, 2407–2418. [Google Scholar] [CrossRef] [Green Version]
- Torres, V.E.; Chapman, A.B.; Devuyst, O.; Gansevoort, R.T.; Perrone, R.D.; Koch, G.; Ouyang, J.; McQuade, R.D.; Blais, J.D.; Czerwiec, F.S.; et al. Tolvaptan in Later-Stage Autosomal Dominant Polycystic Kidney Disease. N. Engl. J. Med. 2017, 377, 1930–1942. [Google Scholar] [CrossRef]
- Bellos, I.; Kontzoglou, K.; Psyrri, A.; Pergialiotis, V. Tolvaptan Response Improves Overall Survival in Patients with Refractory Ascites: A Meta-Analysis. Dig. Dis. 2020, 38, 320–328. [Google Scholar] [CrossRef]
- Yamamura, Y.; Ogawa, H.; Yamashita, H.; Chihara, T.; Miyamoto, H.; Nakamura, S.; Onogawa, T.; Yamashita, T.; Hosokawa, T.; Mori, T.; et al. Characterization of a novel aquaretic agent, OPC-31260, as an orally effective, nonpeptide vasopressin V2 receptor antagonist. Br. J. Pharmacol. 1992, 105, 787–791. [Google Scholar] [CrossRef] [Green Version]
- Yamamura, Y.; Nakamura, S.; Itoh, S.; Hirano, T.; Onogawa, T.; Yamashita, T.; Yamada, Y.; Tsujimae, K.; Aoyama, M.; Kotosai, K.; et al. OPC-41061, a highly potent human vasopressin V2-receptor antagonist: Pharmacological profile and aquaretic effect by single and multiple oral dosing in rats. J. Pharmacol. Exp. Ther. 1998, 287, 860–867. [Google Scholar]
- Doggrell, S.A. Tolvaptan (Otsuka). Curr. Opin. Investig. Drugs 2004, 5, 977–983. [Google Scholar]
- Fujiki, T.; Ando, F.; Murakami, K.; Isobe, K.; Mori, T.; Susa, K.; Nomura, N.; Sohara, E.; Rai, T.; Uchida, S. Tolvaptan activates the Nrf2/HO-1 antioxidant pathway through PERK phosphorylation. Sci. Rep. 2019, 9, 9245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Natarajan, S.K.; Basivireddy, J.; Ramachandran, A.; Thomas, S.; Ramamoorthy, P.; Pulimood, A.B.; Jacob, M.; Balasubramanian, K.A. Renal damage in experimentally-induced cirrhosis in rats: Role of oxygen free radicals. Hepatology 2006, 43, 1248–1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakaida, I.; Kawazoe, S.; Kajimura, K.; Saito, T.; Okuse, C.; Takaguchi, K.; Okada, M.; Okita, K.; Group, A.-D.S. Tolvaptan for improvement of hepatic edema: A phase 3, multicenter, randomized, double-blind, placebo-controlled trial. Hepatol. Res. 2014, 44, 73–82. [Google Scholar] [CrossRef]
- Okita, K.; Kawazoe, S.; Hasebe, C.; Kajimura, K.; Kaneko, A.; Okada, M.; Sakaida, I.; ASCITES Dose-Finding Trial Group. Dose-finding trial of tolvaptan in liver cirrhosis patients with hepatic edema: A randomized, double-blind, placebo-controlled trial. Hepatol. Res. 2014, 44, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Wang, Y.; Han, T.; Mao, Q.; Cheng, J.; Ding, H.; Shang, J.; Zhang, Q.; Niu, J.; Ji, F.; et al. Tolvaptan therapy of Chinese cirrhotic patients with ascites after insufficient diuretic routine medication responses: A phase III clinical trial. BMC Gastroenterol. 2020, 20, 391. [Google Scholar] [CrossRef] [PubMed]
- Hiramine, Y.; Uojima, H.; Nakanishi, H.; Hiramatsu, A.; Iwamoto, T.; Kimura, M.; Kawaratani, H.; Terai, S.; Yoshiji, H.; Uto, H.; et al. Response criteria of tolvaptan for the treatment of hepatic edema. J. Gastroenterol. 2018, 53, 258–268. [Google Scholar] [CrossRef]
- Sakaida, I.; Terai, S.; Kurosaki, M.; Yasuda, M.; Okada, M.; Bando, K.; Fukuta, Y. Effectiveness and safety of tolvaptan in liver cirrhosis patients with edema: Interim results of post-marketing surveillance of tolvaptan in liver cirrhosis (START study). Hepatol. Res. 2017, 47, 1137–1146. [Google Scholar] [CrossRef]
- Hiramine, Y.; Uto, H.; Imamura, Y.; Hiwaki, T.; Kure, T.; Ijuin, S.; Oda, K.; Mawatari, S.; Kumagai, K.; Tokunaga, K.; et al. Efficacy of vasopressin V2 receptor antagonist tolvaptan in treatment of hepatic edema. Hepatol. Res. 2017, 47, 542–557. [Google Scholar] [CrossRef]
- Chishina, H.; Hagiwara, S.; Nishida, N.; Ueshima, K.; Sakurai, T.; Ida, H.; Minami, Y.; Takita, M.; Kono, M.; Minami, T.; et al. Clinical Factors Predicting the Effect of Tolvaptan for Refractory Ascites in Patients with Decompensated Liver Cirrhosis. Dig. Dis. 2016, 34, 659–664. [Google Scholar] [CrossRef]
- Iwamoto, T.; Maeda, M.; Hisanaga, T.; Saeki, I.; Fujisawa, K.; Matsumoto, T.; Hidaka, I.; Ishikawa, T.; Takami, T.; Sakaida, I. Predictors of the Effect of Tolvaptan on the Prognosis of Cirrhosis. Intern. Med. 2016, 55, 2911–2916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adachi, T.; Takaki, A.; Sato, S.; Tobita, H.; Kobashi, H.; Kinomura, M.; Nakatsuka, A.; Oyama, A.; Wada, N.; Sakata, M.; et al. High expression of a vascular stricture-related marker is predictive of an early response to tolvaptan, and a low fractional excretion of sodium is predictive of a poor long-term survival after tolvaptan administration for liver cirrhosis. Hepatol. Res. 2020, 50, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Arase, Y.; Kagawa, T.; Tsuruya, K.; Sato, H.; Teramura, E.; Anzai, K.; Hirose, S.; Deguchi, R.; Shiraishi, K.; Mine, T. Impaired Renal Function May Not Negate the Efficacy of Tolvaptan in the Treatment of Cirrhotic Patients with Refractory Ascites. Clin. Drug Investig. 2019, 39, 45–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakaida, I.; Terai, S.; Kurosaki, M.; Okada, M.; Hirano, T.; Fukuta, Y. Real-world effectiveness and safety of tolvaptan in liver cirrhosis patients with hepatic edema: Results from a post-marketing surveillance study (START study). J. Gastroenterol. 2020, 55, 800–810. [Google Scholar] [CrossRef]
- Kawaratani, H.; Fukui, H.; Moriya, K.; Noguchi, R.; Namisaki, T.; Uejima, M.; Kitade, M.; Takeda, K.; Okura, Y.; Kaji, K.; et al. Predictive parameter of tolvaptan effectiveness in cirrhotic ascites. Hepatol. Res. 2017, 47, 854–861. [Google Scholar] [CrossRef]
- Hayashi, M.; Abe, K.; Fujita, M.; Okai, K.; Takahashi, A.; Ohira, H. Association between the Serum Sodium Levels and the Response to Tolvaptan in Liver Cirrhosis Patients with Ascites and Hyponatremia. Intern. Med. 2018, 57, 2451–2458. [Google Scholar] [CrossRef] [Green Version]
- Planas, R.; Montoliu, S.; Balleste, B.; Rivera, M.; Miquel, M.; Masnou, H.; Galeras, J.A.; Gimenez, M.D.; Santos, J.; Cirera, I.; et al. Natural history of patients hospitalized for management of cirrhotic ascites. Clin. Gastroenterol. Hepatol. 2006, 4, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, A.; Atsukawa, M.; Tsubota, A.; Kondo, C.; Okubo, T.; Arai, T.; Itokawa, N.; Narahara, Y.; Iwakiri, K. Usefulness of portal vein pressure for predicting the effects of tolvaptan in cirrhotic patients. World J. Gastroenterol. 2016, 22, 5104–5113. [Google Scholar] [CrossRef]
- Komiyama, Y.; Kurosaki, M.; Nakanishi, H.; Takahashi, Y.; Itakura, J.; Yasui, Y.; Tamaki, N.; Takada, H.; Higuchi, M.; Gotou, T.; et al. Prediction of diuretic response to tolvaptan by a simple, readily available spot urine Na/K ratio. PLoS ONE 2017, 12, e0174649. [Google Scholar] [CrossRef]
- Runyon, B.A. Management of adult patients with ascites due to cirrhosis: An update. Hepatology 2009, 49, 2087–2107. [Google Scholar] [CrossRef]
- Cholongitas, E.; Karatapanis, S.; Nakouti, T.; Birtsou, C.; Skorda, L.; Kouvelis, I.; Papastergiou, V.; Papachrysos, N.; Goulis, J.; Akriviadis, E. Can 24-h urine sodium excretion be replaced by spot urine sodium/potassium in patients with decompensated cirrhosis? Liver Int. 2012, 32, 172–173. [Google Scholar] [CrossRef] [PubMed]
- El Mohii, S.M.; El Mansy, I.M.; Salah, M.; Khedr, M.A. Diagnostic usefulness of the random urine Na/K ratio in predicting therapeutic response for diuretics in cirrhotic patients with ascites. J. Egypt Soc. Parasitol. 2013, 43, 767–776. [Google Scholar]
- Kogiso, T.; Yamamoto, K.; Kobayashi, M.; Ikarashi, Y.; Kodama, K.; Taniai, M.; Torii, N.; Hashimoto, E.; Tokushige, K. Response to tolvaptan and its effect on prognosis in cirrhotic patients with ascites. Hepatol. Res. 2017, 47, 835–844. [Google Scholar] [CrossRef] [PubMed]
- Memon, L.; Spasojevic-Kalimanovska, V.; Bogavac-Stanojevic, N.; Kotur-Stevuljevic, J.; Simic-Ogrizovic, S.; Giga, V.; Dopsaj, V.; Jelic-Ivanovic, Z.; Spasic, S. Assessment of endothelial dysfunction: The role of symmetrical dimethylarginine and proinflammatory markers in chronic kidney disease and renal transplant recipients. Dis. Markers 2013, 35, 173–180. [Google Scholar] [CrossRef]
- Janes, F.; Cifu, A.; Pessa, M.E.; Domenis, R.; Gigli, G.L.; Sanvilli, N.; Nilo, A.; Garbo, R.; Curcio, F.; Giacomello, R.; et al. ADMA as a possible marker of endothelial damage. A study in young asymptomatic patients with cerebral small vessel disease. Sci. Rep. 2019, 9, 14207. [Google Scholar] [CrossRef]
- Sibal, L.; Agarwal, S.C.; Home, P.D.; Boger, R.H. The Role of Asymmetric Dimethylarginine (ADMA) in Endothelial Dysfunction and Cardiovascular Disease. Curr. Cardiol. Rev. 2010, 6, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Stuhlinger, M.C.; Tsao, P.S.; Her, J.H.; Kimoto, M.; Balint, R.F.; Cooke, J.P. Homocysteine impairs the nitric oxide synthase pathway: Role of asymmetric dimethylarginine. Circulation 2001, 104, 2569–2575. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, T.; Maeda, M.; Saeki, I.; Hidaka, I.; Tajima, K.; Ishikawa, T.; Takami, T.; Sakaida, I. Analysis of tolvaptan non-responders and outcomes of tolvaptan treatment of ascites. J. Gastroenterol. Hepatol. 2019, 34, 1231–1235. [Google Scholar] [CrossRef] [PubMed]
- Yatsuhashi, H.; Sano, H.; Hirano, T.; Shibasaki, Y. Real-world hospital mortality of liver cirrhosis inpatients in Japan: A large-scale cohort study using a medical claims database: Prognosis of liver cirrhosis. Hepatol. Res. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Atsukawa, M.; Tsubota, A.; Takaguchi, K.; Toyoda, H.; Iwasa, M.; Ikegami, T.; Chuma, M.; Nozaki, A.; Uojima, H.; Hiraoka, A.; et al. Analysis of factors associated with the prognosis of cirrhotic patients who were treated with tolvaptan for hepatic edema. J. Gastroenterol. Hepatol. 2019, 35, 1229–1237. [Google Scholar] [CrossRef]
- Kida, Y. Positive Response to Tolvaptan Treatment Would Be a Good Prognostic Factor for Cirrhotic Patients with Ascites. Dig. Dis. 2019, 37, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Namba, M.; Hiramatsu, A.; Aikata, H.; Kodama, K.; Uchikawa, S.; Ohya, K.; Morio, K.; Fujino, H.; Nakahara, T.; Murakami, E.; et al. Management of refractory ascites attenuates muscle mass reduction and improves survival in patients with decompensated cirrhosis. J. Gastroenterol. 2020, 55, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Tahara, T.; Mori, K.; Mochizuki, M.; Ishiyama, R.; Noda, M.; Hoshi, H.; Lefor, A.K.; Shinozaki, S. Tolvaptan is effective in treating patients with refractory ascites due to cirrhosis. Biomed. Rep. 2017, 7, 558–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Londono, M.C.; Cardenas, A.; Guevara, M.; Quinto, L.; de las Heras, D.; Navasa, M.; Rimola, A.; Garcia-Valdecasas, J.C.; Arroyo, V.; Gines, P. MELD score and serum sodium in the prediction of survival of patients with cirrhosis awaiting liver transplantation. Gut 2007, 56, 1283–1290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanayama, K.; Chiba, T.; Kobayashi, K.; Koroki, K.; Maruta, S.; Kanzaki, H.; Kusakabe, Y.; Saito, T.; Kiyono, S.; Nakamura, M.; et al. Long-term administration of Tolvaptan to patients with decompensated cirrhosis. Int. J. Med. Sci. 2020, 17, 874–880. [Google Scholar] [CrossRef] [Green Version]
- Shiba, S.; Chu, P.S.; Nakamoto, N.; Yamataka, K.; Taniki, N.; Ojiro, K.; Yamaguchi, A.; Morikawa, R.; Yoshida, A.; Ikura, A.; et al. Clinical implications with tolvaptan on monitored bioimpedance-defined fluid status in patients with cirrhotic ascites: An observational study. BMC Gastroenterol. 2020, 20, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohashi, N.; Tsuji, N.; Naito, Y.; Iwakura, T.; Isobe, S.; Ono, M.; Fujikura, T.; Tsuji, T.; Sakao, Y.; Yasuda, H.; et al. Relationship between urinary fractional excretion of sodium and life prognosis in liver cirrhosis patients. Hepatol. Res. 2013, 43, 1156–1162. [Google Scholar] [CrossRef] [PubMed]
- Caraceni, P.; Riggio, O.; Angeli, P.; Alessandria, C.; Neri, S.; Foschi, F.G.; Levantesi, F.; Airoldi, A.; Boccia, S.; Svegliati-Baroni, G.; et al. Long-term albumin administration in decompensated cirrhosis (ANSWER): An open-label randomised trial. Lancet 2018, 391, 2417–2429. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hypothesis | Cohort | Intervention | Outcomes | Reference No. |
|---|---|---|---|---|
| determine the effects of tolvaptan | 164 cirrhosis | Multicenter, double-blind, placebo-controlled. 7-day trial placebo (n = 80), add-on tolvaptan 7.5 mg/day (n = 84) | Tolvaptan decreased the body weight (−1.95 kg in tolvaptan vs. −0.44 kg in placebo) | 47 |
| determine the optimal dose of tolvaptan | 104 cirrhosis | Multicenter, double-blind, placebo-controlled. 7-day trial placebo (n = 27), add-on tolvaptan 7.5 mg/day (n = 26), 15 mg/day (n = 25), 30 mg/day (n = 26) | Tolvaptan at 7.5 mg/day induced a maximum decrease in body weight with preferable tolerability (−2.31 kg in 7.5 mg/day vs. −1.88 kg in 15 mg/day vs. −1.67 kg in 30 mg/day vs. −0.36 kg/day in placebo) | 48 |
| determine the effects of tolvaptan | 530 cirrhosis | Multicenter, double-blind, placebo-controlled. 7-day trial placebo (n = 76), add-on tolvaptan 7.5 mg/day (n = 153) 15 mg/day (n = 301) | Tolvaptan decreased the body weight (−2.0 kg in 7.5 mg/day, −2.2 kg in 15 mg/day vs. −1.2 kg in placebo) | 49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adachi, T.; Takeuchi, Y.; Takaki, A.; Oyama, A.; Wada, N.; Onishi, H.; Shiraha, H.; Okada, H. Management of Cirrhotic Ascites under the Add-on Administration of Tolvaptan. Int. J. Mol. Sci. 2021, 22, 5582. https://doi.org/10.3390/ijms22115582
Adachi T, Takeuchi Y, Takaki A, Oyama A, Wada N, Onishi H, Shiraha H, Okada H. Management of Cirrhotic Ascites under the Add-on Administration of Tolvaptan. International Journal of Molecular Sciences. 2021; 22(11):5582. https://doi.org/10.3390/ijms22115582
Chicago/Turabian StyleAdachi, Takuya, Yasuto Takeuchi, Akinobu Takaki, Atsushi Oyama, Nozomu Wada, Hideki Onishi, Hidenori Shiraha, and Hiroyuki Okada. 2021. "Management of Cirrhotic Ascites under the Add-on Administration of Tolvaptan" International Journal of Molecular Sciences 22, no. 11: 5582. https://doi.org/10.3390/ijms22115582