
Heparin-Tagged PLA-PEG Copolymer-Encapsulated Biochanin A-Loaded (Mg/Al) LDH Nanoparticles Recommended for Non-Thrombogenic and Anti-Proliferative Stent Coating



Abstract
:1. Introduction
2. Results
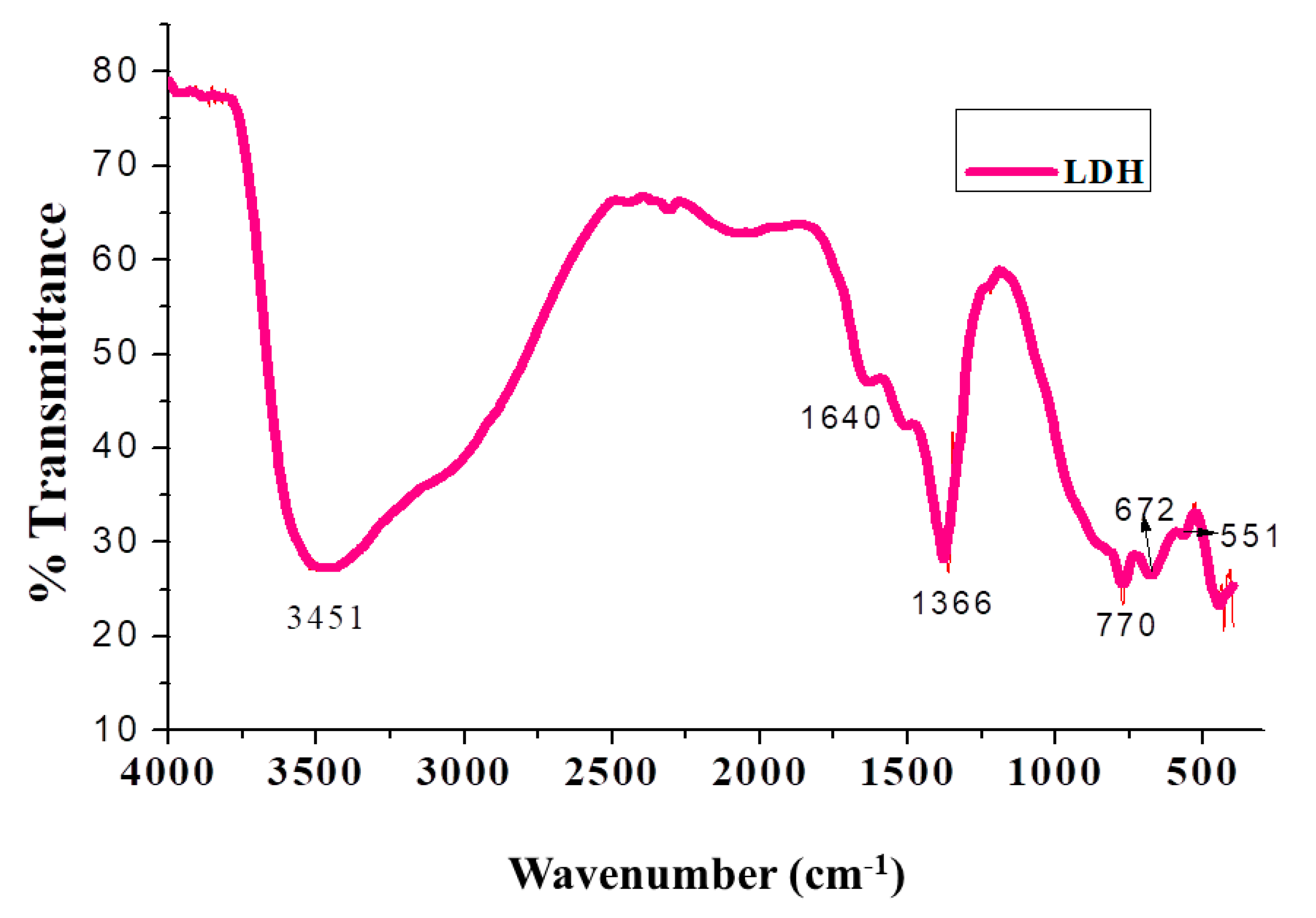
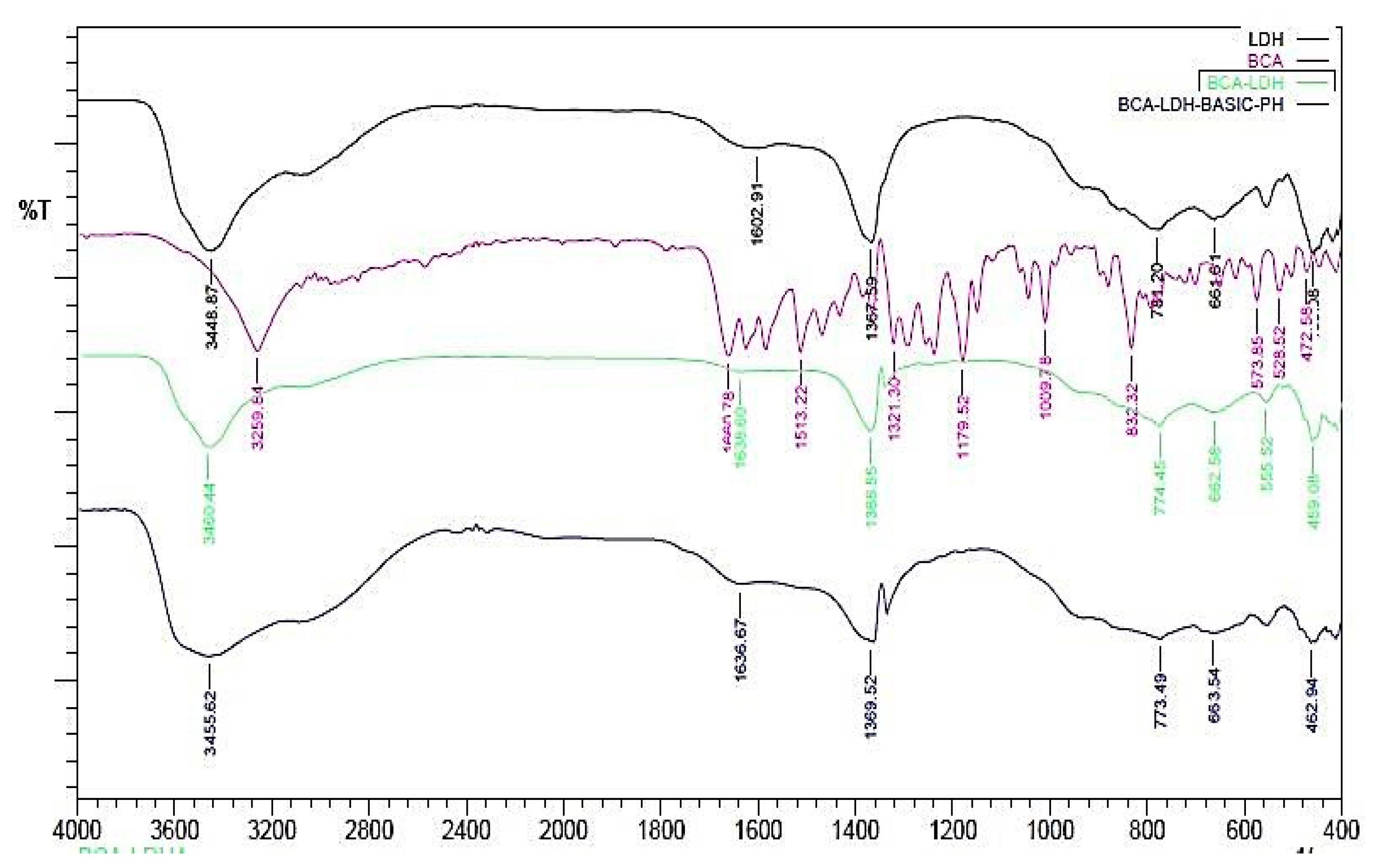
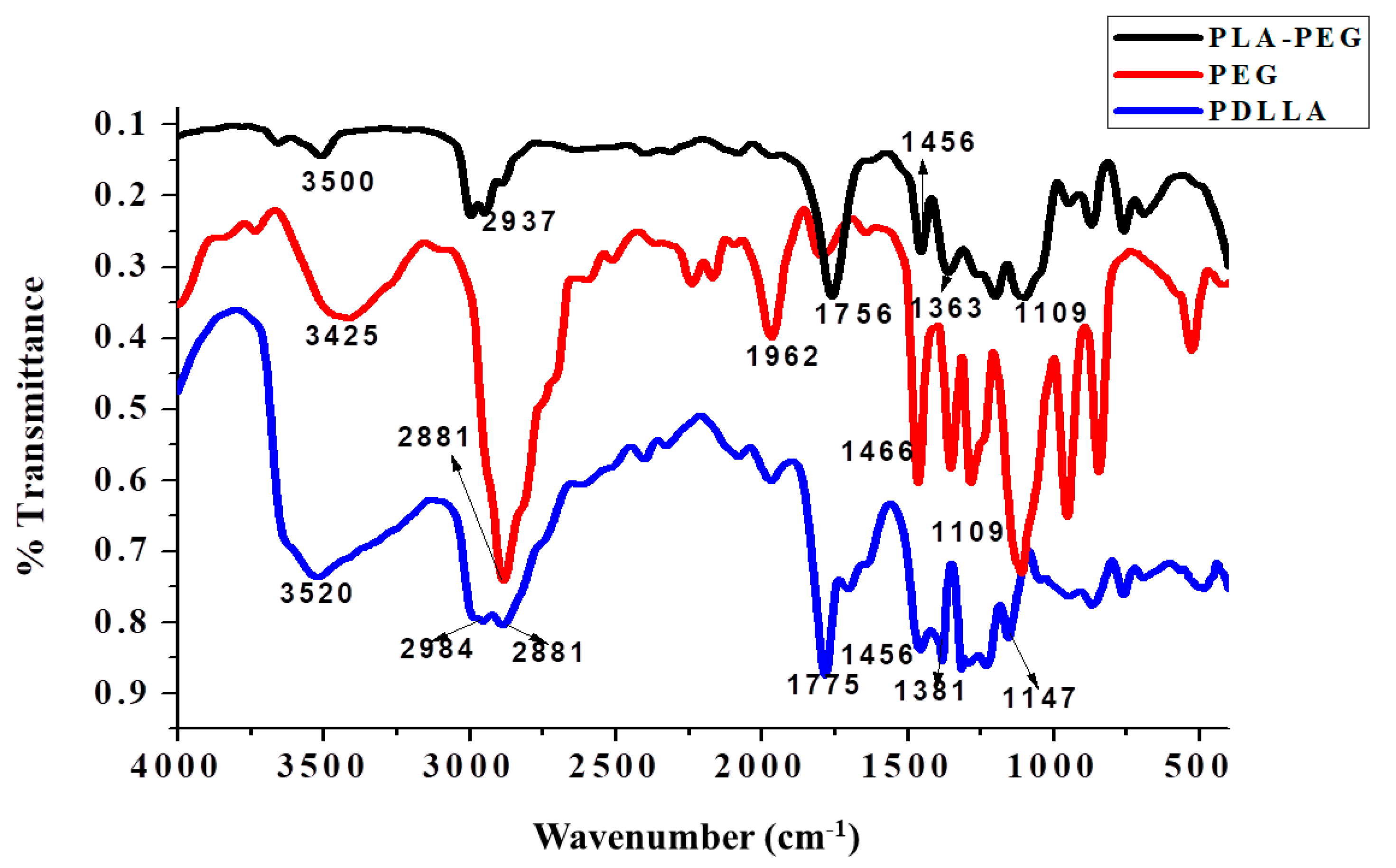
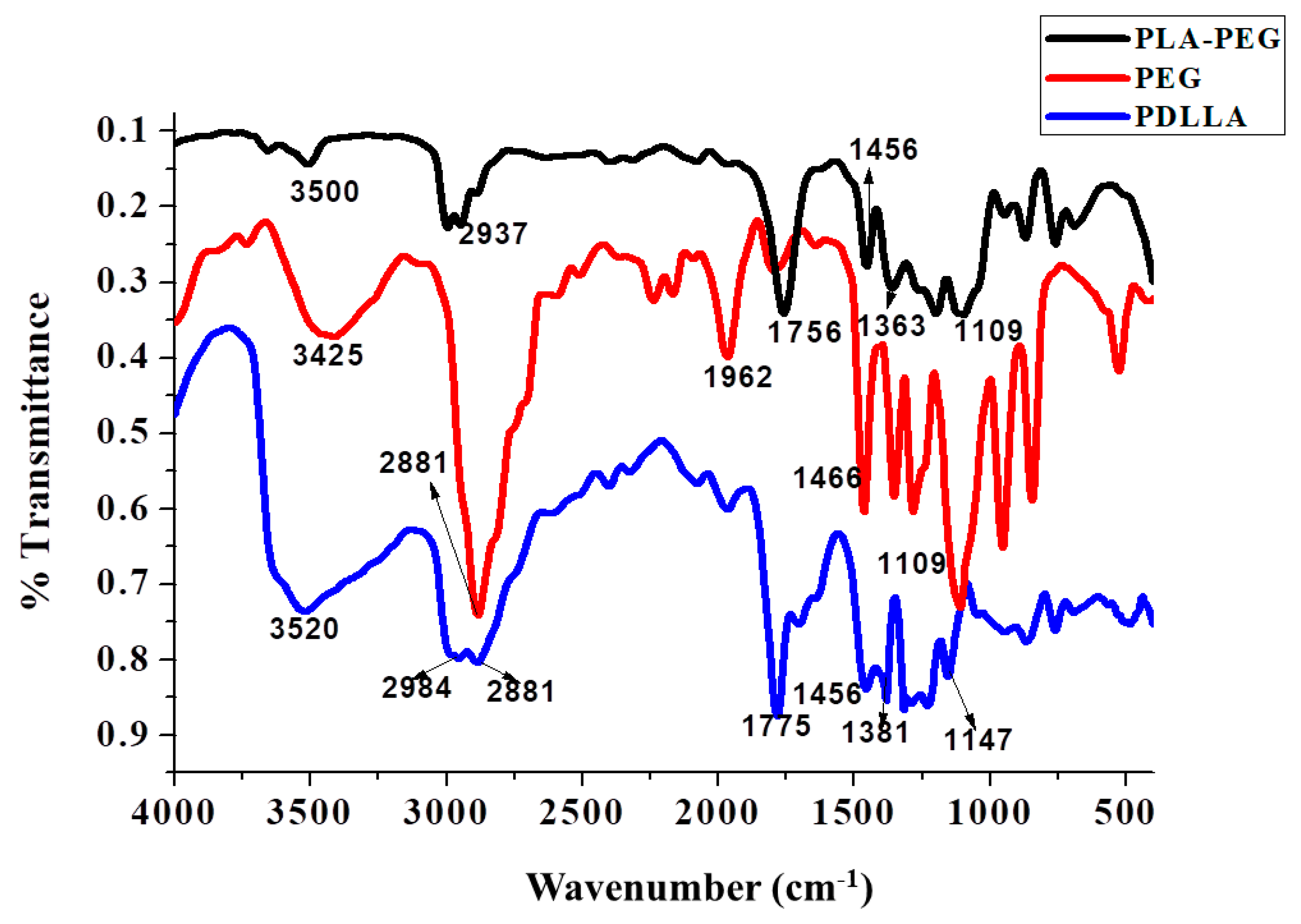
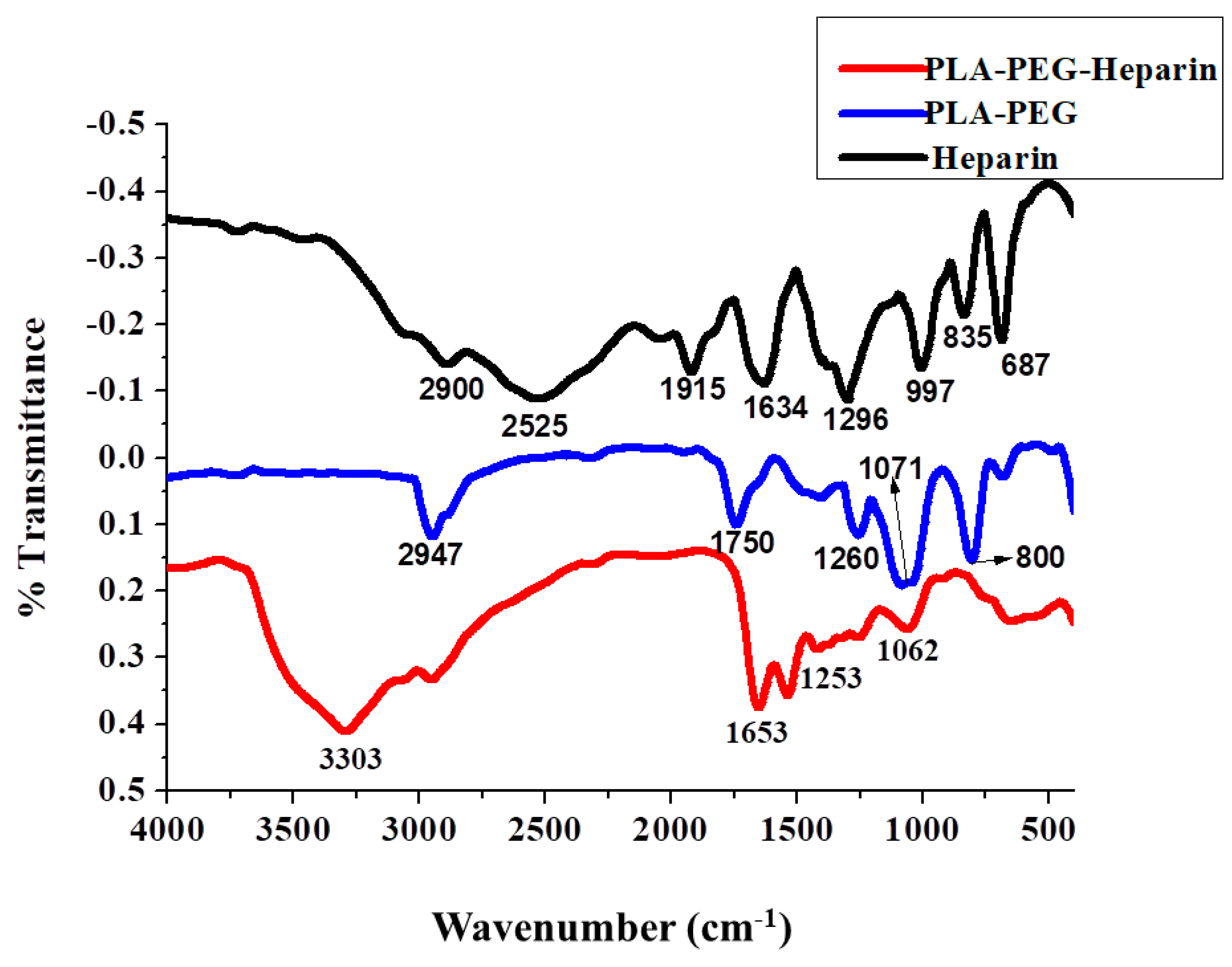
2.1. FTIR
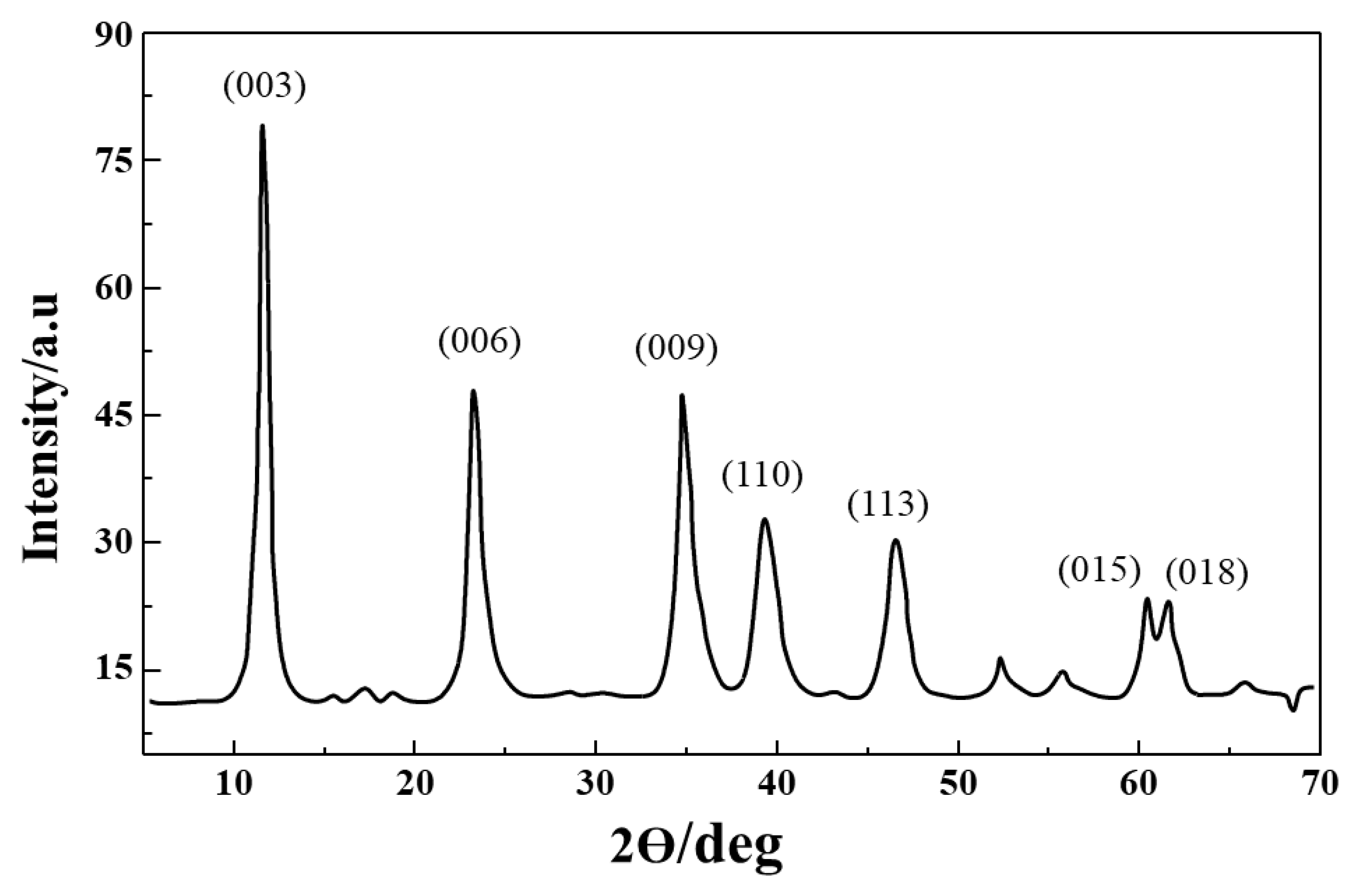
2.2. XRD of Mg/Al (LDH) Nanoparticles
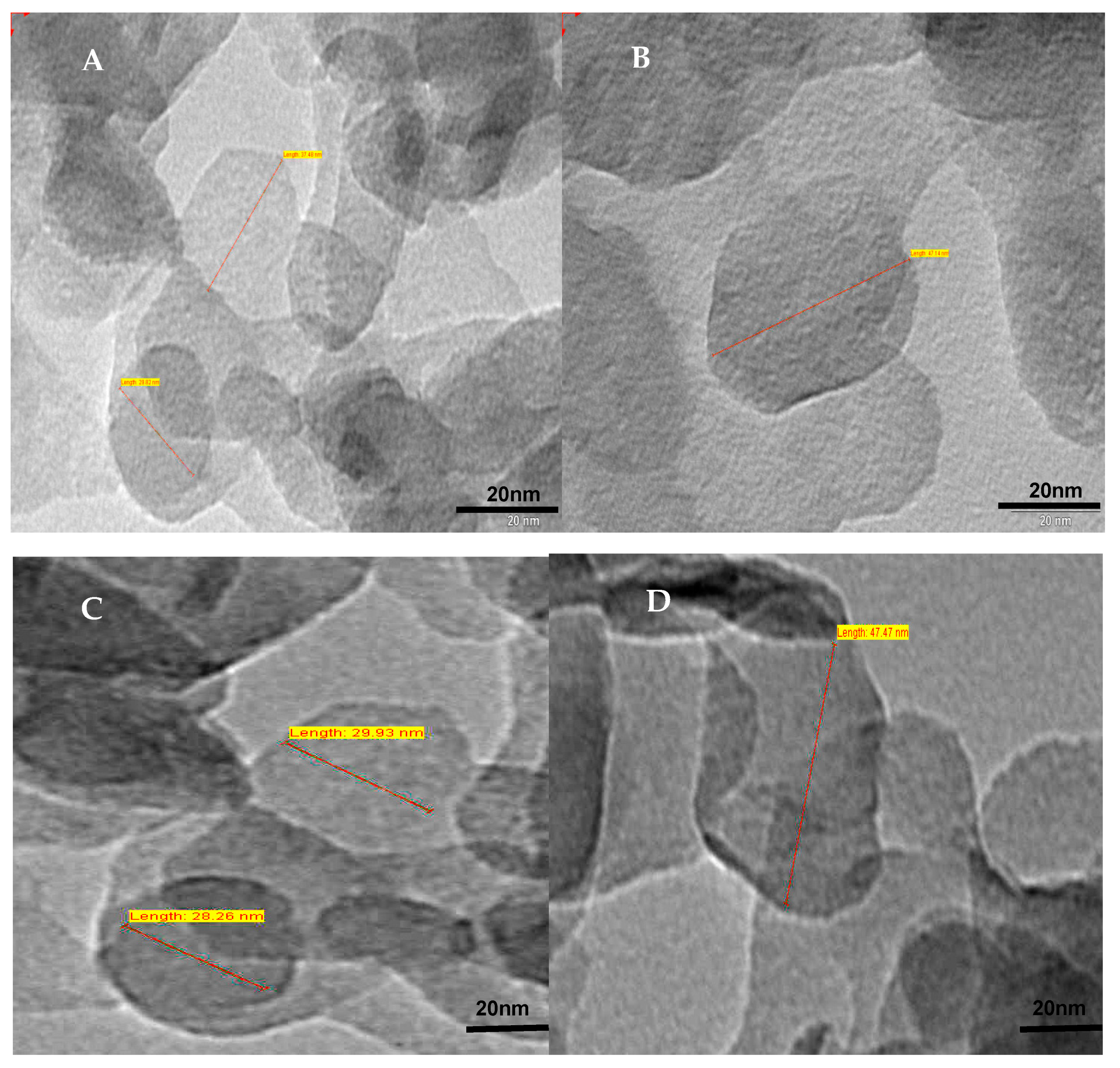
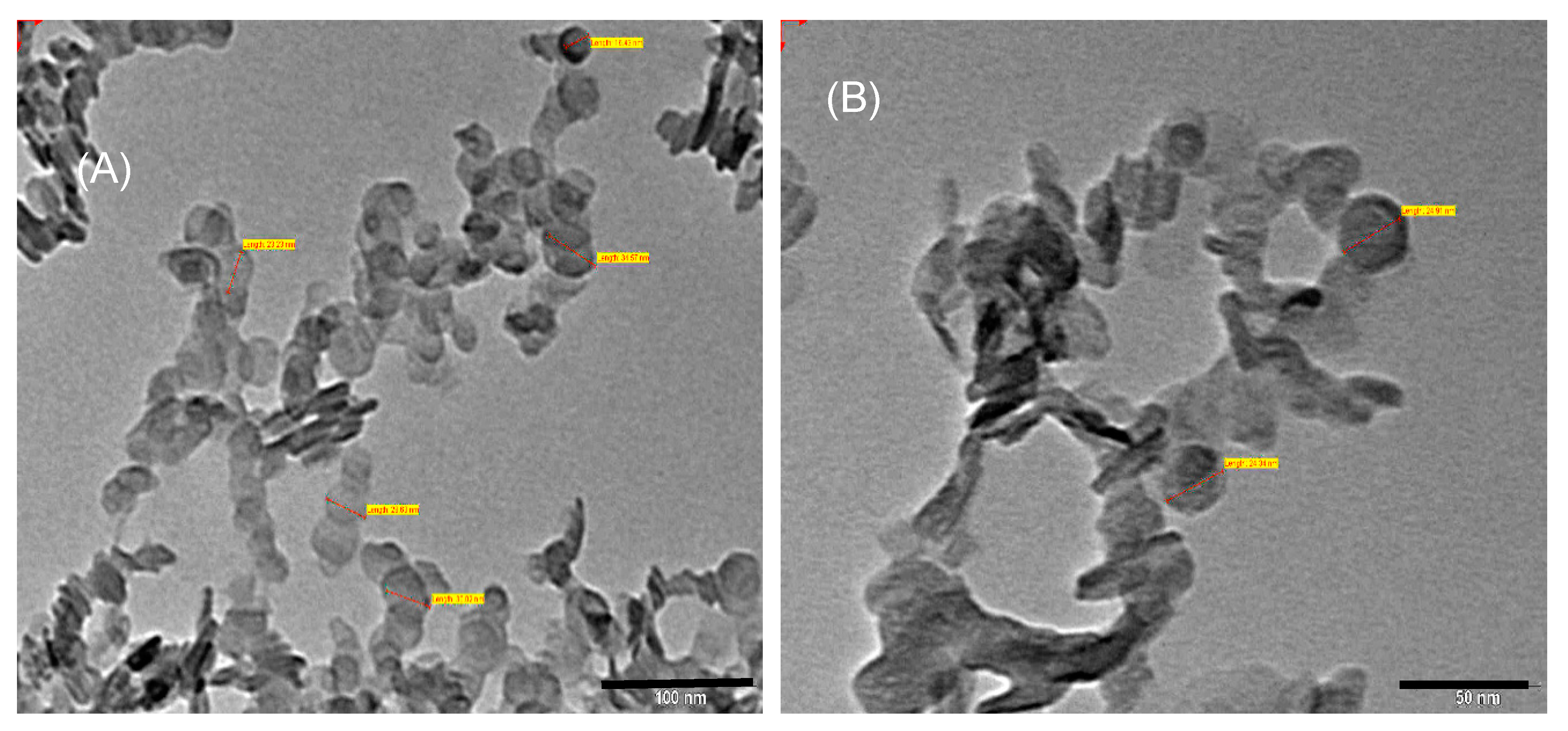
2.3. TEM Images of LDH
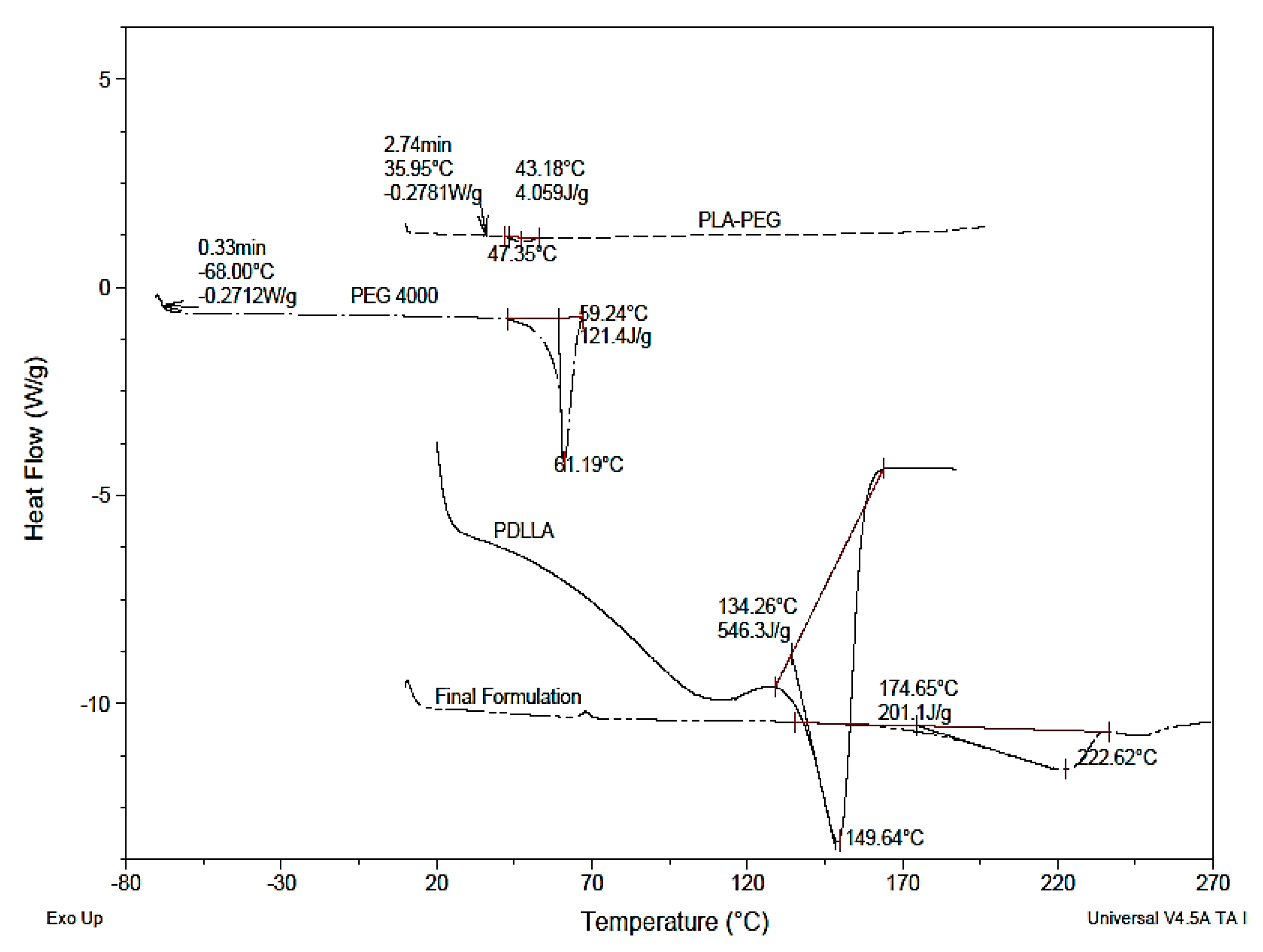
2.4. DSC Thermograms
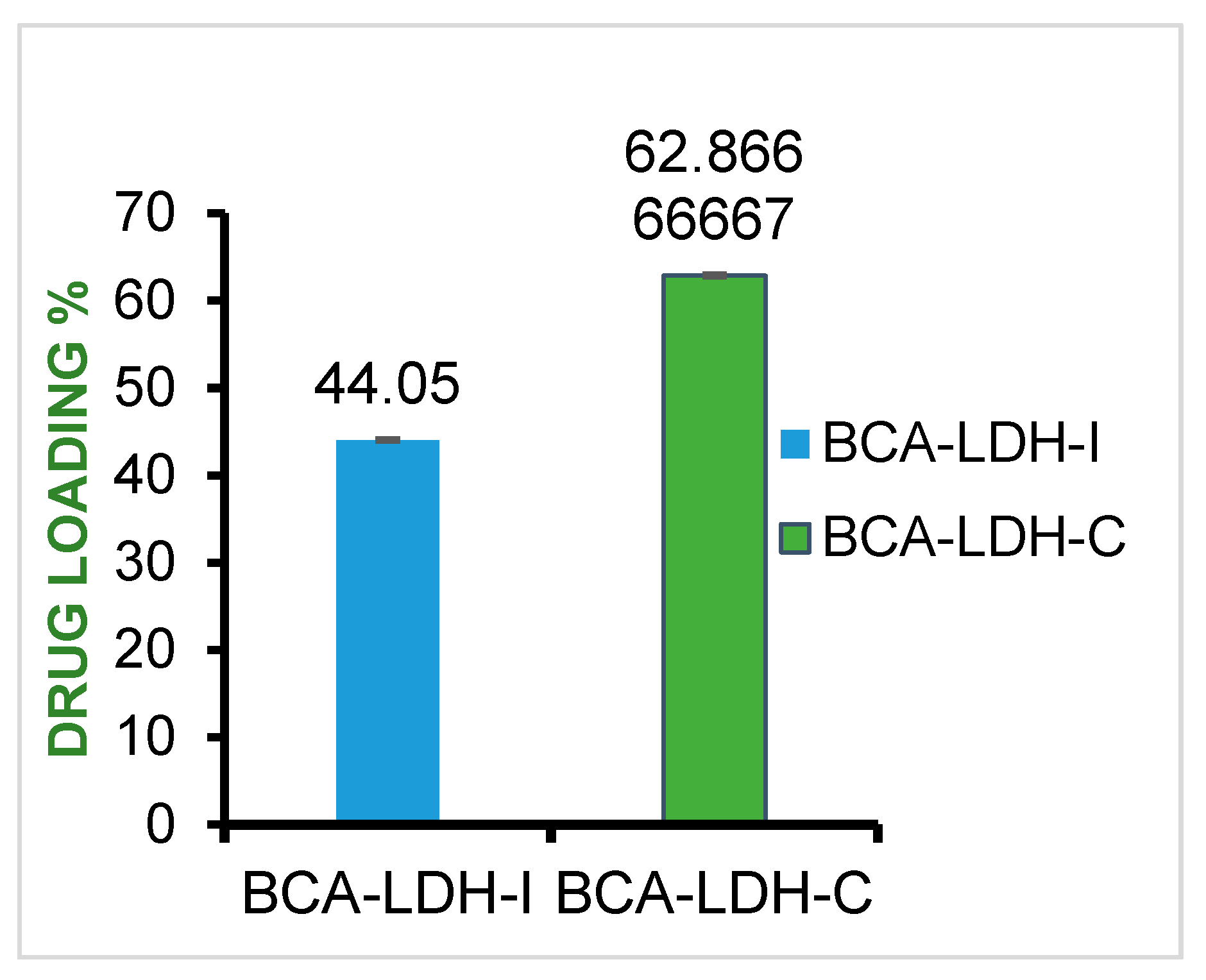
2.5. Drug-Loading Efficiency
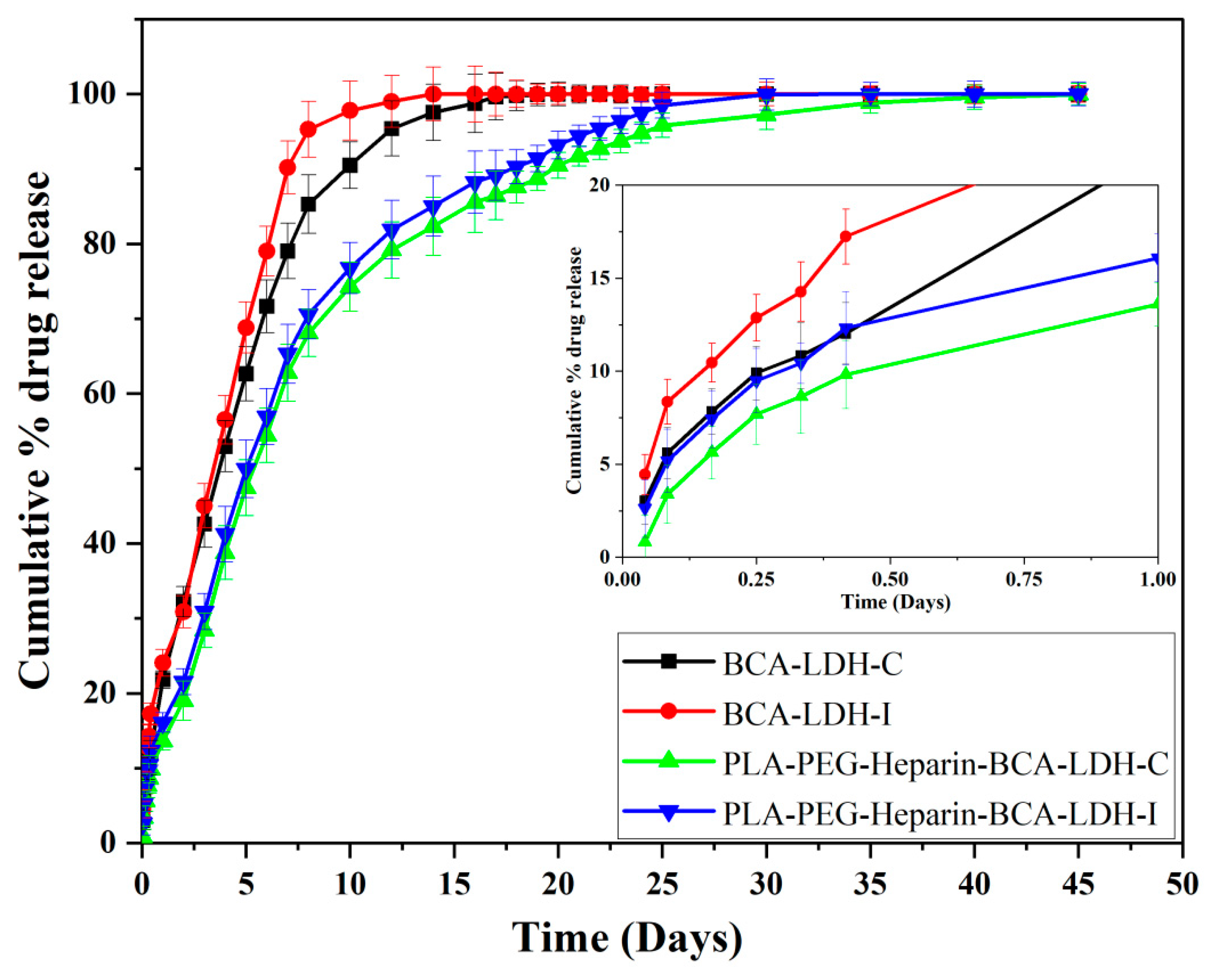
2.6. In Vitro Drug Release Study
2.7. Mathematical Modelling
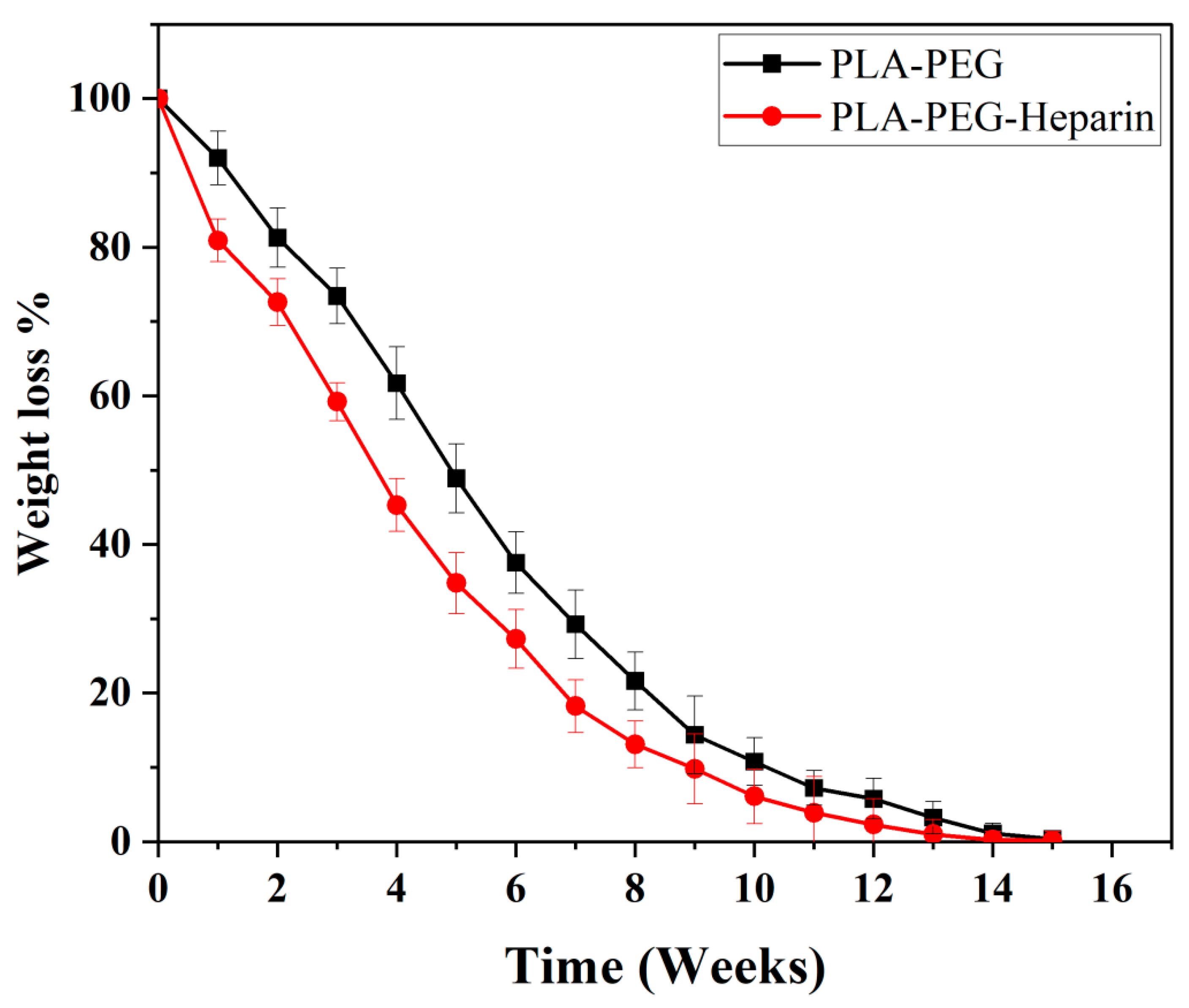
2.8. In Vitro Degradation Study of Polymer
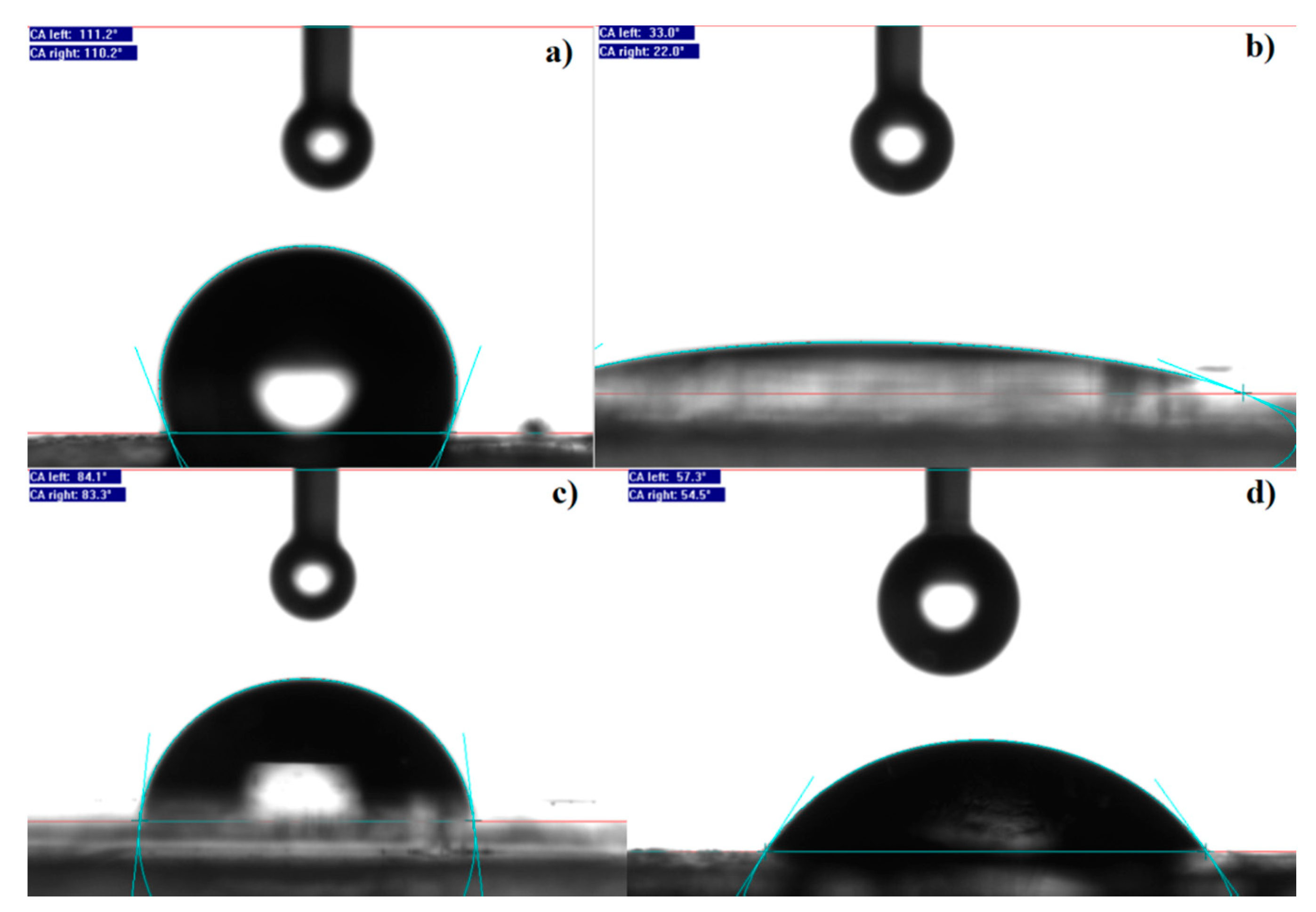
2.9. Wettability Studies
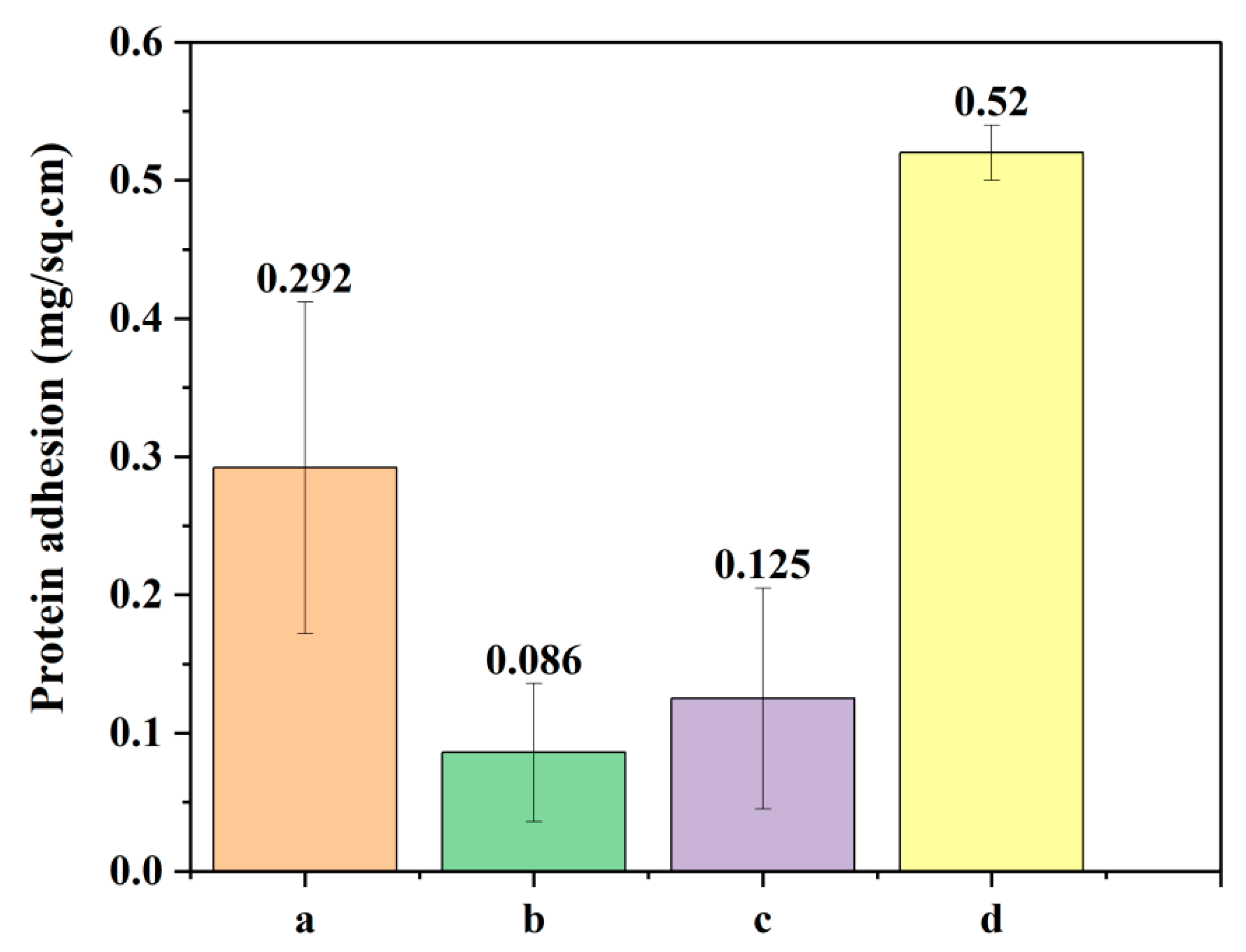
2.10. Protein Adhesion Test
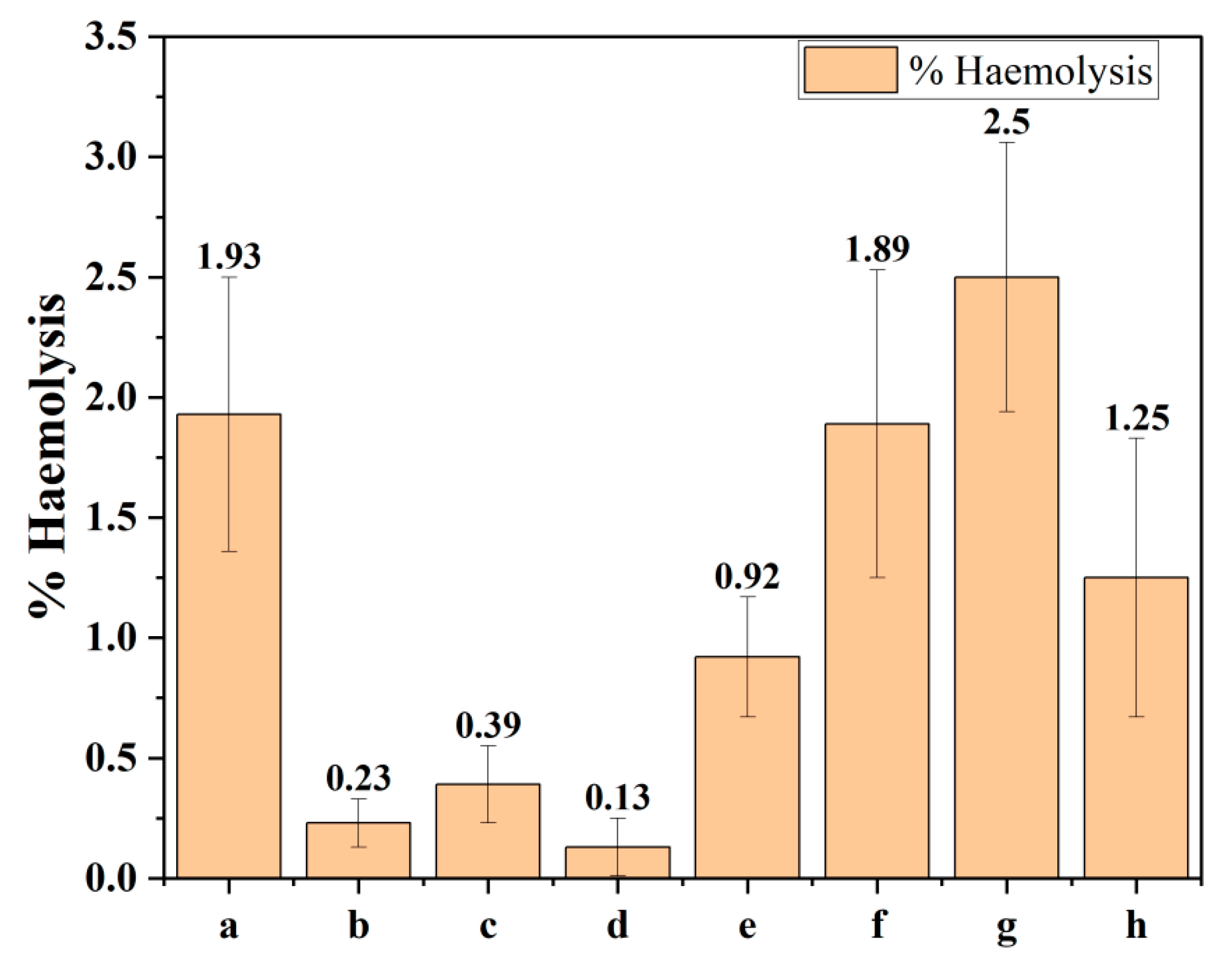
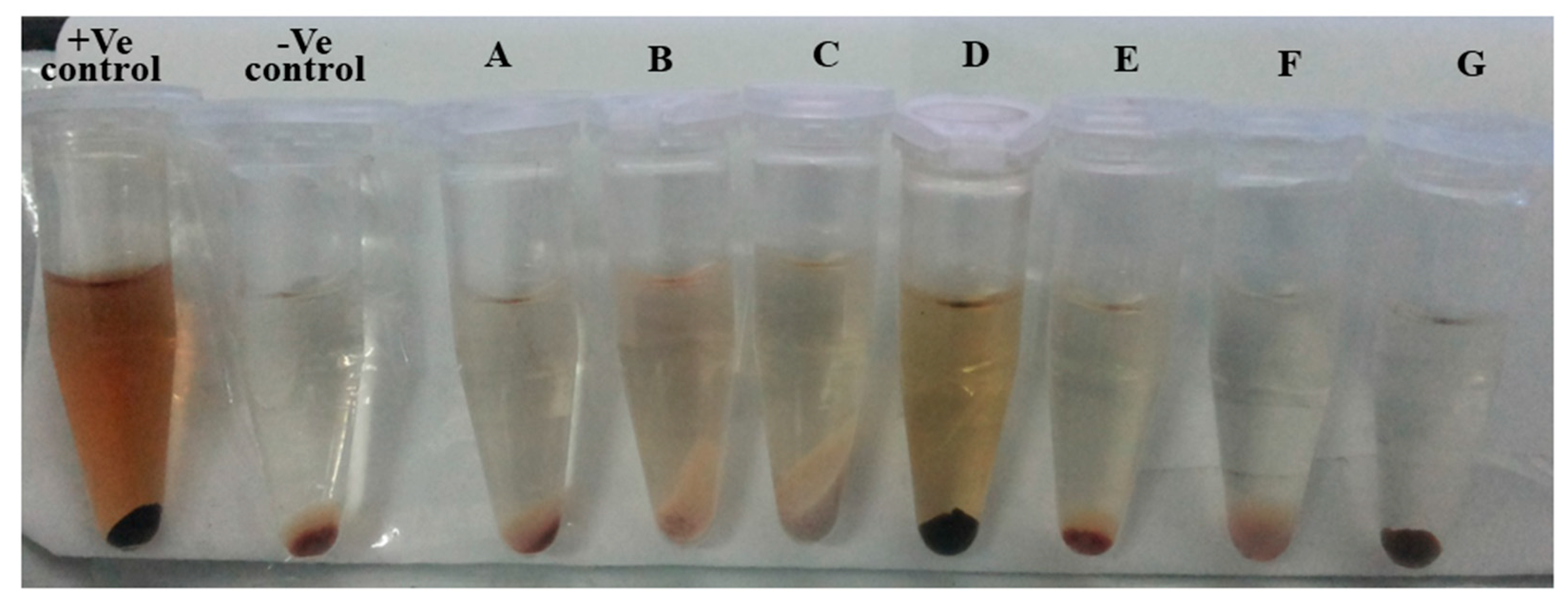
2.11. In Vitro Hemocompatibility Study
2.12. Stability Studies of BCA-LDH Nanoparticles
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Methodology
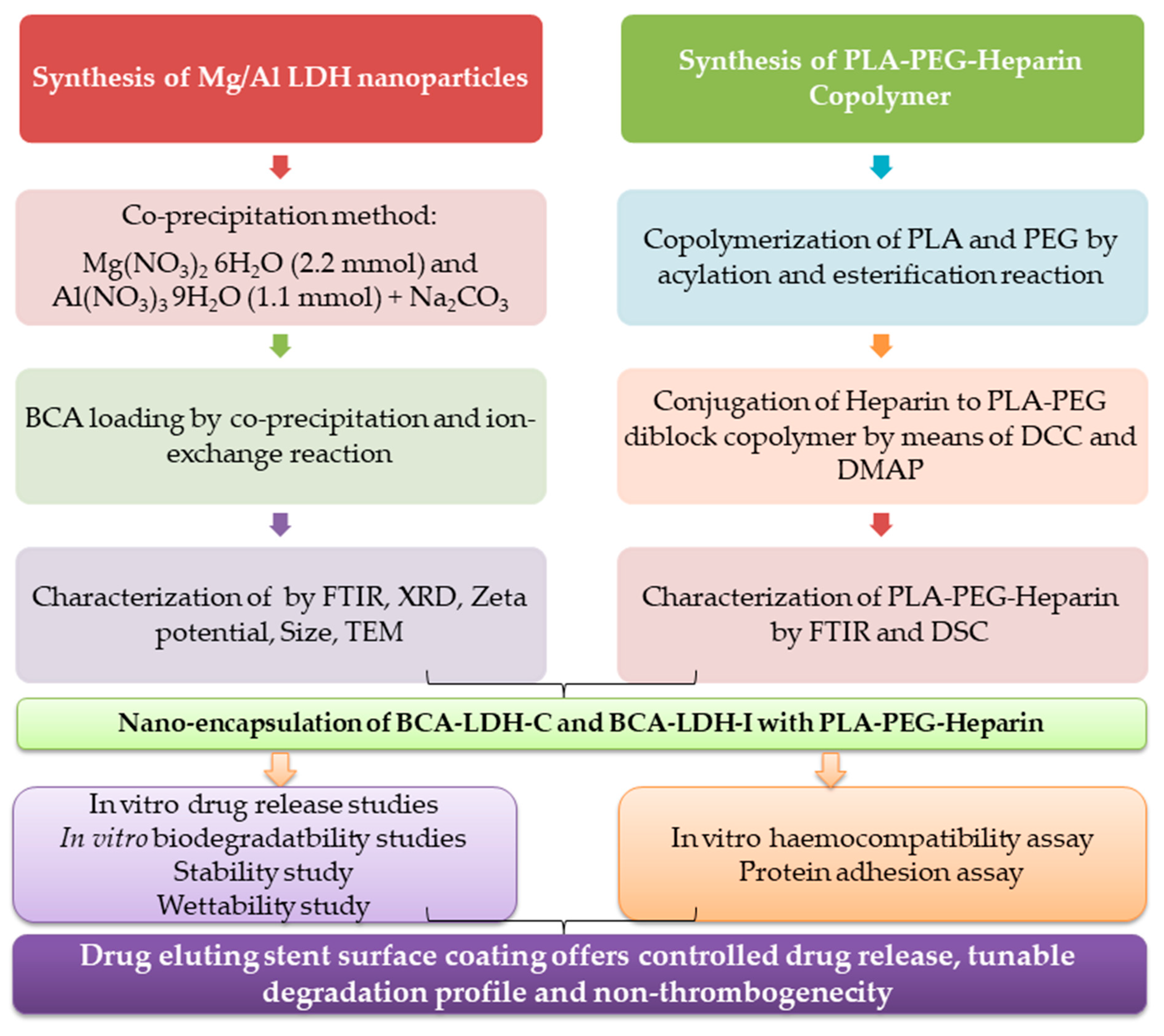
4.2.1. Synthesis
Synthesis of Mg/Al Layered Double Hydroxide (LDH) Nanoparticles
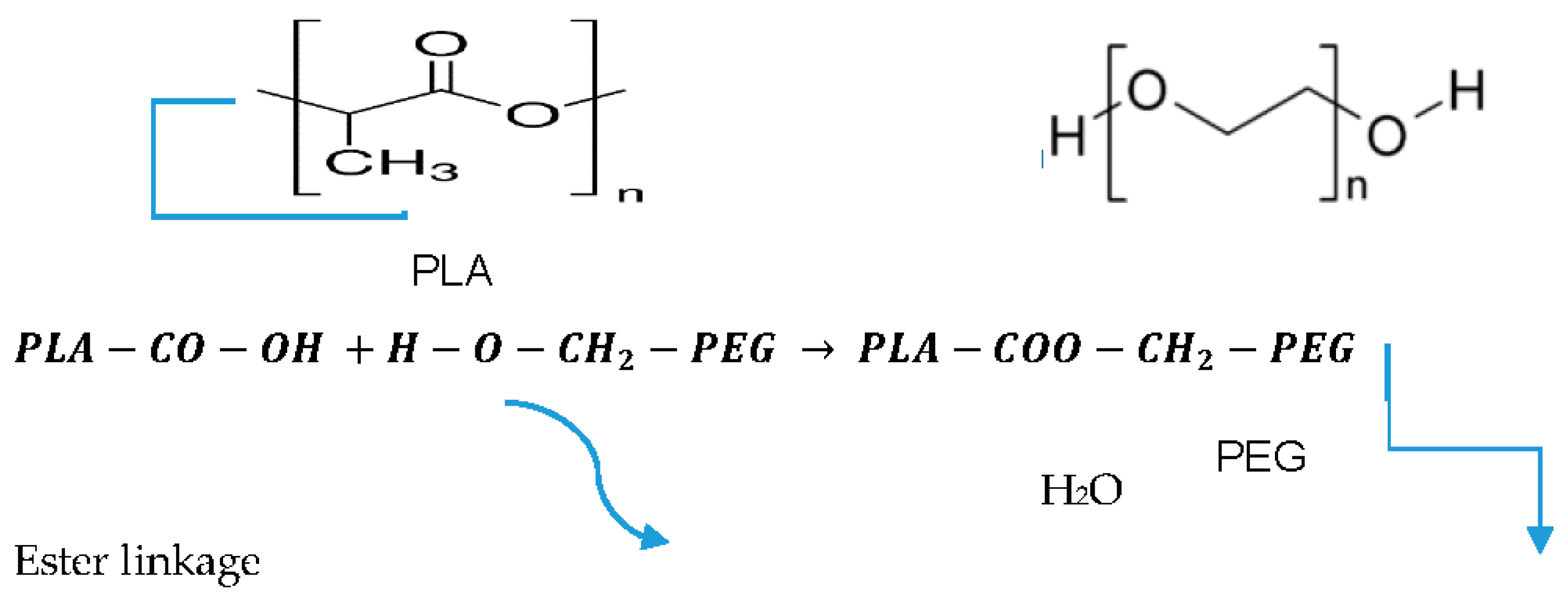
Synthesis of PLA-PEG Copolymer
Synthesis of PLA-PEG Copolymer by Acylation and Esterification Reaction
Synthesis of Heparin-Tagged PLA-PEG Copolymer
4.2.2. Analytical Method Development and Drug Loading in LDH Nanoparticles
Absorption Maxima Determination and Calibration Curve of Biochanin A
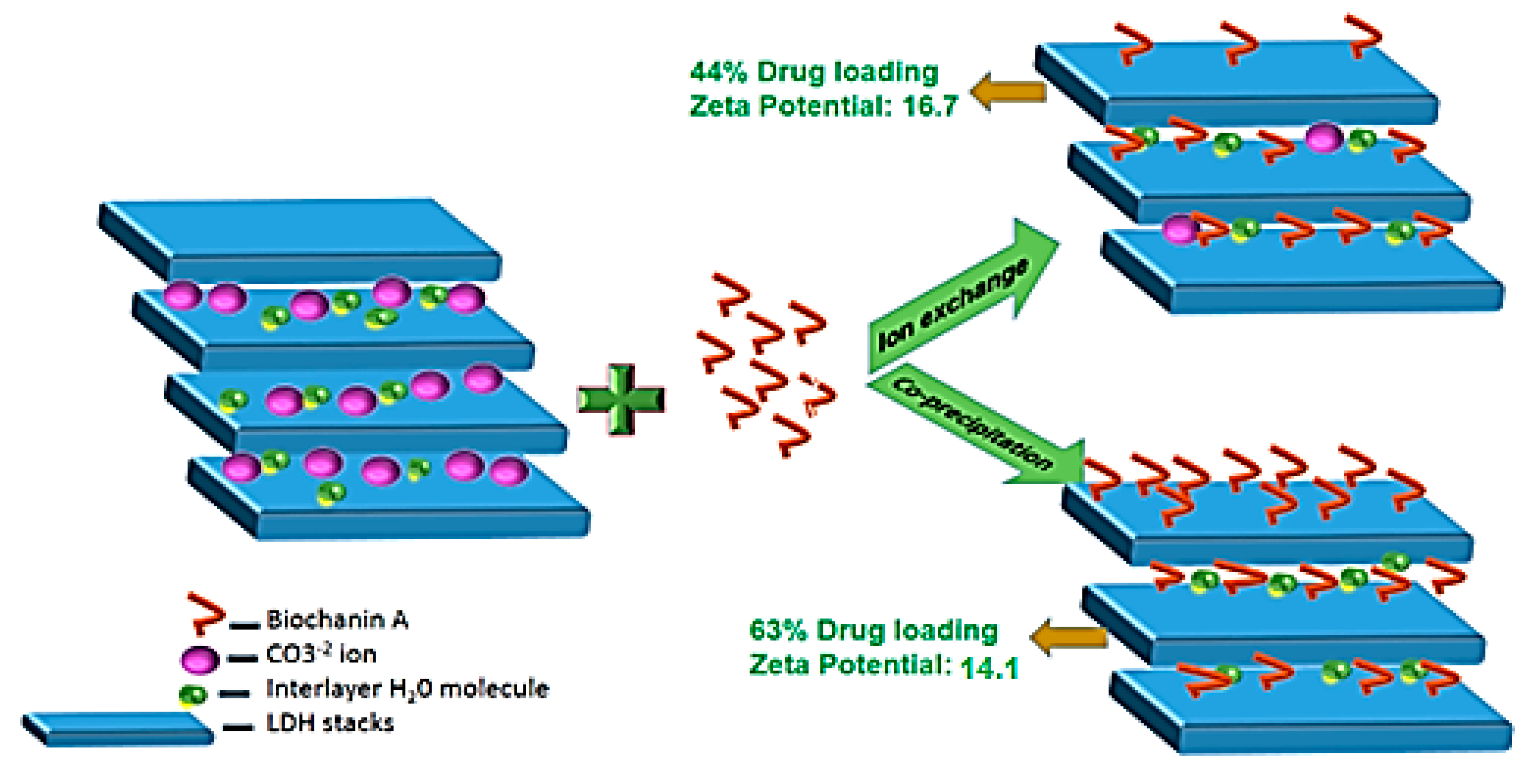
Biochanin A (BCA) Loading in LDH Nanoparticles
Nano-Encapsulation of BCA-LDH-C and BCA-LDH-I with PLA-PEG-Heparin
Drug Release Studies
4.2.3. Characterizations
Functional Group Analysis by FTIR
Zeta Potential and Hydrodynamic Diameter by Photon Correlation Spectroscopy
Crystallite Structure by X-ray Diffraction
Particle Size and Structure by TEM
Thermal Analysis by Differential Scanning Calorimetry (DSC)
4.2.4. Wettability Study
4.2.5. In Vitro Biodegradability Studies
4.2.6. Hemocompatability Study
4.2.7. Protein Adhesion Test
4.2.8. Stability Studies of BCA-LDH Nanoparticles:
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| CAD | Coronary Artery Disease |
| CVD | Cardio Vascular Disease |
| PCI | Percutaneous Coronary Intervention |
| ISR | In Stent Restenosis |
| VSMC | Vascular Smooth Muscle Cells |
| EC | Endothelial Cells |
| NH | Neointimal Hyperplacia |
| PLA-PEG | Poly lactic acid–co-Poly ethylene glycol |
| BMS | Bare Metal Stents |
| DES | Drug-eluting stent |
| LDH | Layered Double Hydroxide |
| BCA | Biochanin A |
| PLA | Poly-DL-Lacticacid |
| PEG | Polyethylene glycol |
| PLA-PEG | Polylactide-co-polyethylene glycol |
| PLA-PEG-Heparin | Heparin-tagged Polylactide-co-polyethylene glycol |
| BCA-LDH | Biochanin A-loaded LDH |
| BCA-LDH-I | Biochanin A-loaded LDH nanoparticles produced by ion-exchange method |
| BCA-LDH-C | Biochanin A-loaded LDH nanoparticles produced by co-precipitation method |
| PLA-PEG-Heparin-BCA-LDH-I | Biochanin A-loaded LDH nanoparticles produced by ion-exchange method encapsulated in PLA-PEG-Heparin copolymer |
| PLA-PEG-Heparin-BCA-LDH-C | Biochanin A-loaded LDH nanoparticles produced by co-precipitation method encapsulated in PLA-PEG-Heparin copolymer |
| BSA | Bovine serum albumin |
| ACD | Acid Citrate Dextrose |
References
- Butt, M.; Connolly, D.; Lip, G.Y. Drug-eluting stents: A comprehensive appraisal. Future Cardiol. 2009, 5, 141–157. [Google Scholar] [CrossRef]
- Costa, M.A.; Simon, D.I. Molecular Basis of Restenosis and Drug-Eluting Stents. Circulation 2005, 111, 2257–2273. [Google Scholar] [CrossRef]
- Martin, D.M.; Boyle, F.J. Drug-eluting stents for coronary artery disease: A review. Med. Eng. Phys. 2011, 33, 148–163. [Google Scholar] [CrossRef] [Green Version]
- Inoue, T.; Croce, K.; Morooka, T.; Sakuma, M.; Node, K.; Simon, D.I. Vascular Inflammation and Repair: Implications for Re-Endothelialization, Restenosis, and Stent Thrombosis. JACC Cardiovasc. Interv. 2011, 4, 1057–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simard, T.; Hibbert, B.; Ramirez, F.D.; Froeschl, M.; Chen, Y.-X.; O’Brien, E.R. The Evolution of Coronary Stents: A Brief Review. Can. J. Cardiol. 2014, 30, 35–45. [Google Scholar] [CrossRef]
- Hayashi, S.-I.; Yamamoto, A.; You, F.; Yamashita, K.; Ikegame, Y.; Tawada, M.; Yoshimori, T.; Shimizu, S.; Nakashima, S. The Stent-Eluting Drugs Sirolimus and Paclitaxel Suppress Healing of the Endothelium by Induction of Autophagy. Am. J. Pathol. 2009, 175, 2226–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K. Dual drug-eluting stent. J. Control. Release 2012, 159, 1. [Google Scholar] [CrossRef]
- Finn, A.V.; Kolodgie, F.D.; Harnek, J.; Guerrero, L.; Acampado, E.; Tefera, K.; Skorija, K.; Weber, D.K.; Gold, H.K.; Virmani, R. Differential Response of Delayed Healing and Persistent Inflammation at Sites of Overlapping Sirolimus- or Paclitaxel-Eluting Stents. Circulation 2005, 112, 270–278. [Google Scholar] [CrossRef] [Green Version]
- Zimarino, M.; Corazzini, A.; Ricci, F.; Di Nicola, M.; De Caterina, R. Late thrombosis after double versus single drug-eluting stent in the treatment of coronary bifurcations: A meta-analysis of randomized and observational studies. JACC Cardiovasc. Interv. 2013, 6, 687–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceylan, H.; Tekinay, A.B.; Guler, M.O. Selective adhesion and growth of vascular endothelial cells on bioactive peptide nanofiber functionalized stainless steel surface. Biomaterials 2011, 32, 8797–8805. [Google Scholar] [CrossRef]
- Chen, J.P.; Hou, D.; Pendyala, L.; Goudevenos, J.A.; Kounis, N.G. Drug-Eluting Stent Thrombosis: The Kounis Hypersensitivity-Associated Acute Coronary Syndrome Revisited. JACC Cardiovasc. Interv. 2009, 2, 583–593. [Google Scholar] [CrossRef] [Green Version]
- Massberg, S.; Byrne, R.A.; Kastrati, A.; Schulz, S.; Pache, J.; Hausleiter, J.; Ibrahim, T.; Fusaro, M.; Ott, I.; Schömig, A. Polymer-free sirolimus-and probucol-eluting versus new generation zotarolimus-eluting stents in coronary artery disease: The Intracoronary Stenting and Angiographic Results: Test Efficacy of Sirolimus-and Probucol-Eluting versus Zotarolimus-eluting Stents (ISAR-TEST 5) trial. Circulation 2011, 124, 624–632. [Google Scholar] [PubMed]
- Kim, W.; Jeong, M.H.; Cha, K.S.; Hyun, D.W.; Hur, S.H.; Kim, K.B.; Hong, Y.J.; Park, H.W.; Kim, J.H.; Ahn, Y.K.; et al. Effect of Anti-Oxidant (Carvedilol and Probucol) Loaded Stents in a Porcine Coronary Restenosis Model. Circ. J. 2005, 69, 101–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houston, S.A.; Ugusman, A.; Gnanadesikan, S.; Kennedy, S. An investigation of the antiplatelet effects of succinobucol (AGI-1067). Platelets 2016, 28, 295–300. [Google Scholar] [CrossRef]
- Dourron, H.M.; Jacobson, G.M.; Park, J.L.; Liu, J.; Reddy, D.J.; Scheel, M.L.; Pagano, P.J. Perivascular gene transfer of NADPH oxidase inhibitor suppresses angioplasty-induced neointimal proliferation of rat carotid artery. Am. J. Physiol. Circ. Physiol. 2005, 288, H946–H953. [Google Scholar] [CrossRef]
- Bräsen, J.H.; Leppänen, O.; Inkala, M.; Heikura, T.; Levin, M.; Ahrens, F.; Rutanen, J.; Pietsch, H.; Bergqvist, D.; Levonen, A.-L.; et al. Extracellular Superoxide Dismutase Accelerates Endothelial Recovery and Inhibits In-Stent Restenosis in Stented Atherosclerotic Watanabe Heritable Hyperlipidemic Rabbit Aorta. J. Am. Coll. Cardiol. 2007, 50, 2249–2253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakazawa, G.; Granada, J.F.; Alviar, C.L.; Tellez, A.; Kaluza, G.L.; Guilhermier, M.Y.; Parker, S.; Rowland, S.M.; Kolodgie, F.D.; Leon, M.B.; et al. Anti-CD34 Antibodies Immobilized on the Surface of Sirolimus-Eluting Stents Enhance Stent Endothelialization. JACC Cardiovasc. Interv. 2010, 3, 68–75. [Google Scholar] [CrossRef] [Green Version]
- Kleinedler, J.J.; Foley, J.D.; Alexander, J.S.; Roerig, S.C.; Hebert, V.Y.; Dugas, T.R. Synergistic effect of resveratrol and quercetin released from drug-eluting polymer coatings for endovascular devices. J. Biomed. Mater. Res. Part B Appl. Biomater. 2011, 99, 266–275. [Google Scholar] [CrossRef]
- Kleinedler, J.; Foley, J.; Dugas, T. Cytotoxicity and efficacy evaluation of polymeric nanoparticles containing resveratrol and quercetin for use on drug eluting stents. FASEB J. 2009, 23. [Google Scholar] [CrossRef]
- Yang, J.; Zeng, Y.; Zhang, C.; Chen, Y.-X.; Yang, Z.; Li, Y.; Leng, X.; Kong, D.; Wei, X.-Q.; Sun, H.-F.; et al. The prevention of restenosis in vivo with a VEGF gene and paclitaxel co-eluting stent. Biomaterials 2013, 34, 1635–1643. [Google Scholar] [CrossRef] [Green Version]
- Naghavi, N.; De Mel, A.; Alavijeh, O.S.; Cousins, B.G.; Seifalian, A.M. Nitric Oxide Donors for Cardiovascular Implant Applications. Small 2013, 9, 22–35. [Google Scholar] [CrossRef] [PubMed]
- Majewska, P.; Oledzka, E.; Sobczak, M. Overview of the latest developments in the field of drug-eluting stent technology. Biomater. Sci. 2020, 8, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.K.; Mahmud, E.; Tsimikas, S. Estrogen-Eluting Stents. J. Cardiovasc. Transl. Res. 2009, 2, 240–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- New, G.; Moses, J.W.; Roubin, G.S.; Leon, M.B.; Colombo, A.; Iyer, S.S.; Tio, F.O.; Mehran, R.; Kipshidze, N. Estrogen-eluting, phosphorylcholine-coated stent implantation is associated with reduced neointimal formation but no delay in vascular repair in a porcine coronary model. Catheter. Cardiovasc. Interv. 2002, 57, 266–271. [Google Scholar] [CrossRef]
- Airoldi, F.; Di Mario, C.; Ribichini, F.; Presbitero, P.; Sganzerla, P.; Ferrero, V.; Vassanelli, C.; Briguori, C.; Carlino, M.; Montorfano, M.; et al. 17-Beta-Estradiol Eluting Stent Versus Phosphorylcholine-Coated Stent for the Treatment of Native Coronary Artery Disease. Am. J. Cardiol. 2005, 96, 664–667. [Google Scholar] [CrossRef]
- Abizaid, A.; Albertal, M.; Costa, M.A.; Abizaid, A.S.; Staico, R.; Feres, F.; Mattos, L.A.; Sousa, A.G.; Moses, J.; Kipshidize, N. First human experience with the 17-beta-estradiol–eluting stent: The estrogen and stents to eliminate restenosis (EASTER) trial. J. Am. Coll. Cardiol. 2004, 43, 1118–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrepfer, S.; Deuse, T.; Münzel, T.; Schäfer, H.; Braendle, W.; Reichenspurner, H. The selective estrogen receptor-β agonist biochanin A shows vasculoprotective effects without uterotrophic activity. Menopause 2006, 13, 489–499. [Google Scholar] [CrossRef]
- Kumar, T.; Sharma, M.; Rana, A.; Lingaraju, M.C.; Parida, S.; Kumar, D.; Singh, T.U. Biochanin-A elicits relaxation in coronary artery of goat through different mechanisms. Res. Veter. Sci. 2020, 131, 206–214. [Google Scholar] [CrossRef]
- Somjen, D.; Knoll, E.; Kohen, F.; Stern, N. Effects of phytoestrogens on DNA synthesis and creatine kinase activity in vascular cells. Am. J. Hypertens. 2001, 14, 1256–1262. [Google Scholar] [CrossRef] [Green Version]
- Puranik, A.S.; Dawson, E.R.; Peppas, N.A. Recent advances in drug eluting stents. Int. J. Pharm. 2013, 441, 665–679. [Google Scholar] [CrossRef] [Green Version]
- Kolandaivelu, K.; Swaminathan, R.; Gibson, W.J.; Kolachalama, V.B.; Nguyen-Ehrenreich, K.-L.; Giddings, V.L.; Coleman, L.; Wong, G.K.; Edelman, E.R. Stent thrombogenicity early in high-risk interventional settings is driven by stent design and deployment and protected by polymer-drug coatings. Circulation 2011, 123, 1400–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strohbach, A.; Busch, R. Polymers for Cardiovascular Stent Coatings. Int. J. Polym. Sci. 2015, 2015, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Yazdani, S.K.; Sheehy, A.; Pacetti, S.; Rittlemeyer, B.; Kolodgie, F.D.; Virmani, R. Stent Coating Integrity of Durable and Biodegradable Coated Drug Eluting Stents. J. Interv. Cardiol. 2016, 29, 483–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizas, K.D.; Mehilli, J. Stent Polymers. Circ. Cardiovasc. Interv. 2016, 9, e002943. [Google Scholar] [CrossRef] [PubMed]
- Stefanini, G.G.; Byrne, R.A.; Serruys, P.W.; De Waha, A.; Meier, B.; Massberg, S.; Jüni, P.; Schömig, A.; Windecker, S.; Kastrati, A. Biodegradable polymer drug-eluting stents reduce the risk of stent thrombosis at 4 years in patients undergoing percutaneous coronary intervention: A pooled analysis of individual patient data from the ISAR-TEST 3, ISAR-TEST 4, and LEADERS randomized trials. Eur. Heart J. 2012, 33, 1214–1222. [Google Scholar] [CrossRef] [Green Version]
- Tada, N.; Virmani, R.; Grant, G.; Bartlett, L.; Black, A.; Clavijo, C.; Christians, U.; Betts, R.; Savage, D.; Su, S.-H.; et al. Polymer-Free Biolimus A9-Coated Stent Demonstrates More Sustained Intimal Inhibition, Improved Healing, and Reduced Inflammation Compared With a Polymer-Coated Sirolimus-Eluting Cypher Stent in a Porcine Model. Circ. Cardiovasc. Interv. 2010, 3, 174–183. [Google Scholar] [CrossRef] [Green Version]
- Ormiston, J.A.; Serruys, P.W.; Regar, E.; Dudek, D.; Thuesen, L.; Webster, M.W.; Onuma, Y.; Garcia-Garcia, H.M.; McGreevy, R.; Veldhof, S. A bioabsorbable everolimus-eluting coronary stent system for patients with single de-novo coronary artery lesions (ABSORB): A prospective open-label trial. Lancet 2008, 371, 899–907. [Google Scholar] [CrossRef]
- Bae, I.-H.; Park, I.-K.; Park, D.S.; Lee, H.; Jeong, M.H. Thromboresistant and endothelialization effects of dopamine-mediated heparin coating on a stent material surface. J. Mater. Sci. Mater. Electron. 2012, 23, 1259–1269. [Google Scholar] [CrossRef]
- Yang, Z.; Yang, Y.; Zhang, L.; Xiong, K.; Li, X.; Zhang, F.; Wang, J.; Zhao, X.; Huang, N. Mussel-inspired catalytic selenocystamine-dopamine coatings for long-term generation of therapeutic gas on cardiovascular stents. Biomaterials 2018, 178, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Luo, R.; Tang, L.; Zhong, S.; Yang, Z.; Wang, J.; Weng, Y.; Tu, Q.; Jiang, C.; Huang, N. In Vitro Investigation of Enhanced Hemocompatibility and Endothelial Cell Proliferation Associated with Quinone-Rich Polydopamine Coating. ACS Appl. Mater. Interfaces 2013, 5, 1704–1714. [Google Scholar] [CrossRef]
- Hou, R.; Wu, L.; Wang, J.; Yang, Z.; Tu, Q.; Zhang, X.; Huang, N. Surface-Degradable Drug-Eluting Stent with Anticoagulation, Antiproliferation, and Endothelialization Functions. Biomolecules 2019, 9, 69. [Google Scholar] [CrossRef] [Green Version]
- Lockwood, N.A.; Hergenrother, R.W.; Patrick, L.M.; Stucke, S.M.; Steendam, R.; Pacheco, E.; Virmani, R.; Kolodgie, F.D.; Hubbard, B. In Vitro and In Vivo Characterization of Novel Biodegradable Polymers for Application as Drug-Eluting Stent Coatings. J. Biomater. Sci. Polym. Ed. 2010, 21, 529–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steele, T.W.; Huang, C.L.; Widjaja, E.; Boey, F.Y.; Loo, J.S.; Venkatraman, S.S. The effect of polyethylene glycol structure on paclitaxel drug release and mechanical properties of PLGA thin films. Acta Biomater. 2011, 7, 1973–1983. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.; Sharma, R.; Pandey, V.; Patel, V.; Yadav, A.K. Heparin-Tailored Biopolymeric Nanocarriers in Site-Specific Delivery: A Systematic Review. Crit. Rev. Ther. Drug Carr. Syst. 2017, 34, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Chawla, A.S.; Chang, T.M.S. In-Vivo Degradation of Poly(Lactic Acid) of Different Molecular Weights. Biomater. Med. Devices Artif. Organs 1985, 13, 153–162. [Google Scholar] [CrossRef]
- Sakiyama-Elbert, S.E. Incorporation of heparin into biomaterials. Acta Biomater. 2014, 10, 1581–1587. [Google Scholar] [CrossRef] [Green Version]
- Pugazhendhi, A.; Edison, T.N.J.I.; Karuppusamy, I.; Kathirvel, B. Inorganic nanoparticles: A potential cancer therapy for human welfare. Int. J. Pharm. 2018, 539, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Baeza, A.; Ruiz-Molina, D.; Vallet-Regí, M. Recent advances in porous nanoparticles for drug delivery in antitumoral applications: Inorganic nanoparticles and nanoscale metal-organic frameworks. Expert Opin. Drug Deliv. 2017, 14, 783–796. [Google Scholar] [CrossRef]
- Chatterjee, A.; Bharadiya, P.; Hansora, D. Layered double hydroxide based bionanocomposites. Appl. Clay Sci. 2019, 177, 19–36. [Google Scholar] [CrossRef]
- Ladewig, K.; Xu, Z.P.; Lu, G.Q. (Max) Layered double hydroxide nanoparticles in gene and drug delivery. Expert Opin. Drug Deliv. 2009, 6, 907–922. [Google Scholar] [CrossRef]
- Li, L.; Gu, W.; Chen, J.; Chen, W.; Xu, Z.P. Co-delivery of siRNAs and anti-cancer drugs using layered double hydroxide nanoparticles. Biomaterials 2014, 35, 3331–3339. [Google Scholar] [CrossRef] [Green Version]
- Kuthati, Y.; Kankala, R.K.; Lee, C.-H. Layered double hydroxide nanoparticles for biomedical applications: Current status and recent prospects. Appl. Clay Sci. 2015, 112–113, 100–116. [Google Scholar] [CrossRef]
- Bi, X.; Zhang, H.; Dou, L. Layered Double Hydroxide-Based Nanocarriers for Drug Delivery. Pharmaceutics 2014, 6, 298–332. [Google Scholar] [CrossRef]
- Sohrabnezhad, S.; Poursafar, Z.; Asadollahi, A. Synthesis of novel core@shell of MgAl layered double hydroxide @ porous magnetic shell (MgAl-LDH@PMN) as carrier for ciprofloxacin drug. Appl. Clay Sci. 2020, 190, 105586. [Google Scholar] [CrossRef]
- Chakraborty, J.; Roychowdhury, S.; Sengupta, S.; Ghosh, S. Mg–Al layered double hydroxide–methotrexate nanohybrid drug delivery system: Evaluation of efficacy. Mater. Sci. Eng. C 2013, 33, 2168–2174. [Google Scholar] [CrossRef]
- Zhao, H.; Liu, Z.; Park, S.-H.; Kim, S.-H.; Kim, J.-H.; Piao, L. Preparation and Characterization of PEG/PLA Multiblock and Triblock Copolymer. Bull. Korean Chem. Soc. 2012, 33, 1638–1642. [Google Scholar] [CrossRef] [Green Version]
- Jee, K.S.; Park, H.D.; Park, K.D.; Kim, Y.H.; Shin, J.-W. Heparin Conjugated Polylactide as a Blood Compatible Material. Biomacromolecules 2004, 5, 1877–1881. [Google Scholar] [CrossRef] [PubMed]
- Anjum, M.J.; Zhao, J.; Asl, V.Z.; Yasin, G.; Wang, W.; Wei, S.; Zhao, Z.; Khan, W.Q. In-situ intercalation of 8-hydroxyquinoline in Mg-Al LDH coating to improve the corrosion resistance of AZ31. Corros. Sci. 2019, 157, 1–10. [Google Scholar] [CrossRef]
- Jadhav, N.R.; Gaikwad, V.L.; Nair, K.J.; Kadam, H.M. Glass transition temperature: Basics and application in pharmaceutical sector. Asian J. Pharm. 2009, 3, 82. [Google Scholar] [CrossRef]
- Ritger, P.L.; Peppas, N.A. A simple equation for description of solute release II. Fickian and anomalous release from swellable devices. J. Control. Release 1987, 5, 37–42. [Google Scholar] [CrossRef]
- Paarakh, M.P.; Jose, P.A.; Setty, C.; Christoper, G. Release kinetics–concepts and applications. Int. J. Pharm. Res. Tech. 2018, 8, 12–20. [Google Scholar]
- Bedair, T.M.; Yu, S.J.; Im, S.G.; Park, B.J.; Joung, Y.K.; Han, D.K. Effects of interfacial layer wettability and thickness on the coating morphology and sirolimus release for drug-eluting stent. J. Colloid Interface Sci. 2015, 460, 189–199. [Google Scholar] [CrossRef]
- Spijker, H.; Graaff, R.; Boonstra, P.; Busscher, H.; van Oeveren, W. On the influence of flow conditions and wettability on blood material interactions. Biomaterials 2003, 24, 4717–4727. [Google Scholar] [CrossRef]
- Qi, P.; Maitz, M.F.; Huang, N. Surface modification of cardiovascular materials and implants. Surf. Coatings Technol. 2013, 233, 80–90. [Google Scholar] [CrossRef]
- Ranade, S.V.; Miller, K.M.; Richard, R.E.; Chan, A.K.; Allen, M.J.; Helmus, M.N. Physical characterization of controlled release of paclitaxel from the TAXUS™ Express2™ drug-eluting stent. J. Biomed. Mater. Res. Part A 2004, 71, 625–634. [Google Scholar] [CrossRef]
- Shanshan, C.; Lili, T.; Yingxue, T.; Bingchun, Z.; Ke, Y. Study of drug-eluting coating on metal coronary stent. Mater. Sci. Eng. C 2013, 33, 1476–1480. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Lin, S.; Du, R.; Fu, M.; Rao, Q.; Yin, T.; Huang, Y.; Wang, G. Design, preparation and performance of a novel drug-eluting stent with multiple layer coatings. Biomater. Sci. 2017, 5, 1845–1857. [Google Scholar] [CrossRef]
- Sevim, K.; Pan, J. A model for hydrolytic degradation and erosion of biodegradable polymers. Acta Biomater. 2018, 66, 192–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raval, A.; Parikh, J.; Engineer, C. Mechanism and in Vitro Release Kinetic Study of Sirolimus from a Biodegradable Polymeric Matrix Coated Cardiovascular Stent. Ind. Eng. Chem. Res. 2011, 50, 9539–9549. [Google Scholar] [CrossRef]
- Zhu, X.; Braatz, R.D. A mechanistic model for drug release in PLGA biodegradable stent coatings coupled with polymer degradation and erosion. J. Biomed. Mater. Res. Part A 2015, 103, 2269–2279. [Google Scholar] [CrossRef] [Green Version]
- Vos, N.S.; Fagel, N.D.; Amoroso, G.; Herrman, J.-P.R.; Patterson, M.S.; Piers, L.H.; van der Schaaf, R.J.; Slagboom, T.; Vink, M.A. Paclitaxel-coated balloon angioplasty versus drug-eluting stent in acute myocardial infarction: The REVELATION randomized trial. JACC Cardiovasc. Interv. 2019, 12, 1691–1699. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Wang, W.; Zhou, C.; Jin, C.; Leng, X.; Li, Y.; Zhang, X.; Chen, S.; Zhang, B.; Yang, K. In vitro degradation and biocompatibility evaluation of fully biobased thermoplastic elastomers consisting of poly (β-myrcene) and poly (l-lactide) as stent coating. Polym. Degrad. Stab. 2020, 179, 109254. [Google Scholar] [CrossRef]
- El-Hayek, G.; Bangalore, S.; Dominguez, A.C.; Devireddy, C.; Jaber, W.; Kumar, G.; Mavromatis, K.; Tamis-Holland, J.; Samady, H. Meta-Analysis of Randomized Clinical Trials Comparing Biodegradable Polymer Drug-Eluting Stent to Second-Generation Durable Polymer Drug-Eluting Stents. JACC Cardiovasc. Interv. 2017, 10, 462–473. [Google Scholar] [CrossRef] [PubMed]





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Models | R2 Values | ||||
|---|---|---|---|---|---|
| BCA-LDH-I | BCA-LDH-C | PLA-PEG-Heparin-BCA-LDH-I | PLA-PEG-Heparin-BCA-LDH-C | ||
| Zero-order | 0.952 | 0.996 | 0.906 | 0.912 | |
| (First 60%) | (First 60%) | (First 60%) | (First 60%) | ||
| 0.901 (overall) | 0.859 (overall) | 0.845 (overall) | 0.878 (overall) | ||
| First-order | 0.730 | 0.793 | 0.815 | 0.762 | |
| Higuchi | 0.825 | 0.898 | 0.932 | 0.955 | |
| Korsmeyer–Peppas (Mt/M∞ ≤ 0.6) | R2 | 0.912 | 0.917 | 0.889 | 0.901 |
| n | 0.92 | 1.11 | 0.85 | 0.79 | |
| Models | Release Coefficient (k) | |||
|---|---|---|---|---|
| BCA-LDH-I | BCA-LDH-C | PLA-PEG-Heparin-BCA-LDH-I | PLA-PEG-Heparin-BCA-LDH-C | |
| Zero-order | 13.1 | 12.2 | −4.3 | −3.5 |
| First-order | 1.4 | 1.5 | 2.7 | 2.9 |
| Higuchi | 2.77 | 2.65 | 0.975 | 0.955 |
| Korsmeyer–Peppas (Mt/M∞ ≤ 0.6) | 0.35 | 0.41 | 1.23 | 1.12 |
| Time (In Weeks) | Zeta Potential (mV) | Mean Zeta Potential (mV) | ||
|---|---|---|---|---|
| i | ii | iii | ||
| 1 | 15.1 | 15.0 | 15.2 | 15.1 |
| 2 | 15 | 15.1 | 14.9 | 15 |
| 3 | 15 | 14.9 | 15.1 | 15 |
| 4 | 14.7 | 14.9 | 14.8 | 14.7 |
| 5 | 14.8 | 14.9 | 14.7 | 14.8 |
| 6 | 14.9 | 15 | 14.8 | 14.9 |
| 7 | 14.8 | 14.7 | 14.9 | 14.8 |
| Time (In Weeks) | Size (nm) | Average (nm) | PDI | ||
|---|---|---|---|---|---|
| i | ii | iii | |||
| 1 | 241.1 | 241.0 | 241.2 | 241.1 | 0.272 |
| 2 | 244.1 | 244.0 | 244.2 | 244.1 | 0.253 |
| 3 | 248.1 | 248.3 | 248.0 | 248.2 | 0.241 |
| 4 | 250.1 | 250.0 | 250.3 | 250.1 | 0.220 |
| 5 | 250.1 | 250.3 | 250.1 | 250.2 | 0.213 |
| 6 | 255.5 | 255.6 | 255.5 | 255.5 | 0.261 |
| 7 | 258.3 | 258.4 | 258.3 | 258.3 | 0.274 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adepu, S.; Luo, H.; Ramakrishna, S. Heparin-Tagged PLA-PEG Copolymer-Encapsulated Biochanin A-Loaded (Mg/Al) LDH Nanoparticles Recommended for Non-Thrombogenic and Anti-Proliferative Stent Coating. Int. J. Mol. Sci. 2021, 22, 5433. https://doi.org/10.3390/ijms22115433
Adepu S, Luo H, Ramakrishna S. Heparin-Tagged PLA-PEG Copolymer-Encapsulated Biochanin A-Loaded (Mg/Al) LDH Nanoparticles Recommended for Non-Thrombogenic and Anti-Proliferative Stent Coating. International Journal of Molecular Sciences. 2021; 22(11):5433. https://doi.org/10.3390/ijms22115433
Chicago/Turabian StyleAdepu, Shivakalyani, Hongrong Luo, and Seeram Ramakrishna. 2021. "Heparin-Tagged PLA-PEG Copolymer-Encapsulated Biochanin A-Loaded (Mg/Al) LDH Nanoparticles Recommended for Non-Thrombogenic and Anti-Proliferative Stent Coating" International Journal of Molecular Sciences 22, no. 11: 5433. https://doi.org/10.3390/ijms22115433