
Towards a Precision Medicine Approach Based on Machine Learning for Tailoring Medical Treatment in Alkaptonuria

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset
- painkillers: opioid, paracetamol, metamizole;
- anti-inflammatories: Non-steroidal anti-inflammatory drugs (FANS), corticosteroid;
- others: antiacid, antiarhythmic, antiasthma, antibiotic, anticoagulant, anticonvulsant, antidepressant, antiglaucoma, antigout, antihistamine, antihyperglycemic, antihypertensive, antimuscarinic, antiosteoporotic, antiparkinson, antipsychotic, antireumatic, antiviral, calcium, cholesterol-lowering medication, corticosteroid, diuretic, hormone, methotrexate, proton pump inhibitor, skeletal muscle relaxant, sodium chloride, thyroid hormones, vitamins.
2.2. Machine Learning Classification
- accuracy:
- recall:
- precision:
- score:
- Matthews correlation coefficient (MCC) [20]:
2.3. Techniques in Determining Correlation
3. Results
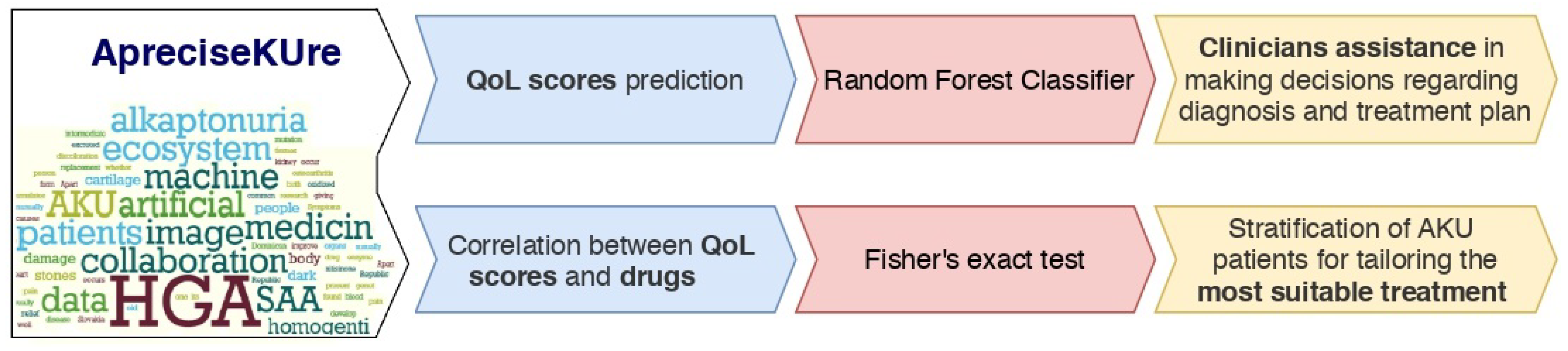
3.1. Quality of Life Scores Prediction
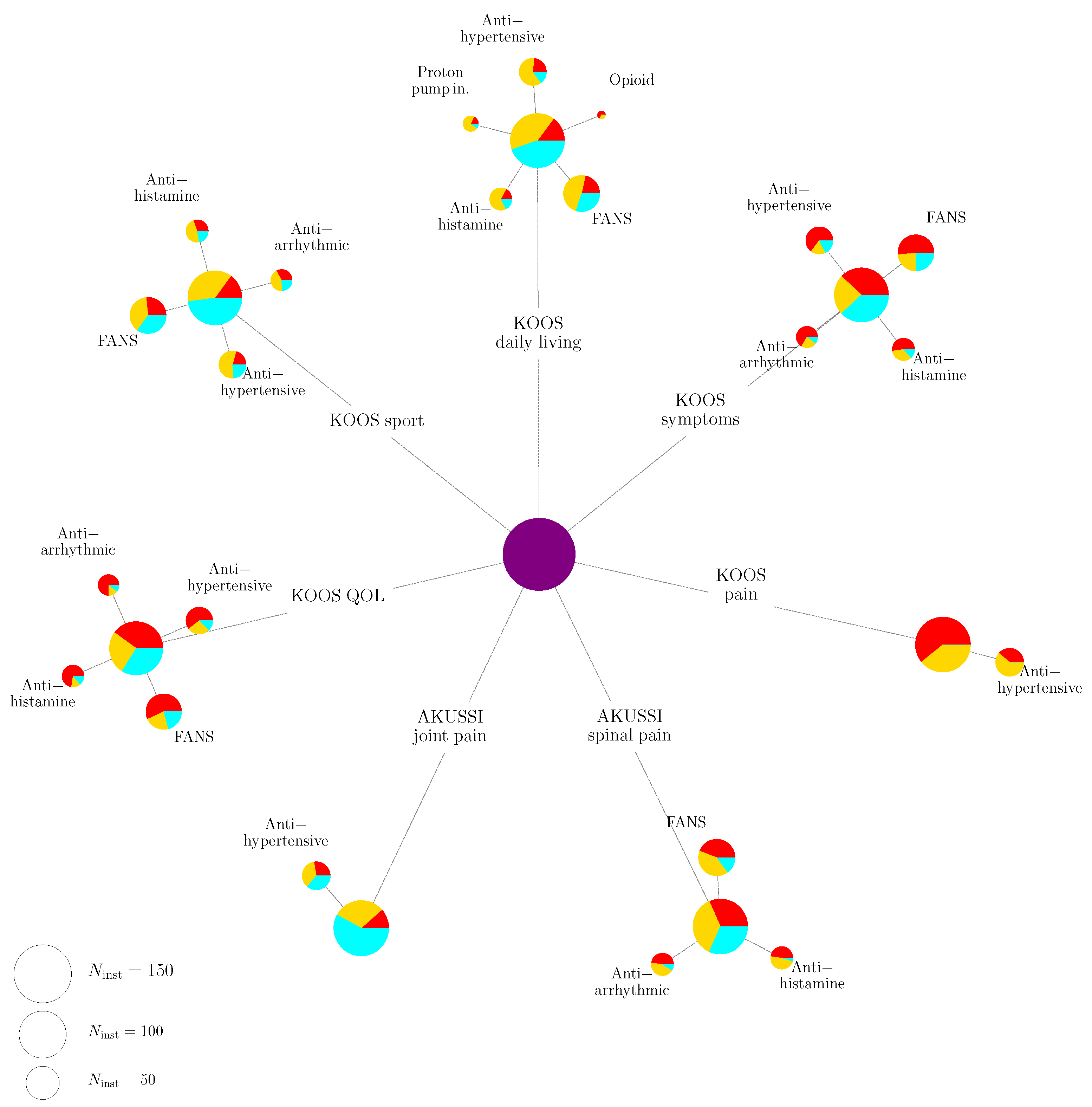
3.2. Correlation between Drugs and Quality of Life Scores
4. Discussion
5. Conclusions
- Prediction of the QoL scores based on both personal and clinical AKU patients’ information collected in ApreciseKUre.
- The investigation of the correlation between the values of the QoL scores and the drugs the patients take.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bahcall, O. Precision medicine. Nature 2015, 335. [Google Scholar] [CrossRef] [PubMed]
- Aronson, S.; Rehm, H. Building the foundation for genomics in precision medicine. Nature 2015, 526, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Nemethova, M.; Radvanszky, J.; Kadasi, L.; Ascher, D.B.; Pires, D.E.V.; Blundell, T.L.; Porfirio, B.; Mannoni, A.; Santucci, A.; Milucci, L.; et al. Twelve novel HGD gene variants identified in 99 alkaptonuria patients: Focus on ‘black bone disease’ in Italy. Eur. J. Hum. Genet. 2016, 24, 66–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ascher, D.; Spiga, O.; Sekelska, M.; Pires, D.; Bernini, A.; Tiezzi, M.; Kralovicova, J.; Borovska, I.; Soltysova, A.; Olsson, B.; et al. Homogentisate 1,2-dioxygenase (HGD) gene variants, their analysis and genotype-phenotype correlations in the largest cohort of patients with AKU. Eur. J. Hum. Genet. 2019, 27, 888–902. [Google Scholar] [CrossRef]
- Millucci, L.; Bernardini, G.; Spreafico, A.; Orlandini, M.; Braconi, D.; Laschi, M.; Geminiani, M.; Lupetti, P.; Giorgetti, G.; Viti, C.; et al. Histological and Ultrastructural Characterization of Alkaptonuric Tissues. Calcif. Tissue Int. 2017, 101, 50–64. [Google Scholar] [CrossRef]
- Bernardini, G.; Laschi, M.; Geminiani, M.; Braconi, D.; Vannuccini, E.; Lupetti, P.; Manetti, F.; Millucci, L.; Santucci, A. Homogentisate 1,2 dioxygenase is expressed in brain: Implications in alkaptonuria. J. Inherit. Metab. Dis. 2015, 38, 807–814. [Google Scholar] [CrossRef]
- Millucci, L.; Ghezzi, L.; Paccagnini, E.; Giorgetti, G.; Viti, C.; Braconi, D.; Laschi, M.; Geminiani, M.; Soldani, P.; Lupetti, P.; et al. Amyloidosis, inflammation, and oxidative stress in the heart of an alkaptonuric patient. Mediat. Inflamm. 2014, 2014, 258471. [Google Scholar] [CrossRef]
- Millucci, L.; Ghezzi, L.; Braconi, D.; Laschi, M.; Geminiani, M.; Amato, L.; Orlandini, M.; Benvenuti, C.; Bernardini, G.; Santucci, A. Secondary amyloidosis in an alkaptonuric aortic valve. Int. J. Cardiol. 2014, 172, 121–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braconi, D.; Millucci, L.; Bernardini, G.; Santucci, A. Oxidative stress and mechanisms of ochronosis in alkaptonuria. Free. Radic. Biol. Med. 2015, 88, 70–80. [Google Scholar] [CrossRef]
- Cicaloni, V.; Zugarini, A.; Rossi, A.; Zazzeri, M.; Santucci, A.; Bernini, A.O.S. Towards an integrated interactive database for the search of stratification biomarkers in Alkaptonuria. PeerJ Prepr. 2016. [Google Scholar] [CrossRef]
- Spiga, O.; Cicaloni, V.; Bernini, A.; Zatkova, A.; Santucci, A. ApreciseKUre: An approach of Precision Medicine in a Rare Disease. BMC Med. Inform. Decis. Mak. 2017, 17, 42. [Google Scholar] [CrossRef] [PubMed]
- Spiga, O.; Cicaloni, V.; Zatkova, A.; Millucci, L.; Bernardini, G.; Bernini, A.; Marzocchi, B.; Bianchini, M.; Zugarini, A.; Rossi, A.; et al. A new integrated and interactive tool applicable to inborn errors of metabolism: Application to alkaptonuria. Comput. Biol. Med. 2018, 103, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cicaloni, V.; Spiga, O.; Dimitri, G.M.; Maiocchi, R.; Millucci, L.; Giustarini, D.; Bernardini, G.; Bernini, A.; Marzocchi, B.; Braconi, D.; et al. Interactive alkaptonuria database: Investigating clinical data to improve patient care in a rare disease. FASEB J. 2019, 33, 12696–12703. [Google Scholar] [CrossRef] [Green Version]
- Spiga, O.; Cicaloni, V.; Fiorini, C.; Trezza, A.; Visibelli, A.; Millucci, L.; Bernardini, G.; Bernini, A.; Marzocchi, B.; Braconi, D.; et al. Machine learning application for development of a data-driven predictive model able to investigate quality of life scores in a rare disease. Orphanet J. Rare Dis. 2020, 15, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossi, A.; Giacomini, G.; Cicaloni, V.; Galderisi, S.; Milella, M.S.; Bernini, A.; Millucci, L.; Spiga, O.; Bianchini, M.; Santucci, A. AKUImg: A database of cartilage images of Alkaptonuria patients. Comput. Biol. Med. 2020, 122, 103863. [Google Scholar] [CrossRef] [PubMed]
- Spreafico, A.; Millucci, L.; Ghezzi, L.; Geminiani, M.; Braconi, D.; Amato, L.; Chellini, F.; Frediani, B.; Moretti, E.; Collodel, G.; et al. Antioxidants inhibit SAA formation and pro-inflammatory cytokine release in a human cell model of alkaptonuria. Rheumatology 2013, 52, 1667–1673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millucci, L.; Spreafico, A.; Tinti, L.; Braconi, D.; Ghezzi, L.; Paccagnini, E.; Bernardini, G.; Amato, L.; Laschi, M.; Selvi, E.; et al. Alkaptonuria is a novel human secondary amyloidogenic disease. Biochim. Biophys. Acta Mol. Basis Dis. 2012, 1822, 1682–1691. [Google Scholar] [CrossRef] [Green Version]
- Ho, T.K. Random decision forests. In Proceedings of the 3rd International Conference on Document Analysis and Recognition, Montreal, QC, Canada, 14–16 August 1995; Volume 1, pp. 278–282. [Google Scholar]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Matthews, B. Comparison of the predicted and observed secondary structure of T4 phage lysozyme. Biochim. Biophys. Acta Protein Struct. 1975, 405, 442–451. [Google Scholar] [CrossRef]
- Chicco, D. Ten quick tips for machine learning in computational biology. BioData Min. 2017, 10, 35. [Google Scholar] [CrossRef]
- Chicco, D.; Jurman, G. The advantages of the Matthews correlation coefficient (MCC) over F1 score and accuracy in binary classification evaluation. BMC Genom. 2020, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortes, C.; Vapnik, V. Support-Vector Networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 1–8. [Google Scholar]
- de Haas, V.; Weber, E.C.; De Klerk, J.; Bakker, H.; Smit, G.; Huijbers, W.; Duran, M. The success of dietary protein restriction in alkaptonuria patients is age-dependent. J. Inherit. Metab. Dis. 1998, 21, 791–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thakur, S.; Markman, P.; Cullen, H. Choice of valve prosthesis in a rare clinical condition: Aortic stenosis due to alkaptonuria. Hear. Lung Circ. 2013, 22, 870–872. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| QoL Score | |||||
|---|---|---|---|---|---|
| AKU joint pain | 10 | 0.718 | 6 | 8 | 53 |
| AKU spinal pain | 23 | 0.990 | 27 | 14 | 72 |
| KOOS pain | 1 | 0.718 | 5 | 17 | 51 |
| KOOS symptoms | 10 | 0.609 | 21 | 17 | 94 |
| KOOS daily living | 2 | 0.554 | 25 | 44 | 78 |
| KOOS sport | 23 | 0.663 | 23 | 52 | 56 |
| KOOS QOL | 6 | 0.554 | 10 | 25 | 80 |
| hapVAS | 24 | 0.554 | 24 | 13 | 38 |
| Accuracy | Precision | Recall | MCC | N | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| AKU joint pain | 0.669 | 0.052 | 0.530 | 0.082 | 0.593 | 0.061 | 0.530 | 0.071 | 0.180 | 0.095 | 138 |
| AKU spinal pain | 0.589 | 0.046 | 0.327 | 0.111 | 0.440 | 0.065 | 0.342 | 0.084 | 0.037 | 0.101 | 138 |
| KOOS pain | 0.648 | 0.064 | 0.487 | 0.084 | 0.547 | 0.077 | 0.495 | 0.085 | 0.204 | 0.127 | 134 |
| KOOS symptoms | 0.657 | 0.070 | 0.543 | 0.111 | 0.585 | 0.089 | 0.542 | 0.102 | 0.235 | 0.147 | 134 |
| KOOS daily living | 0.718 | 0.044 | 0.553 | 0.064 | 0.623 | 0.061 | 0.578 | 0.061 | 0.346 | 0.089 | 134 |
| KOOS sport | 0.689 | 0.049 | 0.415 | 0.086 | 0.546 | 0.073 | 0.464 | 0.079 | 0.275 | 0.096 | 130 |
| KOOS QOL | 0.662 | 0.050 | 0.463 | 0.129 | 0.509 | 0.076 | 0.460 | 0.090 | 0.232 | 0.112 | 134 |
| hapVAS | 0.571 | 0.054 | 0.371 | 0.136 | 0.359 | 0.086 | 0.325 | 0.098 | 0.066 | 0.127 | 136 |
| HAQ-DI | 0.624 | 0.084 | 0.624 | 0.104 | 0.624 | 0.084 | 0.596 | 0.096 | 0.163 | 0.183 | 138 |
| FANS | Antiarry- | Antihi- | Antihyper- | Cholesterol- | Opioid | Proton | Vitamins | |
|---|---|---|---|---|---|---|---|---|
| Thmic | Stamine | Tensive | Lowering | Pump in. | ||||
| AKUSSI | no | no | no | yes | no | no | no | no |
| joint pain | ||||||||
| AKUSSI | no | no | no | yes | no | no | no | no |
| spinal pain | ||||||||
| KOOS | yes | yes | yes | yes | no | yes | yes | yes |
| pain | ||||||||
| KOOS | no | no | no | yes | no | no | no | no |
| symptoms | ||||||||
| KOOS | yes | no | no | yes | yes | no | yes | no |
| daily living | ||||||||
| KOOS | yes | no | no | yes | no | yes | yes | no |
| sport | ||||||||
| KOOS | yes | no | no | yes | no | yes | yes | no |
| QOL | ||||||||
| HAQ- | yes | no | no | no | no | yes | yes | no |
| DI | ||||||||
| hap- | yes | no | no | no | no | yes | yes | no |
| VAS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spiga, O.; Cicaloni, V.; Visibelli, A.; Davoli, A.; Paparo, M.A.; Orlandini, M.; Vecchi, B.; Santucci, A. Towards a Precision Medicine Approach Based on Machine Learning for Tailoring Medical Treatment in Alkaptonuria. Int. J. Mol. Sci. 2021, 22, 1187. https://doi.org/10.3390/ijms22031187
Spiga O, Cicaloni V, Visibelli A, Davoli A, Paparo MA, Orlandini M, Vecchi B, Santucci A. Towards a Precision Medicine Approach Based on Machine Learning for Tailoring Medical Treatment in Alkaptonuria. International Journal of Molecular Sciences. 2021; 22(3):1187. https://doi.org/10.3390/ijms22031187
Chicago/Turabian StyleSpiga, Ottavia, Vittoria Cicaloni, Anna Visibelli, Alessandro Davoli, Maria Ausilia Paparo, Maurizio Orlandini, Barbara Vecchi, and Annalisa Santucci. 2021. "Towards a Precision Medicine Approach Based on Machine Learning for Tailoring Medical Treatment in Alkaptonuria" International Journal of Molecular Sciences 22, no. 3: 1187. https://doi.org/10.3390/ijms22031187